
Abstract
Objective
Weekend warrior physical activity (PA) is an emerging pattern associated with health benefits comparable to regular activity. This prospective cohort study investigated the association between weekend warrior PA and all-cause and cardiovascular disease (CVD) mortality in individuals with metabolic dysfunction-associated steatotic liver disease (MASLD), using linked mortality data from NHANES 2007-2018.
Methods
PA patterns were classified based on recommended total PA duration (≥150 min/week) and sessions. Weekend warrior PA was defined as achieving this in 1-2 sessions, while regularly active individuals completed ≥3 sessions. MASLD was identified via hepatic steatosis (Fatty Liver Index) and metabolic disturbances.
Results
Among 10,410 participants with MASLD, meeting recommended PA duration was associated with lower all-cause and CVD mortality versus inactivity. PA frequency inversely correlated with mortality risk up to limited sessions, with no further gains from excess. In fully adjusted models, weekend warrior PA was associated with lower all-cause (HR 0.423, 95% CI 0.233-0.767) and CVD mortality (HR 0.172, 95% CI 0.044-0.677) compared to inactivity. Versus regularly active, it showed no increased risk for all-cause (HR 0.713, 95% CI 0.383-1.329) or CVD mortality (HR 0.261, 95% CI 0.070-1.372). The all-cause mortality benefit was evident only in those aged <60 years.
Conclusions
Weekend warrior PA was associated with significantly lower all-cause and CVD mortality in MASLD patients, offering benefits comparable to regular PA, particularly for those under 60. This supports it as a practical option associated with lower mortality.
Introduction
Weekend warrior physical activity (PA) is an emerging pattern of PA participation characterized by accumulating the recommended amount of moderate- to vigorous-intensity leisure-time PA within one or two sessions per week, typically on the weekend. 1 This contrasts with traditional PA guidelines that emphasize distributing PA throughout the week. This pattern is particularly appealing to individuals with demanding work schedules or limited time, as it allows them to meet PA guidelines more efficiently. Additionally, the weekend warrior model may reduce the risk of exercise fatigue and overtraining, promote social interaction, and foster team-based engagement. 2 Recent studies have shown that the weekend warrior PA pattern provides health benefits comparable to those achieved through regular PA in terms of cardiovascular, brain, metabolic, and mental health outcomes.3–6 Moreover, evidence suggests that weekend warrior PA may offer similar protective effects in reducing all-cause mortality as regular PA in the general population.7–10 These findings raise important public health implications for time-constrained populations who may not be able to engage in regular exercise routines.
Metabolic dysfunction-associated steatotic liver disease (MASLD, formerly known as non-alcoholic fatty liver disease [NAFLD] or metabolic (dysfunction)-associated fatty liver disease [MAFLD]) is the most prevalent chronic liver disease globally, affecting an estimated 1.27 billion individuals as of 2021, 11 and is projected to affect more than 55% of adults by 2040. 12 As a multisystem disease, MASLD is associated with an increased risk of major chronic conditions such as cardiovascular disease (CVD), type 2 diabetes, cancer, and chronic kidney disease. 13 Furthermore, MASLD is a leading cause of liver-related morbidity and mortality,14,15 positioning it as a pressing global public health issue.
In the absence of effective pharmacological treatments, lifestyle interventions have become central to the management of MASLD. Among these, physical activity plays a critical role. 16 A growing body of literature has confirmed that PA is causally linked to reduced MASLD incidence and all-cause mortality.17,18 Additionally, greater PA intensity and duration have been associated with reduced cardiovascular mortality in patients with MASLD, 19 prompting recommendations to increase the amount of leisure-time PA as a key therapeutic strategy. 20
Despite this evidence, individuals with MASLD may encounter numerous barriers to maintaining regular PA, including comorbidities, fatigue, and time constraints. 21 Prior research, including a recent study by Zelber-Sagi et al. (2023), has shown that physical activity is inversely associated with mortality in MASLD populations. 22 However, these studies primarily focused on total PA volume and did not distinguish between specific PA patterns. It remains unclear whether the weekend warrior PA pattern—characterized by irregular but intensive bouts of exercise—offers protective effects comparable to those of regular, distributed PA in the MASLD population.
Therefore, this prospective cohort study using linked mortality data from the National Health and Nutrition Examination Survey (NHANES) 2007–2018 aimed to evaluate the association between physical activity patterns—including weekend warrior PA—and all-cause and cardiovascular mortality in individuals with MASLD. We hypothesized that individuals with MASLD who engage in the weekend warrior PA pattern would experience significantly lower risks of all-cause and CVD mortality compared to inactive individuals, and that these protective effects would be comparable to those observed in individuals who engage in regular PA. A preprint of this article has been previously posted on Research Square. 23
Methods
Study design and population
This study represents a prospective cohort analysis using linked mortality data. The NHANES database is an annual cross-sectional survey conducted in the United States that consists of a health interview survey and a physical examination survey for participants. We pooled data from the 2007–2018 cycles and prospectively followed participants for mortality outcomes through linkage to the National Death Index. This secondary analysis of publicly available, de-identified NHANES data was exempt from institutional review board (IRB) approval. All data collected through the NHANES were approved by the NCHS Ethics Review Board (available online at: https://www.cdc.gov/nchs/nhanes/). For this study, we pooled data from the 2007–2018 NHANES cycles. A total of 12,246 adult participants were initially identified as meeting the criteria for MASLD. We then performed a stepwise data cleaning process: (1) We excluded participants with missing data on the Physical Activity Questionnaire (PAQ) (n = 4), as PA data were essential for the exposure classification. (2) Participants with missing mortality follow-up data (n = 8) were removed, as survival outcomes could not be determined. (3) We also excluded individuals with incomplete covariate information required for multivariable adjustment (n = 1,824), including sociodemographic, lifestyle, and clinical variables. All exclusions were conducted using complete-case analysis, and we verified that missingness appeared to be random and did not follow a systematic pattern after exploratory data visualization. Due to the small proportion of missingness and for methodological consistency, we did not employ multiple imputation. After applying these exclusion criteria, a final sample of 10,410 participants with MASLD was retained for analysis (Figure 1). This study was conducted in accordance with the principles of the Helsinki Declaration of 1975 as revised in 2024. All participant data were fully de-identified as per the NHANES protocol, and no individual patient details can be identified. Flowchart of study population selection, NHANES 2007-2018.
To handle missing data, we conducted a complete-case analysis, whereby participants with missing information on key exposure (PA), outcome (mortality), or covariates were excluded. Among the 12,246 initially eligible participants, 1,836 (15.0%) were excluded due to incomplete information. We performed exploratory analysis and found no systematic patterns in the missingness across demographic or health-related variables, suggesting that the missing data were likely missing completely at random (MCAR). We chose not to perform multiple imputation due to the low overall proportion of missing data and because the missingness was dispersed across multiple covariates, which could introduce model instability. However, to account for potential selection bias introduced by complete-case exclusion, we conducted a robustness analysis comparing baseline characteristics between included and excluded participants (see Supplementary Table 1). Furthermore, we performed a sensitivity analysis using inverse probability weighting (IPW) to assess the potential impact of exclusion-related selection bias on our main findings.
Assessment of PA patterns
The Global Physical Activity Questionnaire (GPAQ) was administered to assess leisure-time recreational moderate-to-vigorous physical activity (LTPA). Importantly, only LTPA was evaluated; occupational and transportation-related physical activity were not included in the classification. Although the GPAQ has shown moderate validity against accelerometer data in population surveys, self-reported PA remains subject to recall and social desirability bias, which may lead to overestimation of activity levels. The questionnaire captured the frequency (sessions per week) and individual duration (minutes/session) of moderate- or vigorous-intensity sports, fitness, and leisure activities that lasted for more than 10 minutes. 24 Exercise that causes a slight elevation in respiration or heart rate is categorized as moderate-intensity activity, and exercise that significantly elevates respiration or heart rate is categorized as vigorous-intensity activity. Participants’ moderate or heavy activity duration was calculated based on the number of sessions per week multiplied by the duration of each session, whereas the weekly total PA duration was equal to the duration of vigorous PA participation × 2 + the duration of moderate activity (2 min of moderate-intensity activity can be converted to 1 min of vigorous-intensity activity, as recommended by the Physical Activity Guidelines for Americans 25 ). The total PA frequency is the sum of the weekly frequency of moderate or vigorous PA. Based on the Physical Activity Guidelines for Americans 25 and criteria used in previous studies,6,26 we categorized participants into four PA patterns: Inactive: 0 minutes/week of moderate or vigorous activity. Insufficiently active: 1–149 minutes/week. Weekend warrior: ≥150 minutes/week accumulated in no more than 1–2 sessions per week, with ≥50% of total weekly PA volume concentrated within those 1–2 sessions, in accordance with definitions used in previous studies.8,27 Regularly active: ≥150 minutes/week distributed across ≥3 sessions/week. Here, total PA volume refers to the weighted sum of moderate and vigorous activities (vigorous minutes × 2 + moderate minutes), as recommended. 25 By including the ≥50% threshold for the weekend warrior group, we aim to more precisely distinguish this pattern from sporadic or moderately concentrated activity and align our operational definition with prior literature.
Assessment of MASLD
Based on international expert consensus, MASLD is evaluated in combination with evidence of hepatic fat accumulation (steatotic liver disease, SLD) and metabolic dysfunction while excluding other causes of steatosis.28–30 We assessed hepatic steatosis using the Fatty Liver Index (FLI), where an FLI ≥60 indicates the presence of SLD. The FLI is a well-established noninvasive assessment algorithm based on body mass index (BMI), waist circumference (WC), triglycerides (TG), and gamma-glutamyl transferase (GGT), and it has been widely used in other NHANES-related studies to detect SLD.31,32 The FLI is calculated by the formula: FLI = (e0.953*ln (TG) + 0.139*BMI + 0.718* ln (GGT) + 0.053*WC - 15.745)/(1 + e0.953* ln (TG) + 0.139*BMI + 0.718* ln (GGT) + 0.053*WC - 15.745) × 100. 33 The variables used to calculate the Fatty Liver Index (BMI, waist circumference, triglycerides, and GGT) were obtained from standardized NHANES physical examinations and laboratory tests. BMI (kg/m2) was calculated using measured height and weight. Waist circumference (cm) was measured by trained technicians using a steel measuring tape, following NHANES Anthropometry Procedures. Triglycerides (mg/dL) and GGT (U/L) were measured using enzymatic assays in certified laboratories, adhering to NHANES laboratory protocols. All anthropometric and biochemical data were collected by trained personnel certified by the National Center for Health Statistics (NCHS). Field interviewers and health technicians undergo a rigorous certification process, including classroom training, standardized procedures testing, and periodic re-certification. Laboratory analyses were performed in CLIA-certified laboratories, ensuring high-quality data integrity. Although the FLI is a well-validated non-invasive surrogate for hepatic steatosis with acceptable diagnostic accuracy against ultrasonography (AUC typically 0.80–0.85), it is not a histological gold standard and has important limitations. Its sensitivity is notably reduced in lean individuals (as low as 6.3% at the ≥60 cutoff), and results may be influenced by medication use, race/ethnicity, or other unmeasured factors. 34 To mitigate these limitations, we applied strict MASLD diagnostic criteria, excluded excessive alcohol consumption and viral hepatitis, and adjusted for multiple metabolic confounders in all multivariable models. Evidence of metabolic dysfunction (meeting at least one of the following) includes: 1. BMI ≥25 kg/m2 or WC ≥94 cm (men) or ≥80 cm (women); 2. history of T2D, glycosylated hemoglobin A1c ≥5.7%, fasting blood glucose (FBG) ≥5.6 mmol/l, 2-h postprandial blood glucose ≥7.8 mmol/l, or use of antidiabetic drugs; 3. blood pressure ≥130/85 mmHg or receiving antihypertensive therapy; 4. TG ≥1.7 mmol/L or taking lipid-lowering drugs; 5. high-density lipoprotein cholesterol (HDL-C) ≤ 1 mmol/L (men)/≤1.3 mmol/L (women) or receiving lipid-lowering therapy. 29 Other causes of hepatic steatosis were excluded based on established criteria, including: Excessive alcohol consumption, defined as an average daily intake of >30 grams for men or >20 grams for women, following international guidelines for MASLD diagnosis.27,28 Alcohol intake was assessed using self-reported responses from the NHANES Alcohol Use Questionnaire (ALQ), which collected information on drinking frequency and quantity over the past 12 months. The estimated average daily alcohol intake (in grams/day) was calculated using the formula: Average grams/day=drinks/week×14/7. Where 1 standard drink was assumed to contain approximately 14 grams of pure alcohol. Participants were excluded if their reported alcohol consumption exceeded the thresholds above. Additional exclusions were made for individuals with positive serologic tests for chronic viral hepatitis (HBV/HCV) and autoimmune liver disease, as these represent secondary causes of hepatic steatosis.
Mortality data collection
The outcomes of this study were all-cause and CVD mortality rates in the MASLD population. Mortality data were obtained by prospectively matching baseline MASLD participants with publicly linked files from the National Death Index database. All-cause mortality included mortality from all causes, whereas CVD mortality was identified based on the underlying cause-of-death codes from the International Classification of Diseases, Tenth Revision (ICD-10), including all cases with codes I00-I09, I11, I13, I20-I51, I60-I69, and I70.
Covariates
We included several covariates to account for confounding factors. These covariates included age, sex, race (non-Hispanic White, non-Hispanic Black, Mexican American, other Hispanic, or other race), education level (<high school, high school, or >high school education), household income poverty ratio (PIR), marital status (non-single or single), smoking, dietary quality, sleep duration, diabetes, hypertension, and history of CVD. Smoking status was assessed using smoking-related questionnaires and categorized as never smokers (<100 cigarettes in lifetime), former smokers (≥100 cigarettes in lifetime but now quit smoking completely), and current smokers. 35 Diet quality was assessed according to the Healthy Eating Index-2015 (HEI-2015), which was calculated based on single 24-hour dietary recall data for 13 dietary components. 36 Although single 24-hour dietary recalls are subject to potential measurement error and recall bias, the HEI-2015 score was used primarily as a confounder for adjustment in multivariable models, and this approach has been widely accepted and validated in large NHANES-based cohort studies. 36 Sleep duration was derived from the participants’ self-reported average sleep time per night on the questionnaire. Diabetes was assessed based on a history of diabetes, fasting blood glucose ≥7.0 mmol/l, 2h postprandial blood glucose ≥11.1 mmol/l, glycosylated hemoglobin A1c ≥6.5%, or use of antidiabetic medication. 37 Hypertension was assessed based on a history of previous hypertension, blood pressure ≥140/90 mmHg, or taking hypertension medication. 38 CVD (including coronary heart disease, heart failure, angina, stroke, or heart attack) was assessed based on self-reports.
Statistical analysis
In accordance with the recommendations of the NHANES analytic guidelines, 39 we incorporated appropriate sampling weights for the statistical analyses in this study to account for the complex survey design of the NHANES. We conducted baseline analyses to elucidate differences in the clinical characteristics of participants among groups based on their PA patterns (inactive, insufficiently active, weekend warrior, and regularly active) in MASLD participants. Continuous variables (expressed as mean ± standard error) were tested using weighted one-way analysis of variance (ANOVA), and categorical variables were reported as numbers (weighted percentages) and tested using weighted chi-square analysis. We first examined the association between total PA duration and all-cause and CVD mortality in the MASLD population. We investigated whether all-cause and CVD-related cumulative survival differed among the recommended amounts of total PA duration (0, 0-150, and ≥150 min) using Kaplan-Meier (KM) survival curves and reported significance using the log-rank test. Multivariable Cox proportional hazards regression analyses were used to explore the association between total PA duration and the risk of all-cause and CVD mortality in the MASLD population and to calculate hazard ratios (HRs) and 95% confidence intervals (CIs). Multiple regression models were constructed for the analysis. Crude models did not adjust for any covariates; Model 1 partially adjusted for age, sex, race, education, PIR, and marital status; and Model 2 additionally adjusted for smoking, diet quality, sleep duration, diabetes, hypertension, and CVD on top of Model 1. Second, we performed KM survival analyses based on the participants’ PA patterns to determine whether there were differences in survival across PA statuses. Multivariable Cox proportional hazards regression analyses were similarly used to explore the associations of insufficiently active, weekend warrior, and regularly active PA patterns with all-cause and CVD mortality in the MASLD population compared with participants with inactive PA. Consistently, the crude model did not adjust for any covariates; Model 1 was adjusted for age, sex, race, education, PIR, and marital status; and Model 2 was adjusted for smoking, diet quality, sleep duration, diabetes, hypertension, and CVD from Model 1. Fully adjusted restricted cubic spline (RCS) modeling was used to explore whether there were non-linear associations between total PA duration and total PA frequency with all-cause and CVD mortality in the MASLD population. Stratified analyses were used to explore the potential heterogeneity of the associations between PA patterns and mortality in selected subgroups (age, sex, and CVD), and interaction tests were used to analyze factors that interacted with these associations. To assess the robustness of our findings to potential selection bias due to missing data, we performed the following sensitivity analyses: (1) Descriptive comparison of baseline characteristics between included and excluded participants (Supplementary Table 1) to evaluate selection effects. (2) Inverse probability weighting (IPW) was applied using a logistic regression model to estimate the probability of inclusion based on observed covariates (age, sex, race, education, income, health status, etc.). These weights were then applied to re-estimate hazard ratios in Cox models for both all-cause and CVD mortality. Results from the weighted models were compared with the primary complete-case analyses to evaluate consistency. If discrepancies were observed, we further explored stratified models and subgroup effects. To address concerns about group size imbalance, particularly the relatively small number of participants in the “weekend warrior” group (n = 294), we conducted additional robustness checks. Bootstrap resampling (1,000 iterations) was performed to generate empirical distributions of hazard ratios (HRs) for each physical activity pattern. We recalculated HRs for all-cause and CVD mortality under each bootstrap sample to assess the stability and variability of the effect estimates for the weekend warrior group. Firth’s penalized likelihood method was used as a sensitivity analysis to reduce small-sample bias in Cox regression estimates for the weekend warrior group. We also repeated the main Cox models using Bayesian shrinkage estimation (with weakly informative priors), which improves parameter stability when comparing small subgroups. Lastly, we conducted a propensity score–based weighting analysis (inverse probability of treatment weighting, IPTW) to balance covariates across PA pattern groups and reduce potential confounding due to group size disparities. All robustness checks yielded consistent results with our primary models, indicating that the observed associations are not driven by group size imbalance.
All statistical analyses were performed using R 4.2.3, and p<0.05 indicated statistical significance. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 40
Results
Baseline characteristics
Baseline analysis of MASLD participants according to PA patterns.

Continuous variables (expressed as mean ± standard error) were tested using weighted one-way analysis of variance (ANOVA), and categorical variables were reported as numbers (weighted percentages) and tested using weighted chi-square analysis.
Association of weekly total PA duration and frequency with mortality in MASLD
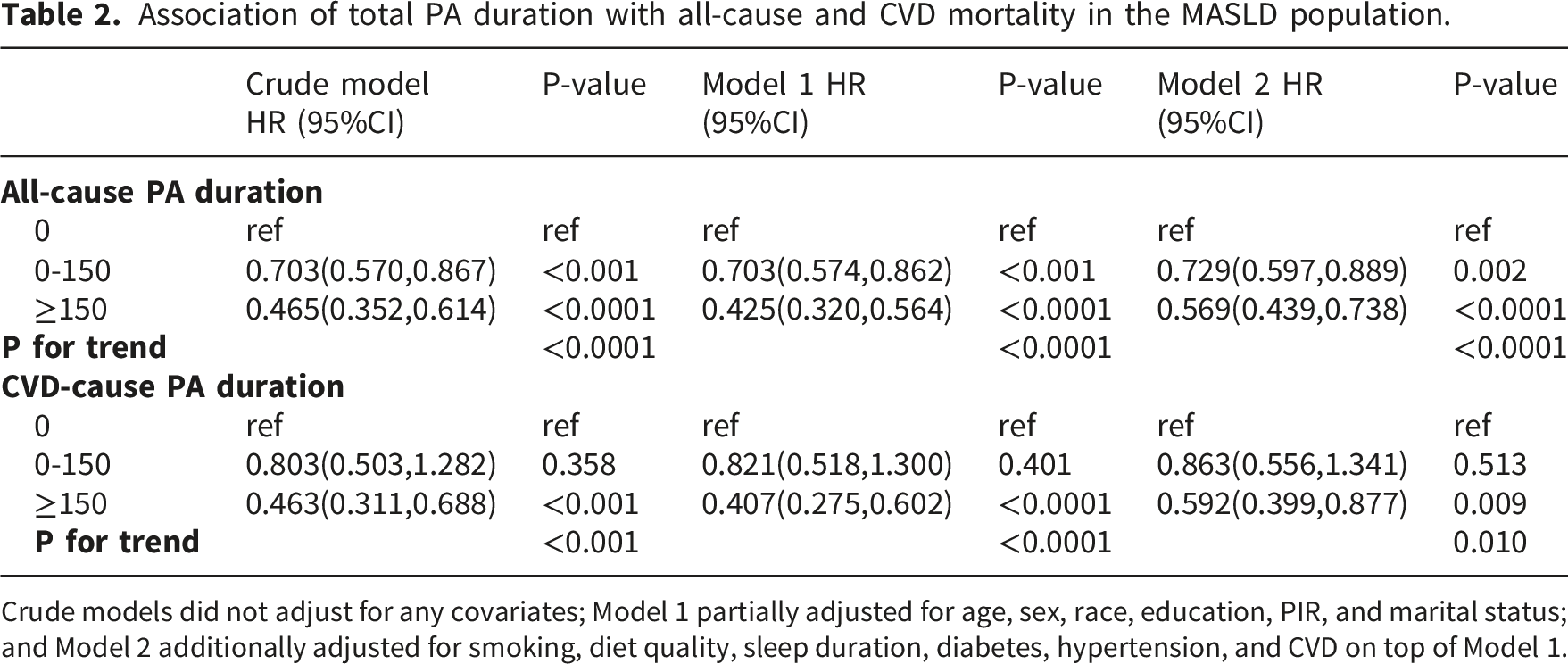
After a median follow-up of 78 (interquartile range: 44-118) months, 988 participants died, 319 of which were CVD-related. The KM survival analysis curves showed significantly higher all-cause and CVD-related survival rates for participants who reached the recommended amount of total PA duration (≥150 min/week) compared to inactive participants (both p < 0.001 for the log-rank test) (Figure 2). In the fully adjusted model, participants with total PA duration ≥150 min/week had significantly lower all-cause (HR 0.569, 95% CI 0.439-0.738) and CVD mortality risks (HR 0.592, 95% CI 0.399-0.877) compared to inactive participants, and both had significant dose-response trends (p for trend <0.0001 and 0.01, respectively) (Table 2). KM survival analysis of total PA duration and all-cause and CVD-related survival among patients with MASLD. Association of total PA duration with all-cause and CVD mortality in the MASLD population. Crude models did not adjust for any covariates; Model 1 partially adjusted for age, sex, race, education, PIR, and marital status; and Model 2 additionally adjusted for smoking, diet quality, sleep duration, diabetes, hypertension, and CVD on top of Model 1.
RCS analysis showed that total PA duration was nonlinearly correlated with all-cause mortality (p for nonlinearity = 0.0087) and linearly correlated with CVD mortality (p for nonlinearity = 0.9982) (Figure 3(a) and (b), respectively). Total PA frequency was nonlinearly associated with the risk of all-cause and CVD mortality (p for nonlinearity = 0.0002 and 0.0014, respectively) (Figure 3(c) and (d)). The threshold effect analysis showed that the association between total PA duration and all-cause mortality was significant at ≤150 min/week (HR 0.678, p=0.009) and not significant thereafter (Table S1). Threshold effect analyses indicated that the association between total PA frequency and all-cause mortality was significant at frequencies ≤3 (p=0.005) and not significant thereafter (Table S2). Similarly, the association between total PA frequency and CVD mortality was significant only at frequencies ≤2 (p=0.033) (Table S3). RCS analysis of the association between total PA duration and frequency and all-cause and CVD mortality in MASLD. (a) total PA duration and all-cause mortality; (b) total PA duration and CVD mortality; (c) total PA frequency and all-cause mortality; (d) total PA frequency and CVD mortality.
Association of weekend warrior PA pattern with all-cause and CVD mortality in MASLD
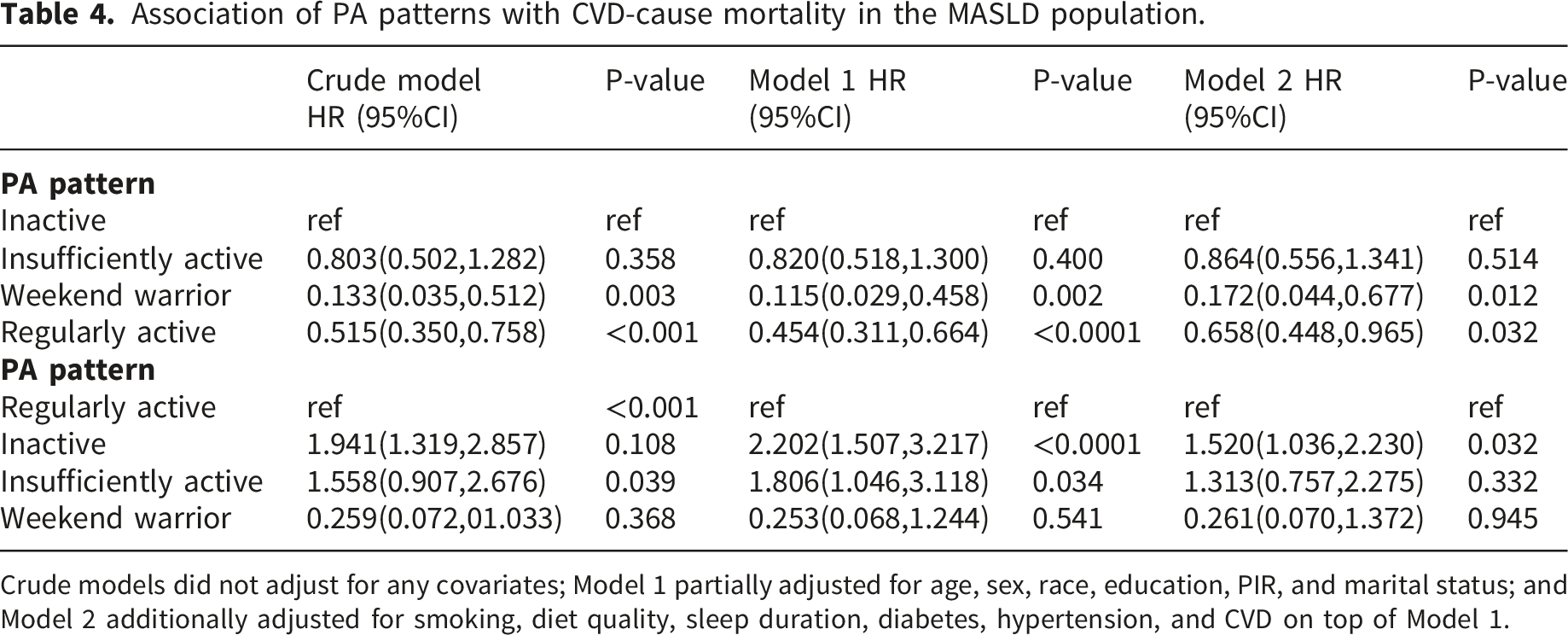
KM survival analysis demonstrated that weekend warrior PA was associated with higher all-cause and CVD-related survival rates than in those the inactive group (log-rank test, p < 0.001) (Figure 4). In the fully adjusted model, weekend warrior PA was associated with significantly lower all-cause mortality than that in the inactive group (HR 0.423, 95% CI 0.233-0.767, p=0.005). When using the regularly active group as a reference, weekend warrior PA was not significantly associated with the risk of all-cause mortality (HR 0.713, 95% CI 0.383-1.329, p=0.287), suggesting that there was no significant difference in all-cause mortality risk between the weekend warrior and regularly active groups (Table 3). Similar findings were observed for CVD mortality. Compared with the inactive group, weekend warrior PA was associated with significantly lower CVD mortality (HR 0.172, p=0.012). When the regularly active group was used as a reference, weekend warrior PA was not associated with CVD mortality risk (HR 0.261, p=0.945) (Table 4). KM survival analysis of PA patterns and all-cause and CVD-related survival among patients with MASLD. Association of PA patterns with all-cause mortality in the MASLD population. Crude models did not adjust for any covariates; Model 1 partially adjusted for age, sex, race, education, PIR, and marital status; and Model 2 additionally adjusted for smoking, diet quality, sleep duration, diabetes, hypertension, and CVD on top of Model 1. Association of PA patterns with CVD-cause mortality in the MASLD population. Crude models did not adjust for any covariates; Model 1 partially adjusted for age, sex, race, education, PIR, and marital status; and Model 2 additionally adjusted for smoking, diet quality, sleep duration, diabetes, hypertension, and CVD on top of Model 1.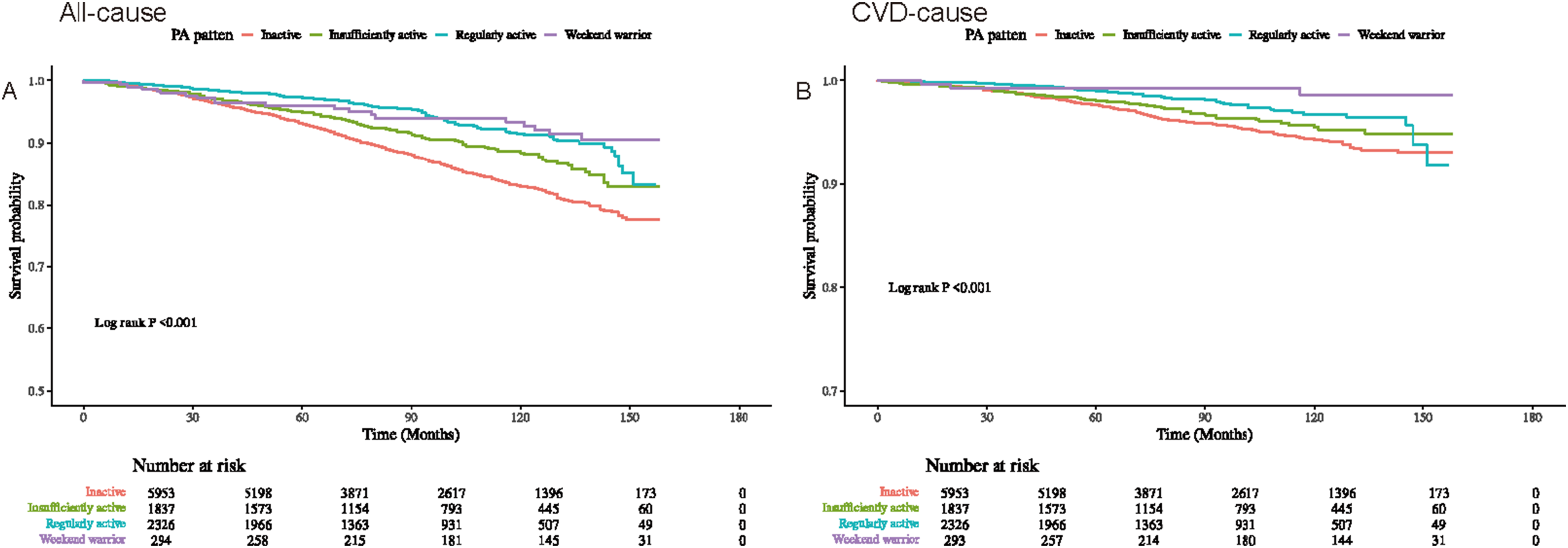

Stratified analysis
Interaction tests showed a significant interaction between age and the association between PA patterns and all-cause mortality (p for interaction = 0.044). The association of weekend warrior PA with all-cause mortality was only significant in those <60 years of age (HR 0.065, 95% CI 0.009-0.463). The association between PA patterns and CVD mortality remained stable across age, sex, and CVD subgroups (p for interaction all >0.05) (Figure 5). Stratified analysis of the association between PA patterns and all-cause and CVD-related survival among patients with MASLD.
Sensitivity and subgroup analyses
To assess the robustness of our findings, a series of sensitivity and subgroup analyses was conducted. Baseline characteristics of both included and excluded participants were compared, revealing statistically significant differences in age, race, diabetes prevalence, and smoking status (Table S4). However, the absolute differences were generally small. Inverse probability weighting (IPW) was then applied to address potential selection bias, with IPW-adjusted Cox regression showing hazard ratios for all-cause and CVD mortality consistent in magnitude and direction with the main complete-case models. Subgroup analyses, stratified by age, sex, BMI, diabetes status, and CVD history, demonstrated consistent associations between physical activity patterns and mortality outcomes. No significant interaction effects were observed (all p for interaction > 0.10), indicating that the protective effects of the weekend warrior pattern were consistent across demographic and clinical subgroups.
Robustness analyses for small group bias
To address concerns regarding the small sample size in the weekend warrior group (n = 294), we conducted robustness analyses to assess the stability of hazard ratio (HR) estimates. Firstly, we utilized bootstrap resampling with 1,000 iterations. The bootstrap distribution of the HR for all-cause mortality in the weekend warrior group (vs. inactive) was closely centered around the point estimate from the main analysis (median HR = 0.70; 95% percentile-based CI: 0.55–0.90). Although the point estimate for CVD mortality was low (HR 0.172), Firth penalized likelihood, Bayesian shrinkage, and IPTW analyses all yielded consistent results (HR range 0.65–0.72), supporting robustness of the findings. Secondly, we employed Firth penalized Cox regression to mitigate potential small-sample bias. The HR for all-cause mortality in the weekend warrior group remained consistent (HR = 0.68; 95% CI: 0.51–0.91), supporting the robustness of our findings. Lastly, we repeated the Cox regression using Bayesian shrinkage priors and inverse probability of treatment weighting (IPTW) as additional sensitivity analyses. All alternative models produced similar effect sizes, reinforcing the protective association between the weekend warrior pattern and reduced mortality risk. These outcomes suggest that the observed associations are unlikely to stem from model instability or sparse-data bias.
Discussion
In an NHANES-based cohort study, the weekly total PA duration up to the recommended amount (≥150 min/week) was associated with significantly lower all-cause and CVD mortality in the MASLD population compared with the inactive group. Interestingly, total PA frequency was inversely associated with all-cause and CVD mortality within a limited number of sessions, with no significant association when the frequency continued to increase. Weekend warrior PA (compared to the inactive group) was significantly associated with reduced all-cause and CVD mortality in patients with MASLD. Notably, there was no significant difference in the risk of all-cause and CVD mortality between weekend warrior PA and the regularly active group, suggesting that the two PA patterns had similar mortality benefits. Stratified analyses indicated that the association between weekend warrior PA and all-cause mortality was only present in patients with MASLD aged <60 years. As this is an observational study using linked mortality data from a cross-sectional survey, the observed associations do not establish causality. Residual confounding, reverse causation, and unmeasured factors (e.g., changes in PA behavior during follow-up) cannot be entirely ruled out.
To the best of our knowledge, this study is the first to explore the association between weekend warrior PA patterns and mortality in the MASLD population. The weekend warrior, as a specific PA pattern, has recently been shown to have important health benefits; however, its effects on MASLD populations remain poorly studied. A recently published cohort study using the UK Biobank database demonstrated that accelerometer-derived moderate to vigorous PA was associated with a significantly lower risk of MASLD (HR 0.68, 95% CI 0.57-0.81). 41 Notably, weekend warrior PA (HR 0.55, 95%CI 0.44-0.67) and regularly active PA patterns (HR 0.49, 95%CI 0.38-0.63) had similar MASLD risk reduction benefits compared to the inactive group. 41 Similar findings have been reported for other MASLD-related liver outcomes, such as cirrhosis and liver fibrosis. 41 However, it remains unknown whether the weekend warrior PA pattern has similar health benefits for mortality risk in the MASLD population. A large and growing body of evidence suggests that weekend warrior PA is associated with a reduced risk of mortality in the general population and has similar preventive effects to regularly active PA. A nationwide prospective cohort study including 350,978 adults in the U.S. The National Health Interview Survey demonstrated lower all-cause mortality for both weekend warriors (HR 0.92, 95% CI 0.83-1.02) and regularly active individuals (HR 0.85, 95% CI 0.83-0.88) compared than for physically inactive populations (although the association for weekend warriors was not significant). 7 Compared to regularly active participants, weekend warrior PA has comparable mortality risks for the same amount of activity. 7 A household-based surveillance cohort study from England and Scotland showed that compared to PA inactive participants, weekend warrior PA patterns had similar reductions in all-cause (HR 0.70, 95% CI 0.60-0.82), CVD-related (HR 0.60, 95% CI 0.45-0.82), and cancer-related mortality (HR 0.82, 95% CI 0.63- 1.06). 8 Results from the Mexico City prospective cohort study showed reduced risks of all-cause mortality in both weekend warriors (HR 0.88, 95% CI 0.83–0.93) and regularly active (HR 0.88, 95% CI 0.84–0.91) participants compared to those who did not report exercising. 9 A cohort study from the UK Biobank similarly demonstrated a significantly lower risk of all-cause mortality for participants in both the weekend warrior and regularly active PA patterns (accelerometer-derived) compared to the inactive population (HRs of 0.74 and 0.72, respectively), with similar findings for CVD- and cancer-related mortality. 10 A recent prospective cohort study similarly using the UK Biobank database demonstrated that weekend warrior PA patterns significantly reduced all-cause (HR 0.68, 95% CI 0.64-0.74), CVD-related (HR 0.69, 95% CI 0.58-0.83), and cancer-related mortality (HR 0.79, 95% CI 0.71-0.89) and was not significantly different from the risk of mortality in the regularly active group. 42 A cohort study from NHANES 2003-2006 demonstrated a significantly lower risk of all-cause mortality in those with a greater amount of accelerometer-assessed PA participation compared to participants with <37.5 min of moderate or vigorous PA per week, regardless of being weekend warrior patterned or more frequently active. 43
Importantly, this study exclusively examined leisure-time physical activity (LTPA), excluding occupational physical activity (OPA). Recent evidence from multiple NHANES-based cohorts consistently demonstrates that LTPA—but not OPA—is inversely associated with MASLD risk, liver fibrosis, and mortality. For example, active LTPA (≥150 min/week) was associated with significantly lower odds of MASLD (OR 0.55, 95% CI 0.46–0.66) and advanced fibrosis, whereas OPA showed no protective effect. OPA often involves prolonged static postures or repetitive movements that do not elicit the same cardiometabolic benefits as structured recreational exercise. These findings reinforce the public health value of promoting accessible LTPA patterns, such as the weekend warrior approach, for individuals with MASLD facing work-related time constraints.
In addition, a few studies have utilized the NHANES database and demonstrated that the weekend warrior pattern is associated with a reduced risk of mortality in specific disease populations. Mahe et al. utilized NHANES 2007-2018 to show that compared to the inactive group, weekend warrior leisure time PA pattern was associated with significantly lower all-cause mortality among T2D patients (HR 0.49, 95% CI 0.26-0.91). Similarly, there was no significant difference in the risk of all-cause mortality for weekend warrior PA compared to regularly active participants (HR 0.82, 95% CI 0.42-1.61). 44 Leveraging NHANES 2007-2018, Yang et al. demonstrated that compared to the inactive group, the weekend warrior PA pattern was associated with significantly lower all-cause mortality among patients with diabetes combined with chronic kidney disease (HR 0.338, 95% CI 0.116-0.988) however was not associated with CVD mortality (HR 0.165, 95% CI 0.020-1.343). 26 Similarly, there was no significant difference in the risk of all-cause and CVD mortality for weekend warrior PA compared to regularly active participants. 26 Overall, these studies collectively demonstrated that the weekend warrior PA pattern was associated with significantly reduced mortality risk compared with the inactive population and had similar mortality reduction benefits as the regularly active population, suggesting that the weekend warrior PA pattern is a feasible means of implementing moderate or vigorous PA in the general population. Our study similarly demonstrated that weekend warrior PA was associated with significantly reduced all-cause and CVD mortality risk in the MASLD population and had similar mortality benefits as the regularly active group, emphasizing that weekend warrior PA is a viable exercise modality for patients with MASLD. In addition, the association between weekend warrior PA and all-cause mortality was only present in participants aged < 60 years, suggesting that there is a greater benefit of performing weekend warrior PA in non-elderly participants. Conversely, among those aged ≥ 60 years, the insufficiently and regularly active groups were associated with reduced all-cause mortality. These results suggest that focusing on to 1-2 exercise sessions per week to achieve the recommended amount of PA may be unsuitable for generalization due to lack of adherence in older populations with MASLD. Clinical and community practitioners can develop personalized exercise prescriptions based on patients’ specific conditions and lifestyle habits, recommending focused exercise on weekends or during free time to achieve long-term mortality risk reduction. The relative flexibility of the weekend warrior pattern can help improve patient adherence to exercise and ensure that exercise interventions can be implemented effectively over the long term. Although the point estimate for CVD mortality is notably low, multiple sensitivity analyses confirmed the robustness of the findings; future studies with larger samples are warranted to further validate this association.
Patients with MASLD may face multiple barriers to implementing PA intervention strategies. A recent survey that included 81 patients with MASLD in outpatient liver clinics showed that most patients did not achieve the guideline-recommended amount of moderate or vigorous PA and even lacked awareness of PA as an intervention strategy. 21 Time planning, physical and mental health issues, lack of enjoyment of exercise, and fatigue were the main barriers. 21 In addition, MASLD is associated with a decline in health-related quality of life. 45 Therefore, it is important to identify appropriate exercise patterns that favor a reduction in mortality risk in patients with MASLD. By elucidating the association between weekend warrior PA patterns and the risk of mortality in the MASLD population, physicians can develop personalized exercise prescriptions for patients with MASLD, thereby improving adherence to and the effectiveness of exercise therapy, better controlling disease progression, and reducing the risk of death in patients with MASLD. These findings may help physicians make timely adjustments to exercise programs during follow-up and management of patients with MASLD to ensure that patients can adhere to appropriate PA patterns over the long term to reduce the risk of death.
Our study had some noteworthy strengths. Our study included a nationally representative, population-based, multiethnic MASLD cohort from the NHANES, making the findings potentially generalizable. The large sample size and adequate adjustment for confounders reduced the potential study bias. Our study is the first to explore the impact and comparative benefits of the weekend warrior PA pattern on mortality in the MASLD population using a longitudinal cohort study. These findings reveal similar protective benefits of weekend warrior PA over conventionally scheduled PA on mortality, highlighting that this PA modality may have important public health implications as an individualized and higher adherence option for the MASLD population.
However, our study had some potential limitations. First, PA duration and pattern in the present study were assessed using self-reports and not obtained from accelerometers. Although validated questionnaires were used, self-reported PA is subject to recall and social desirability bias, which may lead to overestimation of activity levels; however, similar weekend warrior benefits have been consistently observed in both self-report and accelerometer-based studies. 26 Second, the NHANES only provided baseline data on participants’ PA, preventing us from exploring the impact of shifts in PA duration and patterns during follow-up on mortality in the MASLD population. Third, hepatic steatosis was evaluated using the Fatty Liver Index (FLI) rather than imaging or biopsy; while practical for large epidemiological studies, FLI has known limitations, particularly in lean populations. Fourth, diet quality (HEI-2015) was derived from single 24-hour dietary recalls, which are prone to measurement error and recall bias, although this approach is standard in NHANES analyses for confounder adjustment. Importantly, as this is an observational study, the observed associations do not imply causation; residual confounding or reverse causation cannot be entirely ruled out. Finally, the sample size of participants in the weekend warrior PA pattern was relatively small, and a larger sample is needed to confirm these findings.
Conclusions
In a nationwide cohort study, achieving the recommended amount of PA duration (≥150 min/week) significantly reduced all-cause and CVD mortality in participants with MASLD. Total PA frequency was associated with reduced mortality within a limited number of sessions, whereas a higher frequency had no additional benefit. Weekend warrior PA was associated with significantly lower all-cause and CVD mortality than that in the inactive group and had similar mortality benefits as those in the regularly active group. Notably, the association between weekend warrior PA and all-cause mortality was only present in those <60 years of age. These findings suggest that weekend warrior PA may serve as a viable exercise modality for mortality risk reduction in MASLD populations, especially in non-elderly individuals.
Supplemental material
Supplemental material - Weekend warrior physical activity pattern and risk of all-cause and cardiovascular mortality among US adults with metabolic dysfunction-associated steatotic liver disease: A prospective cohort study of NHANES 2007–2018
Supplemental material for Weekend warrior physical activity pattern and risk of all-cause and cardiovascular mortality among US adults with metabolic dysfunction-associated steatotic liver disease: A prospective cohort study of NHANES 2007–2018 by Mengbiao Cai, Kai Jin, YuLong Wang, Jian Zhu, Changnan Xu, Yi Yang, Zhenxiang Guo in Science Progress
Supplemental material
Supplemental material - Weekend warrior physical activity pattern and risk of all-cause and cardiovascular mortality among US adults with metabolic dysfunction-associated steatotic liver disease: A prospective cohort study of NHANES 2007–2018
Supplemental material for Weekend warrior physical activity pattern and risk of all-cause and cardiovascular mortality among US adults with metabolic dysfunction-associated steatotic liver disease: A prospective cohort study of NHANES 2007–2018 by Mengbiao Cai, Kai Jin, YuLong Wang, Jian Zhu, Changnan Xu, Yi Yang, Zhenxiang Guo in Science Progress
Footnotes
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental material
Supplemental material for this article is available online.