
Abstract
Objectives:
Public health emergencies can elevate the risk for intimate partner violence (IPV). Our objectives were 2-fold: first, to assess the prevalence of physical IPV and increased aggression from a husband or partner that occurred during pregnancy and was perceived to be due to the COVID-19 pandemic; second, to examine associations between these experiences and (1) COVID-19–related stressors and (2) postpartum outcomes.
Methods:
We used data from the Pregnancy Risk Assessment Monitoring System that were collected in 29 US jurisdictions among individuals with a live birth in 2020. We estimated the prevalence of violence during pregnancy by demographic characteristics and COVID-19–related stressors. We calculated adjusted prevalence ratios (APRs) to examine associations of physical IPV or increased aggression with COVID-19–related stressors, postpartum outcomes, and infant birth outcomes.
Results:
Among 14 154 respondents, 1.6% reported physical IPV during pregnancy, and 3.1% reported increased aggression by a husband or partner due to the COVID-19 pandemic. Respondents experiencing any economic, housing, or childcare COVID-19–related stressors reported approximately twice the prevalence of both types of violence as compared with those without COVID-19–related stressors. Physical IPV and increased aggression were associated with a higher prevalence of postpartum depressive symptoms (APRs, 1.73 and 2.28, respectively) and postpartum cigarette smoking (APRs, 1.74 and 2.19). Physical IPV was associated with a lower prevalence of attending postpartum care visits (APR, 1.84).
Conclusions:
Our findings support the need for ongoing efforts to prevent IPV during pregnancy and to ensure the availability of resources during public health emergencies.
Intimate partner violence (IPV) during pregnancy, including physical, sexual, and psychological violence, is a public health problem that can have cascading detrimental effects on the health of IPV survivors and their infants.1,2 The consequences can be severe. Trauma resulting from physical violence during pregnancy can cause obstetric complications and injury or death to the pregnant individual, infant, or both.3 -5 In addition, experiencing emotional, sexual, or physical violence during pregnancy has been associated with substance use, depression, anxiety, and other mental health issues that can have lifelong effects on health.3,6,7
Public health emergencies such as the COVID-19 pandemic elevate the risk for IPV and create unique challenges for those who are pregnant and postpartum. 8 While social distancing and other mitigation measures may be necessary during a public health emergency, some strategies may have unintended negative consequences. 9 For example, early response measures to the COVID-19 pandemic, such as stay-at-home orders, were associated with increases in IPV.9,10
Likewise, social stressors induced by the COVID-19 pandemic (economic, housing, and food insecurity) have been associated with increases in interpersonal violence. 9 A systematic review of 15 studies published in 2020 examined the social consequences of mass quarantine for 6 worldwide outbreaks, including COVID-19, and identified psychological distress, food insecurity, economic challenges, and gender-based violence among the negative consequences of quarantines. 11 A systematic review of 18 studies specific to the COVID-19 pandemic found an increase in reports of domestic violence in response to stay-at-home or lockdown orders, 10 and a review of 24 studies revealed that key factors contributing to increases in IPV during the pandemic were low socioeconomic status, unemployment, overcrowding, family mental illness, and personal or familial COVID-19 diagnosis. 9 Several studies identified pregnant women among the groups at elevated risk for IPV and certain types of insecurity, including housing insecurity, during the pandemic.12,13
While emerging literature has examined the effect of COVID-19 quarantine measures and COVID-19–related stressors on IPV, few studies have examined the COVID-19–related stressors around the time of pregnancy and their effect on postpartum outcomes. We examined experiences of IPV among individuals who gave birth to a live-born infant in the latter part of 2020 in 29 states and jurisdictions in the United States. Our objectives were to (1) estimate the prevalence of physical IPV during pregnancy and increases in physical, sexual, or emotional aggression by a husband or partner due to the COVID-19 pandemic; (2) examine the association between physical IPV and increased aggression, separately, and COVID-19–related stressors; and (3) examine associations between physical IPV and increased aggression, separately, and postpartum health conditions, behaviors, and infant health outcomes.
Methods
We analyzed 2020 data from the Pregnancy Risk Assessment Monitoring System (PRAMS). 14 We included data from 29 PRAMS jurisdictions that implemented a questionnaire supplement on COVID-19 experiences at the end of the regular PRAMS surveys for individuals who gave birth to a live-born infant primarily from June through December 2020 (70 respondents [<1%] in Puerto Rico had births between April 1 and May 31). Jurisdictions that achieved a response rate ≥50% were included in the analyses (Alaska, Arizona, Arkansas, Connecticut, Delaware, District of Columbia, Florida, Georgia, Illinois, Iowa, Louisiana, Maryland, Massachusetts, Michigan, Missouri, Nebraska, New Jersey, New York City, North Dakota, Oregon, Pennsylvania, Puerto Rico, South Dakota, Tennessee, Utah, Vermont, Virginia, West Virginia, and Wyoming). The sample included 14 154 people with live births in the participating jurisdictions during the study period.
PRAMS is a jurisdiction-specific, population-based surveillance system conducted by the Centers for Disease Control and Prevention in collaboration with state, city, and territorial health departments. Each participating jurisdiction uses a standardized data collection protocol and draws a stratified random sample from birth certificate records every month. Individuals are sampled 2 to 6 months after a live birth and are mailed up to 3 surveys. Mail nonrespondents are contacted to complete the survey by telephone. People who gave birth to singletons, twins, and triplets are included in the sample. Prior to release for analysis, data are weighted to account for the complex survey design of PRAMS. Details of the PRAMS methodology have been described previously. 14 The institutional review boards of the Centers for Disease Control and Prevention and each participating jurisdiction approved the PRAMS surveillance protocol.
The measure of physical IPV was from the PRAMS core survey used by all jurisdictions. The question asked respondents if a current or former husband or partner physically hurt them during their most recent pregnancy. The measure of increased aggression was from a question on the Maternal COVID-19 Experiences supplemental questionnaire that asked respondents if any of the following things happened to them that they perceived to be due to the COVID-19 pandemic: “My husband or partner was more physically, sexually, or emotionally aggressive towards me.” 15
Data on demographic characteristics and infant outcomes were obtained from the linked birth certificate file; information on postpartum health was from the PRAMS questionnaire; and COVID-19–related stressors (economic, housing, food, and childcare challenges; mental health issues; COVID-19 illness) were derived from the Maternal COVID-19 Experiences supplemental questionnaire (Table 1).
Study variables, definitions, and sources for analysis of physical intimate partner violence and increased aggression due to the COVID-19 pandemic: PRAMS, 2020
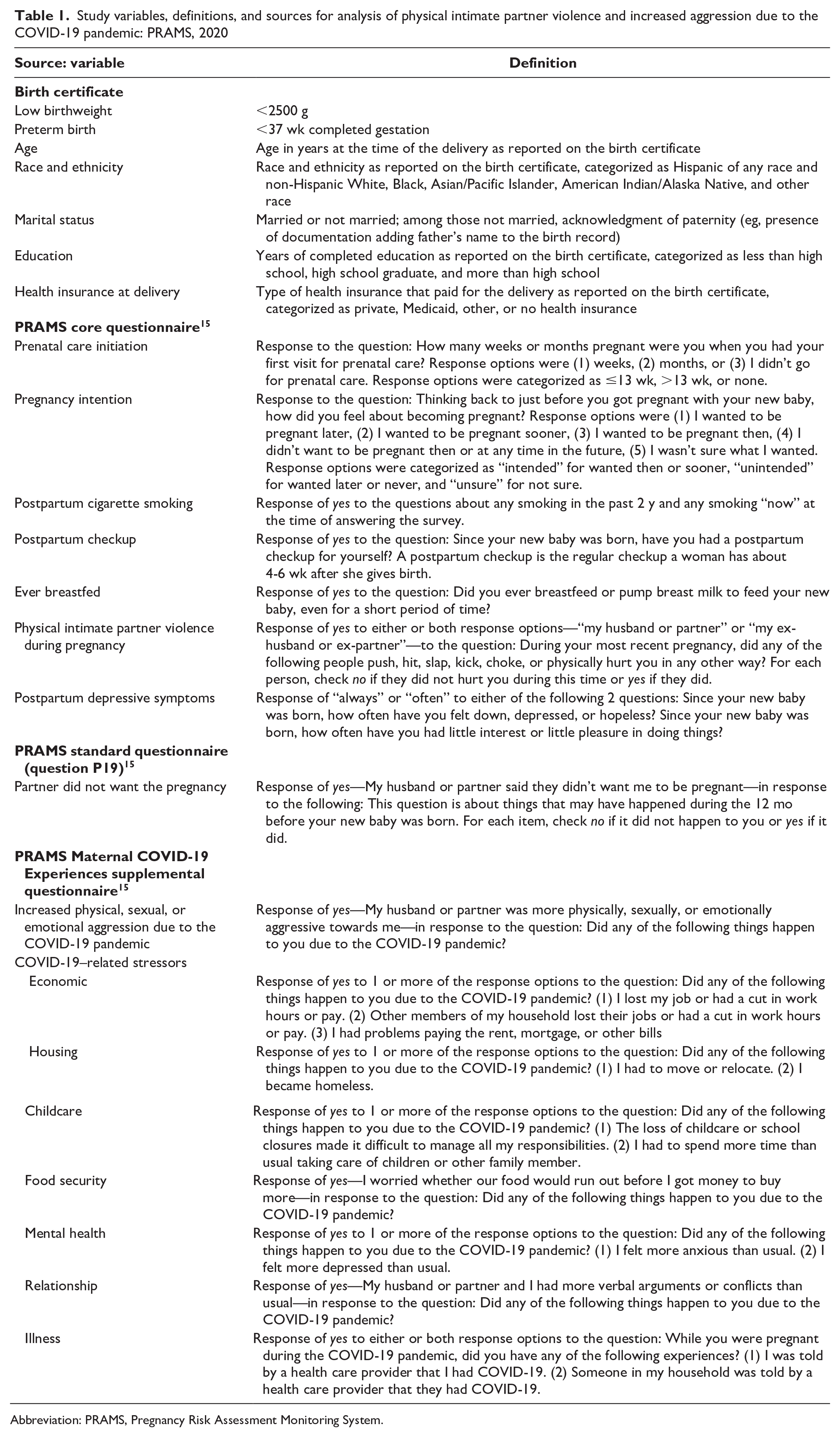
Abbreviation: PRAMS, Pregnancy Risk Assessment Monitoring System.
We calculated weighted prevalence estimates and 95% CIs for report of experiencing physical IPV during pregnancy or increased aggression by a husband or partner due to the COVID-19 pandemic, by respondent characteristics, COVID-19–related stressors, postpartum health indicators, and infant birth outcomes. To assess differences among those who experienced each outcome, we used the Wald χ2 test, with P < .05 considered significant. For variables that had >2 levels (eg, age, education level), we reviewed 95% CIs of the weighted prevalence to identify those that were nonoverlapping. This typically conservative approach might fail to note differences between estimates more often than formal statistical testing. 16
We totaled the number of COVID-19–related stressors reported (range, 0-7) and grouped individuals by number of stressors experienced (0, 1-2, 3-4, and 5-7) to examine the cumulative impact of stressors on experiencing violence. We looked at the prevalence of reporting physical IPV or increased aggression by race and ethnicity for Hispanic, non-Hispanic Black, and non-Hispanic White respondents by the number of stressors. For this analysis examining the number of stressors, we had insufficient sample size to generate reliable estimates for other racial and ethnic groups.
We calculated adjusted prevalence ratios (APRs) to examine the associations of physical IPV during pregnancy and increased physical, sexual, or emotional aggression from a husband or partner due to the COVID-19 pandemic with (1) COVID-19–related stressors and (2) postpartum health conditions and behaviors and infant birth outcomes. Based on previous literature, multivariable logistic regression models were adjusted for age, race and ethnicity, marital status, health insurance at delivery, and jurisdiction of residence (P < .05). 17 All analyses were conducted with SUDAAN version 11.0 (RTI International).
Results
Overall, 1.6% of respondents reported physical IPV during pregnancy, and 3.1% reported increased physical, sexual, or emotional aggression from a husband or partner due to the COVID-19 pandemic (Table 2). The prevalence of physical IPV and aggression was higher among respondents aged 20 to 24 (vs ≥25) years, among unmarried respondents (vs married respondents), among those with high school education or less (vs more than high school education), and among those who received Medicaid at the time of delivery (vs private health insurance). Non-Hispanic White respondents had a lower prevalence of physical IPV during pregnancy (1.0%; 95% CI, 0.7%-1.4%) than Hispanic respondents (2.2%; 95% CI, 1.6%-3.1%), non-Hispanic Black respondents (3.0%; 95% CI, 2.1%-4.1%), and non-Hispanic American Indian/Alaska Native respondents (4.3%; 95% CI, 2.7%-6.8%). Non-Hispanic White respondents had a lower prevalence of increased intimate partner aggression (2.4%; 95% CI, 1.8%-3.1%) than non-Hispanic Black respondents (4.8%; 95% CI, 3.7%-6.3%).

Abbreviations: AOP, acknowledgment of paternity; IPV, intimate partner violence; PRAMS, Pregnancy Risk Assessment Monitoring System.
Data source: PRAMS. 14
Reported by individuals with a recent live birth (June–December 2020) in 29 sites conducting PRAMS: Alaska, Arizona, Arkansas, Connecticut, Delaware, District of Columbia, Florida, Georgia, Illinois, Iowa, Louisiana, Maryland, Massachusetts, Michigan, Missouri, Nebraska, New Jersey, New York City, North Dakota, Oregon, Pennsylvania, Puerto Rico, South Dakota, Tennessee, Utah, Vermont, Virginia, West Virginia, and Wyoming.
Respondent indicated yes to husband/partner or ex-husband/ex-partner doing any of the following during pregnancy: “hit, slap, kick, choke, or physically hurt you in any way.”
Unweighted sample size varies due to missing responses.
Weighted prevalence (expressed as a percentage).
Wald χ2 test with P < .05 considered significant.
Indicator used by 17 sites: Alaska, Connecticut, Delaware, Florida, Georgia, Illinois, Iowa, Louisiana, Massachusetts, Michigan, Missouri, Nebraska, New York City, Oregon, Pennsylvania, Utah, and Wyoming.
As compared with individuals who had an intended pregnancy, those who reported that their pregnancy was unintended or that they were unsure had a higher prevalence of physical IPV during pregnancy (unintended, 3.2% [95% CI, 2.4%-4.3%]; unsure, 2.8% [95% CI, 2.0%-3.9%]) and increased intimate partner aggression (unintended, 5.1% [95% CI, 4.0%-6.5%]; unsure, 5.0% [95% CI, 3.6%-6.9%]) (Table 2). We also found a higher prevalence for physical IPV and increased aggression among respondents who reported (vs did not report) that their partners said that they did not want the pregnancy (physical IPV, 13.1% [95% CI, 9.3%-18.0%]; increased aggression, 19.9% [95% CI, 15.1%-25.8%]).
Except for COVID-19 illness, all COVID-19–related stressors were significantly associated with physical IPV during pregnancy and increased aggression from a husband or partner due to the COVID-19 pandemic (Table 3). The strongest association was with increased verbal conflicts due to COVID-19 (physical IPV: APR, 6.63 [95% CI, 4.23-10.38]; increased aggression: APR, 25.37 [95% CI, 16.76-38.41]). Other stressors strongly associated with physical IPV and increased intimate partner aggression were any mental health stressors (physical IPV: APR, 2.88 [95% CI, 1.78-4.68]; increased aggression: APR, 4.54 [95% CI, 3.04-6.76]) and food insecurity (physical IPV: APR, 2.51 [95% CI, 1.57-4.02]; increased aggression: APR, 3.72 [95% CI, 2.61-5.28]). Respondents who reported any economic problems, any housing instability, or any childcare challenges had approximately 2 to 4 times the prevalence of reporting physical IPV during pregnancy or increased intimate partner aggression as compared with respondents who did not report these stressors.

Abbreviations: APR, adjusted prevalence ratio; IPV, intimate partner violence; PRAMS, Pregnancy Risk Assessment Monitoring System.
Data source: PRAMS. 14
Reported by individuals with a recent live birth (June–December 2020) in 29 sites conducting PRAMS: Alaska, Arizona, Arkansas, Connecticut, Delaware, District of Columbia, Florida, Georgia, Illinois, Iowa, Louisiana, Maryland, Massachusetts, Michigan, Missouri, Nebraska, New Jersey, New York City, North Dakota, Oregon, Pennsylvania, Puerto Rico, South Dakota, Tennessee, Utah, Vermont, Virginia, West Virginia, and Wyoming.
Respondent indicated yes to husband/partner or ex-husband/ex-partner doing any of the following during pregnancy: “hit, slap, kick, choke, or physically hurt you in any way.”
Weighted prevalence (expressed as a percentage).
Adjusted for age, race and ethnicity, marital status, health insurance at delivery, and jurisdiction of residence.
Respondents reported that loss of childcare or school closures made it difficult to manage responsibilities and/or that they needed to spend more time than usual taking care of children or other family members.
Respondents reported that they or another member of their household was told that they had COVID-19 infection during the time when they were pregnant.
The report of experiencing physical IPV during pregnancy or increased intimate partner aggression due to the COVID-19 pandemic increased as the number of stressors increased for Hispanic, non-Hispanic Black, and non-Hispanic White respondents (Figure).
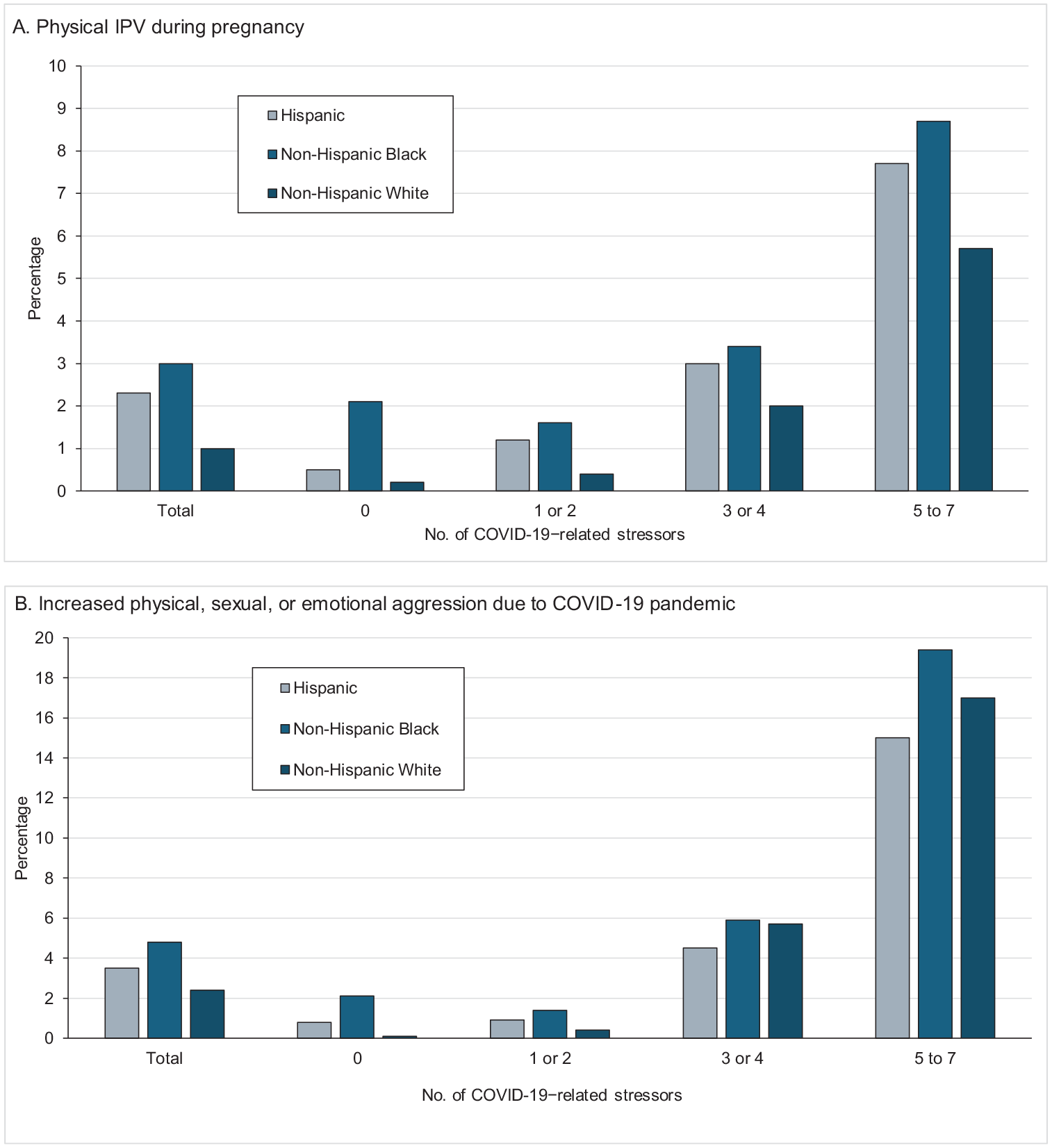
Prevalence of experiencing intimate partner violence (IPV) during pregnancy or increased physical, sexual, or emotional aggression from an intimate partner due to the COVID-19 pandemic, by number of COVID-19–related stressors and by race and ethnicity, among individuals with a live birth, Pregnancy Risk Assessment Monitoring System (PRAMS), 2020. Data source: PRAMS.14 Reported by individuals with a recent live birth (June–December 2020) in 29 sites conducting PRAMS: Alaska, Arizona, Arkansas, Connecticut, Delaware, District of Columbia, Florida, Georgia, Illinois, Iowa, Louisiana, Maryland, Massachusetts, Michigan, Missouri, Nebraska, New Jersey, New York City, North Dakota, Oregon, Pennsylvania, Puerto Rico, South Dakota, Tennessee, Utah, Vermont, Virginia, West Virginia, and Wyoming.
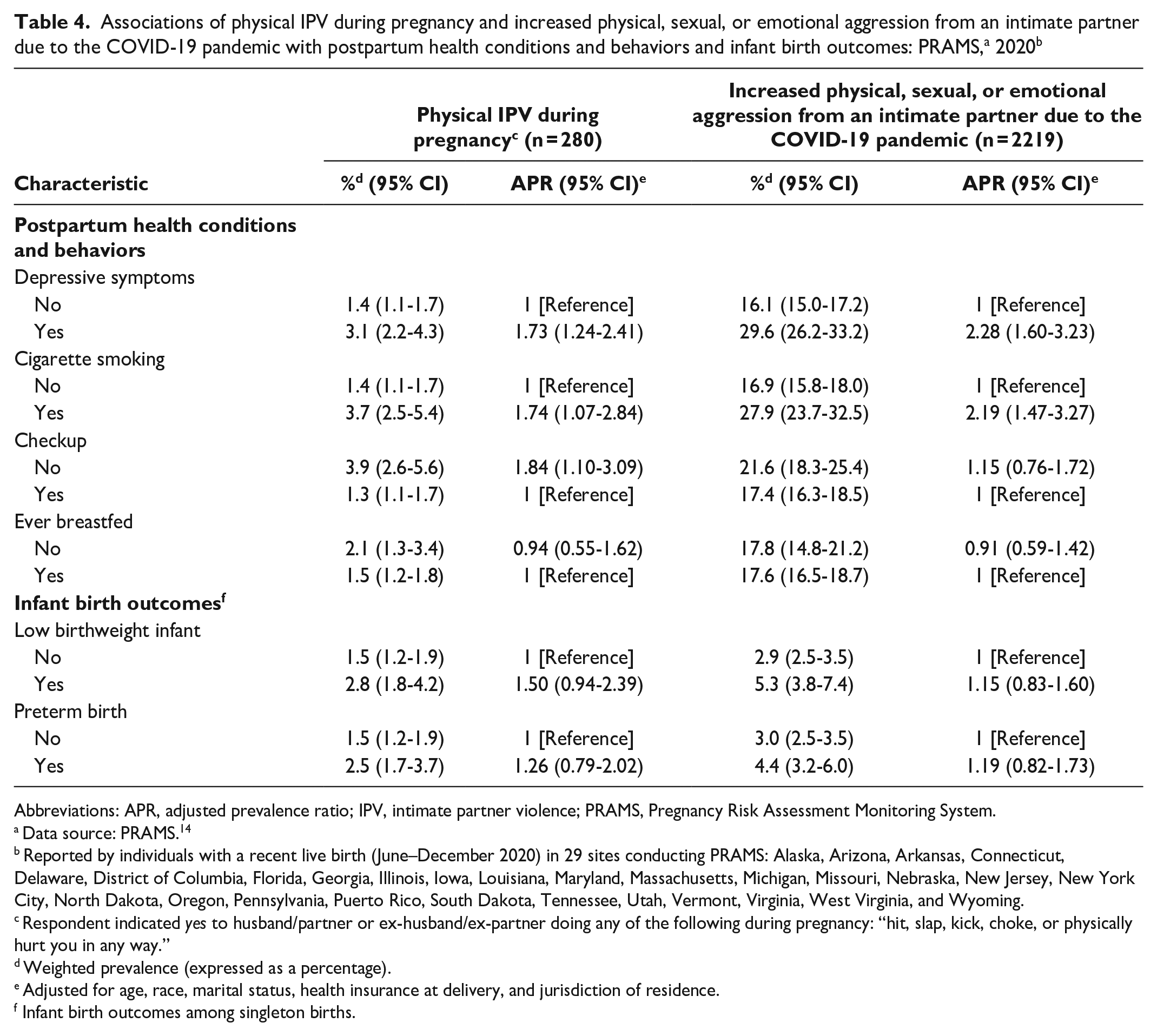
For postpartum outcomes, we found significant differences for the prevalence of postpartum depressive symptoms and postpartum smoking by comparing those who experienced physical IPV or increased aggression with those who did not (Table 4). For example, the prevalence of postpartum depressive symptoms was approximately twice as high for those who experienced violence as for those who did not (physical IPV: APR, 1.73 [95% CI, 1.24-2.41]; increased aggression: APR, 2.28 [95% CI, 1.60-3.23]), as was the prevalence of postpartum cigarette smoking (physical IPV: APR, 1.74 [95% CI, 1.07-2.84]; increased aggression: APR, 2.19 [95% CI, 1.47-3.27]). The prevalence of not attending a postpartum checkup was higher for respondents reporting physical IPV during pregnancy (APR, 1.84; 95% CI, 1.10-3.09) but not significantly different for respondents reporting increased aggression. We found no significant differences in breastfeeding or infant birth outcomes for either indicator.
Abbreviations: APR, adjusted prevalence ratio; IPV, intimate partner violence; PRAMS, Pregnancy Risk Assessment Monitoring System.
Data source: PRAMS. 14
Reported by individuals with a recent live birth (June–December 2020) in 29 sites conducting PRAMS: Alaska, Arizona, Arkansas, Connecticut, Delaware, District of Columbia, Florida, Georgia, Illinois, Iowa, Louisiana, Maryland, Massachusetts, Michigan, Missouri, Nebraska, New Jersey, New York City, North Dakota, Oregon, Pennsylvania, Puerto Rico, South Dakota, Tennessee, Utah, Vermont, Virginia, West Virginia, and Wyoming.
Respondent indicated yes to husband/partner or ex-husband/ex-partner doing any of the following during pregnancy: “hit, slap, kick, choke, or physically hurt you in any way.”
Weighted prevalence (expressed as a percentage).
Adjusted for age, race, marital status, health insurance at delivery, and jurisdiction of residence.
Infant birth outcomes among singleton births.
Discussion
Physical IPV during pregnancy and increased intimate partner physical, sexual, or emotional aggression due to the COVID-19 pandemic were both strongly associated with COVID-19–related stressors and some postpartum outcomes. A study that surveyed women, nonbinary individuals, and transgender people in Michigan during the summer of 2020 found that new experiences of IPV and more severe IPV both increased during the beginning of the pandemic and were more prevalent among pregnant people than among nonpregnant people. 13
While other studies have found increases in IPV during the pandemic,9,10,18 few have examined these experiences during pregnancy. When compared with estimates of IPV during pregnancy before the pandemic, our estimate of 1.6% of respondents experiencing physical IPV during pregnancy was slightly lower than PRAMS estimates from 2016-2019, which ranged from 2.0% to 2.2%. 19 Several factors may be associated with the lower self-report of physical IPV in our study. The jurisdictions in our analysis overlapped with, but were not identical to, those used to calculate earlier estimates. In addition, our sample consisted of individuals who gave birth in the latter part of 2020, all of whom were pregnant during the early stages of the COVID-19 pandemic, when lockdown and quarantine measures were initially put into place. Individuals who were in lockdown situations or experienced other stressors with an abusive partner may have had less opportunity to privately complete the survey, thereby reducing the likelihood of responding affirmatively to questions about violence. Conversely, the lockdowns may have been protective if respondents were separated from abusive partners or if other unmeasured factors reduced exposure during the study period for this population.
Our second measure encompassed sexual or emotional aggression in addition to physical aggression. For this question, respondents were asked if they had experienced increases in any of these types of behavior from a husband or partner that they attributed to the COVID-19 pandemic. The prevalence estimate for this measure was about twice (3.1%) the physical IPV estimate (1.6%). The fact that this indicator captured multiple types of aggression and asked about escalation may explain the higher prevalence as compared with the physical violence indicator.
We found associations between IPV and COVID-19–related stressors. In particular, increased verbal arguments or conflict due to the COVID-19 pandemic showed the strongest association with physical IPV (nearly 5 times higher) and increased aggression (>25 times higher). Numerous studies have identified the role of arguments, jealousy, conflicts, and other situational factors in the perpetration of IPV,20 -23 and our findings related to increased verbal arguments and conflicts corroborate this phenomenon.
Non-Hispanic American Indian and Alaska Native respondents and non-Hispanic Black respondents had a higher prevalence of reporting physical IPV or increased intimate partner aggression than non-Hispanic White respondents. Higher rates of IPV among American Indian and Alaska Native and Black women as compared with women from other racial and ethnic groups have been documented, 24 as have disproportionate rates of the negative health effects of the COVID-19 pandemic on marginalized racial and ethnic groups.25,26 Many reports have illuminated the role of underlying structural inequities contributing to the disparities in health outcomes due to the COVID-19 pandemic. 27 Structural factors and racism also place individuals from marginalized racial and ethnic groups at greater risk of experiencing IPV than people in other racial and ethnic groups.28,29 These same factors may be underlying drivers for the higher levels of IPV found in our study.
We found that physical IPV during pregnancy and increased aggression were associated with a higher prevalence of postpartum depressive symptoms and postpartum cigarette smoking when compared with the prevalence among people who did not experience these types of violence. Other studies have found a relationship between physical IPV and a higher prevalence of cigarette smoking.30 -32 A higher prevalence of mental health conditions is also well established among individuals who experience IPV as compared with those who do not. 7 Our study adds to this evidence by illuminating the association of COVID-19–related stressors and increased aggression during pregnancy on postpartum mental health.
We found an association between physical IPV during pregnancy and lower attendance at postpartum care visits. People experiencing IPV may have difficulty attending health care visits. 33 The COVID-19 pandemic posed numerous additional challenges to health care access with clinic closures and the expansion of new approaches to care, such as telehealth, which may not have been equally accessible for everyone.34,35 Nevertheless, postpartum respondents in our study who experienced physical IPV during pregnancy were less likely to attend postpartum check-ups than those who did not report this experience. Screening for IPV is universally recommended, as are referrals to resources and social supports to ensure safety and avoid delayed or missed care.36 -38 Health care providers and health care systems may consider systematic processes to follow up with patients who miss their initial postpartum checkup, including exploring the use of telehealth as an option for increasing access.
We identified a positive association between the 2 measures of IPV and infant birth outcomes (low birthweight and preterm birth), but neither was significant. Serious consequences of trauma during pregnancy, including physical IPV, can include injury or death to the infant, 39 low birthweight, and preterm birth. 40 However, we did not have information on the severity, timing, or type of physical violence, which may be a reason why we did not see a significant association between physical IPV or increased intimate partner aggression due to the COVID-19 pandemic and infant birth outcomes.
Limitations
This study had several limitations. First, data represent individuals from the 29 jurisdictions in the United States and may not be generalizable beyond these locations. There may be variation in patterns of COVID-19–related stressors and IPV by jurisdiction due to underlying rates of poverty and intensity of the public health response to the pandemic. Second, PRAMS respondents had a recent live birth; as such, these findings do not represent people who experienced other pregnancy outcomes, such as stillbirth. Third, information from the PRAMS survey is self-reported in the postpartum period and may be subject to recall bias and social desirability bias, which may lead to underreporting on sensitive topics such as IPV. Fourth, all the sampled individuals gave birth in the later part of 2020; however, we did not have information on the exact timing of experiences of violence relative to the beginning of the COVID-19 pandemic, nor could we disaggregate the type of increased aggression reported.
Conclusion
Physical IPV and increased physical, sexual, and emotional aggression from a husband or partner due to the COVID-19 pandemic during pregnancy were associated with COVID-19–related stressors for individuals with a recent live birth. This study highlights how these experiences were related to adverse postpartum health experiences, emphasizing the importance of ongoing efforts to prevent IPV and continued research to advance understanding of the ongoing impacts during the postpandemic period. A multisectoral approach incorporating evidence-based strategies that address IPV prevention at the societal, community, relationship, and individual levels may have the greatest impact. Prevention strategies with the best available evidence include teaching relationship skills, strengthening economic supports, and creating protective environments. 41 Health care workers who see postpartum individuals can also play an important role in providing screening and referrals.36,37 In addition, understanding how the COVID-19 pandemic contributed to making screening and access to resources difficult and exacerbated risk factors for violence, such as economic and social stressors, can help inform preparedness efforts ahead of future public health emergencies.
Footnotes
Acknowledgements
The authors thank the PRAMS Working Group, which includes the PRAMS sites in this analysis—Alaska, Arizona, Arkansas, Connecticut, Delaware, District of Columbia, Florida, Georgia, Illinois, Iowa, Louisiana, Maryland, Massachusetts, Michigan, Missouri, Nebraska, New Jersey, New York City, North Dakota, Oregon, Pennsylvania, Puerto Rico, South Dakota, Tennessee, Utah, Vermont, Virginia, West Virginia, and Wyoming—and the PRAMS Team in CDC’s Division of Reproductive Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Qing Li received partial financial support from the University of Colorado School of Medicine, the 2021 and 2022 Slay Community Scholars, and the US Department of Health and Human Services Office on Women’s Health, Violence Against Women, and Substance Use Prevention Initiative (grant ASTWH220111-01-00 WH-AST-22-004).