
Abstract
Objectives:
The Health Resources and Services Administration (HRSA) began collecting data on intimate partner violence (IPV) and human trafficking (HT) in the 2020 Uniform Data System (UDS). We examined patients affected by IPV and HT served by HRSA-funded health centers in medically underserved US communities during the COVID-19 pandemic.
Methods:
We established a baseline and measured trends in patient care by analyzing data from the 2020 (N = 28 590 897) and 2021 (N = 30 193 278) UDS. We conducted longitudinal ordinal logistic regression analyses to assess the association of care trends and organization–level and patient characteristics using proportional odds ratios (PORs) and 95% CIs.
Results:
The number of clinical visits for patients affected by IPV and HT decreased by 29.4% and 88.3%, respectively, from 2020 to 2021. Health centers serving a higher (vs lower) percentage of pediatric patients were more likely to continuously serve patients affected by IPV (POR = 2.58; 95% CI, 1.01-6.61) and HT (POR = 6.14; 95% CI, 2.06-18.29). Health centers serving (vs not serving) patients affected by IPV were associated with a higher percentage of patients who had limited English proficiency (POR = 1.77; 95% CI, 1.02-3.05) and Medicaid beneficiaries (POR = 2.88; 95% CI, 1.48-5.62), whereas health centers serving (vs not serving) patients affected by HT were associated with a higher percentage of female patients of reproductive age (POR = 15.89; 95% CI, 1.61-157.38) and urban settings (POR = 1.74; 95% CI, 1.26-2.37).
Conclusions:
The number of clinical visits for patients affected by IPV and HT during the COVID-19 pandemic declined. Delayed care will pose challenges for future health care needs of these populations.
Keywords
Intimate partner violence (IPV) is prevalent in the United States; in 2016-2017, 47.3% of women (59 million) and 44.2% of men (52 million) reported sexual violence, physical violence, and/or stalking victimization by an intimate partner during their lifetime. 1 The Centers for Disease Control and Prevention (CDC) defines IPV as abuse or aggression that occurs against a current or former romantic or intimate partner. 2 The risk factors for IPV are low socioeconomic status, low educational attainment, social isolation, mental health conditions, substance use, and adverse childhood experiences.3 -5 IPV experiences contribute to harmful health effects such as emotional trauma, injury, posttraumatic stress disorder (PTSD) symptoms, chronic health conditions, and missed work. 6
Human trafficking (HT), a form of interpersonal violence inflicted through forced labor and/or commercial sexual exploitation, is another critical US public health issue that disproportionately affects women, children and adolescents aged <18 years, racial and ethnic minority groups, migrants, individuals with limited social or economic opportunity, individuals experiencing poverty, people with substance use disorder, and other historically marginalized populations.7 -11 Globally, the number of people living in HT conditions increased from 24.9 million in 2016 to 28 million in 2021; 17.3 million people experienced forced labor in private sector industries and 6.3 million people experienced sex trafficking in 2021.12,13 In 2021, incident reports from the National Human Trafficking Hotline identified 17 460 HT victims, a decrease from 19 186 victims in 2020 and 30 684 victims in 2019; however, the total number of signals (eg, telephone calls, text messages, online chats) directly from HT victims seeking assistance increased from 10 362 in 2019 to 13 129 in 2020 and 13 538 in 2021.7,14,15 More reliable national epidemiologic surveillance of HT in the United States would improve our understanding of such data incongruences.
The US health care system’s response to IPV has evolved since the passage of the Violence Against Women Act (VAWA) in 1994 and its subsequent reauthorizations. 16 While this landmark legislation initially sought to improve criminal, legal, and community-based responses to IPV, domestic violence, dating violence, sexual assault, and stalking, the VAWA reauthorization in 2000 included prevention strategies that brought new public health and health care foci. Title V of the VAWA Reauthorization of 2013 further specified strengthening the health care system’s response. 17 In studies from 2014 to 2022, most IPV and HT survivors reported accessing health care services, but many may not have received appropriate screening and care.18 -21 In 2018, the US Preventive Services Task Force updated its IPV screening recommendation to Grade B for women of reproductive age to provide or refer women who screen positive to ongoing support services. 22
Similarly, the public policy for HT victims advanced with the initial 2000 Trafficking Victims Protection Act of 2000, which focused on criminal justice, legal, and victim service responses. 23 Subsequent reauthorizations, particularly the Trafficking Awareness Training for Health Care Act of 2015 and the Stop, Observe, Ask, and Respond (SOAR) to Health and Wellness Act of 2018, specified the development of best practices in health care system and public health responses to HT.9,24 In addition, state legislatures are increasingly passing legislation that requires HT training for health care providers. 25 These policy actions have led health care systems to respond through changes in the definition of child abuse, which now includes child sex trafficking and updated mandatory reporting protocols in compliance with federal and state laws. 26
The risk factors for IPV and HT, public health surveillance, and public policy changes are well documented in the literature. However, little is known about access to primary care and the types of health care organizations that provide services to victims and survivors of IPV and HT in medically underserved communities nationally. In the US health care delivery system, health centers funded by the Health Resources and Services Administration (HRSA) (hereinafter referred to as health centers) are the primary care safety net for medically underserved patients and communities. HRSA has funded nearly 1400 health centers that deliver affordable, accessible, high-quality, and comprehensive primary health care to more than 30 million people in the United States regardless of their ability to pay, through >14 000 clinics in every US state, territory, and the District of Columbia. 27 Health centers serve medically underserved patients confronting similar risk factors as for IPV and HT. Nearly 70% of health center patients lack health insurance or receive Medicaid, more than 60% are from racial and ethnic minority populations, and nearly 25% are patients with limited English proficiency (LEP). 28
The 2020 inaugural collection of national data on IPV and HT in HRSA’s Uniform Data System (UDS) offers the first opportunity to explore access to primary care delivery for patients affected by IPV and at risk for or affected by HT (hereinafter referred to as patients affected by HT) who are served through health centers. This initial data collection coincided with the COVID-19 pandemic, which provided the opportunity to assess the impact of the COVID-19 pandemic on patients affected by IPV and HT in medically underserved communities. Our study objectives were to (1) establish the baseline for patients affected by IPV and HT served by health centers; (2) assess changes in the number of patients served and clinical visits during the COVID-19 pandemic, from 2020 to 2021; and (3) measure the association between health center organization characteristics and continual access to primary care services for patients affected by IPV and HT.
Methods
Health Center Organization and Patient Data
HRSA’s UDS is an annual administrative reporting dataset that encompasses information on patient sociodemographic characteristics, provision of primary care services, primary care workforce, patient visits, clinical quality measures, and health information technology capabilities. UDS data contain aggregated demographic characteristics of the patient population at the health center organization level and do not contain individual patient-level data. Each year, HRSA requires health centers to report on their performance by using measures in the UDS. In 2020 and 2021, 1375 and 1373 health centers, respectively, reported in the UDS. The 2020 and 2021 UDS manuals contain guidance on the applicable International Classification of Diseases, Tenth Revision (ICD-10) codes used to identify patients affected by IPV and HT. 29 In accordance with the US Department of Health and Human Services Policy for Protection of Human Research Subjects, this study was not considered human subjects research because data from UDS were reported at the health center organizational level and did not include the collection of identifiable information about human subjects.
Statistical Analysis
We defined health centers serving patients affected by IPV and HT as health centers reporting 1 or more patients using the applicable ICD-10 codes during the UDS reporting year. For the first study objective, we assessed the number of patients served, the number of clinical visits, and the ratio of patients to clinical visits from 2020 to 2021. For the second study objective, we conducted bivariate analyses of health center organization characteristics to compare differences among health centers overall and those serving IPV and HT patients from 2020 to 2021. Health center organization characteristics included the mean percentages of patients served with respect to sex (male, female), race and ethnicity (Hispanic, non-Hispanic Black, non-Hispanic White, and non-Hispanic Other [Asian, Native Hawaiian, Pacific Islander, American Indian, and Alaska Native]), LEP, age (0-17, 18-64, ≥65 years, and women of reproductive age [15-49 years]), household federal poverty level (FPL) (≤100%, 101%-200%, >200%, unknown), type of health insurance (uninsured, Medicaid, Medicare, other third party), and geography (urban, rural). For the third objective, we conducted longitudinal ordinal logistic regression analyses to identify the health center organization characteristics that influenced changes in patient care from 2020 to 2021. Characteristics tested in the regression analyses were selected from previous literature and included pediatric patients, female patients of reproductive age, patients from racial and ethnic minority groups, patients with LEP, patients with household income ≤100% FPL, Medicaid beneficiaries, and geography.3,22,30,31 We categorized changes in patient care at health centers as follows: (1) health centers that reported patients affected by IPV and HT in both years, (2) health centers that reported patients affected by IPV and HT for the first time in 2021, (3) health centers that reported patients affected by IPV and HT in 2020 but not 2021, and (4) health centers that did not report any patients affected by IPV and HT in both years. We calculated proportional odds ratios (PORs) and 95% CIs. We considered P ≤ .05 to be significant. We performed all analyses using SAS version 9.4 (SAS Institute Inc).
Results
Overall use by health center patients increased by 5.6%, from 28 590 897 patients in 2020 to 30 193 278 patients in 2021; the number of clinical visits rose by 8.8%, from 114 209 146 in 2020 to 124 211 391 in 2021 (Table 1). The number of patients affected by IPV increased by 1.5% in 1 year, from 15 929 to 16 170. The number of health centers serving patients affected by HT decreased from 20.4% (n = 280) in 2020 to 16.5% (n = 227) in 2021, with a 40.5% decrease in the number of patients served, from 4028 to 2396. The number of clinical visits for patients affected by IPV and HT declined by 29.4% and 88.3%, respectively, from 2020 to 2021; similarly, the ratio of patients to clinical visits for those affected by IPV and HT decreased by 30.4% and 80.4%, respectively, from 2020 to 2021.
Trends in intimate partner violence (IPV) and human trafficking (HT) patients served and clinical visits reported by health centers, United States, 2020-2021 a
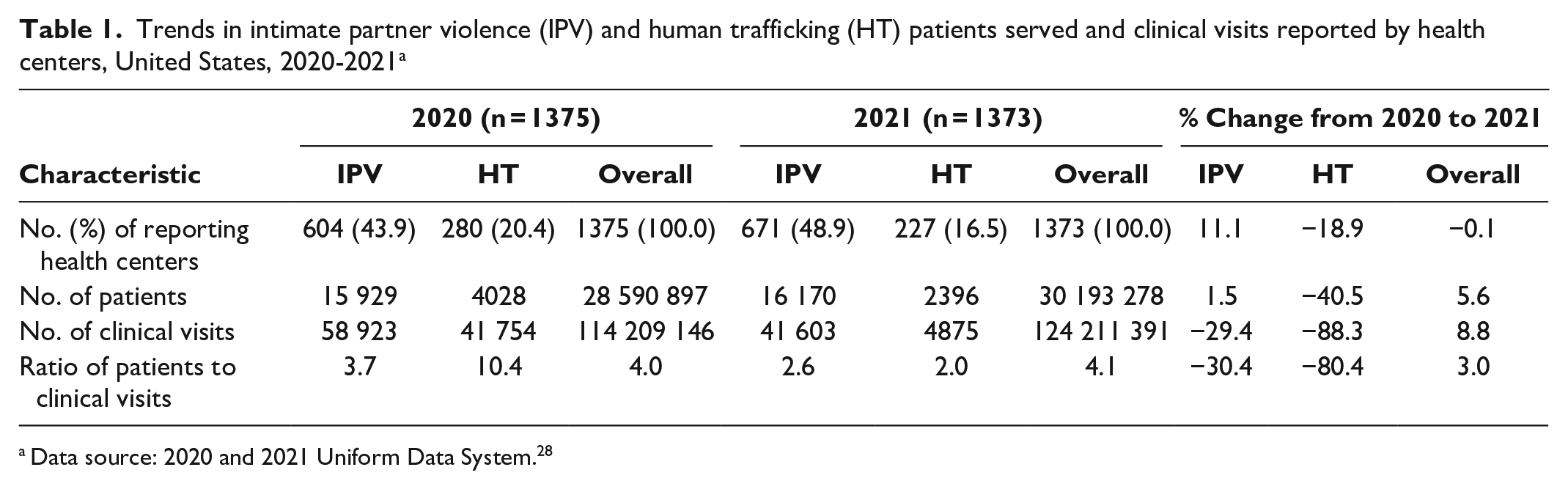
Data source: 2020 and 2021 Uniform Data System. 28
Health centers that reported serving patients affected by IPV had a mean of 31.8% of Hispanic patients in 2020 and 33.5% in 2021 as compared with a mean of 28.5% across all health centers in 2020 (Table 2). In addition, the mean percentage of patients with LEP was 22.4% in 2020 and increased to 23.6% in 2021; across all health centers, 19.7% of patients with LEP at baseline. The percentage of Medicaid beneficiaries was 44.5% in 2020 and 46.5% in 2021; across all health centers, the percentage of Medicaid beneficiaries was 42.1%. The percentage of health centers serving patients affected with IPV in urban settings was 63.7% in 2020 and 65.5% in 2021, in comparison with the overall mean percentage of 58.0% across all health centers at baseline.
Organization and patient characteristics of health centers that reported serving patients affected by intimate partner violence (IPV) and human trafficking (HT), United States, 2020-2021 a

Abbreviation: FPL, federal poverty level.
Data source: 2021 and 2021 Uniform Data System. 28
Using the Student t test. P value is the 2-tailed probability computed using t distribution, with P ≤ .05 considered significant.
Using the Pearson χ2 test, with P ≤ .05 considered significant.
Non-Hispanic Other included Asian, Native Hawaiian, Pacific Islander, American Indian, and Alaska Native.
Among health centers serving patients affected by HT, the mean percentage of Hispanic patients was 34.3% in 2020 and 36.8% in 2021 (Table 2). In addition, the mean percentage of patients with LEP increased from 23.9% in 2020 and to 25.6% in 2021. The mean percentage of Medicaid beneficiaries rose from 44.3% in 2020 to 47.2% in 2021. Finally, increases in the mean percentage of health centers located in urban settings increased from 68.9% in 2020 to 73.3% in 2021.
Health centers with a larger percentage of pediatric patients (vs a lower percentage of pediatric patients) had more than 2 times higher odds (POR = 2.58; 95% CI, 1.01-6.61) of continuously serving patients affected by IPV in 2020 and 2021 (Table 3). Health centers serving a larger percentage of patients with Medicaid (vs a lower percentage of patients with Medicaid) (POR = 2.88; 95% CI, 1.48-5.62) and patients with LEP (vs a lower percentage of patients with LEP) (POR = 1.77; 95% CI, 1.02-3.05) had higher odds of serving patients affected by IPV continuously during the first 2 years of the pandemic (2020-2021). We found no significant differences in the percentage of female patients of reproductive age, patients from racial and ethnic minority groups, patients with low income, and geography.
Ordinal logistic regression analysis of health centers serving patients affected by intimate partner violence (IPV) and human trafficking (HT), United States, 2020-2021 a
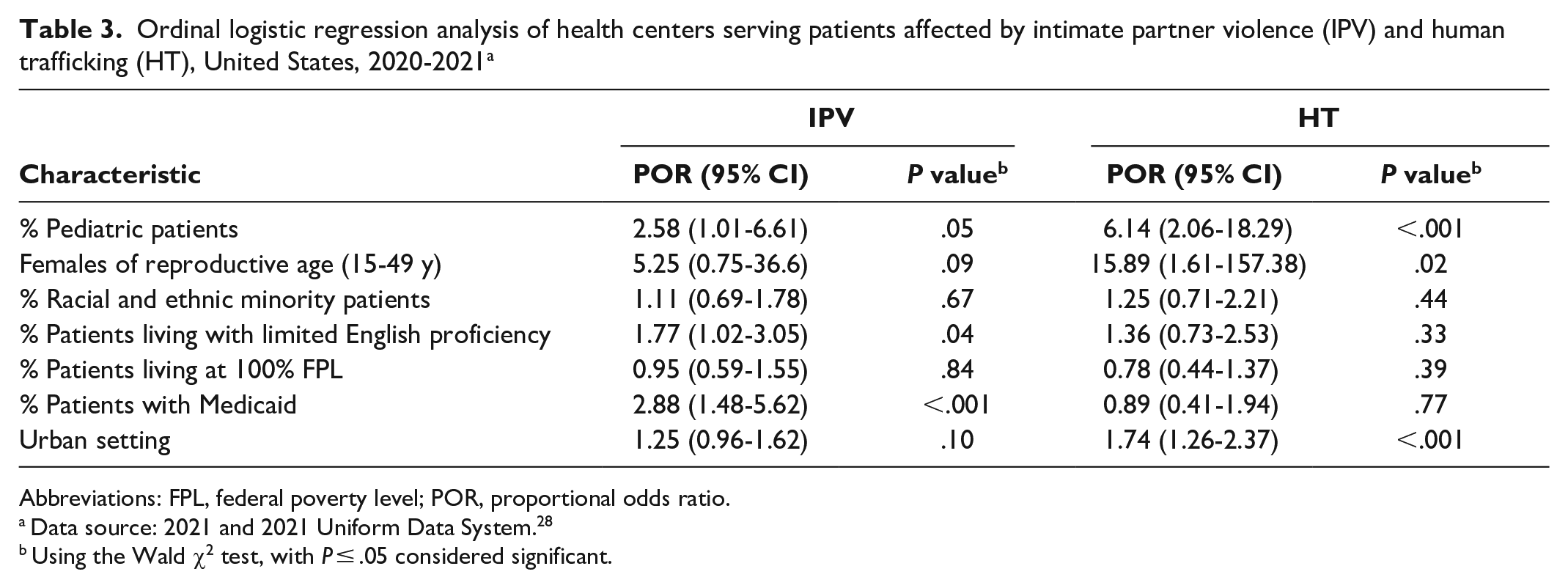
Abbreviations: FPL, federal poverty level; POR, proportional odds ratio.
Data source: 2021 and 2021 Uniform Data System. 28
Using the Wald χ2 test, with P ≤ .05 considered significant.
For health centers serving patients affected by HT, those with a larger proportion of pediatric patients had more than 6 times the odds (POR = 6.14; 95% CI, 2.06-18.29) and nearly 16 times higher odds for health centers serving a greater proportion of female patients of reproductive age (POR = 15.89; 95% CI, 1.61-157.38) throughout the pandemic (Table 3). Finally, health centers located in urban settings had higher odds of continuously serving patients at risk for or affected by HT from 2020 to 2021 (POR = 1.74; 95% CI, 1.26-2.37). We observed no significant differences in percentages of patients from racial and ethnic minority groups, with LEP, low income, and Medicaid.
Discussion
Our study identified a lower prevalence of patients affected by IPV in the health center patient population than nationally in both 2020 and 2021 UDS data.2,31 Challenges in clinical documentation using ICD-10 codes at the patient level could be attributed to barriers with disclosure-based screening, such as shame, judgment, stigma, fear (eg, of immigration, police, child welfare involvement); normalization of violence and limited legal knowledge about the rights of victims, labor, and immigration; lack of trust with the treating health care provider; and language barriers and illiteracy.32,33 Patients who were previously marginalized and harmed by systems including health care may be particularly hesitant to disclose their experiences with IPV or HT.34 -36 The low patient numbers reported in the UDS may also suggest a lack of support and utility in implementing patient universal education (ie, health care provider discussion with patients about healthy and unhealthy relationships and the health effects of violence). Such education could provide an opportunity for patients to make the connection among violence, health problems, and risk behaviors, regardless of disclosure of experiences with IPV and/or HT during the screening process. Finally, with the rapid shift to telehealth during the pandemic, challenges related to privacy and safety of disclosure at home and receipt of primary care may have further exacerbated access to care.37,38
At the health care provider level, familiarity with new ICD-10 diagnosis codes for HT may be limited because they were formally unveiled for use in 2019. 39 Moreover, health center providers may choose not to document experiences with IPV and HT in patients’ medical records because of concerns about patient privacy, confidentiality, or safety. Furthermore, coding for suspected HT depends upon health care provider training, clinical operational protocols, availability of resources for referral and follow-up, and clinicians’ comfort levels with the security, privacy, and confidentiality issues pertaining to electronic health record (EHR) documentation.40,41 Providing health care workforce training for health centers’ primary care teams, enabling service staff (ie, case managers, outreach specialists, community health workers), and front desk personnel in patient-centered, culturally sensitive, and trauma-informed approaches would enable early identification of IPV and HT and appropriate referrals to follow-up services.42,43 In addition, developing innovations in EHR documentation to ensure patient confidentiality and data security and finding new ways to foster effective EHR communication among health care professionals without causing potential harm to the patient would further support patient-centered care.
The substantial declines in the number of clinical visits among patients affected by IPV and HT from medically underserved communities from 2020 to 2021 compared with increases in the number of such visits among patients served across all health centers are concerning. While the decrease in patient visits aligned with delayed or forgone care observed during the COVID-19 pandemic in 2020, the downward trend in clinical visits observed in 2021 suggests that patients affected by IPV and HT did not return to seek primary care. This trend during the COVID-19 pandemic may have resulted from the lockdown and quarantine public health emergency measures that increased the risk of experiencing violence among women and children because of additional time in close proximity with abusers or exploiters, social isolation, and employment and financial insecurities.44 -47 Potential unmet health care needs from delayed care will pose substantial challenges at the patient and health care system level in the future.48,49
Results from the regression analyses found that health centers with a larger (vs smaller) proportion of pediatric patients were more likely to continuously serve patients affected by IPV and HT, which suggests potential clinical observations and heightened awareness of disproportionate risk for children among clinicians and primary care teams. Furthermore, the association of a higher (vs lower) percentage of patients with LEP and Medicaid among health centers that continuously serve patients affected by IPV and the association of a greater proportion of female patients of reproductive age and urban settings among health centers that serve patients affected by HT suggest key factors that health centers should consider in service delivery. Patients affected by IPV and HT are disproportionately affected by social determinants of health and have needs that require holistic patient care and linkages to community-based organizations with victim service programs, effective engagement with medical–legal partnerships, and integrated behavioral health to support patient needs.42,50,51 Because IPV and HT disproportionately affect women, children, people in racial and ethnic minority groups, and people with low socioeconomic status or foreign-born status, health centers may continue to be critical primary care access points for people at risk of and experiencing IPV and HT.44,52,53 Thus, future research on patient use trends, effects of delayed care, and innovative approaches to safe EHR documentation to ensure patient confidentiality are warranted.
Limitations
This study had several limitations. First, the implementation of new IPV and HT UDS data reporting took place in 2020 at the start of the COVID-19 pandemic, with severe disruption to health care delivery. Second, the lag for implementation and operationalization of clinical workflow processes to meet UDS reporting guidelines, including additional time to update EHR systems, may have affected documentation and reporting. Third, the use of ICD-10 codes as a proxy to capture patients’ experience of IPV or HT required relying on an appropriate screening framework for IPV and HT, which continues to emerge in clinical practice. 54 Finally, dependence on patient disclosures of experiences of IPV or HT or a health care provider’s suspicion of HT may result in underreporting and may not measure the true status of patients affected by IPV and HT in primary care service delivery.
Conclusion
To our knowledge, this is the first national study on patients affected by IPV and HT in medically underserved communities and the association between health center organization characteristics and continual access to primary care services for these patients. We observed underreporting of the prevalence of patients affected by IPV and HT in these communities, which suggested the limitations of disclosure-based identification of patients experiencing IPV or HT and highlighted the potential constraints of medical coding in reporting patient care. Substantial declines in clinical visits among patients experiencing IPV and HT differed from the increasing trend in overall patients served from 2020 to 2021 across health centers. Delayed care will pose challenges for the future health care needs of these populations. We found health centers that served larger (vs smaller) pediatric patient populations were associated with continually providing services to patients affected by IPV and HT. Future examinations of patient use trends and various approaches in health care workforce training, implementation of universal education in clinical settings, and innovations in secure and confidential EHR documentation are recommended to enhance patient-centered, culturally sensitive, and trauma-informed care for patients affected by IPV and HT served by health centers.
Footnotes
Disclaimer
The views expressed in this article are solely the opinions of the authors and do not necessarily reflect the official policies of the US Department of Health and Human Services, the Health Resources and Services Administration, or the Administration for Children and Families, nor does mention of the department or agency names imply endorsement by the US government.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.