
Abstract
Intimate partner violence (IPV) is a global public health crisis associated with adverse physical, psychological, economic, and social consequences. Studies on the impact of COVID-19 on IPV against women are scarce. This study aimed to understand the impact of COVID-19 on IPV against women. Google Scholar, PubMed, and the Cochrane Library were searched using the MeSH terms intimate partner violence, COVID-19, and women. Exclusion criteria were male-partner, elder, and child abuse and studies that targeted specific groups such as cancer, HIV, and substance abuse. Two independent reviewers completed the title, abstract screening, and review of selected articles. Thirteen out of 647 articles met the inclusion criteria. IPV against women increased in nine countries (Spain, United States, Nigeria, Ethiopia, Turkey, Peru, Bangladesh, Czech Republic, and the Democratic Republic of Congo); one country showed no change in gender-based violence among adolescent girls and young women (Kenya); and one study reported a decrease in IPV reporting by victims (United States). Policies made to mitigate the pandemic created unintended consequences that exacerbated risk factors for IPV against women. Lessons learned from COVID-19 must be used to develop policy-level support and response services to mitigate IPV against women amid a pandemic and other human crises.
Intimate partner violence (IPV) is an endemic, preventable global health crisis. The World Health Organization (WHO) refers to IPV as the actions by an intimate partner resulting in psychological, physical, or sexual harm. IPV is one of the widespread forms of brutality against women. It is associated with poor physical and psychological outcomes for victims and destroys their self-esteem. Survivors of IPV are susceptible to multiple mental health disorders (anxiety, disordered eating, posttraumatic stress disorder, substance use disorder, alcohol dependency, mood disorders) and health problems such as sexually transmitted diseases and infections, cardiovascular disorders, chronic pain, sleep disorders, craniocerebral trauma, and digestive issues. 1
Economic, social, and cultural norms influence IPV. Before the pandemic, the WHO estimated that 35 percent of women globally suffered various forms of violence from their intimate partners. 2 According to WHO, close to one in three, or 30 percent of women, have been exposed to physical and sexual harm. 2 The WHO stipulated that the prevalence estimates of lifetime IPV vary from 20 percent in the Western Pacific region, 22 percent in wealthy nations and Europe, and 25 percent in the Americas to 33 percent in African countries, 31 percent in the Eastern Mediterranean countries, and 33 percent in Southeast Asia. 2
Governments worldwide introduced restrictive social distancing and quarantining strategies to mitigate the pandemic. 3 The restrictive measures impacted families and communities and created unintended consequences, which affected interpersonal relationships, family bonding, income, access to health care and social services, mental health, and general well-being.4,5
Among the adverse effects of the restrictive COVID-19 measures was increased IPV against women. The United Nations General Secretary has recognized violence against women as a “global pandemic”. 6 The coexistence of a pandemic (IPV) in a pandemic (COVID-19) increased IPV's risk factors and severity.7,8 Natural and public health crises, including pandemics, intensify gender inequalities and negatively influence women's access to health care, social service, and social support.8–10
Incipient data have shown increased IPV against women during the first outbreak of the COVID-19 pandemic.11–15 To devise strategies and interventions to mitigate the negative impact of IPV, it is imperative to comprehend the nature and effect of the COVID-19 pandemic on IPV against women through a methodical review of existing literature. This study aims to understand the contributing determinants and the impact of COVID-19 pandemic on IPV against women with measures instituted to mitigate the pandemic.
Method
Study Design
This systematic review was conducted under the recommended reference framework of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 16 A literature search was conducted on Google Scholar, PubMed, and Cochrane Library databases. The algorithm included IPV and COVID-19 and women, OR intimate partner violence AND COVID-19 AND women. Snowball sampling was used for searching the references of eligible studies.
Inclusion Criteria
Primary research articles published between March 2020 to March 2022 were considered. Articles that studied IPV amid COVID-19, described the effect of COVID-19's restrictive measures on IPV against women, discussed the incidence and prevalence of IPV in the course of the pandemic, and excluded other types of violence such as elder abuse, minor abuse, or male-partner abuse were included.
For the study design, cross-sectional studies, ecological studies, comparative studies, surveys, national surveys, mixed-methods prospective studies, randomized studies, and case reports were selected. Studies were limited to the English language and women. There was no restriction on demography or location. Two authors (I.U. and A.A.) independently performed the selection of studies.
Data Extraction and Analysis
In the data evaluation stage, titles and abstracts were initially evaluated to pre-select articles that would be read in full. Two reviewers independently reviewed the pre-selected articles. From each study, the title, name of the first author, year of publication, country where the research took place, language, study design, study period, sample size, age range of sampling, characteristics of the study population, study inclusion and exclusion criteria, association with COVID-19, statistical analysis, outcomes, results, main findings, conclusion, and recommendations were extracted. Disagreements between the reviewers were resolved through team discussion. Six hundred and forty-seven studies were identified, of which 13 articles were read in detail and selected for data procurement to develop the synthesis matrix (Figure 1).
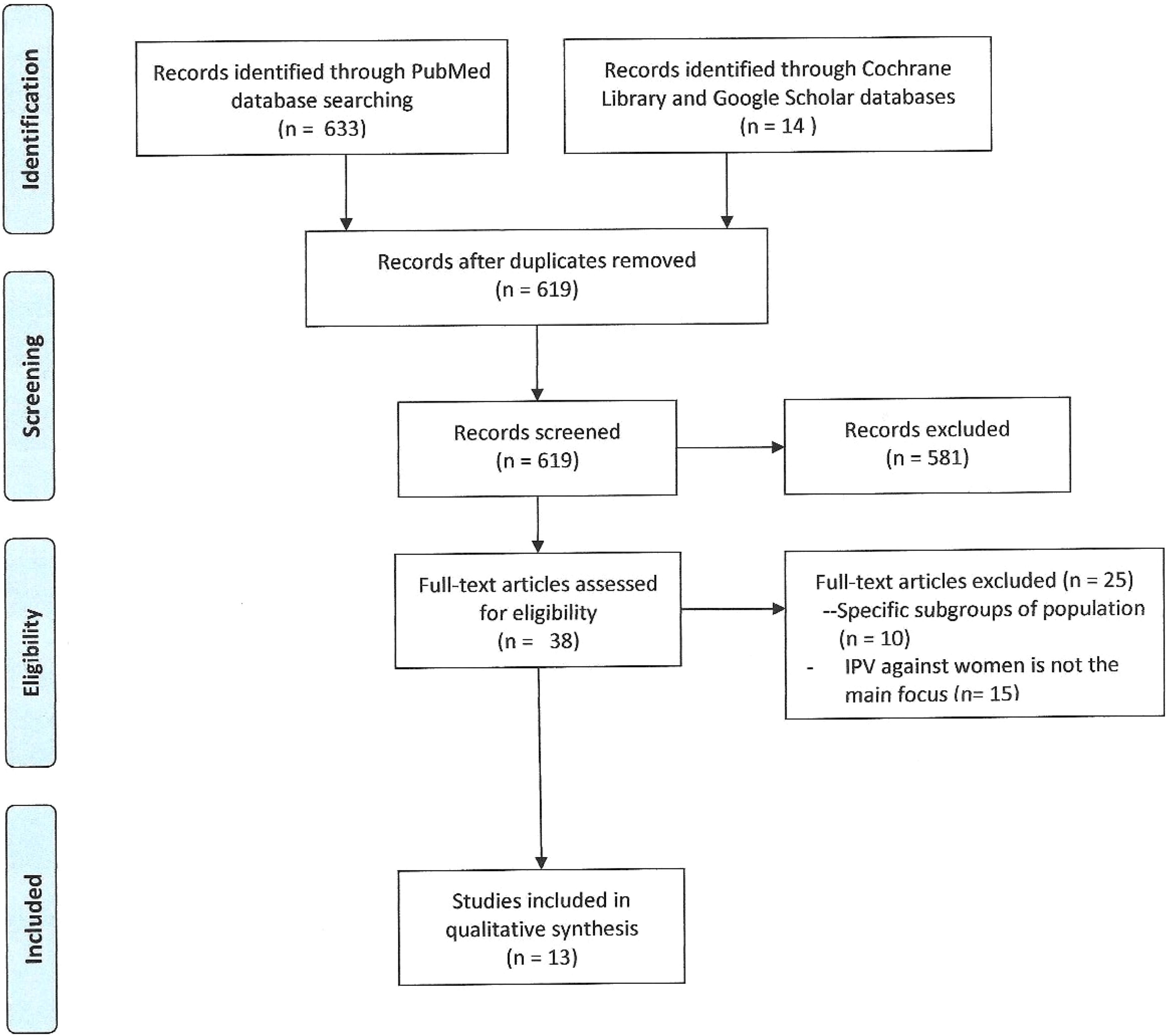
Prisma flowchart depicting study inclusion and exclusion.
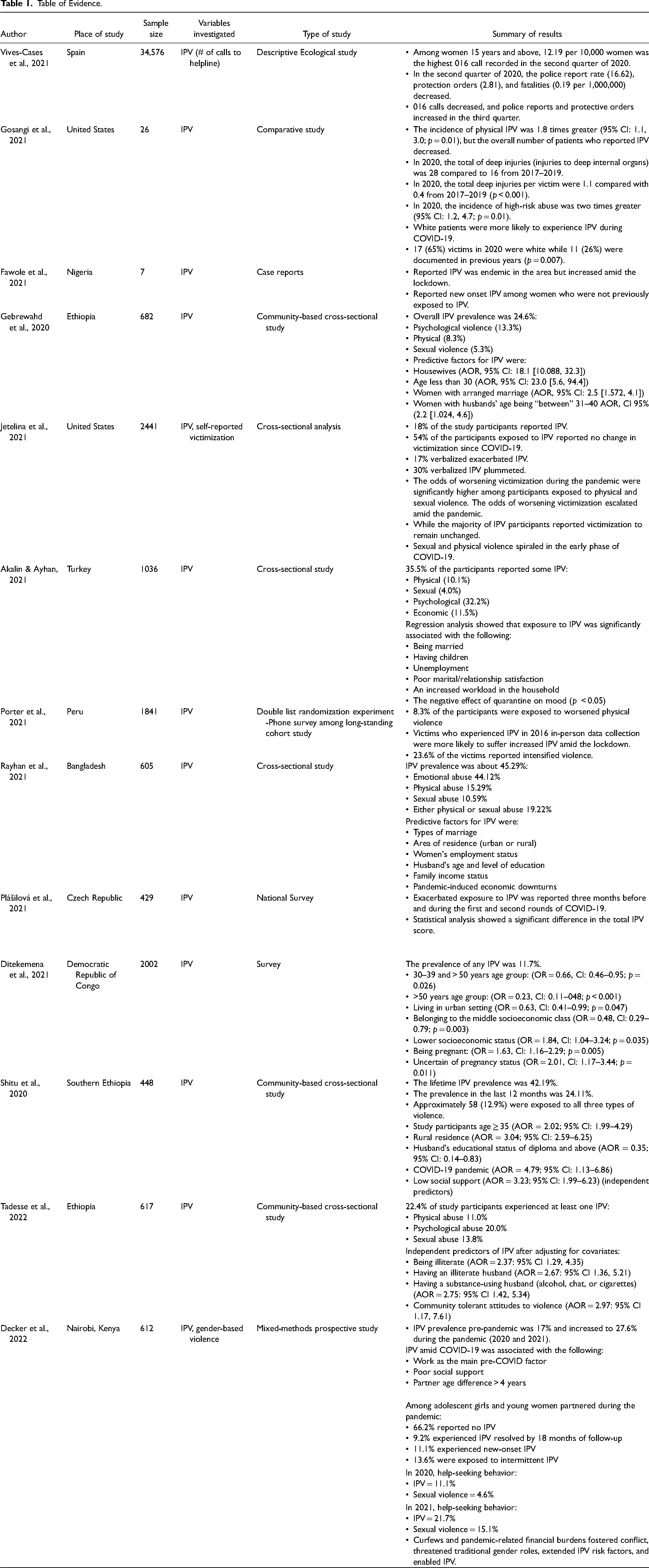
The data collected were arranged in a synthesis matrix, which helped in data grouping and comparison to spot thematic categories (Table 1). Summary of exposure characteristics and predictive factors for increased IPV against women amid the COVID-19 reported across the 13 studies reviewed are listed in Table 2.
Table of Evidence.
Summary of Exposure Characteristics/Predictive Factors for Increased IPV Against Women Amid COVID-19 Reported Across the 13 Studies Reviewed.
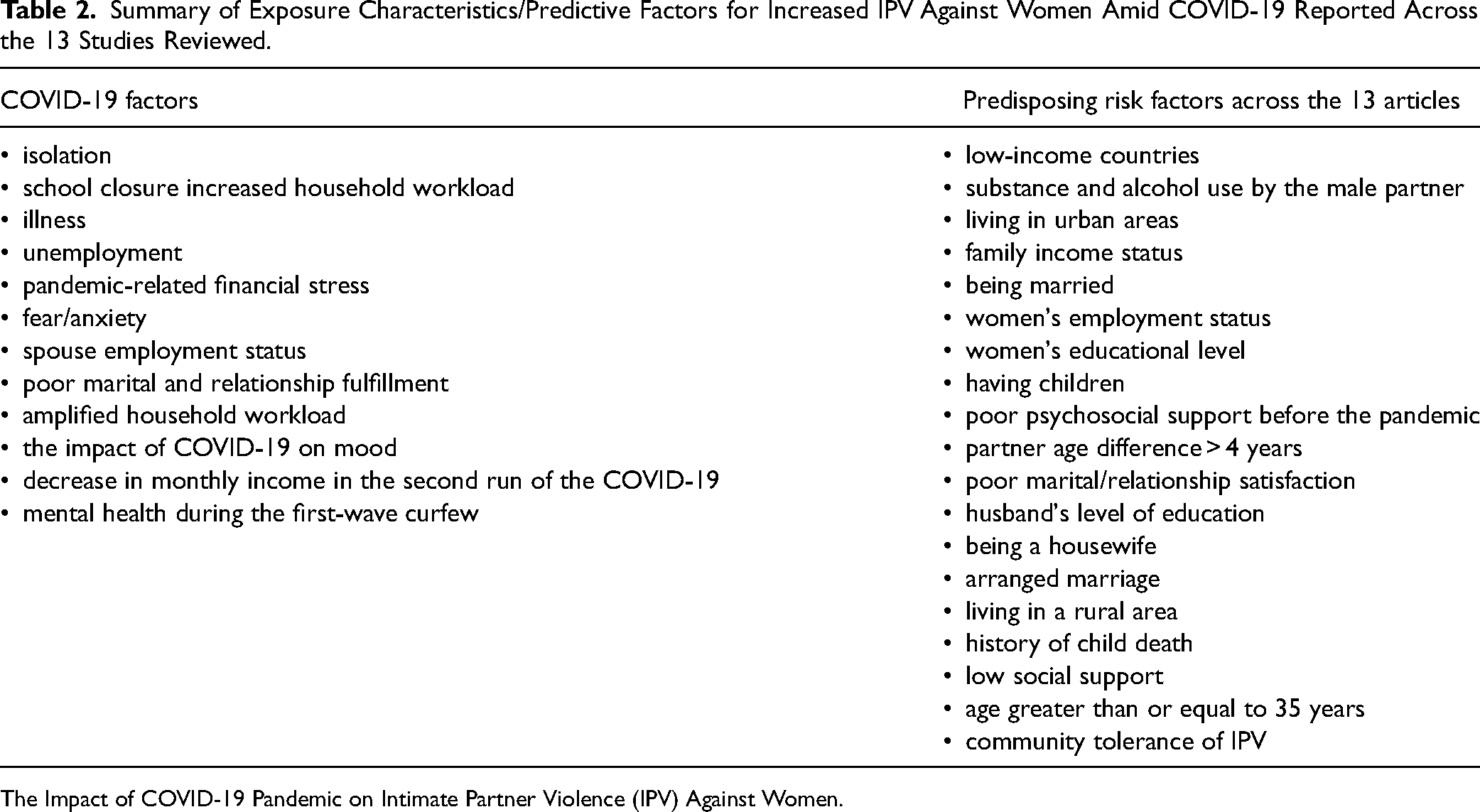
The Impact of COVID-19 Pandemic on Intimate Partner Violence (IPV) Against Women.
Quality Assessment
Two independent reviewers (I.U. and A.A.) conducted quality assessments, evaluating the risk of bias in eligible studies.
Results
Selection of Studies
Six hundred and forty-seven studies were retrieved from the databases. Fourteen of the 647 were duplicates. Consequently, 619 were screened by abstract, of which 581 were found irrelevant. Of the 38 full-text articles assessed, 25 were excluded because the main focus was not IPV against women or they addressed a specific population subgroup. Thirteen articles were critically read, analyzed, and chosen for data obtainment (Figure 1 and Table 1).9,13,15,17–26 The studies included were conducted in Spain (n = 1), United States (n = 2), Nigeria (n = 1), Ethiopia (n = 3), Turkey (n = 1), Peru (n = 1), Bangladesh (n = 1), Czech Republic (n = 1), Democratic Republic of Congo (n = 1), and Kenya (n = 1). Approximately 50 percent of the articles (n = 6) were cross-sectional studies, descriptive ecological study (n = 1), case report (n = 1), comparative study (n = 1), surveys (n = 2), double list randomization experiment (n = 1), or mixed-methods prospective cohort study (n = 1) (Table 1).
Descriptive Characteristics
All the studies were conducted during COVID-19, approximately from March 2020– March 2022. The descriptive attributes of the eligible and selected studies are presented in Table 1. Ten studies included data from surveys.9,15,17,18,20–24,26 One study included data from 016 calls “emergency helpline call” and police reports. 25 One study included data from emergency department radiological studies for bodily injuries. 13 One study included data from case reports. 19
A common theme across the 13 selected articles was that IPV against women increased significantly during the pandemic because of the COVID-19 restrictive measures, which precipitated underlying predisposing risk factors to IPV. Nine of the 13 articles indicated an increased prevalence of IPV, ranging from 8.3 percent to 45.29 percent.9,17,18,20–23,25,26 Two articles reported increased IPV as verbalized by the victims but did not provide quantifiable data on how much the increase was.15,19 A rise in 016 calls in the second outbreak of 2020 was recorded, with the most significant 016 call rate documented (12.19 per 10,000 women 15 years or older), police report rates (16.62), protection orders (2.81), and fatalities (0.19 per 1,000,000 women 15 years or older). 25 Also, a decrease in 016 calls in the third quarter of 2020 was reported, but police reports and protection orders increased. 25 In addition, 8.3 percent of study participants verbalized experiencing increased physical violence in their households amid the COVID-19 lockdown. 21
Four studies reported that during COVID-19, sociodemographic factors, accessibility to resources, and unemployment were predictive factors for new-onset IPV and increased existing IPV.18,19,22,25 In a four-cluster study (016 calls, protection orders, unemployment rates, and current exiting IPV rates) analysis, significant variations in unemployment rates between clusters were reported (F = 3.05, p < 0.05). 25 Increased IPV was reported among women who lacked resources due to isolation from COVID-19 strategies. 19 Rayhan and Akter documented that women's employment status, husbands’ educational status, household income level, and pandemic-initiated financial decline were linked to IPV amid the pandemic. 22 A negative association was found between belonging to the middle and lower socioeconomic classes and IPV. 18
Five studies documented that type of marriage and relationship, living arrangements (housewife), age of the victim (age less than 30), spousal age (31–40 years), and poor marital/relationship satisfaction were predictive determinants for IPV.17,22−24,26 Increased IPV was noted among couples between 30–39 and > 50 old. 18 Also, living in an urban setting, being pregnant, and uncertainty of pregnancy status increased the prevalence of IPV. 18 Participants aged ≥ 35, living in the countryside, husband's educational level, COVID-19, and poor socioeconomic factors were predictive elements for increased IPV amid COVID-19.23,24 Still, Tadesse and their team added that chemical-dependent husbands and residing in a community where violence is endemic and condoned were independent predictors of IPV among married women. 24 IPV was correlated with work as the major pre-COVID-19 factor, poor social support, and intimate partner age gap > 4 years. 9 Help-seeking behavior for IPV and sexual violence among victims in 2020 (11.1% and 4.6%, respectively) expanded to 21.7 percent and 15.1 percent, subsequently, in 2021. 9
Four articles reported that women experienced psychological IPV more than sexual or physical IPV. Gebrewahd and their team found that the most common IPV was psychological violence and reported psychological abuse (13.3%), physical abuse (8.3%), and sexual abuse (5.3%). 26 Akalin and their team reported psychological IPV (32.2%), economic abuse (11.5%), physical abuse (10.1%), and sexual abuse (4.0%). 17 And Rayhan and their team reported emotional IPV (44.12%), physical IPV (15.29%), and sexual IPV (10.59%). 22
Two articles reported decreased or no change in IPV prevalence during the pandemic—the total number of patients who reported exposure to IPV reduced during COVID-19. 13 However, the new occurrence of physical violence increased 1.8 times above pre-pandemic levels. The aggregate number of deep injuries increased from 16 (2017–2019) to 28 in 2020. 13 Fifty-four percent of their study participants exposed to IPV reported no change in victimization since COVID-19, 30 percent verbalized IPV plummeted, and 17 percent experienced exacerbated IPV. 20 Among women who experienced increased IPV, the odds of worsening victimization increased among those exposed to physical and sexual violence. 20
The prevalence of new-onset, high-risk abuse was more than doubled in 2020 compared to previous years, 13 and White patients were more likely to be exposed to increased IPV amid COVID-19. It was reported that 66.2 percent of young women and adolescent girls partnered during the pandemic did not experience IPV. 9
The review showed that prior exposure to IPV was a predictive factor for IPV during COVID-19. Women exposed to IPV experienced a rise in the severity of IPV or a new form of violence during the lockdown. 19 Women exposed to IPV during the last round of 2016 data acquisition were more likely to be exposed to exacerbated IPV amid the pandemic, noting that 23.6 percent of the study sample verbalized a rise in IPV exposure in the pandemic. 21 The odds of aggravated victimization amid COVID-19 increased among women exposed to physical and sexual abuse. 20
An increase in IPV against women was determined based on calls to helplines, calls to organizations intended for violence victims and survivors, police reports, shelters, increased use of emergency services, radiographic images, and anecdotal evidence.13,25 These studies showed that IPV against women increased during the pandemic.9,15,17–19,21–24,26,27
Despite the evidence for increased IPV portrayed by the increased call to public safety, calls to IPV helplines, and institutions established for survivors, some authors stipulated an increased possibility of underreporting, especially in low-income countries and in cultures where IPV is commonly accepted.9,15,18,19,21,23,24,26
Authors who considered the possibility of underreporting of IPV during the pandemic stipulated the reasons may be due to aggressive and controlling behavior of their perpetrators, low privacy due to staying in lockdown with the aggressor, decreased social support, fear of contracting COVID-19, and inaccessibility to a care facility.9,15,18,19,21,23,24,26 Despite fewer emergency room visits amid COVID-19, women exposed to IPV experienced severe injuries compared to previous years, as the severe radiological injuries show. 13
Although most studies except two9,22 showed that physical and verbal IPV against women increased amid the pandemic, several authors found that sexual abuse was significantly prevalent.17,26
Most studies focused on the epidemiological analysis of IPV during the pandemic. They did not thoroughly discuss interventions to mitigate the effect of the pandemic on IPV or whether the interventions provided made any difference.
Recommendations formulated by the authors to mitigate IPV against women during the pandemic focused on addressing the predictive risk factors, which include the use of telemedicine to maintain contact with patients, traditional paths such as women's shelters, public campaigns, gender equality policies, personal and community support, and fostering of economic independence of vulnerable women and their families. Public health campaigns to highlight awareness and the creation of brochures on the topic can serve as social marketing tools.
Discussion
The increase in IPV amid COVID-19 is a worldwide public health crisis needing immediate intervention. The studies reviewed consist mainly of primary research, case reports, and cross-sectional studies. The studies exposed the unintended consequences of measures used to mitigate the pandemic and factors affecting women's well-being and physical and mental health. This review showed that risk factors for IPV were exacerbated by the pandemic, leading to increased IPV.
Due to a lack of access to IPV resources during the lockdown, women could not seek help. Another common perception is the responsibility of health care providers, public safety, and social service in recognizing and mitigating IPV against women. Although social services play a significant role in finding resources for IPV victims, they are not usually the first point of contact in cases of IPV. In cultures where IPV is tolerated, IPV was thought to be underreported. Physical and verbal abuse was more prevalent than sexual abuse. Changes in income due to unemployment during the lockdown was a major predisposing factor for IPV against women.
Among the COVID-19 factors, economic hardship and staying in isolation with the aggressor were considered most impactful in the increase in IPV incidence and prevalence. Economic problems caused by job loss and disconnection from many community financial and support systems due to stay-at-home orders increased the odds of violence at home. Individuals who lost their sources of income and experienced decreased financial stability could not provide for their families’ daily needs. Financial struggles predispose women to poverty and increase dependency on their aggressors. Also, economic devastation among women makes it strenuous for IPV victims to extricate themselves from their perpetrators, thus making them vulnerable to IPV. Stay-at-home orders resulted in limited movement and led to victims staying in isolation with their aggressors. The increase in time spent together may promote the chance for violence. The isolation may also make it cumbersome for victims to keep in touch with their friends and family, limiting access to social support. The isolation may also increase the opportunity for the perpetrator to control the victim's behavior, restrict access to needed goods at home, or monitor the victims’ phone calls. Before the pandemic, victims of IPV could seek housing, financial, and mental support at designated help centers such as community resource centers and shelters. These facilities were closed during the pandemic, making it difficult for victims to seek help outside their homes and thus increasing women's vulnerability to violence with their intimate partners.
This review showed that during the COVID-19 pandemic, individuals experienced new challenges that affected them physically, emotionally, and financially. Although the strict measures used during the pandemic to confine families at home brought families together and helped curtail the spread of the virus, it also worsened the risk factors for IPV. Hence, an increase in IPV was noted worldwide.28–30 The pandemic was an emerging factor that aggravated new IPV and existing problems. 2 A decrease in IPV was noted during COVID-19 compared to previous data. 13 Still, the authors suggested the reduction may be due to under-reporting resulting from stay-at-home orders whereby victims were locked in with their perpetrators and could not seek help.
A total of nine out of the 10 countries showed an increase in reported IPV (Spain, United States, Nigeria, Ethiopia, Turkey, Peru, Bangladesh, Czech Republic, and the Democratic Republic of Congo). Moderate to high-intensity restrictions were used in these countries, supporting the claim that restrictive measures were among the driving factors for increased IPV during the pandemic.
Spain
This review found that Spain instituted low-moderate intensity restrictions to curtail the spread of the COVID-19 virus, which led to obligatory confinement of IPV victims with their perpetrators, cohabitation with abusers, job instability, the continued presence of minors at home due to school closure, and social isolation. 29 More than a 45 percent increase in 016 calls (helpline calls) were documented compared to the same period in 2019 and not seen in any other quarter since 2015 in Spain. 25 Despite the increase in 016 calls, there was a decrease in IPV complaints, female fatalities, and protection orders granted, which may be due to under-reporting, reduced victim help-seeking, and variations in IPV reporting and responses. Other impact includes limited access to support sources such as health services and social organizations.
United States
The United States was among the countries reviewed that instituted moderate-high intensity restrictions during the pandemic leading to limited access to social amenities and victims isolated from their perpetrators. The incidence of IPV increased more than 1.8 times compared to previous years among women who sought emergency radiological imaging due to IPV. 13 Also, the total number of deep injuries in 2020 was 28 compared to 16 in 2017, and the total number of deep injuries per victim was 1.1 compared to 0.4 from 2017–2019. Although the incidence of high-risk abuse was two times greater in 2020, the number of patients who reported IPV decreased. Eighteen percent of study participants reported IPV, with 54 percent of the study sample reporting no change in victimization and 17 percent reporting exacerbated IPV. 20 During early COVID-19, sexual and physical violence spiraled among their study samples. 20
Nigeria
In Nigeria, IPV was already endemic in the country before the pandemic due to the cultural acceptance of IPV and the patriarchal system, 19 which favors gender inequality and gender-based violence at the country level. During the lockdown, Nigeria was among countries that instituted moderate-high risk restrictions to curtail the virus. The lockdown created new challenges for victims of IPV, including staying in isolation with their abusers, decreased access to social amenities, increased economic stressors, and lack of formal services that inhibited their ability to seek help. 19
Ethiopia
In Ethiopia, the unprecedented COVID-19 lockdown to tackle the virus's spread negatively impacted IPV. In Southern Ethiopia, the lifetime and past 12 months prevalence of women with IPV were 42.19 percent and 24.11 percent, respectively. 23 From this report, 18.2 percent, 36 percent, and 29 percent reported physical, emotional, and sexual violence, with 58 percent experiencing all three types of violence (emotional, sexual, and physical). This report agreed with a study in Northern Ethiopia. 26 The prevalence of IPV was reported as 24.6 percent 26 ; from this study, 8.3 percent, 13.3 percent, 8.3 percent, and 5.5 percent reported physical, psychological, and sexual violence, respectively. 26 IPV prevalence was reported as 22.4 percent 24 ; from this report, 11.0 percent, 20.0 percent, and 13.8 percent reported physical, psychological, and sexual abuse, respectively. All three studies were roughly in agreement with their findings. Besides the impact of COVID-19 restrictive measures, other independent risk factors reported by the authors include being illiterate, having an illiterate husband, having a substance-abusing husband, and having a community tolerant to IPV 24 ; age greater than or equal to 35 years, rural residence, husband's educational level, and low social support 23 ; and being a housewife, age less than 30, arranged marriage, and husband's age between 31–40 years old. 26
Turkey
Turkey instituted a national lockdown to combat the spread of COVID-19 on March 16, 2020. 17 It was noted that 35.55 percent of the participants reported IPV. 17 From this report, 10.1 percent, 32.2 percent, 4.0 percent, and 11.5 percent reported physical, psychological, sexual, and economic violence, respectively. Other predictive factors for IPV besides the pandemic included women with low education, being married, having children, unemployment, poor marital/relationship satisfaction, and increased workload in the household.
Peru
Peru was one of the countries hardest hit by the pandemic. The government instituted extended, extremely restrictive measures to mitigate the spread of the virus, 21 including national emergency, closed borders, mandatory social isolation, closure of schools, and restriction of movement. It was reported that 8.3 percent of the study sample experienced increased IPV and a 23.6 percent IPV increase among victims with a history of IPV. 21
Bangladesh
Bangladesh initiated a restrictive lockdown policy from March 26, 2020, to May 30, 2020 (for public and private offices, but educational institutions remained closed until October 2020). 22 The pandemic and restrictive measures caused severe psychological problems for the Bangladesh public, with IPV as a byproduct. Consequences of the restrictive measures include anxiety, financial difficulty, job loss, depression, and increased IPV. A Bangladesh organization, Manusher Jonno Foundation, reported 4,249 victims of domestic violence during April 2020, among whom 1,672 (39.35%) experienced IPV for the first time in their lives. 22 Also, husbands or intimate partners killed 107 women in Bangladesh, and total of 397 women were murdered due to IPV from January to September in 2020. 22 A study by Hamadani and colleagues 14 reported that more than 50 percent of women reported increased physical or sexual violence during the pandemic movement restriction. IPV prevalence was recorded as 45.29 percent. 22 From this report, 15.29 percent, 44.1 percent, 10.59 percent, and 19.22 percent reported physical, emotional, sexual, or physical or sexual abuse, respectively. 22 Other predictive risk factors include women aged 21–30 years, arranged marriage, rural area, low level of education, women's unemployment status, low family income, husbands aged 30–40 years, and husband's unemployment status.
Czech Republic
The Czech Republic was among the countries hardest hit by the pandemic, especially during the third wave (January to March 2021). It instituted high-intensity restrictions to curtail the spread of the virus. There was conflicting reporting of cases of IPV, with police reports indicating a decline in IPV while nonprofit organizations noted increased cases. 15 Before the pandemic, the Czech Republic had the highest IPV prevalence in central Europe, with 21 percent of Czech women experiencing physical or sexual violence in their lifetimes. 15 Three months before and during the first and second waves of COVID-19, women experienced exacerbated IPV exposure. 15 Other predictive risk factors noted by the authors include emotional support from a partner, the tension in a relationship, and the depression rate of the victim.
Democratic Republic of Congo
Restrictive lockdown measures were initiated by the Democratic Republic of Congo (DRC) on March 18, 2020. 18 Like most developing and low-income countries, IPV was endemic in the DRC before the pandemic and is correlated to gender dynamics and marital power inequities based on traditional norms. 18 In their study, 18 Ditekemena and colleagues reported that lockdown measures in the DRC exacerbated stress due to the confinement at home, loss of employment and income, and inaccessibility to social services, leading to increased IPV. The prevalence of IPV during the pandemic among the study group was 11.7 percent, and the predictive determinants of IPV in DRC include living in an urban area, belonging to middle and lower socioeconomic class, being pregnant, the uncertainty of pregnancy status, and belonging to the age groups 30–39 and greater than 50 years. 18
Kenya
Before the pandemic, IPV and gender-based violence were prevalent in Kenya, with an estimated prevalence of 27.2 percent for women aged 15–24. 9 Kenya instituted restrictive lockdown measures to reduce the spread of the virus. The report showed that the lockdown increased household tension, conflict, and violence. 9 In their study, Decker and colleagues 9 reported an IPV prevalence of 17 percent pre-pandemic, during the pandemic, and at 12-month and 18-month follow-ups, with an overall 27.6 percent of the study group experiencing IPV. Among young women partnered at all three time points (pre-pandemic, at 12 months following, and at 18 months follow-up), 66.2 percent stayed IPV-free (no IPV) and 9.2 percent saw IPV resolve by 18 months follow-up, while 11.1 percent had IPV start and 13.6 percent experienced intermittent IPV. Help-seeking for IPV and sexual violence increased in 2020 from 11.1 percent and 4.6 percent to 21.7 percent and 15.1 percent, respectively, by 2021. Predictive risk factors reported include pre-COVID employment status, low social support, and partner age difference over four years. 9
Six authors reported increased sexual violence against women amid COVID-19,9,17,20,22,24,26 highlighting the association of IPV against women with women's reproductive and sexual rights and affirming the need to foster policies that strengthen gender equality and services that ensure women's reproductive and sexual rights.
In society, women are assigned various roles that increase their vulnerability and exposure to conditions that dissipate their mental and physical well-being. 31 The studies reviewed showed that in the current pandemic, school closure, the need to work to provide for their family, and the need to care for sick family members caused many women to take on many roles of caregiver, family provider, and home-schooling, which may have predisposed them to other risk factors leading to IPV. 32 The confinement measures forced women to stay home with their aggressors and IPV perpetrators, precipitating IPV.32,33 Most women could not seek help, possibly due to the closure of facilities.
Limitation
There were minimal data for IPV incidence among minority populations such as the lesbian, gay, bisexual, transgender, and intersex (LGBTI) and black communities. Like many topics in maternal–child health, IPV faces measurement limitations, and this review is not exempt. First, some of the studies reviewed were based on self-reported surveys, calls to helplines, calls to organizations established to cater to violence, and emergency room visits, which poses an increased risk for bias and the inability to fully understand the actual incidence and prevalence of IPV due to possibility of underreporting. There is a possibility of limitation due to the measurement methods used by each researcher(s) due to the lack of a unified IPV measurement method. The inclusion criteria of using only studies written in English may eliminate other studies that may be relevant to the topic. Due to the context of IPV, there is a considerable possibility of underreporting due to stigma, labeling, and IPV normalization in certain cultures.
Conclusion
This review showed that IPV against women, a significant global and public health crisis, was exacerbated amid COVID-19 by the disease outbreak and the measures instituted to control it. Understanding the determinants of IPV and the effect of COVID-19 on IPV against women is essential for designing evidence-based, targeted interventions and programs to mitigate IPV against women in future pandemics.
Critical Findings
Evidence from increased calls to helplines, emergency room visits, national survey reports, and data from studies has shown that IPV against women was exacerbated by COVID-19 and strategies used to mitigate the pandemic.
The stay-at-home orders created unintended consequences that increased the risk factors for IPV and limited access to help:
victims were in constant contact with their perpetrators decrease in financial resources due to unemployment closure of amenities where victims can seek help
IPV increased among women with increased predisposing factors for IPV, such as financial burden, history of abuse, unemployment, uneducated spouse, and many children, among other factors.
IPV was underreported during the lockdown because victims were confined with their perpetrators.
Implications for Practice, Policy, and Research
There is a need to increase public education and awareness of IPV and available resources during a pandemic or national crisis, especially among cultures and communities where IPV is endemic.
There is a need to establish more IPV-preventing programs and support services.
Programs to foster and empower women's education and employment are needed to curtail financial burden, a significant risk factor for IPV.
The studies reviewed did not investigate the interventions for mitigating pandemic-related IPV in detail. As such, data on the effectiveness of such inventions still need to be discovered.
Future research could focus on understanding whether the interventions employed were effective and to what extent. Such knowledge will prepare public health practitioners for future pandemics and equip them with strategies to address IPV before, during, and after a pandemic.
Interventions Tailored to IPV Survivors Amid the Pandemic
Interventions included the following:
Use of standard code words denoting IPV at pharmacies, to connect with providers, and during telehealth Public campaign to raise awareness and information brochure for survivors Extra funding for social support services for IPV survivors Online support services to complement existing IPV helplines Extra funding to increase additional accommodation and shelters Protective rules for survivors, arrest and prosecution of perpetrators, and outreach policing for at-risk population Advice, guidelines, and information brochures for health care workers Government establishing a task force to observe for IPV during the pandemic
Resources for Victims’ Help-Seeking While Closure of Amenities During a Pandemic
National telephone helplines include:
Emergency Line 911 (United States) National Domestic Violence Hotline: Offers free and confidential 24/7 support and resources. Website: https://www.thehotline.org 1-800-799-SAFE (7233); TTY: 1-800-797-3224; Text “START” to 88788 National Resource Center on Domestic Violence
1-800-537-2238; www.nrcdv.org and www.vawnet.org Futures Without Violence: The National Health Resource Center on Domestic Violence
(415) 678-5500; www.futureswithoutviolence.org National Center on Domestic Violence, Trauma & Mental Health
1-312-726-7020 ext. 2011; www.nationalcenterdvtraumamh.org National Runaway Safeline
1-800-RUNAWAY or 1-800-786-2929; www.1800runaway.org Crisis Text Line (text HOME to 741741) National Sexual Assault Hotline: www.rainn.org
1-800-656-HOPE (4673)
Footnotes
Contributions
All authors contributed to the study's conception and design. Literature search and selection of articles for review were performed by IU and AA. Articles review and thematic analysis were conducted by IU, AA, and KBR. Initial draft of manuscript was written by IU and KBR. All authors commented on previous versions of the manuscript. All authors read and approved the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Baltimore City Health Department-VALUE Baltimore Vaccine Acceptance & Access Lives in Unity, Engagement & Education, Morgan State University Center for Urban Health Equity – Maternal, Child & Family Health Equity Initiative (grant number 527657).