
Abstract
This research examines the level of pre-exposure prophylaxis (PrEP) self-efficacy among HIV-negative men who have sex with men (MSM) in China and identifies the influencing factors associated with the level of PrEP self-efficacy in terms of social-demographic characteristics and social psychological factors. The data were gathered from a baseline assessment of a longitudinal randomized controlled intervention trial. From April 2013 to March 2015, nonprobability sampling was used to recruit HIV-negative MSM at Chongqing, Guangxi, Xinjiang, and Sichuan in west China. A total of 1884 HIV-negative MSM were analyzed. Chi-square test and nonparametric rank sum test were used for univariate analysis. Multivariable linear regression analysis was used to discuss the factors that influence the level of PrEP self-efficacy. Overall levels of PrEP self-efficacy were low, and five factors were found to effect PrEP self-efficacy: age, residence, AIDS-related knowledge, PrEP-related motivation, and anxiety. Age and anxiety score were negatively related to PrEP self-efficacy. The higher the age and anxiety score, the lower the PrEP self-efficacy. AIDS-related knowledge and PrEP-related motivation were actively related to PrEP self-efficacy. The higher the knowledge and motivation score, the higher the PrEP self-efficacy. In addition, the PrEP self-efficacy level of MSM in rural areas is lower than that in urban areas. The lower level of self-efficacy in the MSM population needs to be improved. Pertinent interventions should be taken to promote the self-efficacy of PrEP in MSM, to enhance their willingness to take medicine, improve their medication adherence, and thus reduce HIV infection among MSM.
Pre-exposure prophylaxis (PrEP), a new biological approach to HIV prevention, is currently the most promising HIV prevention strategy. The safety and efficacy of daily oral PrEP using tenofovir/emtricitabine (TDF/FTC) for the prevention of sexually-acquired HIV infection among some high-risk groups, including men who have sex with men (MSM), injection drug users, sex workers, and transgenders, has been demonstrated in randomized trials and open-label studies abroad (Choopanya et al., 2013; Grant et al., 2014; Thigpen et al., 2012). Currently, PrEP is still in the research stage in China. In the “Eleventh-Five” National Science and Technology major projects (2005–2010), both the willingness to use PrEP and PrEP adherence of the MSM population were significantly better than those of female sex workers and negative sexual partners with HIV infection. In the “Twelfth-Five” National Science and Technology major projects (2011–2015), the protective rate in participants with high adherence was 50%, but there was no difference between those with low adherence and those without medication. This study suggests PrEP adherence affects the efficacy of PrEP. Studies have reported that the higher the individuals’ self-efficacy, the greater the positive influence on the adherence to the behavior and the degree of effort (Coffman, 2008). So it is especially necessary to study PrEP self-efficacy.
Self-efficacy was first proposed by the American psychologist Bandura in 1977 (Bandura, 1977). It refers to personal expectations and the subjective confidence of one’s behavior. Personal expectations determine whether coping behavior will be initiated, how much effort will be expended, and how long it will be sustained in the face of obstacles and aversive experiences. Self-efficacy, as the determinant of individual behavior, is also the center of individual factors that often influences the choice and continuation of individual behavior. The higher the level of self-efficacy, the higher the level of behavior adoption, behavior maintenance, and degree of effort (Coffman, 2008). It is necessary to understand the level of self-efficacy of PrEP in the MSM population and to explore the factors affecting the self-efficacy.
The following studies have also been done involving psychosocial factors among Chinese MSM. In a qualitative interview in Shanghai, China, prevention strategies in the MSM population will be hindered due to MSM’s sexual stigma and discrimination (J. X. Liu & Choi, 2006). In other studies of PrEP, self-efficacy was related inversely to involvement in HIV risk practices (Klein, 2014). Domestic and foreign studies of the factors affecting self-efficacy mainly focused on patients with chronic diseases such as diabetes, cancer, chronic obstructive pulmonary disease, and asthma (Champion et al., 2013; Du, Everett, Newton, Salamonson, & Davidson, 2012; Franks, Chapman, Duberstein, & Jerant, 2009; Hays, Finch, Saha, Marrero, & Ackermann, 2014; Hunt et al., 2012; Mancuso, Sayles, & Allegrante, 2010). Studies have reported that the main factors affecting self-efficacy include social demographic characteristics, physiological conditions, and social psychological factors. The studies regarding the factors affecting self-efficacy in the MSM population focused mainly on the use of condoms (Klein, 2014; Li et al., 2017; Træen et al., 2014). PrEP studies are in the self-efficacy description phase, and there is seldom a further exploration of the influencing factors.
As an important part of social cognitive theory, self-efficacy theory can explain the relationship between human cognition and behavior. Many psychological studies suggest that action self-efficacy is an important factor influencing behavioral initiation and behavior persistence. The present study aimed to evaluate the self-efficacy of PrEP and identify the factors affecting PrEP self-efficacy among HIV-negative MSM in China from the prospective of sociodemographic characteristics and social psychology factors and to provide a theoretical basis for pertinent interventions.
Methods
Participants and Design
A total of 1,914 HIV-negative MSM were recruited at the baseline of a longitudinal randomized controlled intervention trial (a PrEP study of oral tenofovir among MSM in western China from April 2013 to March 2015. Registration Number: ChiCTR-TRC-13003849) according to the inclusion criteria; 30 participants did not meet the age criteria. In total, 1,884 MSM data were analyzed. A nonprobability sampling method was used to recruit participants in four research sites in west China including Chongqing, Guangxi, Xinjiang, and Sichuan, from April 2013 to March 2015. The main methods of recruitment included: (a) media publicity, such as publishing information on the MSM website; (b) cooperation with nongovernmental organizations (NGOs); (c) through the Centers for Disease Control and Prevention in each city; (d) after finding the “seed,” through peer introduction and the “snowball” sampling method to find other research subjects; (e) recruitment from existing MSM cohorts of previous research projects. The inclusion criteria were as follows: signing informed consent; age ≥18 and ≤65; HIV antibody negative; participate in sexual intercourse once or more every 2 weeks; at least one or more male partners one month before the trial; willing to use the study medication under guidance and to obey follow-up arrangements; willing to participate in the trial for 96 weeks. A self-administered questionnaire survey on paper including sociodemographic characteristics, HIV-related knowledge, and psychological scales was collected.
Measurement
Sociodemographic characteristics were collected by an anonymous questionnaire survey. The survey included self-reported age, ethnicity and residence, education attainment, employment status, marital status, and average monthly income.
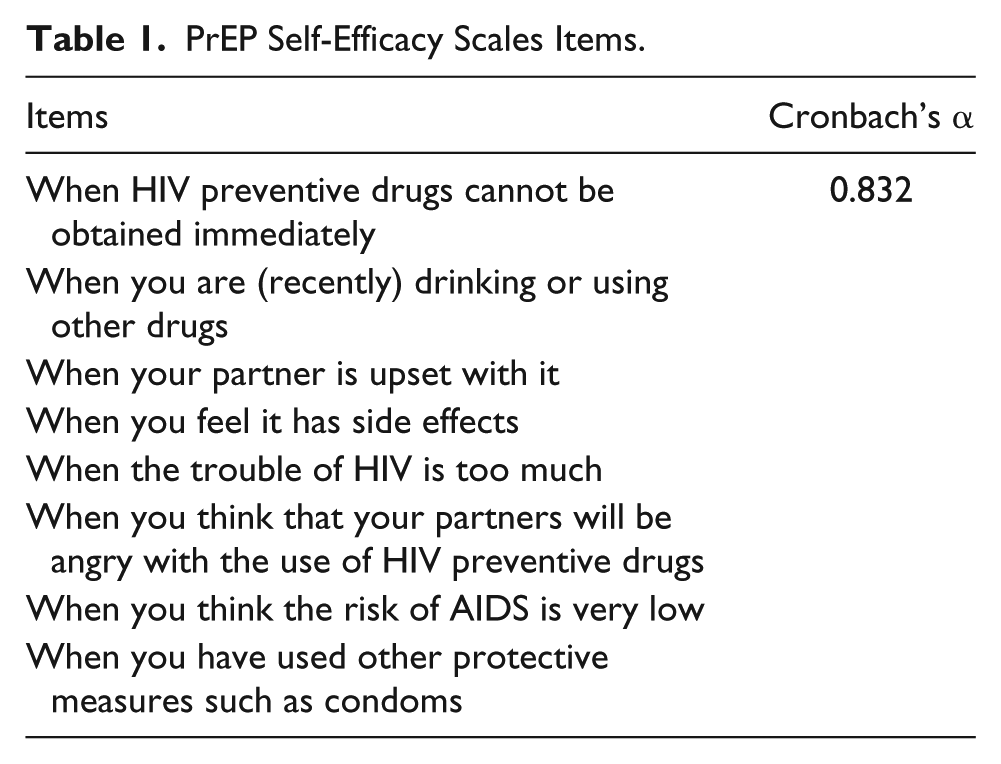
The PrEP self-efficacy scales were measured with eight questions. The scale is based on the revision by Galavotti et al. (1995) and has proven to be reliable. Subjects were asked “In the following situations, how confident are you to continue to use HIV preventive medicine?” The actual items of this scale are shown in Table 1. Answers for each item are as follows: 1 stands for strongly unconfident; 2 for unconfident; 3 for comparatively confident; 4 for confident; and 5 for strongly confident. The higher the total score of these items, the greater the self-efficacy of taking drugs. Usually, strongly unconfident and unconfident suggest a low self-efficacy level, while comparatively confident, confident, and strongly confident suggest a high self-efficacy level (Cronbach’s α = 0.832).
PrEP Self-Efficacy Scales Items.
A self-rating anxiety scale (SAS; Zung, 1971) was widely (J. Liu et al., 2012; S. Liu et al., 2014; Luo, Feng, Xu, & Zhang, 2014; Samakouri et al., 2012) used to evaluate the degree of anxiety because of its good reliability and validity (Zhao et al., 2012). SAS, scored by four grades, was mainly used to evaluate the frequency of the symptoms. Among all the items, 15 were positively scored while 5 were reverse scored. The scores of the 20 items were added together to obtain the raw score, and then multiplied by 1.25, and the integer was taken as the standard score. Usually, 50 was the cut-off value. A total score of anxiety below 50 points was considered normal, 50–59 as mild anxiety, 60–69 as moderate anxiety, and above 70 as severe anxiety (Cronbach’s α = 0.774).
The Center for Epidemiological Studies Depression Scale (CES-D; Radloff, 1977) consists of 20 items, rated on a scale of 0 to 3, with a total score of 60 points. Usually, 16 points (Makambi, Williams, Taylor, Rosenberg, & Adams-Campbell, 2009) is the cut-off value, and ≥16 indicates depression symptoms. Cronbach’s α coefficient has high internal consistency between 0.85 and 0.90.
AIDS-related knowledge included 13 items based on the revision of the International AIDS Knowledge Survey General scale {DiClemente, Zorn, & Temoshok, 1986; Galavotti et al., 1995; Koopman, Rotherman-Borus, Henderson, Bradley, & Hunter, 1990}, involving the infection, spread, and treatment of AIDS. The items of this scale are shown in Table 2. The answers were set as True, False, or Don’t know. There was 1 point assigned for a positive answer, 0 for a negative answer, and “not known” was rated as negative. The higher the score, the more information is known. These items compose of the AIDS-related knowledge score (Cronbach’s α = 0.84).
AIDS-Related Knowledge Items.

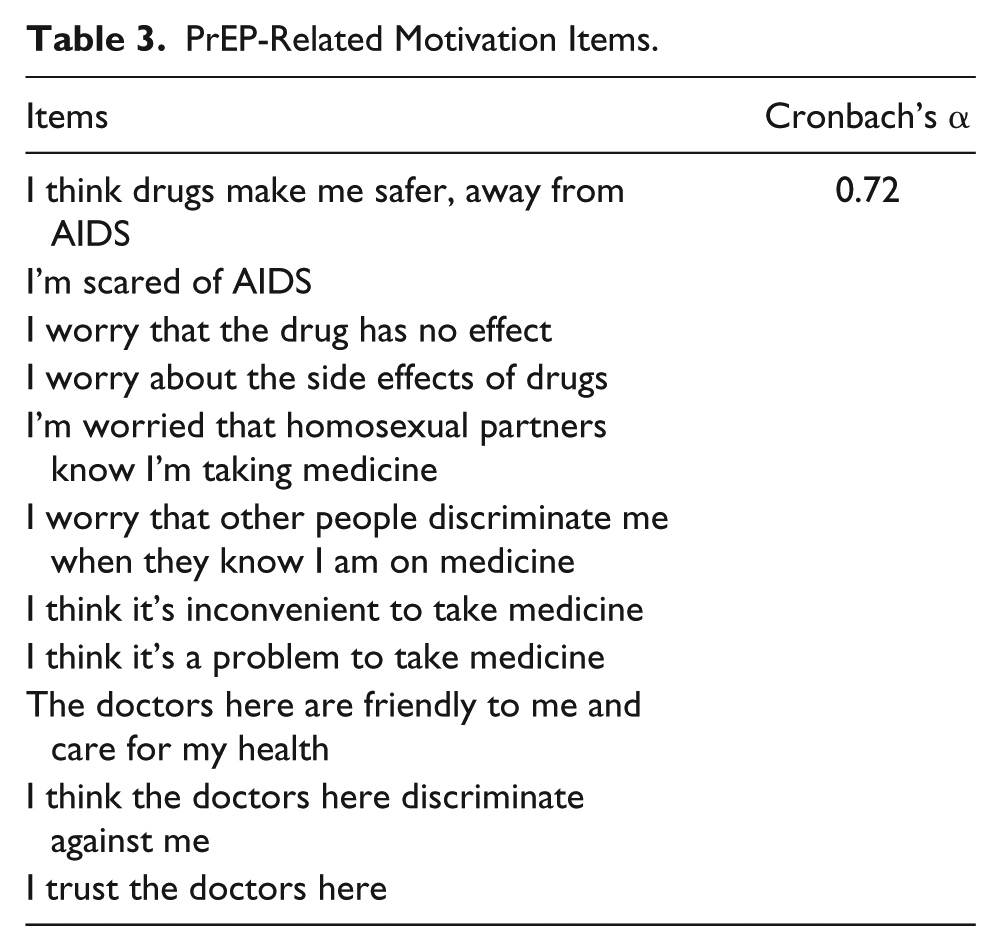
PrEP-related motivation was measured with 11 items. The scale is a self-designed questionnaire by experts (see Table 3 for details). Its range is 11–55. It includes risk perception of AIDS, negative effects of drugs, knowledge and attitude of sexual partners, objective factors of drugs, and the interaction between doctors and patients. It has been proven to have good construct validity and content validity and has been used in previous studies (He & Zhong, 2014) A 5-point Likert scale was used to measure the answer of motivation (1 = completely no and 5 = always). An adverse value was used in questions No. 4 to No. 9. These items compose the PrEP-related motivation score. The higher the score, the greater the PrEP motivation (Cronbach’s α = 0.720).
PrEP-Related Motivation Items.
Statistical Analysis
Epidata 3.1 was used to establish a database and double-entry data and logical verification were conducted. IBM SPSS 21 was used for data processing analysis. Measurement data were statistically described using the mean, standard deviation, median, and extreme values. The count data were described by frequency distribution. The mean ± standard deviation was used to describe the self-efficacy level, knowledge score, anxiety level, and depression level. Chi-square test and nonparametric rank sum test were used for univariate analysis, while multiple stepwise regression was used for multivariable analysis. The inclusion and removal criteria were 0.05. The statistical significance level was p values < .05.
Results
Social-Demographic Characteristics
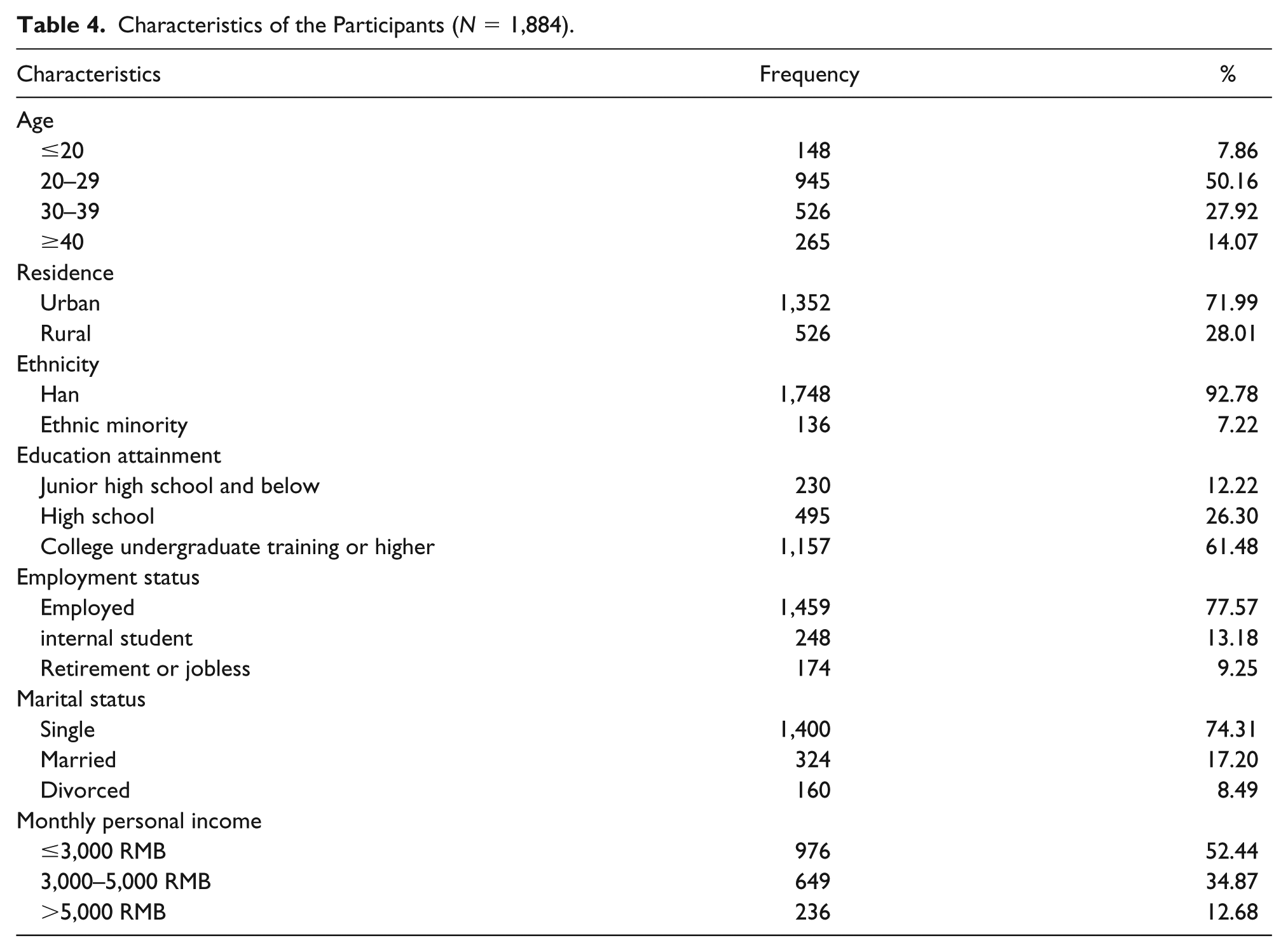
A total of 1,914 MSM were recruited, among which 1,884 MSM were analyzed according to the inclusion criteria with ages ranging from 18 to 58, and a median age of 28. Most participants were unmarried (74.31%), of Han nationality (92.78%), employed (77.57%), urban residents (71.99%), had a college or higher degree (61.48%), and reported a monthly income below 3,000 RMB (52.44%; Table 4).
Characteristics of the Participants (N = 1,884).
Self-Efficacy Level
The results showed that the minimum self-efficacy score of 1,884 MSM was 8 points, while the maximum was 40 points, with a mean score of 22.24 ± 6.40. Of the participants, 1,133 (60.14%) felt strongly unconfident or unconfident using HIV prevention drugs, and 751 (39.86%) felt confident using HIV prevention drugs.
Anxiety and Depression Status
The mean SAS and CES-D scores for 1,884 MSM were 41.57 ± 10.30 and 17.96 ± 10.55, respectively. Among them, 401 participants had anxiety symptoms, accounting for 21.28% of participants, and the mild, moderate, and severe anxiety symptoms were 16.61%, 4.03%, and 0.64% of participants, respectively. There were 946 participants with depression symptoms (50.21%).
Knowledge and Motivation Status
The mean scores of AIDS-related knowledge and PrEP-related motivations were 8.28 ± 2.36 and 40.19 ± 5.84, respectively. Only 17.57% of the 1884 MSM participants scored above 10 points on the AIDS-related knowledge test, while 82.43% scored below or equal to 10 points.
Univariate Analysis of PrEP Self-Efficacy in MSM Population
Social-demographic univariate analysis of PrEP self-efficacy in MSM
The results showed that self-efficacy differs in residence, education, and marital status (p < .05). The self-efficacy of the MSM population in urban areas is higher than that in rural areas. The self-efficacy of those whose education was above college level is higher than those with an education level below high school. The self-efficacy scores of those who are unmarried are higher than the score for those who are married or divorced. There was no significant difference in the self-efficacy of the MSM population with regard to age, ethnicity, employment status, and monthly income (p > .05; see Table 5).
Univariate Analysis of the Influence of Social-Demographic Characteristics on MSM Self-Efficacy.

Note. aChi-square test. bRank sum test.
Multivariable Analysis of the PrEP Self-Efficacy Level Among MSM
Independent variable values
Self-efficacy is a dependent variable. The social-demographic characteristics, knowledge score, motivation score, anxiety, and depression were set as independent variables with p < .15 after univariate analysis. The inclusion and exclusion criteria were set at 0.05. The independent variable values are presented in Table 6.
Assignment Sheet of the Influencing Factors of PrEP Self-Efficacy.
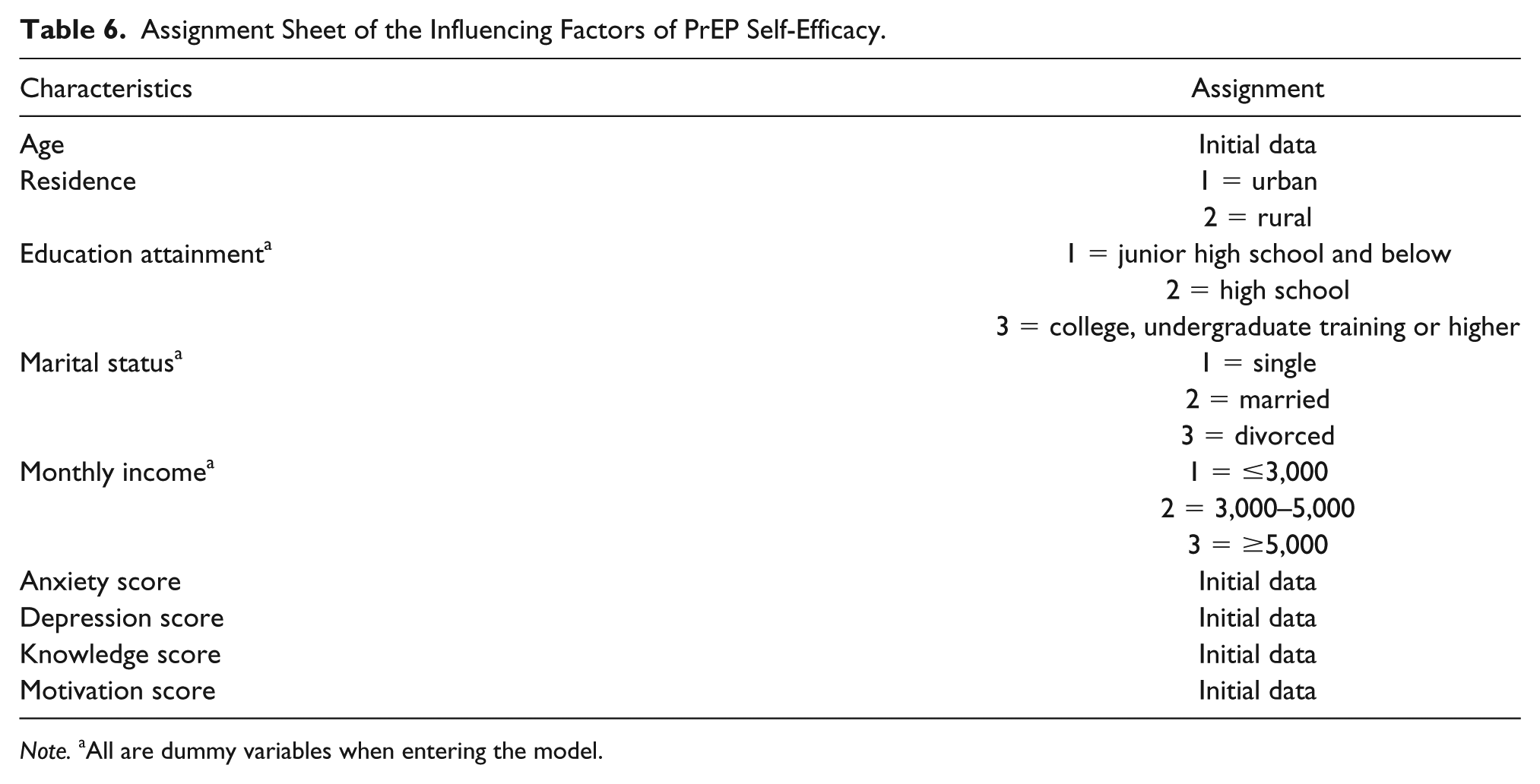
Note. aAll are dummy variables when entering the model.
Multivariable Regression Result
Table 7 presented that five statistically significant factors entered the regression equation. According to the standard partial regression coefficient, the factors affecting self-efficacy were age, residence, motivation, anxiety, and knowledge score. The results showed that the higher the AIDS-related knowledge and the PrEP-related motivation score, the higher the PrEP self-efficacy level. The older the age, the lower the PrEP self-efficacy level. Those who registered as living in a rural area had a low PrEP self-efficacy level. The higher the anxiety score, the lower the self-efficacy of PrEP.
Multivariable Regression Results of Factors Affecting Self-Efficacy.

Discussion
Many psychological studies suggest that action self-efficacy is an important factor influencing behavioral initiation and behavior persistence. The results of this study show that the PrEP self-efficacy level was low among HIV-negative MSM in China, with an average score of 22.24 points. Over 60% participants felt strongly unconfident or unconfident using PrEP. The reason may be that in China, the MSM population is viewed as immoral and unacceptable, and even the mere perception of stigma can influence individual behavior, adding to chronic stress and detracting from physical and psychological well-being. The particular population suffered from fears, prejudices, and discrimination, and their inner health beliefs were weak.
The AIDS-related knowledge score was low among Chinese HIV-negative MSM, with an average score of 8.28. Only 17.57% participants answered more than 10 questions correctly. PrEP-related motivation is at a moderate level, with an average score of 40.19. Overall, AIDS-related knowledge and the PrEP motivation level among HIV-negative MSM in this study was not high. The proportion of anxiety and depression symptoms in the MSM population was relatively high, with average score of 41.57 and 17.96, respectively. Among the 1,884 MSM participants, 21.28% had anxiety symptoms and 50.21% had depression symptoms.
Further analysis shows that sociodemographic factors, AIDS-related knowledge, PrEP-related motivation, and anxiety are all related to PrEP self-efficacy. The older the age, the lower the PrEP self-efficacy. This is consistent with most studies at home and abroad. As age increases, the MSM population suffers from gradual deterioration of physical function, and as self-perception declines, the sense of self-existence decreases. It was also identified that MSM in rural areas had lower self-efficacy of PrEP compared to urban areas. In rural areas, MSM are conservative, lack access to health knowledge, and lack of confidence in carrying out healthy behaviors, so their self-efficacy is low. For rural and high-age populations, health education and knowledge promotion were used to improve the PrEP self-efficacy.
This survey shows the significant differences in AIDS-related knowledge, PrEP motivation, and PrEP self-efficacy. The more the AIDS-related knowledge and the stronger the motivation for PrEP, the higher the PrEP self-efficacy. According to the Knowledge, Attitude and Practice (KAP) theory, knowledge can help participants establish correct health beliefs and increase their confidence. In motivation constructs, the risk perception of AIDS, negative effects of PrEP, knowledge and attitude of sexual partners, and objective factors of PrEP all affect PrEP self-efficacy. Negative effects of PrEP are related inversely to self-efficacy. The risk perception of AIDS and the interaction between doctors and patients are actively related to the self-efficacy. Bandura reported in his “desensitization” study that mental state is one of the key factors affecting self-efficacy. The study suggests that PrEP self-efficacy has a negative correlation with anxiety level, while there was no significant difference between different depression levels. This result is consistent with previous findings in other populations (Razavi, Shahrabi, & Siamian, 2017). Therefore, we should continue to popularize AIDS knowledge and PrEP-related knowledge, and strengthen MSM psychological intervention to promote health.
This study suggests that in the process of PrEP intervention among HIV-negative MSM in China, it is necessary to analyze the general self-efficacy, psychological state, and PrEP-related motivation of the MSM population. For MSM, we should strengthen the propaganda of routine AIDS prevention and control knowledge, conduct health education and psychological guidance, reduce the incidence of anxiety and depression, so as to improve the self-efficacy of AIDS prevention. Adjusting the intervention strategy is of great significance to the prevention and control of AIDS. Regarding the older and rural MSM, we should support them and enhance their sense of self-efficacy. We should strengthen the intimate relationship between medical workers and the MSM population to make the population feel social warmth and support, to improve their self-efficacy.
There are some potential limitations in this study that deserve our attention. First, this study is a cross-sectional study that only examined the level of self-efficacy of MSM at the current stage and did not observe the dynamic change of PrEP self-efficacy in MSM. Therefore, this problem has yet to be further studied. Second, self-administered questionnaires were used. Because the content of the survey involves sensitive issues and the questionnaires were completed with the help of the investigators, some of the participants may not have been willing to answer the relevant questions, resulting in bias and missing data.
The results of this study are similar to those of other Chinese research populations, and they are more credible. The results of this study are of great significance to the MSM population’s willingness and adherence to PrEP. Tailored interventions should be taken to strengthen the health beliefs of the Chinese HIV-negative MSM and improve the self-efficacy of PrEP among MSM populations, thereby increasing the willingness of MSM to take medications, improve drug compliance, and reduce HIV infection among MSM populations.
Footnotes
Acknowledgements
We thank all participants and investigators for their help. We are also grateful to the staff from local offices of Centers for Disease Control in Guangxi, Sichuan, and Chongqing for their aid in the data collection during our research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Key Project for Infectious Diseases of the Ministry of Science and Technology of China, NO.2012ZX10001007.
Ethics
The study was approved by the ethics committee of Chongqing Medical University and before taking part in this research, participants were fully informed about the purpose, significance, voluntary participation, and confidentiality of the research. Each participant signed an informed consent. (Approval NO.2012010)