
Abstract
Objectives:
Patterns of HIV transmission vary widely across demographic groups. Identifying and engaging these groups are necessary to prevent new infections and diagnose disease among people who are unaware of their infection. The objective of this study was to determine characteristics of newly diagnosed individuals across an entire state to determine patterns of HIV transmission.
Methods:
We evaluated data on people with new HIV diagnoses in Rhode Island from 2013 through 2015. We performed a latent class analysis (LCA) to identify underlying demographic and behavioral characteristics of people with newly diagnosed HIV.
Results:
Of 167 people with new HIV diagnoses interviewed in Rhode Island from 2013 through 2015, 132 (79%) were male, 84 (50%) were nonwhite, 112 (67%) were men who have sex with men (MSM), 112 (67%) were born in the United States, and 61 (37%) were born in Rhode Island. LCA revealed 2 major classes. Of the 98 people in class 1, 96% were male, 85% were MSM, 80% were white, 94% were born in the United States, and 80% believed they acquired HIV in Rhode Island. Class 2 was 63% male and 69% Hispanic/Latino; 29% were born in the United States, and 61% believed they acquired HIV in Rhode Island.
Conclusions:
Most new HIV diagnoses in Rhode Island were among MSM born in the United States, and a substantial number were likely infected in-state. People with newly diagnosed HIV who were foreign-born, including Hispanic/Latino and heterosexual groups, were less likely to have acquired HIV in Rhode Island than were MSM. HIV prevention approaches, including pre-exposure prophylaxis, should be adapted to the needs of specific groups. Rhode Island offers lessons for other states focused on eliminating HIV transmission.
HIV is a public health concern in the United States, and disparities persist across geographic regions and racial/ethnic, sexual, and gender minority populations. 1 Of the estimated 39 782 people newly diagnosed with HIV in 2016 in the United States, 26 570 (67%) were gay, bisexual, or other men who have sex with men (MSM), and 69% were black or Hispanic/Latino. 1 Recent data indicate a lifetime HIV risk of 1 in 2 for black MSM and 1 in 5 for Hispanic/Latino MSM. 2 Eliminating HIV in the United States requires addressing regional microepidemics, developing treatment and prevention approaches that respond to local transmission patterns, engaging sexual networks, and focusing on geographic clustering of infections. 3,4
In 2014, UNAIDS (Joint United Nations Programme on HIV/AIDS) announced an aggressive initiative to eliminate HIV with the “90-90-90” campaign, which included the goals that 90% of HIV-positive people will know their status, 90% of those diagnosed will be engaged in antiretroviral therapy (ART), and 90% of those receiving ART will be virally suppressed by 2020. 5 Understanding local epidemiology is critical for achieving the 90-90-90 goals given that HIV transmission patterns vary widely by race/ethnicity and geographic location. In 2015, Rhode Island reported 65 new HIV diagnoses, down from a peak of 125 in 2009, the highest number of diagnoses in the past decade. Also in 2015, Rhode Island endorsed the UNAIDS 90-90-90 campaign with new commitments to allocate resources to promote HIV testing, prevention, and treatment efforts.
An estimated 89% of HIV-positive people in Rhode Island had received a diagnosis, 67% of those who received a diagnosis had been engaged in care, and 85% of those engaged in care were virally suppressed as of 2015. 6 These achievements likely stem from the state’s longstanding commitments to needle-exchange programs, 7,8 linking prisoners to treatment during incarceration and upon release, 9,10 and an HIV care model in which most care and treatment is provided in one central setting. 11 In addition, close collaborations among the state health department, clinical centers, and academic institutions have led to statewide HIV prevention initiatives among marginalized populations, and recent advances in HIV prevention and care approaches—including treatment as prevention (TasP) 12 and pre-exposure prophylaxis (PrEP) 13 –16 —have been implemented across the state. 17 –20 Other prevention approaches include improving access to care and conducting routine HIV testing, the cornerstones of the test-and-treat model to achieve viral suppression and reduce transmission. 21 –23
To inform ongoing efforts to achieve the UNAIDS 90-90-90 goals in Rhode Island, we attempted to interview all people with newly diagnosed HIV in the state from 2013 through 2015. We evaluated their demographic and behavioral characteristics and identified targets for HIV prevention and treatment efforts.
Methods
A total of 236 people received a diagnosis of HIV in Rhode Island from January 1, 2013, through December 31, 2015. We recruited people with new diagnoses from all major HIV outpatient clinics in the state. Those who provided informed consent participated in a one-time structured interview designed to collect demographic, behavioral, and clinical data. We collected the following data: (1) demographic characteristics, including age, sex, race, ethnicity, place of birth, education level, annual income, and insurance coverage; (2) behaviors in the 12 months before HIV diagnosis, including substance use, number and sex of sex partners, frequency of condom use, and locations for meeting sexual partners (eg, bar, club, bathhouse, online); and (3) clinical data, including history of mental illness, history of other sexually transmitted diseases (STDs), date of last negative HIV test result, when and where the person believed he or she acquired HIV, CD4 cell count, history of opportunistic infections, and previous signs and symptoms consistent with acute retroviral syndrome. Based on self-report and a review of medical records, we categorized HIV-infected people by likely HIV transmission risk behavior, including MSM, male who has sex with females, female who has sex with males, or person who injects drugs.
We categorized the most likely place of residence at suspected time of HIV infection as follows: living in Rhode Island and infected in-state, living in Rhode Island but infected in another state or country, living and infected in another state, and living and infected in another country. We conducted descriptive analyses of demographic and behavioral data stratified by sexual behavior and residence at suspected time of infection. We defined significance in all analyses as a 2-tailed P < .05 based on Pearson χ tests; we used Fisher exact tests when expected cell counts were <5. This study was approved by the Miriam Hospital Institutional Review Board.
We used latent class analysis (LCA) to identify distinct groups of newly diagnosed people based on demographic and behavioral characteristics. LCA is a statistical approach that generates classes based on patterns of data with the goal of identifying clusters, or groupings, of people with similar characteristics. 24 We used Mplus version 7.1 to test a series of LCA models with 1 to 4 classes. 25 To avoid the likelihood of converging on a local maximum, we generated 500 start values for each model. To determine the optimal LCA solution, we used the following indices: the Akaike information criterion (AIC), the sample-size-adjusted Bayesian information criterion (BIC), and the bootstrap likelihood ratio test (BLRT) for model fit. The BLRT tests the null hypothesis of no improvement in fit for the model under consideration compared with a model with 1 fewer class. The analysis also considered entropy, which measures the extent to which classes are distinct from each other, average posterior probability of class membership, and interpretability of the classes; entropy values range from 0 (no separation) to 1 (perfect separation).
Variables used in the LCA included sex, age, race/ethnicity, insurance status, education level, annual income, place of birth, and residence at suspected time of infection, with MSM behavior included as a covariate. Outcomes of primary interest included route of transmission, substance use, lifetime STD history, frequency of condom use, number of partners in the 12 months before HIV diagnosis, previous HIV testing, concurrent HIV and AIDS diagnoses, and where individuals met their sexual partners. After identifying the LCA model with the optimal number of classes based on these criteria, we used Pearson χ2 tests to compare classes on behavioral outcomes. We calculated odds ratios (ORs) and 95% confidence intervals (CIs) for each comparison.
Results
We interviewed 167 of 236 (71%) people who received a diagnosis of HIV in Rhode Island from 2013 through 2015. Of the 167 people with newly diagnosed HIV, 132 (79%) were non-transgender male, 84 (50%) were nonwhite, 53 (32%) were Hispanic/Latino, and 80 (48%) reported an annual income of <$12 000 (Table 1). Most new diagnoses (n = 112, 67%) were among MSM, followed by females who have sex with males (16%), males who have sex with females (14%), and people who inject drugs (2%). Seventy-one (43%) people reported ≥4 sexual partners in the 12 months before diagnosis, and 60 (37%) reported rarely or never using condoms. Forty-five (27%) people had not been tested for HIV before diagnosis; 49 (29%) had AIDS at the time of diagnosis. Thirty-five (21%) people had a concurrent STD at the time of HIV diagnosis. MSM with newly diagnosed HIV were significantly more likely to be younger, be white, have a higher education level and income, have more sexual partners, and use condoms more frequently than non-MSM in the sample.
Demographic and behavioral characteristics of a sample of individuals newly diagnosed with HIV in Rhode Island, 2013-2015
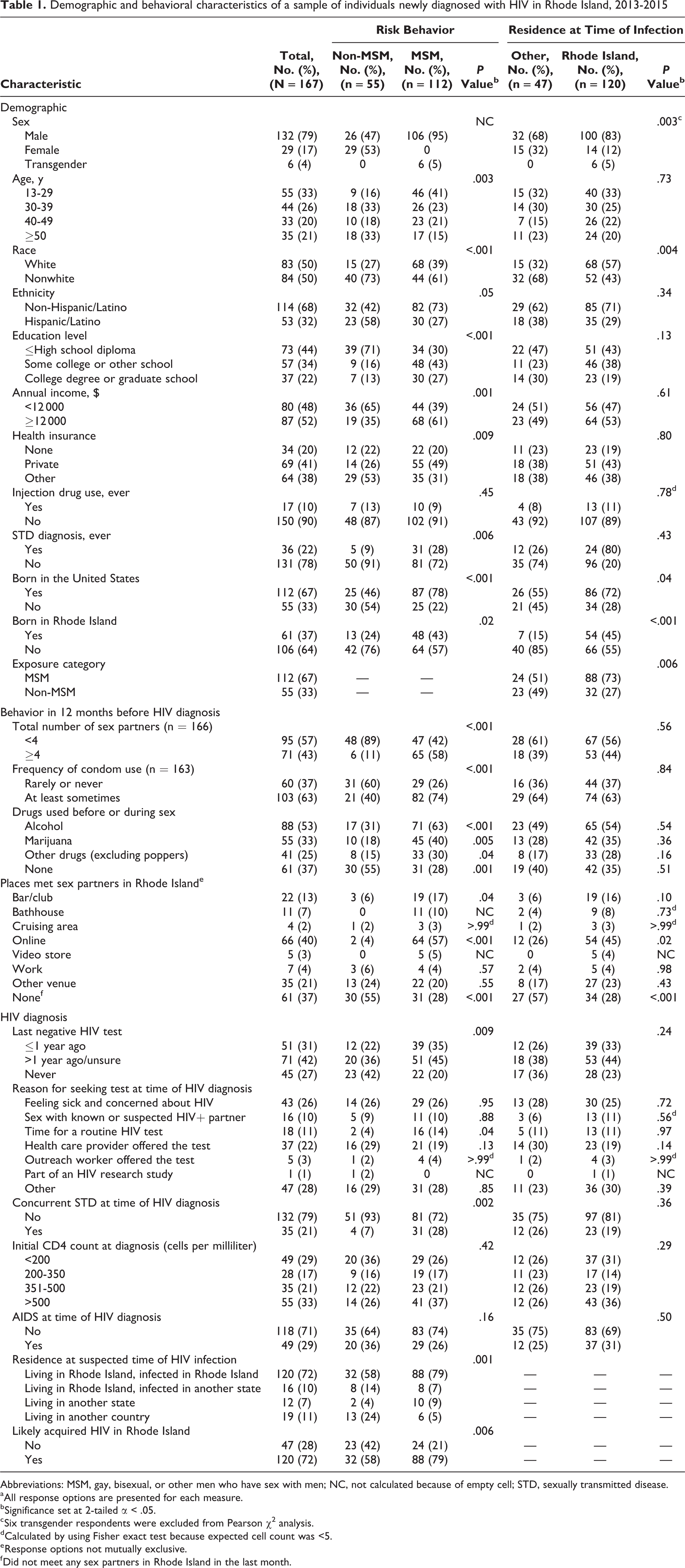
Abbreviations: MSM, gay, bisexual, or other men who have sex with men; NC, not calculated because of empty cell; STD, sexually transmitted disease.
a All response options are presented for each measure.
b Significance set at 2-tailed α < .05.
c Six transgender respondents were excluded from Pearson χ2 analysis.
d Calculated by using Fisher exact test because expected cell count was <5.
e Response options not mutually exclusive.
f Did not meet any sex partners in Rhode Island in the last month.
Of the 167 newly diagnosed people, 112 (67%) were born in the United States, and 61 (37%) were born in Rhode Island (Table 1). One hundred twenty (72%) people were living in Rhode Island and believed they acquired HIV in-state, 16 (10%) people were living in Rhode Island and believed they acquired HIV elsewhere, 12 (7%) people were living in another state at the suspected time of infection, and 19 (11%) were living in another country at the suspected time of infection. Compared with non-MSM, MSM were more likely to be born in Rhode Island (n = 48/112 [43%], P = .02) and infected in Rhode Island (n = 88/112 [79%], P = .001). Those who believed they acquired HIV in Rhode Island were more likely than those who believed they did not acquire HIV in Rhode Island to be white, born in the state, and report meeting sex partners online in the 12 months before diagnosis.
In the LCA, comparison of overall model fit indices demonstrated that a 2-class solution was preferable (Table 2). Compared with the 1-class model and the 3-class model (a 4-class model did not converge), the 2-class solution provided low BIC and AIC values and good entropy (0.84). The 2-class model also showed a substantial improvement in fit compared with the 1-class model, according to the BLRT. Although the AIC was slightly lower in the 3-class model than in the 2-class model, the BLRT suggested no substantial improvement in fit for the 3-class model compared with the 2-class model. The average probability of latent class membership was 0.96 for class 1 and 0.95 for class 2.
Fit indices for 1-class, 2-class, and 3-class models in a latent class analysis of a sample of individuals with newly diagnosed HIV in Rhode Island, 2013-2015
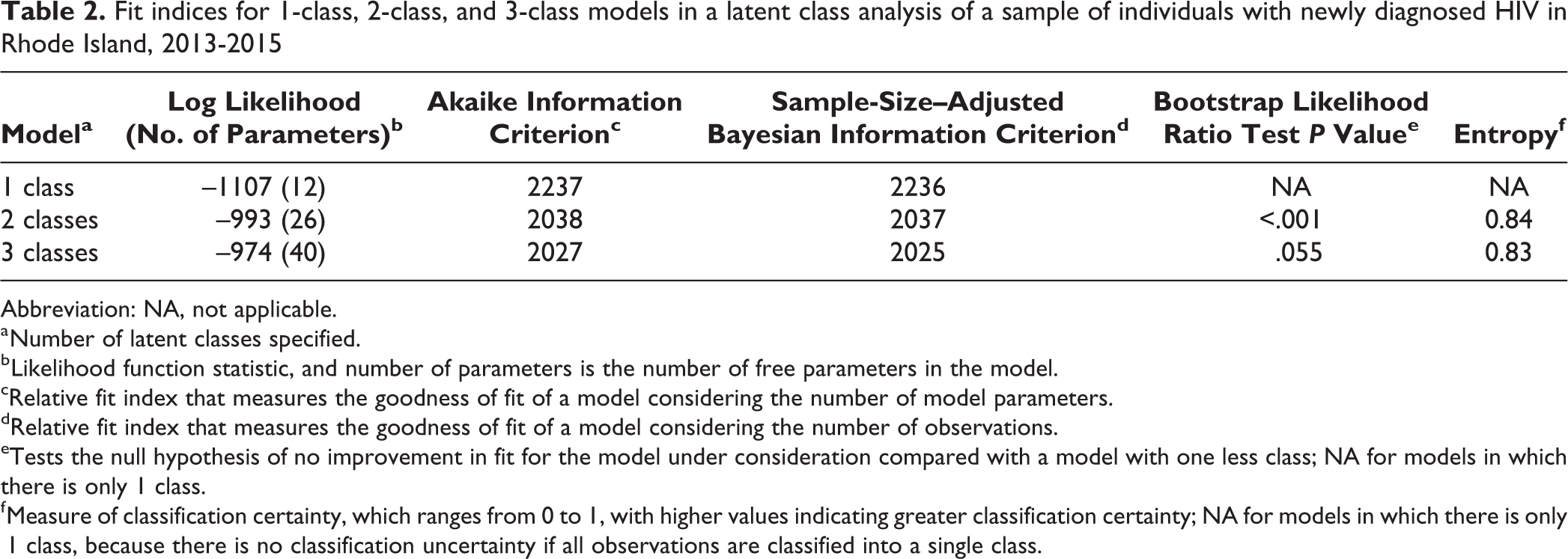
Abbreviation: NA, not applicable.
a Number of latent classes specified.
b Likelihood function statistic, and number of parameters is the number of free parameters in the model.
cRelative fit index that measures the goodness of fit of a model considering the number of model parameters.
dRelative fit index that measures the goodness of fit of a model considering the number of observations.
eTests the null hypothesis of no improvement in fit for the model under consideration compared with a model with one less class; NA for models in which there is only 1 class.
f Measure of classification certainty, which ranges from 0 to 1, with higher values indicating greater classification certainty; NA for models in which there is only 1 class, because there is no classification uncertainty if all observations are classified into a single class.
LCA item probabilities indicated that class 1 (59% [98/167] of the cohort) was 96% male, 85% MSM, and 80% white; 94% were born in the United States, and 80% believed they were infected in Rhode Island. Class 2 (41% [69/167] of the cohort) was 37% female and 69% Hispanic/Latino; 29% were born in the United States, and 61% believed they were infected in Rhode Island (Table 3). Those in class 1 were significantly more likely than those in class 2 to be MSM (OR = 8.35; 95% CI, 2.48-27.94; P = .001), have met sexual partners online (OR = 3.07; 95% CI, 1.05-8.98; P = .04), and have a concurrent AIDS diagnosis (OR = 2.90; 95% CI, 1.05-8.05; P = .04) (Table 4).
Probabilities of variables used in the 2-class solution in a latent class analysis of people with newly diagnosed HIV in Rhode Island, 2013-2015
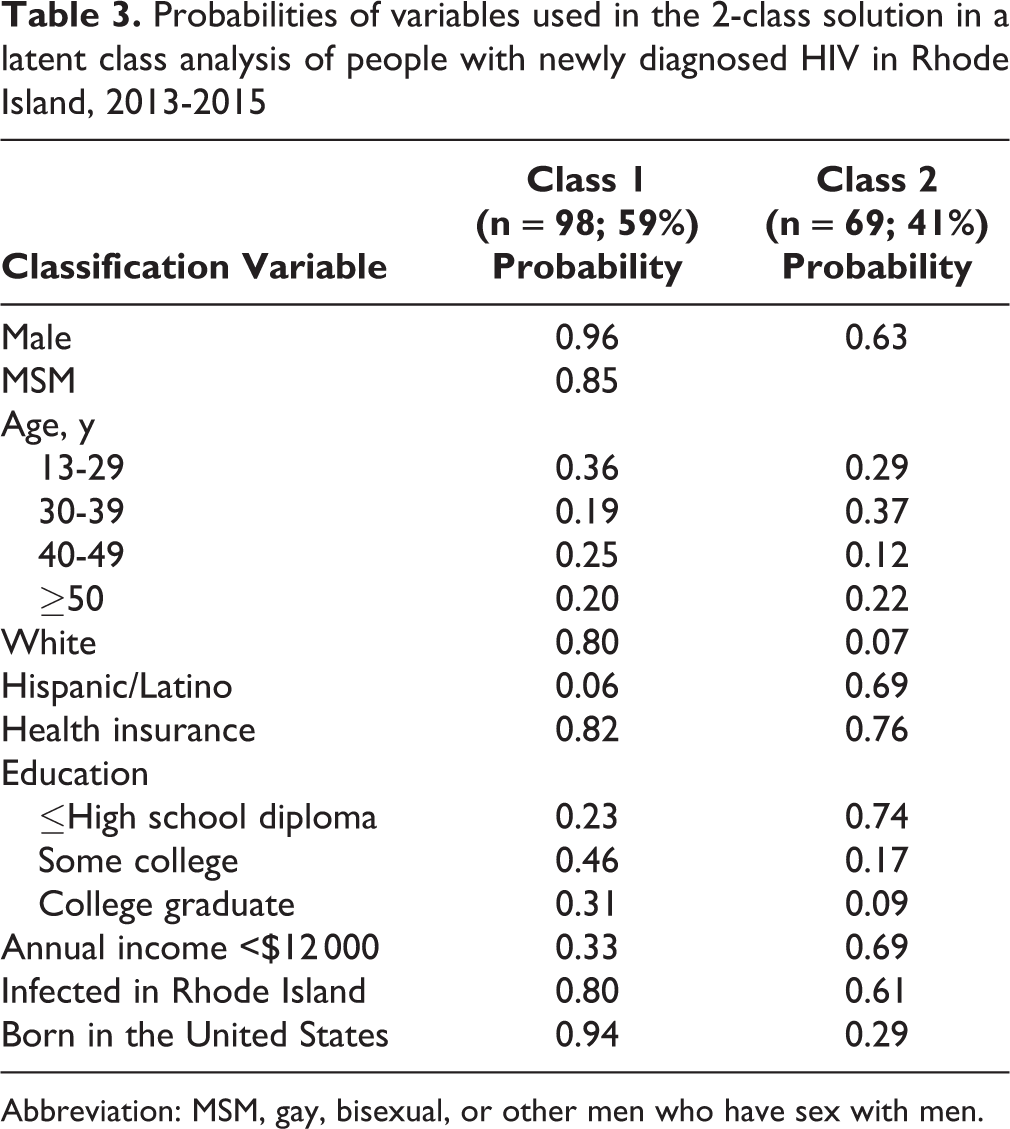
Abbreviation: MSM, gay, bisexual, or other men who have sex with men.
Latent class characteristics and logistic regression odds ratios for differences between classes in a latent class analysis of individuals with newly diagnosed HIV in Rhode Island, 2013-2015
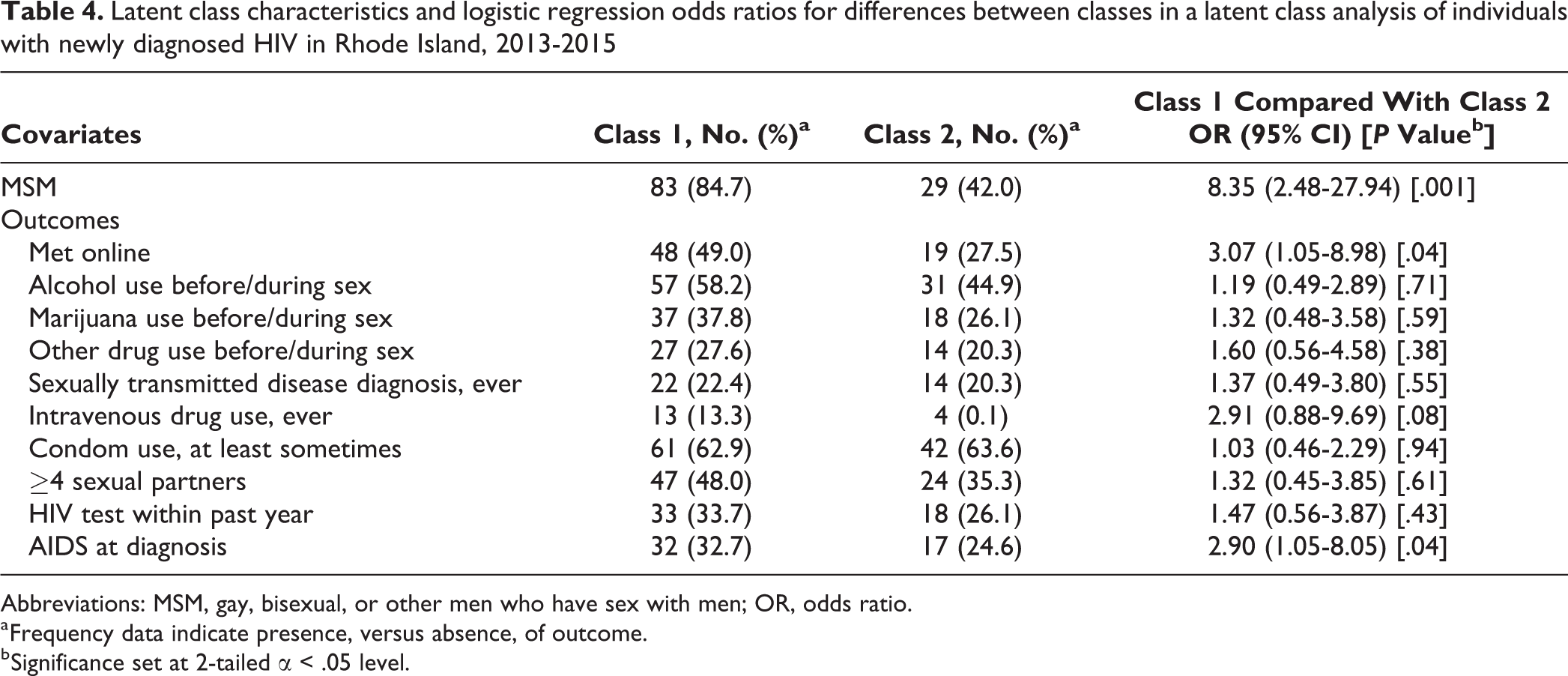
Abbreviations: MSM, gay, bisexual, or other men who have sex with men; OR, odds ratio.
a Frequency data indicate presence, versus absence, of outcome.
b Significance set at 2-tailed α < .05 level.
Discussion
This comprehensive attempt to characterize all new HIV diagnoses in Rhode Island is among the first statewide efforts to evaluate detailed clinical, demographic, and behavioral characteristics of this population across an entire state. The analysis revealed 2 main classes of people who constitute most new HIV diagnoses in Rhode Island. Class 1 consisted mainly of white MSM born in the United States and those who believed they acquired HIV while living in Rhode Island. In Rhode Island as well as nationally, new HIV diagnoses disproportionately affect MSM. 1 Class 2 consisted of mostly foreign-born and Hispanic/Latino people who believed they acquired HIV outside of Rhode Island.
The characteristics of class 1 also reflected the mostly white racial/ethnic distribution of the state population. However, rates of new HIV diagnoses were disproportionately higher among African American/black and Hispanic/Latino populations compared with white populations in Rhode Island in other studies. State surveillance data from 2015 demonstrate that, when compared with the rates among white people, the rates of HIV were 9 times higher among people who were black/African American and nearly twice as high among Hispanic/Latino populations. 6 In our study, 69% of members of class 2 were Hispanic/Latino, and only 29% were born in the United States. By comparison, foreign-born people constituted 13% of the total Rhode Island population during 2008-2012 26 and 16% of new HIV diagnoses annually in the United States during a similar period (2007-2010). 27 In our study, compared with members of class 1, members of class 2 were more likely to be female, to identify heterosexual behavior as the main risk factor for HIV infection, and to have been infected outside the United States.
Our study also demonstrated a low prevalence of injection drug use among those with a new diagnosis of HIV. This finding is consistent with the low number of new HIV diagnoses attributed to injection drug use during the past decade in Rhode Island (<5 per year), a change attributed to needle-exchange programs and other harm-reduction initiatives in this group. 28 However, close surveillance is needed given the widespread use of opioids across the state.
Despite Rhode Island’s small size and dense population (1.1 million residents spread across 1200 square miles 28 ) and close proximity to several other states, nearly 75% of people in the cohort indicated living in Rhode Island at the time they believe they were infected. The population density and close proximity of Rhode Island to neighboring New England states facilitate travel between states, which in turn creates opportunities for out-of-state HIV infections or in-state infections with an out-of-state origin. One reason for the high prevalence of in-state infections may be that, despite the ease of interstate travel, most US residents reside in their state of birth. 29 Previous studies also indicate that high-risk populations from surrounding regions may travel to Rhode Island to engage in both transactional and non-transactional sex. In a 2012 study, more than half of MSM recruited from a Rhode Island sex venue were from out of state. 30 Rhode Island has had lax regulations on sex work in the past and is host to a substantial number of sex venues (eg, pornographic video stores, bathhouses, sex clubs).
In our study, MSM reported a high frequency of sexual and substance use risk behaviors, along with infrequent HIV testing. Together, these factors may contribute to an increased risk of local transmission among MSM. 31,32 Class 1 findings indicate numerous points for public health intervention, including condom distribution, counseling and education, PrEP implementation, and partner notification services. Among those likely infected outside of Rhode Island, the primary public health approach should include early diagnosis and linkage to care, via routine opt-out testing and outreach efforts. In addition, to address HIV diagnoses among those in class 2, these efforts may need to focus on those who are female, Hispanic/Latino, and at risk of heterosexual HIV transmission.
With only 65 new HIV diagnoses in 2016, Rhode Island is among the states closest in the nation to achieving the 90-90-90 goals and is surpassing national estimates for diagnosis, retention in care, and viral suppression. 33 Based on our results, achieving these goals will require keen focus on 2 priority populations: MSM who meet their sexual partners online and foreign-born populations who may acquire HIV outside the state (in another state or country). These 2 groups require distinct interventions and public policy responses. Interventions designed to prevent HIV transmission (such as PrEP) may be most applicable for MSM, as characterized in class 1. At least half of newly diagnosed MSM in Rhode Island meet their partners online, 34 highlighting public health opportunities to reach this population before infection. Conversely, the findings from class 2 indicate a need for efforts to promote early diagnosis and engagement in HIV care, which may be more salient for immigrant populations who acquire HIV outside of Rhode Island. Test-and-treat strategies would likely benefit both groups.
Limitations
Our study had several limitations. First, we were unable to interview all people with newly diagnosed HIV during the study period, which may have affected the demographic and behavioral results. Second, we relied on self-report for data on residence at suspected time of HIV infection, which is subject to recall bias. Third, some Rhode Island population demographic characteristics may limit the generalizability of our findings to other settings. However, our sample represents most HIV diagnoses statewide during the study period, an accomplishment facilitated in part by the small size and highly centralized HIV care system in the state. In addition, we attempted to verify approximate dates of diagnosis by collecting data about last HIV test date and date of immigration to help determine when a given person may have acquired HIV. Finally, the application of LCA was a novel approach to analyzing these data. Thus, although demographic characteristics of populations and HIV diagnoses vary by state, our findings from Rhode Island provide a model for characterizing risk groups to target public health interventions.
Conclusion
Our findings suggest that achieving the 90-90-90 goals and eliminating HIV in Rhode Island will require distinct, focused efforts among 2 groups: (1) MSM, many of whom report high-risk sexual and substance use behaviors and meet their partners online, and (2) foreign-born and Hispanic/Latino people with heterosexual transmission risk, who may acquire HIV outside of Rhode Island. By informing the delivery of behavioral and biomedical interventions to groups most likely to benefit from them, our findings can help prioritize public health approaches in a state that is close to eliminating HIV transmission.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Philip A. Chan was supported by the National Institute of Allergy and Infectious Diseases grant K23AI096923. Additional support was provided by the Providence/Boston Center for AIDS Research (P30AI042853 and R25 MH083620).