
Abstract
Great strides have been made globally toward ending HIV and AIDS as a threat by 2030, although the rate of new HIV infections among men who have sex with men remains very high. Due to their risk of getting HIV and AIDS, utilization of pre-exposure prophylaxis (PrEP) can potentially reduce the risk of HIV transmission among this population. This study sought to analyze the accessibility, knowledge, and potential barriers and facilitators to assessing PrEP by men who have sex with men. The quantitative method was conducted on 65 men who have sex with men through questionnaires loaded on Kobo Collect. Chi-square test, odds ratios, and logistic regression were used to associate different demographic characteristics with knowledge and significance of barriers in PrEP access using STATA 15. A hotspot map of PrEP and locations was created using QGIS. About 84% of respondents accessed pills from friendly facilities. The remaining accessed them from public hospitals, namely Mpilo and United Bulawayo Hospitals. Over 90% of the respondents were found to be highly knowledgeable. Notably, barriers included lack of information, fear of side effects, pills not accessible, pill taste, odor and size, stigma, and lack of protection from other sexually transmitted infections. Facilitators were educated about PrEP, the existence of friendly health facilities, making pills available at all times, partner support, increased number of friendly health facilities and support groups. Maximizing the potential of PrEP as an efficient HIV-prevention intervention among this population requires ongoing efforts to remove barriers and promote facilitators.
Background
Human immunodeficiency virus (HIV) and acquired immunodeficiency syndrome (AIDS) have been a global concern for the last four decades as it is chronic and without an effective cure. This means that once a person gets the virus, they will have it for life (Centers for Disease Control and Prevention [CDC], 2022a). With proper and good medical care, HIV progression can be effectively managed, that is, as much as it cannot be cured, the progression from being infected with HIV to developing full-blown AIDS can be significantly delayed (Adeagbo et al., 2021; CDC, 2022a). An HIV-infected person can transmit the virus to another person through anal or vaginal sex and by sharing needles and syringes or other drug injection equipment (Adeagbo et al., 2021; CDC, 2022a). One of the critical strategies used to delay the virus’s progression and onset of full-blown AIDS has been the use of viral suppressants (Cusini et al., 2013). Pre-exposure prophylaxis (PrEP) has become integral in reducing the chances of the spread of HIV and has been extended to men who have sex with men (MSM). The World Health Organization (WHO) and the CDC recommend that individuals at substantial risk of acquiring HIV, including MSM, should take PrEP to minimize their chances of acquiring and transmitting HIV.
PrEP is an HIV-prevention method in which HIV-negative people take a daily pill to reduce their risk of becoming infected if they engage in risky sexual behaviors (McCormack et al., 2016; WHO, 2015a). When used consistently, PrEP has been shown to reduce the risk of HIV-1 infection among adult men and women at very high risk of HIV infection through sex or injection drug use. PrEP is typically used as part of a combination approach that includes regular HIV testing, condom use, and other risk-reduction strategies (UNAIDS, 2016a, 2016b). Significant progress has been made in preventing new HIV infections, although HIV transmission among MSM remains challenging (UNAIDS, 2016a, 2016b). Many countries have laws prohibiting same-sex sexual relations, and Pérez-Jiménez et al. (2009) noted that most interventions for people living with HIV have focused largely on heterosexuals in Latin America and Sub-Saharan Africa (Khozah & Nunu, 2023). There is a significant lack of programmatic intervention research to address self-management among this population.
PrEP was approved in 2012 by the Food and Drug Administration (FDA, 2019). WHO recommended PrEP as an HIV-prevention method for high-risk groups, including lesbians, gays, bisexuals, transgender, intersex, asexual, and others (LGBTQIA+). PrEP is now a widely used biomedical intervention, such as oral PrEP and microbicides, available in health care centers worldwide (WHO, 2015b). Three types of PrEP are available: daily oral PrEP, on-demand PrEP (take the pill before and after sex), and long-acting injectable PrEP (Cao et al., 2020). According to Saul et al. (2018), oral PrEP was introduced in 2015 in Zimbabwe as a strategy to reduce HIV incidence among adolescent girls and young women (Saul et al., 2018). PrEP was then expanded to key populations, particularly MSM, transgender people, sex workers, and serodiscordant couples (Saul et al., 2018). Based on the evidence of several clinical trials, PrEP is highly effective in reducing the risk of HIV transmission through sexual intercourse by 99% (CDC, 2022b). However, inconsistency in the uptake of PrEP compromises its effectiveness (Koenig et al., 2013). Different economic, structural, psychological, and social factors influence PrEP uptake and adherence (Liu et al., 2017). Factors negatively affecting PrEP uptake and acceptability include stigma, social norms and beliefs, lack of social support, poverty, and poor health care services (Hood et al., 2016).
According to LGBT+ PRIDE 2021, Global Survey (Ipsos, 2021) targeting about 19,069 adults aged between 18 and 74 years, 80% of the global population identify as heterosexual, 3% as gay or lesbian, 4% as bisexual, 1% as pansexual, 1% as asexual, 1% as other, and 11% do not know or did not say (Pride). Although the LGBTIQ+ community constituted a small percentage of the global population in 2019, 62% of the new infections were among LGBTIQ+ and their partners (UNAIDS, 2019). Many countries have laws criminalizing same-sex sexual behavior, including Zimbabwe. UNAIDS (2019) alludes that MSM living in these countries are five times more likely to live with HIV than countries that do not criminalize same-sex sexual behavior. The reported risk of acquiring HIV was 26 times higher for gay men and MSM than for the rest of the adult male population in 2019 (UNAIDS, 2019). It is reported that approximately 25% of the new infections in Africa were from LGBTIQ+ and their partners in 2018 (UNAIDS, 2019). UNAIDS 2019 Data Report indicates that Sub-Saharan Africa is still the epicenter of the HIV epidemic, with an HIV prevalence of 17.9% in MSM (UNAIDS, 2019).
According to UNAIDS (2019), Zimbabwe had 31% HIV prevalence among MSM, yet the Ministry of Health and Child Care states that information on HIV prevalence among MSM is unknown (UNAIDS, 2019). These numbers are alarming, hence the need for MSM to access sexual and reproductive health services (SRHS) because curbing the HIV epidemic cannot be possible without reaching this population (Gupta & Granich, 2017). Accessing SRHS such as PrEP by MSM in Bulawayo is highly influenced by barriers such as discrimination, stigma and social exclusion (Moyo et al., 2021), and the existence of public health care facilities that have no standardized services that cater for the needs of MSM (Munyimani & Nunu, 2022). This research article aims to explore the accessibility of PrEP, knowledge of PrEP among MSM, potential barriers, and facilitators to improve PrEP uptake among this population.
Methodology
Study Area
The study was conducted in the Bulawayo Metropolitan Province. The area under study has an estimated population of 665,940 (Zimstat, 2022). It is the second largest city in Zimbabwe and is considered a very busy town with diverse communities. According to the HIV and STI Biobehavioral Survey (2020), Bulawayo has 763 MSM. Both public and private health facilities serve the city, with most of these facilities owned and operated by the government (HIV and STI Biobehavioral Survey, 2020). The city is home to many clinics run by the Ministry of Health and Child Care and Bulawayo City Council and three referral hospitals, including United Bulawayo Hospitals, Mpilo Central Hospital, and an inpatient mental health facility called Ingutsheni Hospital. In the city, the private sector also manages many health care facilities. The Study Area map is presented in Figure 1.

Study Area Map
Study Design
A quantitative cross-sectional survey was conducted on MSM in Bulawayo. This design enabled the researcher to explore relationships between different variables on PrEP accessibility, knowledge, barriers, and facilitators that influence PrEP utilization among this population.
Target Population
The study population consisted of MSM in Bulawayo. The inclusion criteria for the study were MSM, aged 18 years or older, and assigned male sex at birth. Respondents younger than 18 were excluded from the study as they needed parental consent and might not give accurate responses due to fear and insecurity. The study also identified and mapped all health care facilities that provide PrEP services to MSM.
Sampling
A sample size calculator, RAOSOFT, was used to calculate the sample size at a 90% confidence interval, 10% margin of error, and 50% response distribution. According to the HIV and STI Biobehavioral Survey (2020), Bulawayo has 763 MSM, and the sample size was 63 (HIV and STI Biobehavioral Survey, 2020). To gain access to this population (MSM), the Sexual Rights Centre (SRC) (an organization that provides services for MSM and runs support groups for this community) assisted in the recruitment of respondents. Respondents were chosen using systematic sampling from databases of the SRC. However, some respondents were purposively selected to participate in the study. Snow-balling was also used to identify other potential respondents through the network of respondents. The respondents were asked to invite other members of MSM who met the inclusion criteria to participate in the study if they were interested. The health care facilities were selected by purposive sampling because they have offered PrEP before.
Data Collection Procedure and Tools
Structured Questionnaire Guide
A structured questionnaire was designed and deployed using KoboToolBox. KoboToolBox is an open and free open-source suite tool used for field data collection and data storage (Lakshminarasimhappa, 2022; Poloju et al., 2022). The KoboToolBox facilitates data collection for researchers by utilizing an online platform that collects, stores, and aggregates data (Poloju et al., 2022). This platform replaces the paper-based traditional way of collecting data by using smart gadgets linked to a private online server that is only accessed by the researchers through created passwords (Poloju et al., 2022). It is a widely used tool for monitoring and evaluating programs (Poloju et al., 2022). The questionnaire was developed on Microsoft Word and then imported/deployed onto the KoboToolBox. The questionnaire had four sections as informed by the outcome of a qualitative survey that was conducted before this research; the first probed on the socio-demographic characteristics, the second focussing on knowledge, the third probed on the barriers, and the fourth probed on the facilitators to the uptake of PrEP by MSM. The tool was developed in English and translated into Ndebele and Shona, the most spoken languages in the province. The tool was pretested and translated from the local languages to English to determine if the questions retained the original meaning regardless of the language used in data collection.
Geographic Information System
A site visit to the MSM centers providing PrEP services was done. Coordinates of the location of these health care facilities that offer PrEP services were captured using the Kobo Collect tool Global Positioning Systems (GPS). Also, the addresses of the respondents were captured using the Kobo Collect tool and mapped against the PrEP services offered. A hotspot map of PrEP facilities to show the spatial distribution of the preferred facilities using the number of respondents who reported accessing their PrEP from those facilities was created using QGIS. GPS data points were captured twice with two different devices to ensure the consistency and reliability of the data.
Data Analysis
Quantitative data collected using the Kobo Collect Tool were exported to Excel to generate graphs on barriers and facilitators of PrEP. Knowledge levels were assessed using ten questions with predetermined responses, some correct and some wrong. A correct response was scored 1, and an incorrect response was scored 0, with higher scores indicating that the respondent was knowledgeable. A Likert-type scale adopted from other authors guided the analysis with a person scoring between 0 and 5 correct answers deemed not knowledgeable and those scoring six and above deemed knowledgeable (Mudonhi et al., 2020; Nunu et al., 2018). Chi-square tests assessed the relationship between demographic characteristics and knowledge levels. A simple logistic regression odds ratio was used to assess differences in age, gender, and education on knowledge of PrEP at a 95% confidence interval. These statistical analyses were conducted using Stata 15, and statistically significant differences were considered when a p value < .05 was obtained. GPS points were uploaded to QGIS and overlaid with other shape files.
Ethics Consideration
An application for ethical approval was lodged with the institutional review board. This committee granted ethics clearance. An information and consent sheet was developed and shared with respondents who went through and had the opportunity to seek clarification on issues they did not understand relating to the study. After this, they provided written consent before they participated in the research. It should be noted that participation was voluntary, and no one was coerced to participate.
Findings
Socio-Demographic Characteristics
The sample included 65 MSM, and the mean age of the respondents was 28.85 years. Most MSM identified as gay (34: 52.3%), while most were Black (53: 81.5%). Other socio-demographic information of the respondents is presented in Table 1.
Socio-Demographic Characteristics of Respondents

Note. (f) represents frequency. PrEP = pre-exposure prophylaxis.
Spatial Distribution of MSM and MSM Facilities
Main facilities noted to offer PrEP services include the SRC, Population Solutions for Health, United Bulawayo Hospital and Mpilo Hospital. The spatial distribution of MSM locations and MSM facilities is presented in Figure 2.
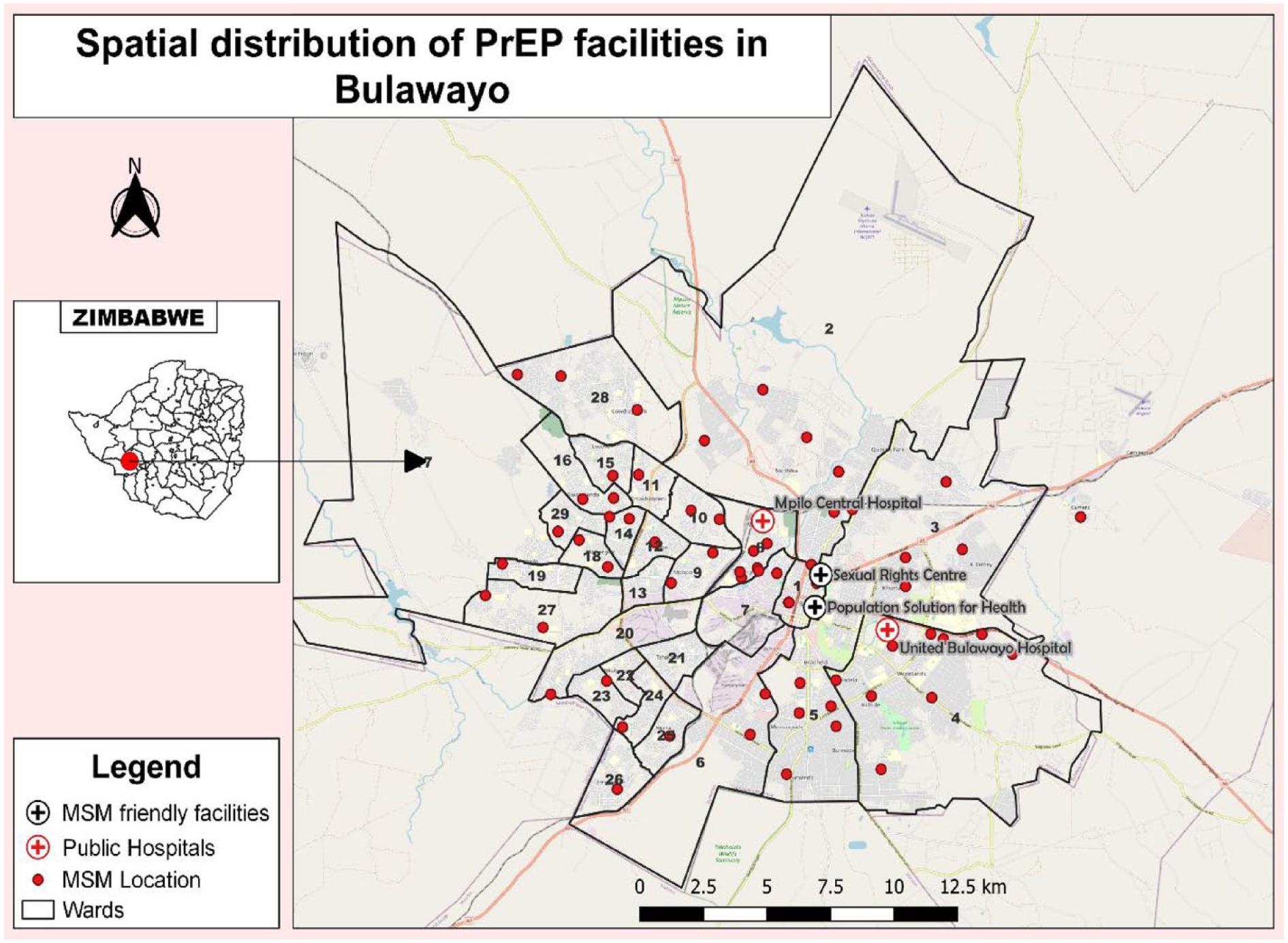
Spatial Distribution of MSM Against PrEP Facilities in Bulawayo
Hotspot Map of Where MSM Access PrEP and Location
MSM was highly concentrated in wards 8, 7, 12, 11, 18, and 15. MSM’s preferred PrEP facility was SRC (36: 55%) and Population Solutions for Health (19: 29%). Public hospitals (10: 16%) were this population’s least preferred facilities to access PrEP. The hotspot map of MSM distribution and where MSM access their PrEP is presented in Figure 3. SRC and Population Solutions for Health were the most preferred because they offer differentiated services and a friendly environment to MSM due to their centrality in terms of location compared to public hospitals.

Hotspot Maps of MSM Locations and Where MSM Access PrEP
Knowledge Levels of MSM on PrEP
A total of (59) 90.8% of MSM were knowledgeable, scoring at least 6 out of 10 on PrEP, HIV, and AIDS. The highest level of education was the only socio-demographic characteristic significantly associated with the level of knowledge, as indicated by the Chi-square p value (<.001). Half of the population that was not knowledgeable had primary as their highest level of education. Primary education refers to a level of the education system in Zimbabwe that is foundational (roughly offered to 6- to 12-year-olds) and prepares them for high school. Other socio-demographic characteristics reported no significant association with the level of knowledge, as indicated by the Chi-square p value greater than .05. Age was not significantly associated with knowledge; however, some age groups reported higher chances of being knowledgeable than others. For instance, the age group 25–29 and 30–34 were 4.8 times more likely to be knowledgeable than those younger than 20 and aged 35 and above. The logistic regression odds ratio indicated that Black MSM was more likely to be knowledgeable than other ethnic races, and these findings are presented in Table 2.
Relationship Between Knowledge Levels and Socio-Demographic Characteristics
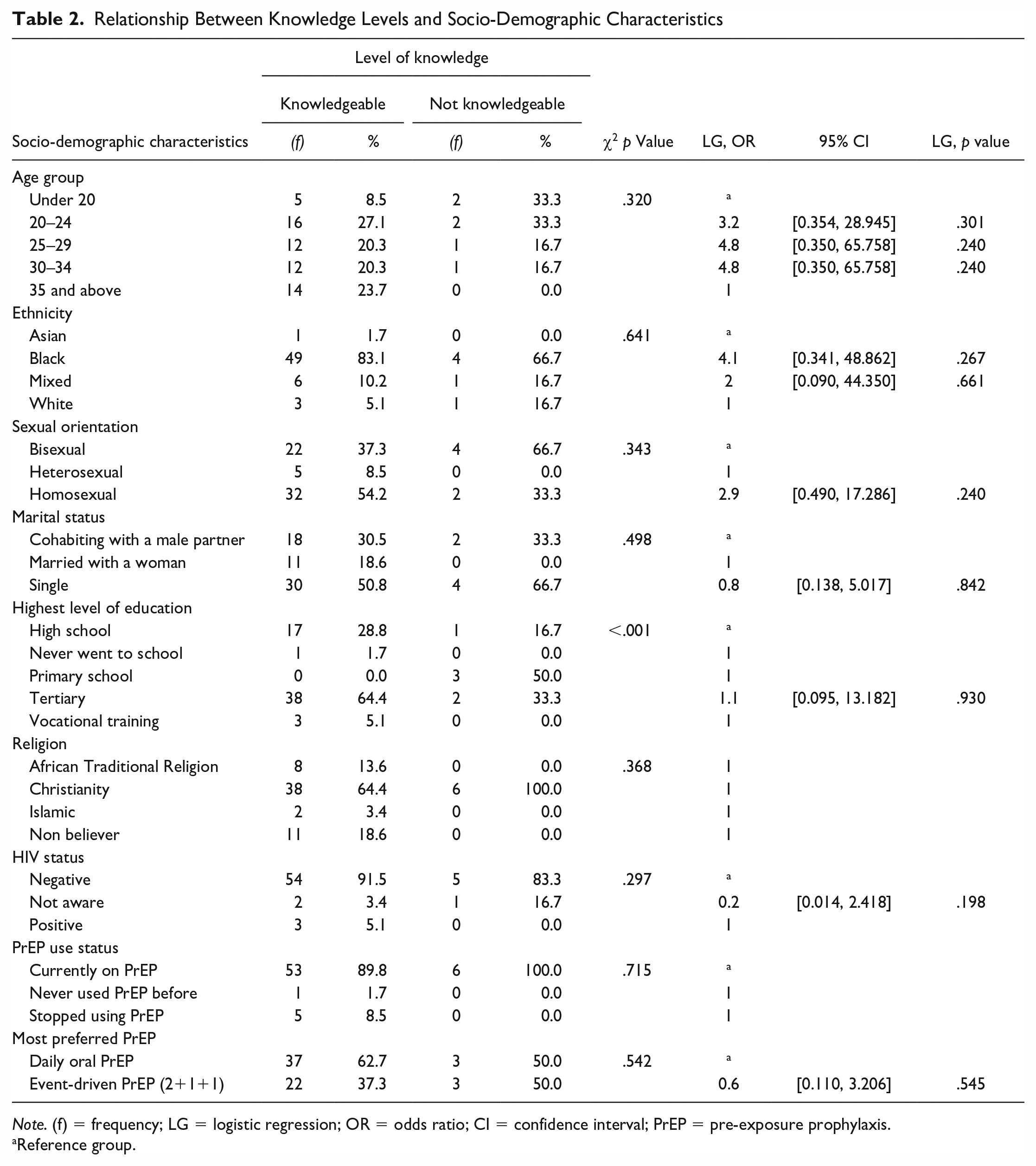
Note. (f) = frequency; LG = logistic regression; OR = odds ratio; CI = confidence interval; PrEP = pre-exposure prophylaxis.
Reference group.
Barriers to PrEP Use
About 46 (70%) of the respondents concurred that of the 20 predetermined barriers in the questionnaire, 15 influenced access to PrEP and its use. These findings are presented in Figure 4. The most disagreed barriers to PrEP use among this population were negative attitudes from health care workers and PrEP being not reliable, affordable, and effective. These barriers were least agreed upon because 84% of the respondents reported accessing their PrEP from MSM-friendly facilities free of charge.

Barriers Influencing PrEP Use Among MSM (n = 65)
Relationship Between Barriers and Accessibility of PrEP
Of all the 20 barriers cross-tabulated with this outcome variable (have you accessed PrEP), none of the barriers were significantly associated with this outcome variable, as indicated by the Chi-square p value (<.05). These findings are presented in Table 3.
Relationship Between Barriers and Access to PrEP
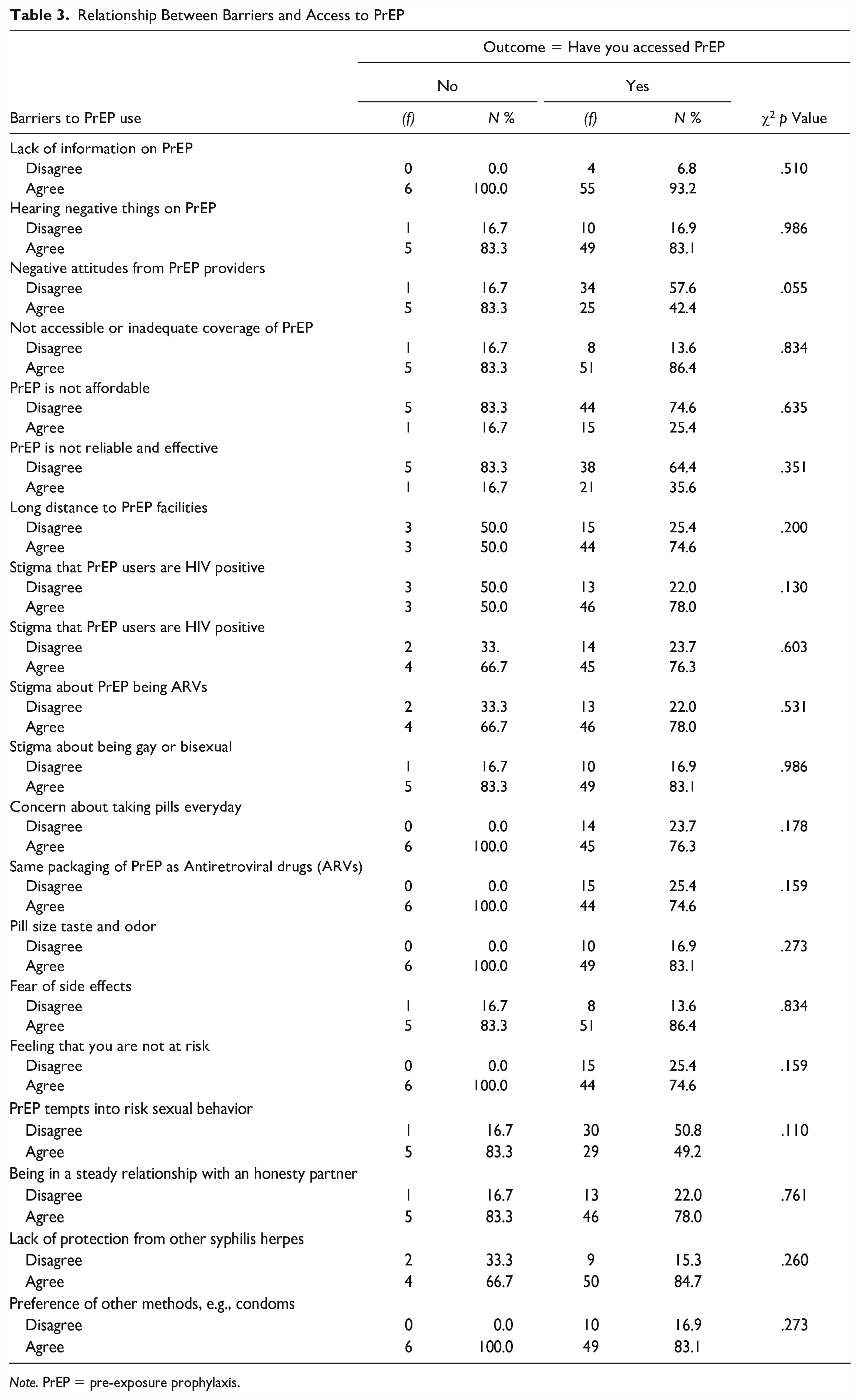
Note. PrEP = pre-exposure prophylaxis.
PrEP education, friendly PrEP facilities, and making PrEP available at all times were agreed upon by all the respondents in the study as effective facilitators to improve PrEP use among MSM. Improving the packaging of PrEP pills was the least agreed to as a facilitator, and the results are presented in Figure 5.
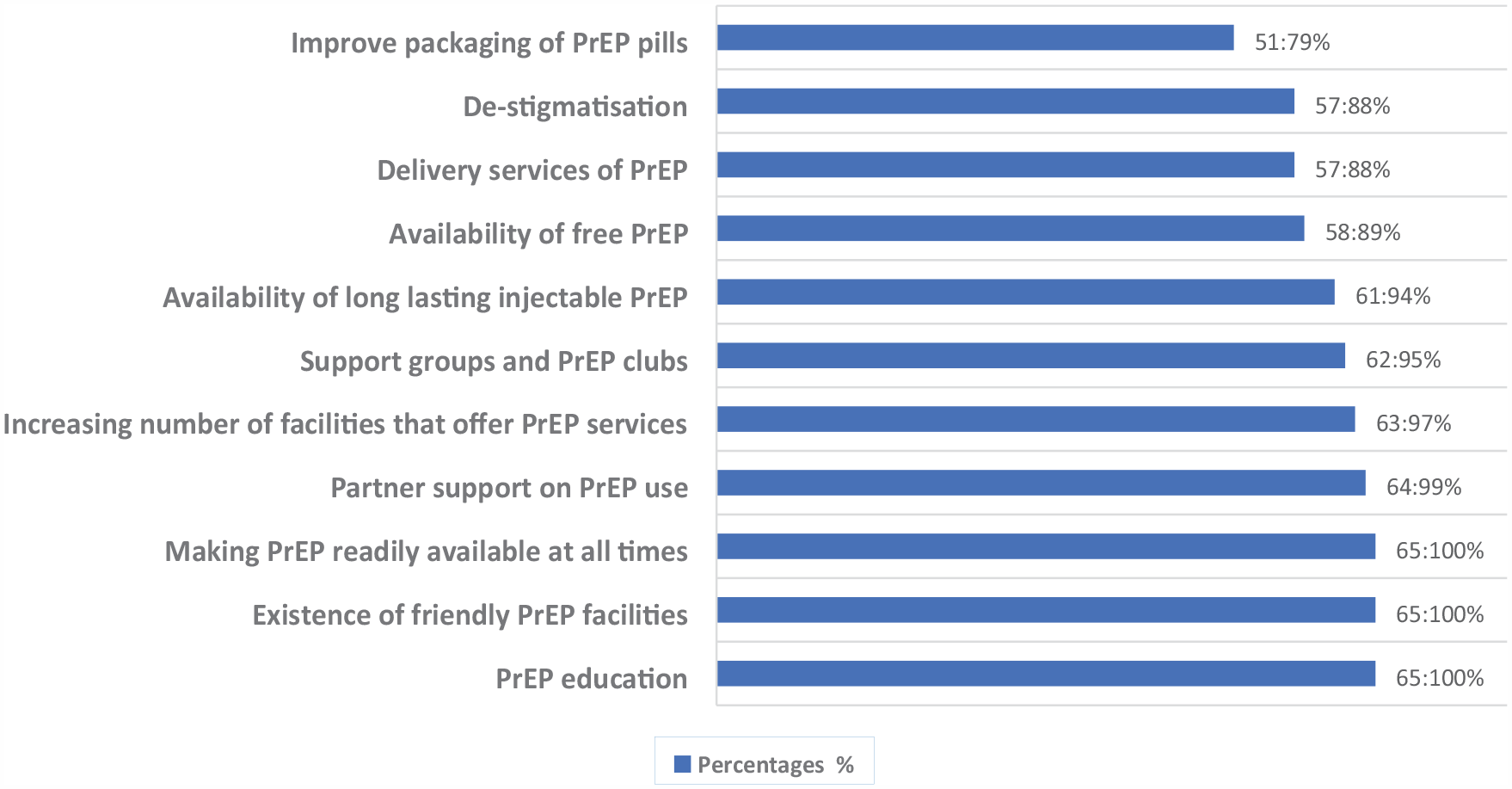
Facilitators to Improve Use Among MSM
Discussions
It was noted that only four PrEP providers were used by the respondents to access PrEP, with SRC (55%) being the most preferred facility, followed by Population Solutions for Health (29%). These two facilities are MSM-friendly, and these organizations are notable champions in providing SRHS and upholding human rights to LGBQIT+. The findings concur with Graham et al. (2022), Pichon et al. (2022), and Yu et al. (2021), who reported that MSM preferred accessing their pills from MSM-friendly facilities as compared to other PrEP providers (Graham et al., 2022; Pichon et al., 2022; Yu et al., 2021). The study reported that these MSM facilities are centrally located in the Central Business District (CBD), which is convenient for MSM to access compared to the public hospitals located outside CBD. The study corresponds with another one in Kenya by Graham et al. (2022), which reported that long distances to a PrEP facility could hinder PrEP uptake (Graham et al., 2022). Pelletier et al. (2019) also noted that distance to the distribution center is a player in the acceptability of PrEP among MSM.
The study reported that 90.8% of MSM were highly knowledgeable about PrEP, HIV, and AIDS-related services. This could be explained by the fact that most participants access PrEP in MSM-friendly facilities that take time to educate and accommodate their unique needs. This is consistent with the results of a study done by Voglino et al. (2021) in Italy, which recorded a high level of knowledge of 100%, and Holloway et al. (2017) recorded 82.3% of respondents being knowledgeable in the United States of America (Voglino et al., 2021). However, other studies conducted in low-income or middle-income countries such as Swaziland, Ghana, and Cote d’Ivoire reported that MSM was not knowledgeable (Ogunbajo et al., 2020; Pelletier et al., 2019; Sithole, 2017).
The results also reported that knowledge was associated with the highest level of education (p < .001) among a sample of MSM who participated in the study. Usually, the higher the level of education, the higher the literacy level, and the hungrier one becomes in the quest for knowledge. The study concurs with Ahouada et al. (2020) and Voglino et al. (2021), who also found an association between knowledge of PrEP and the highest level of education (Ahouada et al., 2020; Voglino et al., 2021). The logistic regression odds ratio reported no significant differences between age groups on the level of knowledge of PrEP. The findings contradict the study in Latin America by Assaf et al. (2021), which reported an association between age and PrEP awareness (Assaf et al., 2021). Logistic regression odds ratio reported that Black MSM was knowledgeable as compared to other ethnic groups; these findings contradict the study findings of Kahle et al. (2018), which reported that knowledge levels were higher among White MSM than among other minority races (Kahle et al., 2018). This could have been the case because Blacks in Zimbabwe accounted for a large and dominant proportion. Low awareness of PrEP has been reported in other studies to be associated with racial/ethnic minorities (Eaton et al., 2015); this is consistent with the findings of this study that minority groups (Asian, mixed, and White) had the lowest odds of being knowledgeable about PrEP as compared to Blacks.
Similar to previous research investigating barriers that influence PrEP use among MSM. The most commonly identified barriers include stigma on PrEP users being promiscuous and HIV positive, their sexuality, inadequate information on PrEP, negative attitudes from PrEP providers, daily pill taking, fear of side effects, and inadequate coverage of PrEP. The findings correspond with many studies identifying the aforementioned barriers (Adeagbo et al., 2021; Dean et al., 2023; Klein & Washington, 2020; Pichon et al., 2022; Pingel et al., 2017). The findings, however, identified the unaffordability of PrEP as not a significant barrier, as noted by the respondents; this was attributed to the fact that most respondents reported accessing their PrEP for free in either MSM-friendly facilities or public hospitals. These results contradict some studies which mentioned the unaffordability of PrEP as a notable barrier (Dean et al., 2023; Emmanuel et al., 2020; Graham et al., 2022; Gredig et al., 2016; Han et al., 2019; Harawa et al., 2016; Hojilla et al., 2018; Holloway et al., 2017; Patrick et al., 2019; Pérez-Figueroa et al., 2015; Pérez-Jiménez et al., 2009; Voglino et al., 2021). Cross-tabulation was done to explore whether the barriers had any influence using the outcome variable of whether MSM has accessed PrEP. None of the barriers reported any significant association between the two variables, as indicated by the Chi-square p value. The findings contradict most of the studies that established an association between barriers and accessibility of PrEP. More studies need to be carried out to understand the situation.
The study’s findings align with many literature sources indicating that MSM’s decision to forgo PrEP is significantly influenced by the barriers they face at different levels. To improve the uptake of PrEP among this population, different facilitators identified include correct messaging on PrEP, PrEP education, the existence of friendly PrEP facilities, making PrEP available at all times, partner support on PrEP use, increasing the number of PrEP facilities, support groups, and availability of long-lasting injectable PrEP. These usually ensure consistency in services received, thus creating demand for the services and confidence to access these services. The results concur with the findings by other scholars who also identified different facilitators to improve PrEP, such as PrEP education and dissemination of information, the existence of MSM-friendly facilities, increasing health care centers that provide PrEP services, preference of long-lasting injectable PrEP, and support groups or PrEP clubs (Chakrapani et al., 2015; Graham et al., 2022; Harawa et al., 2016; Pichon et al., 2022; Yu et al., 2021; Zhou et al., 2022).
Limitations
The study focused on respondents in the urban setup of Bulawayo. They had ties or relations with the SRC and came out about their sexuality. This could have led to those not disclosed being excluded from the study. This study was not funded; therefore, this resulted in the recruitment of a small sample size guided by the few resources the researchers had. It would have been ideal to conduct a study with a larger sample size to gather the varied views of more respondents. The strategy that was used to recruit respondents could have led to those MSM who were not in the databases of organizations that had sexual health programs targeting MSM to have been left out and their views missed. These findings, therefore, could not be generalized to the broader population as far as MSM is concerned.
Conclusions
PrEP uptake among MSM in Bulawayo has generally been significantly high. This can be attributed to various factors, including increased awareness campaigns, the existence of MSM facilities, and the effectiveness of PrEP in preventing HIV transmission. Overall, PrEP has been well-received among many MSM communities in Bulawayo. Acceptability of PrEP among MSM has also been generally positive. It was revealed that MSM had favorable attitudes and knowledge toward it. Providing PrEP to MSM for free by health care facilities has contributed to its acceptability among many MSM diversities in Bulawayo. It is important to note that barriers and challenges to PrEP uptake and acceptability still exist among some MSM populations. These can include concerns about side effects, negative attitudes by health care providers, stigma, and access to health care services.
Footnotes
Authors’ Note
P.L.M. is a BSc Environmental Science and Health degree holder at the National University of Science and Technology in Zimbabwe. The author is also a Master’s student in the same institution. This article was part of the research project required for partial fulfillment of the Master’s Degree in Environmental Health. W.N.N. is a PhD in Public Health degree holder and an Executive Dean in the Faculty of Environmental Science. The author is the supervisor to the student and provided guidance and mentorship in the conceptualization and writing of this manuscript.
Author Contributions
P.L.M. conceptualized the research idea and drafted the manuscript. W.N.N. coordinated the manuscript writing process, guided the manuscript writing process, and revised the draft manuscript. Both authors read and approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
An application for ethical approval was lodged with the Institutional Review Board at the National University of Science and Technology in Bulawayo, Zimbabwe. This committee granted ethics clearance (Ethics Clearance Number: NUST/IRB/2023/52).