
Abstract
Objective:
Human trafficking is a public health issue affecting young people across the United States, and trafficked young people frequently present to emergency departments (EDs). The identification of trafficked young people by pediatric EDs during the COVID-19 pandemic is not well understood. We examined trends in the identification of young people with current or lifetime experiences of trafficking in US pediatric EDs before and during the COVID-19 pandemic.
Methods:
We performed an interrupted time-series analysis using the Pediatric Health Information System database, which includes data from 49 US children’s hospitals, to determine differences in rates of trafficked young people identified in pediatric EDs before and during the COVID-19 pandemic.
Results:
We included 910 patients; 255 prepandemic (October 1, 2018, through February 29, 2020) and 655 during the COVID-19 pandemic (March 1, 2020, through February 28, 2023). We found a 1.92-fold increase in the incidence rate of identified trafficked young people at the start of the COVID-19 pandemic in March 2020 (incidence rate ratio = 1.92; 95% CI, 1.47-2.51; P < .001), followed by a decrease over time.
Conclusions:
The observed increase in identified trafficked young people during the onset of the COVID-19 pandemic should alert pediatric ED providers to the opportunity to identify and provide services for trafficked young people as an important part of improving preparedness for future disease outbreaks. Our observed identification trends do not represent the true incidence of trafficked young people presenting to pediatric EDs during the COVID-19 pandemic. Future work should seek to better understand the true occurrence and the health and service needs of trafficked young people during emergencies.
Human trafficking is a pervasive public health issue that affects young people across the United States.1,2 Human trafficking is broadly defined as compelling a person to engage in a sex or labor act through means of force, fraud, or coercion.3,4 Human trafficking affects an estimated 50 million people globally. 5 While the true prevalence and scope of human trafficking in the United States is not known, trafficking of young people occurs in all 50 states, and children and adolescents aged <18 years account for almost 30% of reported cases in the United States.5 -7 Young people are affected by both sex and labor trafficking and experience a wide range of associated medical problems, including physical and psychological trauma, infections, and exacerbations of chronic diseases.8,9 Studies indicate that nearly 90% of survivors have used health care services while trafficked.10,11 Although people experiencing exploitation may present to any part of the health care system, 60% to 95% present to emergency departments (EDs).10,12,13 Emergency medicine practitioners therefore play an important role in identifying and providing resources to exploited young people.
Prior global disease outbreaks, such as the Ebola outbreak in 2014, were associated with an increased risk of human trafficking. 14 Worsnop suggested that this increased risk in trafficking resulted from economic, criminal, and sociocultural factors as well as a shift in the use of health care and social services. 14 Antitrafficking experts predicted a particularly substantial increase in human trafficking during the COVID-19 pandemic because of exacerbations of job, food, and housing insecurity, all of which contribute to the vulnerability of exploitation.15,16 Additional concerns of experts included the potential for COVID-19–related policies of social distancing, closures of services, and increased patient volumes at EDs to reduce identification of trafficked people, despite this predicted true increase in the incidence of trafficking. 17
Evidence since the start of the COVID-19 pandemic indicates that human trafficking increased in certain sectors. The National Human Trafficking Hotline found that reports of labor trafficking among agricultural workers increased by 70% in the first 6 months of the COVID-19 pandemic. 18 Separately, reporting of online child sexual exploitation to the National Center for Missing and Exploited Children doubled in 2020. 19 This increase is consistent with reports from the National Human Trafficking Hotline showing a more than 45% increase in reports of online sexual exploitation. 20 It is unclear if this increase represented a true increase in trafficking or a shift to virtual forms of child trafficking. While many forms of online child sexual exploitation overlap with human trafficking and are included in typologies of modern slavery, online child exploitation that does not involve commercial exploitation or monetary gain is not defined as trafficking.5,21,22
Trafficked people presenting to the health care system during the COVID-19 pandemic, however, have not been well-studied, and no studies exploring the identification of trafficked young people in pediatric EDs have been published for this period. Improving our understanding of associations between trafficked young people and presentation to EDs during the COVID-19 pandemic will improve the ability to support this population both in the immediate aftermath of the COVID-19 pandemic and in preparation for responding to future health emergencies. The objective of this study was to examine trends in the identification of trafficked young people in US pediatric EDs before and during the COVID-19 pandemic.
Methods
We performed an interrupted time-series analysis using data from the Pediatric Health Information System (PHIS) database, which contains pediatric hospital data from 49 children’s hospitals across the United States. 23 PHIS hospitals are the largest and most advanced children’s hospitals in the United States and have the most demanding standards of pediatric service in the United States. 23 We followed the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) reporting guidelines for cohort studies. 24
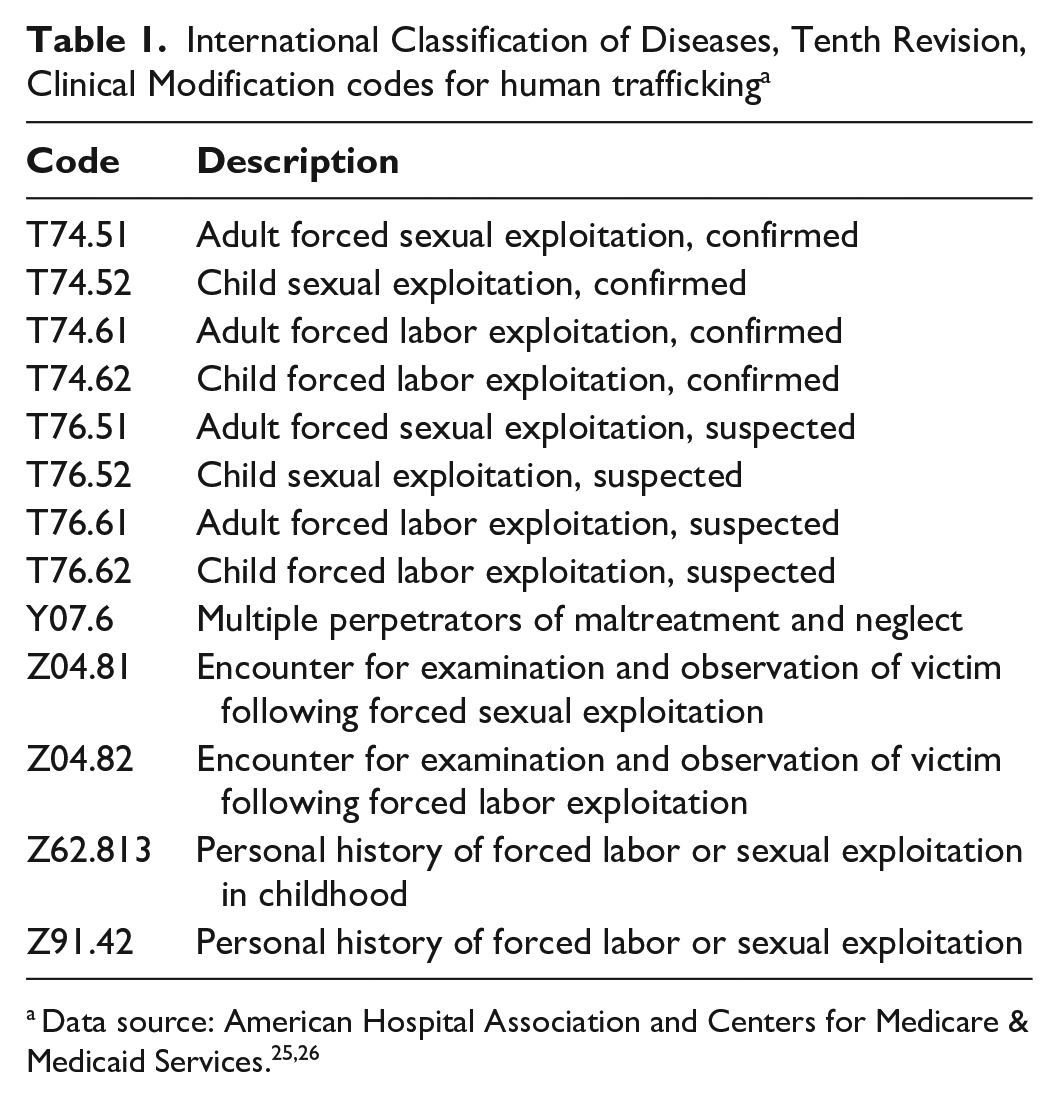
We included young people aged ≤24 years who presented for an ED visit and had an International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) diagnosis for human trafficking, inclusive of labor and sex trafficking (Table 1).25,26 The rationale for the age criteria was based on commonly used standards in the fields of pediatric and adolescent medicine, as young adults aged >18 years are frequently seen in pediatric EDs. We therefore used the United Nations definition of young people, which specifies an upper age limit of 24 years. 27 Because the experiences of individuals who endure human trafficking vary, acknowledging that each person has a different path to survivorship, with some individuals experiencing reexploitation, we included ICD-10-CM codes corresponding to individuals who were currently experiencing trafficking and individuals who had histories of being trafficked.28,29 Therefore, for the purposes of this analysis, we defined “identified trafficked young people” as individuals who had experienced trafficking in their lifetime. Because the ICD-10-CM codes for human trafficking were first introduced in 2018, we defined the prepandemic period to include patient data from January 1, 2018, through February 29, 2020. We defined the pandemic period to include patient data from March 1, 2020, through February 28, 2023.
International Classification of Diseases, Tenth Revision, Clinical Modification codes for human trafficking a
The primary outcome of the interrupted time-series analysis was the number of trafficked young people identified per month. We performed a Poisson regression; we chose a level- and slope-change impact model to best fit the data as follows:

E[Y] represents our primary outcome, the number of identified trafficked young people per month. T is the time elapsed from the start of the study in months, and X is the intervention variable denoting the prepandemic or pandemic period. As the total volume of young people presenting to EDs was expected to be affected by both seasonal variation and the COVID-19 pandemic, the total number of young people presenting for ED visits per month (N) was used as an offset variable in the model to provide the rate of identified trafficked young people adjusted for the total number of young people presenting to EDs. 30
The descriptive analysis included calculating the average number of trafficked young people identified per month and the average rate of trafficked young people identified per month before and during the COVID-19 pandemic. We collected demographic data, including age, sex, US Census region, and rural or urban area, to describe the cohort. We collected data on race and ethnicity to explore differences in the identification of trafficked young people who are from racial and ethnic minority populations after the start of the COVID-19 pandemic.31,32 Race and ethnicity data captured by the PHIS database are based on the collection of this patient information by each participating hospital in their respective registration and billing systems. Reporting of race and ethnicity was therefore limited by categorization in the PHIS database, which included race categories of Asian, Black, Native American, Pacific Islander, and White, and ethnic categories of Hispanic or Latinx and not-Hispanic or Latinx. Sex was limited to male or female categories, as the database currently does not have available information on gender minority groups. We performed Pearson χ2 tests for binary or categorical outcomes, Fisher exact tests for binary or categorical outcomes with sparse data, and Wilcoxon rank-sum tests for continuous outcomes, to assess for differences in the demographic makeup of identified trafficked young people before and during the pandemic.
This study was not considered human subjects research as the methods consisted of a secondary analysis of deidentified data (institutional review board [IRB] #64341, Stanford University IRB).
Results
We identified 1024 patients with an ICD-10-CM diagnosis of human trafficking; 108 patients did not have an ED encounter, and 6 patients were aged >24 years. A total of 910 patients met the study inclusion criteria. While we prespecified the inclusion criteria for the prepandemic period from January 1, 2018, through February 29, 2020, the first patient in the PHIS database with a trafficking-related ICD-10-CM code was seen in October 2018. We therefore identified 255 patients in the prepandemic period (October 1, 2018, through February 29, 2020) and 655 patients in the pandemic period (March 1, 2020, through February 28, 2023).
The median (IQR) age for the overall cohort was 15 (13-16) years. Of 910 patients, most (n = 785; 86.3%) were female (Table 2). By race and ethnicity, 413 (45.4%) identified as White, 380 (41.8%) as Black, and 155 (17.0%) as Hispanic or Latinx. Most patients were from the southern region of the United States (n = 495; 54.4%). The majority of the cohort (n = 836; 91.9%) was from urban areas. We found no significant differences in the makeup of the prepandemic and pandemic period cohorts across all demographic categories, including by race and ethnicity.
Characteristics of identified trafficked young people aged 0 to 24 years presenting to pediatric emergency departments before and during the COVID-19 pandemic, United States, October 1, 2018, through February 28, 2023
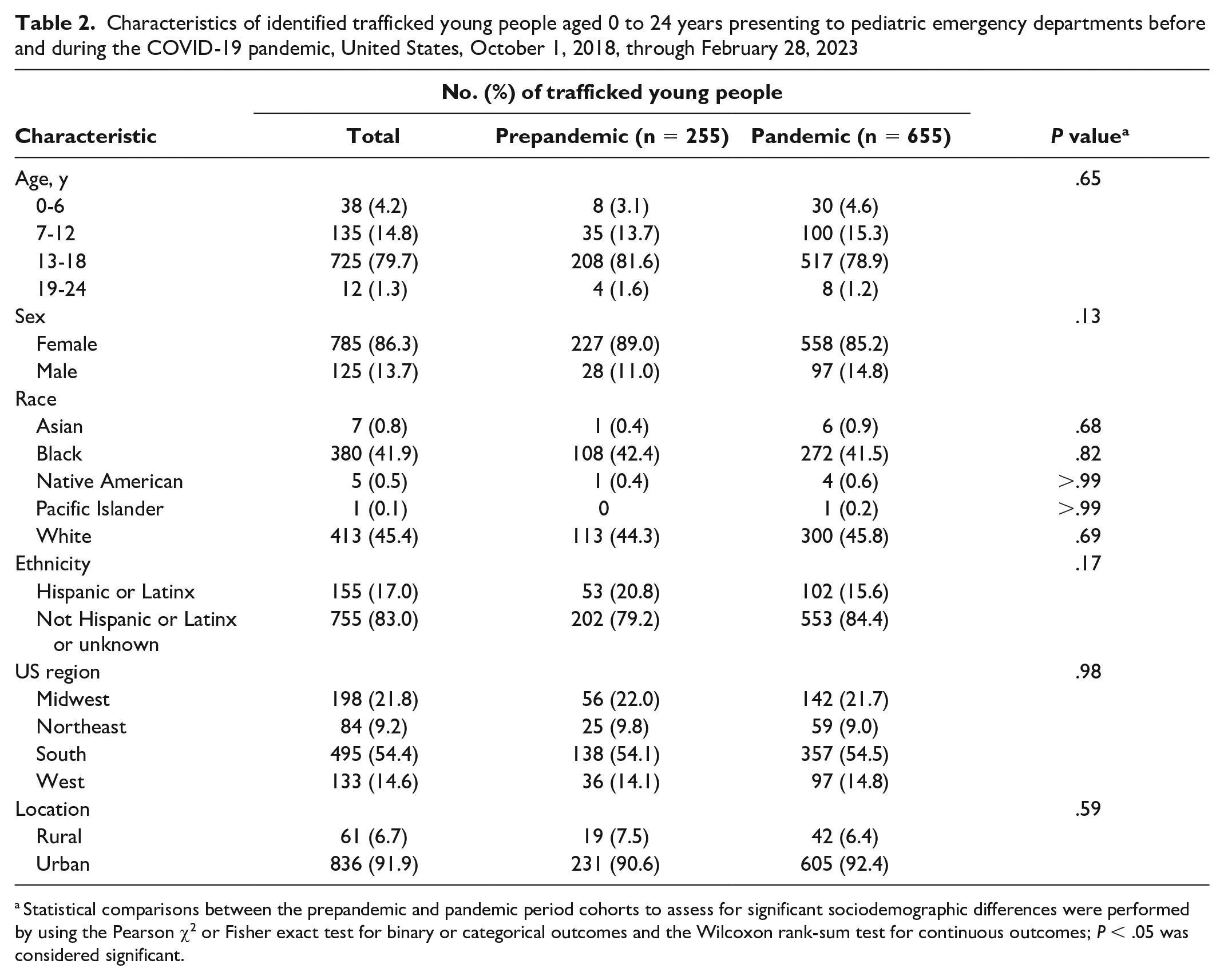
Statistical comparisons between the prepandemic and pandemic period cohorts to assess for significant sociodemographic differences were performed by using the Pearson χ2 or Fisher exact test for binary or categorical outcomes and the Wilcoxon rank-sum test for continuous outcomes; P < .05 was considered significant.
The interrupted time-series analysis demonstrated an initial increase in the rate of identified trafficked young people immediately after the start of the pandemic, followed by a gradual decrease (Figure). The corresponding regression analysis found that the onset of the COVID-19 pandemic, at the beginning of March 2020, was associated with an immediate 1.92-fold increase in the incidence rate of identified trafficked young people (incidence rate ratio [IRR] = 1.92; 95% CI, 1.47-2.51; P < .001). Before the onset of the COVID-19 pandemic, the model demonstrated a slight secular trend such that more trafficked young people were identified over time (IRR = 1.03; 95% CI, 1.00-1.06; P = .02); after the onset of the COVID-19 pandemic, this secular trend changed direction such that fewer trafficked young people were identified over time, trending down toward prepandemic values (IRR = 0.95; 95% CI, 0.92-0.97; P < .001).

Interrupted time-series analysis comparing the rate of trafficked young people aged ≤24 years identified in pediatric emergency departments (EDs) before and after the COVID-19 pandemic, United States, October 1, 2018, through February 28, 2023. The rate of identified trafficked young people per month was adjusted by the total number of young people presenting to EDs for each corresponding month. The black vertical dashed line indicates the onset of the COVID-19 pandemic in March 2020. The solid line is the interrupted time-series analysis representing observed trends. The horizontal dashed line is a counterfactual line removing the effect of the COVID-19 pandemic, which reflects the predicted trend of rate of identification if the COVID-19 pandemic had not occurred.
The average number of identified trafficked young people per month was 15.0 before the COVID-19 pandemic and 18.2 during the COVID-19 pandemic. The average rate of trafficked young people identified per month was 5.2 per 100 000 young people prepandemic and 8.6 per 100 000 young people during the COVID-19 pandemic.
Discussion
This study identified a significant nearly 2-fold increase in the rate of identified trafficked young people presenting to pediatric EDs immediately after the start of the COVID-19 pandemic, followed by a slight decrease over time. The initial observed surge may reflect a true increase in trafficking of young people, an increase in the use of ED care by trafficked young people, or changes in the clinical environment that allowed for increased opportunities for trust building. The secular trend showing a decrease in identification of trafficked young people over time from the onset of the COVID-19 pandemic may be attributed to the relaxing of COVID-19 shelter-in-place and social distancing policies. Although we found no significant differences in the racial and ethnic makeup of identified young people after the start of the COVID-19 pandemic, further work is needed to understand how systems of structural discrimination affected trafficked young people during the COVID-19 pandemic. Our results may reflect increased presentation to EDs because of limited availability of other medical and community support services due to shelter-in-place, social distancing, and capacity restrictions.
Although our observed increase in identified trafficked young people is consistent with sentiments from antitrafficking experts that human trafficking may have increased after the start of the COVID-19 pandemic,16,17 our results represent identification of young people with histories of trafficking but do not represent the true incidence of trafficked young people presenting to pediatric EDs during the COVID-19 pandemic. The rise we observed could be attributed to socioeconomic stressors during the COVID-19 pandemic that caused young people to become increasingly vulnerable to exploitation. Financial shocks for families, including unemployment and increased homelessness, may have placed young people at increased risk of trafficking. 16 Reports of intimate partner violence and child maltreatment rose at the start of the COVID-19 pandemic; both are known factors that contribute to the risks of exploitation of young people. 33 Human trafficking can also contribute to the risk of experiencing other forms of violence, and experiences of various forms of violence overlap in root causes and serve as risk factors for experiencing future violence. 34 Multiple organizations documented an increase in the online sexual exploitation of young people, which was hypothesized to be exacerbated by COVID-19 pandemic–related school closures that contributed to young people spending more time online, although the causal mechanisms have not been explicitly studied.19,20 While noncommercial online exploitation is not considered trafficking, overall trends in child exploitation are important to note to contextualize findings from this study.
Some primary care offices during the COVID-19 pandemic had a limited number of appointments. This decreased accessibility of outpatient medical care may have caused more young people experiencing trafficking to present to EDs. Furthermore, existing situations of trafficking young people may have become more extreme because of pandemic-related socioeconomic stressors, causing health problems in this population to worsen and require emergent medical care. Worsening trafficking situations were documented in a 2021 report by the Polaris Project among exploited agricultural workers in the United States, who experienced an increase in elements of force, fraud, and coercion during the COVID-19 pandemic. 18 Of note, this report on agricultural workers experiencing exploitation did not provide age ranges and may not be generalizable to young people. COVID-19 lockdown policies, social distancing mandates, limits on indoor capacity, and closures of businesses may have restricted the ability of antitrafficking agencies to provide services to trafficked young people. The ED, which is already a well-known safety net for populations that are vulnerable to violence and exploitation, may have therefore been one of the only places trafficked young people could turn to for support.
Changes in the clinical setting during the COVID-19 pandemic may have created an environment more conducive to disclosure of trafficking than the clinical environment before the COVID-19 pandemic. While disclosure of trafficking is not the primary goal of a clinical encounter to support patients experiencing exploitation, exploring risk factors of experiencing trafficking and providing appropriate resources require privacy and enough time to build rapport with the patient. 35 The reduction of visitors during the COVID-19 pandemic may have created opportunities for increased privacy. Decreased overall ED volumes in the early months of the COVID-19 pandemic could have facilitated increased time with patients and improved opportunities to build trust. In addition to these aforementioned changes to the clinical context, changes in mental and behavioral health needs may have contributed to the observed trends. Mental health consequences of human trafficking are well-studied and documented; exacerbations of mental and behavioral health needs during the COVID-19 pandemic may also have resulted in increased ED presentation.36,37 In addition, young people with a history of human trafficking could have presented to EDs for mental health issues related to the psychological impacts of the COVID-19 pandemic. For example, a preliminary report on the effects of the COVID-19 pandemic on people with a history of trafficking found that 73% of survivors from the United States felt their mental health worsened as a result of the COVID-19 panemic. 38 Further research is warranted to examine changes in the prevalence of ED visits for mental health needs during the COVID-19 pandemic among trafficked young people.
The results of our analysis may also reflect increased awareness of either human trafficking and/or trafficking-related ICD-10-CM codes. Health care providers may have become increasingly aware of the ICD-10-CM codes over time since their initial implementation in 2018. As human trafficking education for health care providers becomes more prevalent, the observed increase in identification may also be attributed to improved health care provider knowledge of trafficking of young people and coding as such. 39 Limited literature is available on trends in health care provider use after the initiation of similar ICD-10-CM codes.
The observed decrease in identification of trafficked young people after the initial surge may be explained by the end to shelter-in-place policies, the reopening of businesses and schools, and changes to the clinical environment. The slow return to reopening of businesses after the start of the COVID-19 pandemic and the availability of financial support initiatives for families through government programs may have mitigated the risks of exploitation over time. The direct effects of shelter-in-place policies and business closings on exploitation of young people and access to services should be further studied to help develop strategies to mitigate trafficking of young people during future disease outbreaks. Changes to the clinical environment later in the pandemic may also account for this observed decrease in identified trafficked young people, including increases in patient volumes that could lead to less time spent with patients and relaxing of no-visitor policies that could reduce opportunities for sufficient patient privacy.
Evidence suggests that human trafficking disproportionately affects racial and ethnic minority populations and that exploitation has a deep history in systems of structural racism and oppression.15,40 Furthermore, the COVID-19 pandemic has exacerbated health disparities and inequitably affected individuals who identify as racial and ethnic minority groups.41,42 Although we found no significant differences in the racial and ethnic makeup of young people experiencing trafficking who were identified before compared with during the COVID-19 pandemic, disproportionate effects on trafficked young people from racial and ethnic minority groups may have occurred that our analysis was unable to identify. Furthermore, these observed results may be attributed to poor access to care or inadequate identification of these populations by health care providers. Further work is needed to explore any disproportionate effects of the COVID-19 pandemic on the health of trafficked young people who identify as racial and ethnic minority groups.
Limitations
This study had some limitations. First, this study aimed to identify trends, and, as such, causality could not be determined. Second, the results do not reflect the true rate of trafficking and were limited to rates of health care provider identification and documentation of trafficking of young people. Third, our results likely underestimated the actual number of trafficked young people presenting to pediatric EDs, as many trafficked young people who present for health care are not identified because of barriers to disclosure or lack of health care provider recognition. ICD-10-CM codes are likely underused because of a lack of awareness among health care providers and concerns about confidentiality and patient safety if ICD-10-CM codes were to be viewed by a patient’s trafficker.43 -45 Fourth, the PHIS database only measures data from 49 children’s hospitals and therefore does not capture data on young people who present to other pediatric EDs or young people who present to adult and community setting EDs. Fifth, this analysis did not explore how clinicians and health systems responded to the identified young people and how support and resources were provided. This topic was beyond the scope and objective of this study but would be important to explore in the future to evaluate and improve the public health response to trafficking of young people in pandemic and disaster situations. Sixth, this study examined both young people who were currently experiencing trafficking and those with histories of trafficking, which we felt was relevant given the risks of reexploitation. Future studies looking to better isolate the incidence of trafficked young people presenting to EDs may consider focusing on individuals currently experiencing trafficking.
Conclusions
Our identification of these trends is an important step in understanding how health systems can play a role in providing support services to populations that are vulnerable to trafficking in the aftermath of the COVID-19 pandemic. This study also highlights the importance of considering the needs of young people experiencing trafficking when planning preparedness for future disease outbreaks or other emergency situations when these populations are particularly vulnerable. Further work should examine the perspectives of trafficked young people to understand how the pandemic and its aftermath have affected them and what types of interventions and resources would have been most useful then and during any future public health emergencies.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Stanford Maternal and Child Health Research Institute Clinical Trainee Support Program, the Society for Academic Emergency Medicine Foundation grant no. AG2020-0000000133, and the following National Institutes of Health grants: 1T32HD105176-01A1, R01 LM013866, UL1TR003142, P30CA124435, and P30DK116074.