
Abstract
Plain Language Summary Title
Plain Language Summary: This study looked at how willing men who have sex with men (MSM) in Teresina, Brazil, are to use a medication called pre-exposure prophylaxis (PrEP) that helps prevent human immunodeficiency virus (HIV) infection. The study included 320 men, mostly aged 20 to 39 years, many with higher education and moderate income. They answered questions about their background, sexual habits, knowledge about PrEP, and how they see their risk of getting HIV. Almost all participants (about 93%) said they were willing to use PrEP. Willingness was higher among those with more education, those who had symptoms of other sexually transmitted infections recently, and those who knew more about PrEP. Even though many wanted to use PrEP, knowledge about it and awareness of HIV risk were still low. Understanding what helps or stops people from using PrEP is important to increase its use and reduce HIV infections.
Introduction
The human immunodeficiency virus (HIV) represents one of the most significant public health challenges and, consequently, a global issue in terms of prevention and care. It is estimated that approximately 40.8 million people worldwide were living with HIV in 2024, with 1.3 million new infections occurring in the same year. 1 Furthermore, the HIV epidemic is concentrated among population groups with greater vulnerability, accounting for 65% of new infections globally. These groups, referred to as key populations, include men who have sex with men (MSM), people who inject drugs, female sex workers, and transgender individuals. 2
In this context, MSM—defined as men who engage in sexual relations with other men regardless of whether they also have sexual relations with women, or whether they personally or socially identify with categories such as “gay” or “bisexual”—constitute one of the primary groups vulnerable to HIV. This is particularly relevant given the disproportionate growth of the epidemic in this population across countries with diverse socioeconomic conditions. 3
It is estimated that MSM have a global HIV prevalence of approximately 7.6% and a 23-fold higher relative risk of acquiring HIV compared to the general population. In Brazil, a study conducted in 12 state capitals estimated an HIV prevalence of 18.4% among MSM in 2016, which represents a striking contrast when compared to the prevalence in the general population, at 0.7%.1,4 In this context, according to the national Epidemiological Bulletin, of the 46,495 reported HIV infections in 2023, 53.6% occurred among MSM. 5
It is important to emphasize that being an MSM does not inherently imply a higher risk of HIV infection. The vulnerability of this population is linked to behavioral, social, and cultural factors. Thus, the increased risk of HIV infection among MSM is associated with sexual practices and behaviors, condom use, the type and number of sexual partners, and the use of drugs or alcohol. In addition, factors such as lack of information, stigma, discrimination, and breaches of confidentiality in healthcare services contribute to reduced engagement in care and limited awareness of serostatus, ultimately resulting in a higher occurrence of HIV among MSM.6,7
In light of this, reducing HIV infection among this key population is critical to controlling the epidemic. 8
The combined prevention strategy, adopted in Brazil, integrates biomedical, behavioral, and structural interventions, addressing not only individuals but also their relationships and the social groups to which they belong, while respecting their specific characteristics.9,10
Within this framework, pre-exposure prophylaxis (PrEP) for HIV—which involves providing antiretroviral medications to HIV-negative individuals at high risk before exposure, thereby preventing HIV acquisition—emerges as an essential tool in epidemic control. When used correctly, PrEP can reduce the risk of HIV acquisition by more than 90%.11,12
Brazil was the first country in Latin America to offer nationwide access to PrEP, which is provided free of charge through the Unified Health System (SUS). 13 Moreover, in 2020, the country reported the highest rate of PrEP use among all nations in the region. 14 However, this level of use still falls significantly short of the estimated 66,120 Brazilian MSM aged 15 to 64 years who, in 2018, were considered eligible and expressed willingness to use PrEP. 15
In this context, despite UNAIDS’ recommendation for prioritized access to PrEP and the target of 50% coverage among MSM and transgender individuals at high risk of HIV infection, PrEP remains underutilized in Brazil.10,16 Among HIV-negative MSM, PrEP acceptability is still limited, primarily due to individual barriers such as fear of side effects and concerns regarding adherence. 17
Therefore, it is necessary to develop studies and health interventions that address diverse HIV prevention strategies among MSM, as these measures are essential for promoting health and controlling the epidemic. Understanding the predisposition to use PrEP among MSM, that is, their intention to use it in the future, as well as the factors associated with this predisposition, can help encourage adoption of this strategy within a population at high risk of HIV exposure. Consequently, this study may contribute to future research and support health managers and professionals in designing strategies to overcome adherence barriers to PrEP within the target population.
Given this background, the objective of the present study was to analyze the predisposition to use PrEP for the HIV and the associated factors among MSM.
Methods
Study Design
This is a cross-sectional and analytical study conducted according to the guidelines of the Strengthening the Reporting of Observational Studies in Epidemiology tool.
Setting
The study was conducted at the Counseling and Testing Center (CTA, in Portuguese) in Teresina, the capital of Piauí, Brazil. To optimize data collection, and considering the difficulty of reaching this population, bars, public squares, and cultural spaces of social interaction frequented by the target population—as indicated by the study seeds—were also visited.
Population (Eligibility Criteria) and Sample Size Determination
The source population consisted of MSM residing in Teresina, Piauí, totaling 14,705 individuals.
18
Accordingly, the sample size was calculated using the following formula for an infinite population
19
:

Where n corresponds to the minimum sample size, z represents the score associated with the significance level for a 95% confidence interval (1.96), P indicates the estimated proportion of individuals with the event of interest—assuming a presumed prevalence of 50% predisposition to PrEP use among MSM, given the absence of national data on this event in the study population, and considering that this value maximizes the sample size—and finally, e corresponds to the tolerable sampling error, set at 5.5%. Based on these parameters, the minimum sample size was calculated to be 320 MSM.
MSM who had engaged in at least one sexual relationship with another man in the past 12 months and were aged 18 years or older were included. The exclusion criteria were being visibly under the influence of alcohol and/or drugs, living with HIV, or currently using PrEP.
The dependent variable was the predisposition to use PrEP. Independent variables addressed issues related to sociodemographic characteristics, sexual health, sexual practices, knowledge about PrEP, and perceived risk of HIV.
Sampling
Participant recruitment employed the non-probabilistic Snowball Sampling technique, commonly referred to as the “snowball” method. This method is used to locate rare or unknown populations that cannot be easily listed but are presumed to have connections through shared interests. Members of this population can identify others within it. This technique involves a primary data source, referred to as seeds, which nominate other potential participants for the study. 20
For the initial selection of seeds (wave zero) in the study, the Municipal Council for the Rights of Lesbians, Gays, Bisexuals, Travestis, and Transsexuals was asked to nominate MSM. From each “seed,” additional participants were invited, who, in turn, referred others, thereby forming successive recruitment cycles, referred to as “waves.” Recruitment was concluded once the estimated sample size for this study was reached.
Additional seeds were also recruited at the CTA, chosen for their self-reported extensive social networks. With the collaboration and information provided by these seeds, four social venues frequented by the target population—located in different geographic areas of the city—were visited to identify new seeds, resulting in a total of 11 seeds by the end of data collection. Importantly, when selecting seeds, sociodemographic diversity (such as age and household income) was considered, which was highly beneficial in minimizing participant concentration within a single sociodemographic profile.
MSM were instructed to attend the CTA at pre-scheduled times to participate in the study or to contact the research team by telephone to clarify any questions. No financial compensation was provided to study participants.
Data Collection
Data collection took place from November 2023 to July 2024. The procedures were conducted in two consecutive stages. In the first stage, rapid HIV testing and post-test counseling were offered to those who consented to participate. The testing and counseling process followed the recommendations of Ministry of Health Ordinance No. 151, dated October 14, 2009. 21
For testing, two types of rapid test kits were used: Rapid Check, produced by the Federal University of Espírito Santo laboratory, and Biomanguinhos, produced by Fiocruz. The methodology employed in the rapid test was immunochromatography for the detection of anti-HIV 1 and 2 antibodies. Each kit contained rapid tests, disposable pipettes and lancets, and reagent buffer solution. Participants were informed that the procedure was nearly painless, as it involved only a small finger-prick puncture, and testing was performed by healthcare professionals experienced in this technique. 22
For cases with positive results, participants received counseling and were referred for appropriate follow-up at the Specialized Care Services for HIV/AIDS in Piauí. They were also informed of their exclusion from the study. 22
The second stage consisted of interviews conducted using a questionnaire that included questions from three previously validated instruments and a risk perception scale, all of which were used with authorization from their respective authors.23–26 The first instrument was derived from the study “Validation of an Instrument: Online Sexual Media Consumption and HIV/AIDS Risk Practices,” 23 which underwent content validation by a committee of experts and semantic validation by the target audience, achieving a Content Validity Index of 100.0% and a positivity index of 99%. In the present study, it was used to identify personal characteristics, sexual health, and sexual practices.
The second instrument was developed and validated for use in the study entitled “Knowledge of Health Students about Pre- and Post-Exposure Prophylaxis for HIV.”²⁴ Content validation was performed by a panel of judges composed of PhD researchers with experience in the field of HIV/AIDS, yielding a Content Validity Coefficient of 0.8840. Subsequently, it was evaluated by the target audience, obtaining a positivity index of 100%. In this study, it was used to assess knowledge about PrEP. To classify MSM knowledge regarding PrEP, eight multiple-choice items were analyzed. One point was awarded for each correct response, resulting in a maximum score of 8 points (100%). Knowledge levels were categorized as “unsatisfactory knowledge” (<70% correct answers) and “satisfactory knowledge” (≥70% correct answers). Notably, some items allowed participants to select more than one option when applicable.
The third instrument assessed PrEP acceptability using one of the 13 items from the questionnaire applied in the study “Factors Associated with the Non-Acceptability of PrEP among Transvestites and Transgender Women in the Northeastern Region of Brazil,” 25 selected due to the relevance of that study, which was part of the PopTrans project. This item aimed to identify the willingness to use PrEP through the statement: “I would be willing to use PrEP to prevent HIV infection.” The possible responses were two, scored from 1 to 2: 1 = agree and 2 = disagree.
In addition, the HIV Risk Perception Scale, translated, adapted, and validated for Brazil by Torres et al (2021), 26 was applied. This scale measures how individuals assess their likelihood of contracting HIV. Internal consistency, assessed using Cronbach's alpha, showed values above 0.7. The scale consists of eight items encompassing cognitive (3 items), intuitive (3 items), and behavioral (2 items) aspects. Response formats ranged from four to six options, with a maximum score of 40 points (100%). Risk perception was classified as follows: 1%-79% = unsatisfactory; 80%-100% = satisfactory.
Ethical Aspects
This study complied with the principles established by Resolution No. 466/2012 of the Brazilian National Health Council, which addresses the ethical aspects of research involving human subjects (Brazil, 2012). The study was first submitted for institutional approval by the CTA and subsequently reviewed and approved by the Research Ethics Committee (CEP) of the Federal University of Piauí (UFPI), under opinion No. 6.415.820 and Certificate of Presentation for Ethical Consideration (CAAE) 73169023.6.0000.5214.
Participants were asked to sign the Informed Consent Form (ICF), at which time they were informed about the study objectives, data collection procedures, assurance of anonymity, the right to withdraw at any time, and the confidentiality of all data obtained.
Statistical Analysis
The data were organized in Microsoft Excel spreadsheets and analyzed using RStudio statistical software (version 2024.09.1 + 394). The Shapiro–Wilk test was applied to verify the assumption of normal or Gaussian distribution for continuous quantitative variables.
For univariate analysis, Simple Logistic Regression was used, with variable selection based on the Wald test at the 20% level. For multivariate analysis, to explain the combined effect of predictor variables on the response variable (predisposition to use PrEP among MSM), Multiple Logistic Regression (MLR) with a Bayesian approach was employed. The criterion for including variables in the logistic model was their association at the 20% level (P < 0.200) in the univariate analysis. The significance or retention criterion for variables in the model was their association at the 5% level (P < 0.05).
Finally, the goodness-of-fit test (Hosmer–Lemeshow Test) required for MLR showed that the final model is appropriate for explaining the response variable. Multicollinearity among explanatory variables was checked using the Variance Inflation Factor (VIF) test, with a cutoff point for diagnosing multicollinearity set at a VIF above four, leading to the exclusion of related explanatory variables. 27
Results
Out of 375 MSM approached, eight were excluded for being on PrEP, seven tested positive for HIV, and 40 declined testing, resulting in a final sample of 320 MSM, as planned.
Table 1 presents the sociodemographic profile of the MSM in the study, with a sample of 320 participants. Most participants, 290 (90.6%), were aged between 20 and 39 years; 239 (74.7%) identified as homosexual; 103 (32.2%) reported a family income exceeding four times the minimum wage; and 219 (68.4%) had completed higher education. When asked about their living arrangements, the majority, 204 (63.9%), stated they lived with parents and/or relatives.
Identification Profile of MSM in the Study. Teresina, PI, 2024 (n = 320).

Age (median) = 25 years.
Monthly family income (median) = 3.500.00 Current minimum wage = R$ 1.412.00.
Years of education (median) = 18.
Source: Research database.
MSM: who have sex with men.
Regarding sexual health, as shown in Table 2, in the past 12 months, the most frequently reported symptoms affecting the penis and/or anus were itching or irritation, noted by 46 participants (14.4%). In terms of diagnosed STIs during the past year, syphilis was reported by 45 (14.1%). Concerning HIV testing, 251 (78.4%) had been tested in the last 12 months, 41 (12.8%) more than 12 months ago, and 28 (8.8%) had never been tested for HIV. Among those who had been tested, 195 (60.9%) underwent testing at a CTA.
Sexual Health of MSM in the Study. Teresina, PI, 2024 (n = 320).

Source: Research database.
*Question with multiple answers.
HIV, human immunodeficiency virus, MSM, who have sex with men; CTA, Counseling and Testing Center.
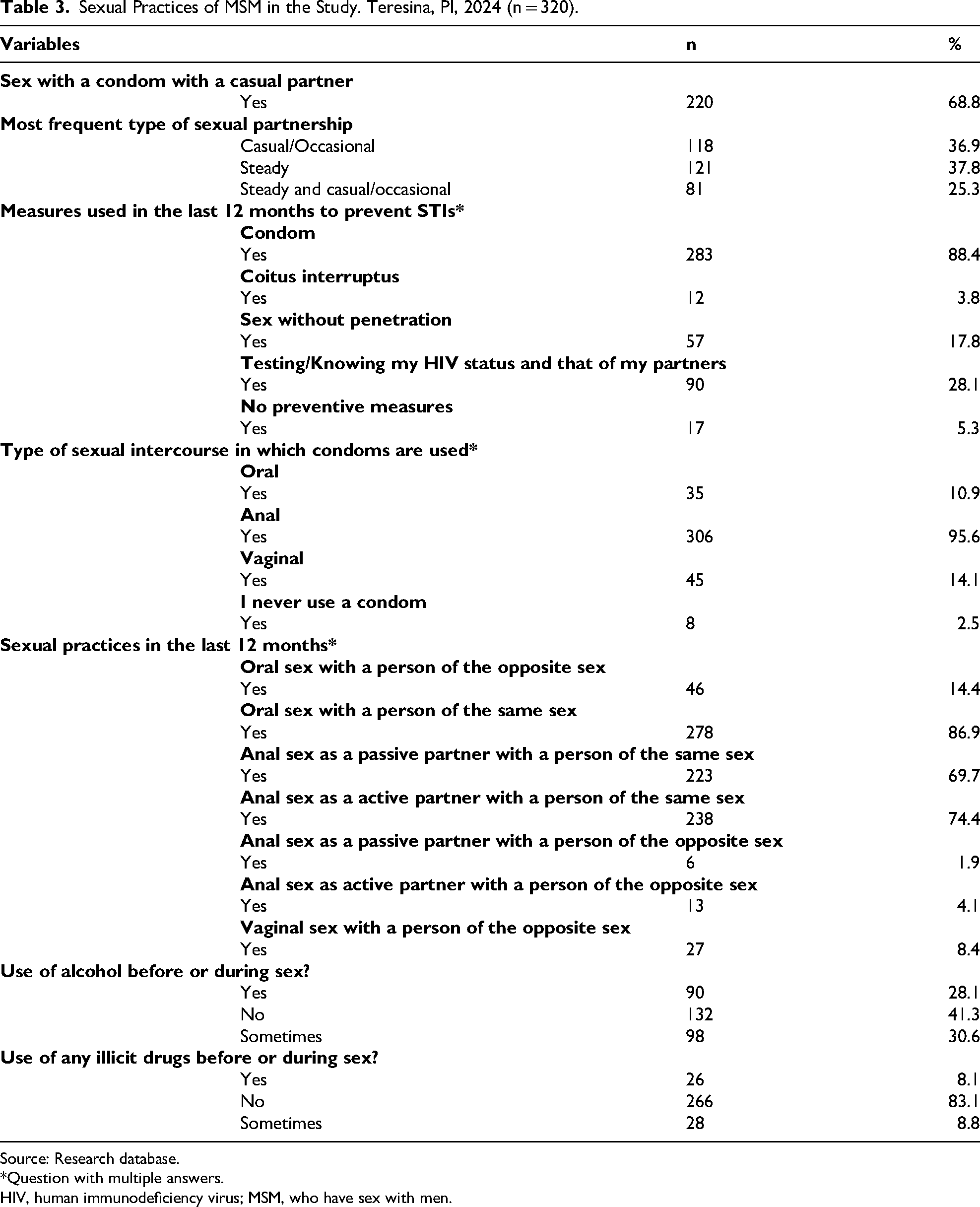
In terms of sexual practices, as shown in Table 3, 220 (68.8%) reported using condoms with casual partners, and 121 (37.8%) reported having a steady sexual partner. Among the most commonly used prevention measures over the past 12 months, condom use was reported by 283 (88.4%). Regarding the type of sexual activity for which condoms were used, anal intercourse predominated, with 306 (95.6%) participants reporting its use.
Sexual Practices of MSM in the Study. Teresina, PI, 2024 (n = 320).
Source: Research database.
*Question with multiple answers.
HIV, human immunodeficiency virus; MSM, who have sex with men.
Table 4 shows that 297 (92.8%) were predisposed to using PrEP for HIV prevention, 262 (81.9%) had unsatisfactory knowledge about PrEP, and 271 (84.7%) had an unsatisfactory perception of their risk for HIV.
Predisposition to PrEP Use, Classification of Knowledge, and HIV Risk Perception Among MSM in Teresina, PI, 2024 (n = 320).

Source: Research database.
*Confidence interval for proportion.
HIV, human immunodeficiency virus; MSM, who have sex with men; PrEP, pre-exposure prophylaxis.
In Table 5, it is evident that the likelihood of predisposition to PrEP use increased 5.56-fold among MSM with higher education (P = 0.046), 3.08-fold among those with STI signs/symptoms in the past 12 months (P = 0.041), and by 69% among MSM with satisfactory knowledge about PrEP (P = 0.045).
Logistic Regression of Predisposition to PrEP Use Among MSM in Teresina, PI, 2024 (n = 320).

Legend: *Crude Odds Ratio (ORb) *Adjusted Odds Ratio (ORa) Hosmer and Lemeshow test: P = 0.491.
Pseudo R2: 0.1951.
HIV, human immunodeficiency virus; MSM, who have sex with men; PrEP, pre-exposure prophylaxis.
Discussion
The results presented in this study demonstrate a high predisposition to the use of PrEP among MSM. In general, it was observed that higher education, the presence of signs/symptoms of STIs, and satisfactory knowledge were associated with a greater predisposition to PrEP use for HIV prevention among the MSM in the sample.
The descriptive analysis of sociodemographic characteristics identified that the MSM population was predominantly young. Although no association was found between age and predisposition to PrEP, it is worth noting that older participants may be less likely to report interest in PrEP than younger participants. Thus, greater emphasis on preventive measures among the younger population, due to the increasing incidence of HIV, may contribute to higher predisposition in this group. 28
The predisposition to PrEP observed in this study exceeded the findings among global MSM populations, where the predisposition to use PrEP was approximately 57.8%. 8 In Brazil, other studies have shown lower rates of predisposition to PrEP. A study aimed at evaluating awareness of PrEP also reported a lower rate than the present study, corresponding to approximately 56% willingness to use PrEP. 29 Furthermore, only 44% of participants from a city in the Brazilian Northeast stated they would be willing to use PrEP. 13 Conversely, the PrEPBrasil demonstration study reported a high PrEP acceptability rate of approximately 82.1%. 30
It is important to emphasize that although predisposition rates are considered high in the literature, the rate of PrEP use does not align with this trend. Despite the progress in expanding PrEP use in Brazil since 2018, among the 15.4% of MSM eligible for PrEP, currently, less than 50% are using it. The UNAIDS Global AIDS Strategy 2021-2026 recommends continuous efforts to reduce barriers to access.14,31
A systematic review and meta-analysis involving 14,040 MSM from low- and middle-income countries that evaluated awareness and willingness to use oral PrEP identified factors affecting predisposition across individual, demographic, social, and structural domains. In the individual domain, insufficient knowledge about PrEP, doubts about its efficacy, fear of side effects, low perception of HIV risk, and the need for frequent medication adherence reduced willingness to use PrEP, while education about PrEP and motivation to maintain health facilitated potential use. 32
Demographic factors such as education, age, and migration can influence both awareness and willingness to use PrEP. In the social domain, stigma related to sexual orientation and PrEP were barriers to potential PrEP use, whereas partner, peer, and family support facilitated potential use. In the structural domain, concerns about healthcare professionals’ attitudes, quality assurance, data protection, and cost were determinants of potential use. 32
When analyzing the association of sociodemographic factors with the predisposition to PrEP use, this study observed that education positively influenced the predisposition to PrEP use, particularly among those with higher education degrees. This association has also been demonstrated in other studies.8,32–34
Thus, higher education is associated with a greater willingness to use PrEP, primarily due to increased opportunities to acquire knowledge about prophylaxis. 35 Knowledge about PrEP was associated with a higher predisposition to its use in the sample of the present study. This can be explained by the growing recognition that knowledge about HIV prevention modalities facilitates their acceptance. 36
Additionally, studies corroborate that individuals with greater knowledge about HIV are more likely to engage with prevention services.37,38 Conversely, a lack of understanding regarding the efficacy and/or side effects of PrEP may lead to decreased willingness to use it. 39
A cross-sectional study with MSM conducted in Brazil demonstrated a high level of HIV knowledge and its significant association with a greater likelihood of PrEP use. Consequently, increasing the dissemination of information about HIV prevention and PrEP may contribute to higher PrEP use among eligible MSM in Brazil. 34
It is important to note that knowledge about PrEP in this study was lower than in developed countries such as the United States and Portugal.40,41 Furthermore, knowledge about PrEP among MSM was also lower when compared to the results of a meta-analysis conducted in low- and middle-income countries (29.7%), which is concerning given that the participants of this study have a high level of education. 32 In Brazil, the PrEPBrasil demonstration study also showed greater knowledge related to PrEP when compared to the findings of the present study. 30 It is worth emphasizing that geographical variability in Brazil and social disparities may influence PrEP knowledge and acceptability.13,30
It is also noteworthy that a high level of knowledge does not necessarily imply a high predisposition to PrEP use. A study conducted in Mexico reported a PrEP knowledge prevalence of 81.3% alongside a use intention rate of 34.2%. 34 Conversely, in alignment with this study, research conducted in Benin with MSM reported a low prevalence of PrEP knowledge (50.7%) but a high prevalence of use intention (90%). 42
One notable finding in this study pertains to the fact that the high rate of unsatisfactory HIV risk perception was not significantly associated with predisposition to PrEP use. However, the presence of a risk indicator, having signs/symptoms of STIs in the past 12 months, strongly increased the likelihood of predisposition to use. In this specific aspect, the results align with those of a systematic review conducted between 2000 and 2020, which revealed that high-risk HIV infection indicators—such as unprotected anal sex, diagnosed STIs in the past 12 months, having six or more sexual partners, or participating in behavioral HIV interventions in the past 12 months—were associated with greater willingness to use PrEP among MSM. 43
It is important to emphasize that the literature widely affirms that risk perception is a key factor in determining the adoption of risk-reduction activities. Individuals who do not perceive themselves at risk for HIV may not see the need to participate in risk-reduction activities.44,45
Thus, low HIV risk perception has been cited as a barrier to PrEP acceptance both in the general population and among groups at higher risk of HIV acquisition, such as MSM.44,45 Previous studies indicate that populations with a higher likelihood of contracting HIV have demonstrated a lower predisposition to use PrEP.46,47
Risk awareness, the desire to minimize the possibility of infection associated with recurrent unprotected anal sex (bareback), and a history of other STIs may lead individuals to seek health services, raising awareness of the importance of this strategy and motivating them to consider using PrEP as a preventive measure. 48
Moreover, the discrepancy between perceived HIV risk and actual risk, particularly based on engagement in risky sexual behaviors, highlights the need for interventions to improve awareness of risky sexual behaviors and thereby enhance the accuracy of risk perceptions. 49 A cohort study conducted in China from 2013 to 2015, which applied the Protection Motivation Theory to study PrEP adherence among MSM, revealed that higher threat perception and stronger susceptibility increased the motivation to adhere to PrEP. 50
PrEP is thus an essential component of combination prevention and is highly effective in preventing HIV acquisition when taken as prescribed. Expanding PrEP access is crucial to achieving the Sustainable Development Goals and ending the AIDS epidemic by 2030. 51 However, despite PrEP being recommended for individuals at substantial risk of HIV acquisition by the WHO since 2014, its availability remains limited in Latin America. It is estimated that only 10% of PrEP users in 77 countries are in Latin America, most of whom are in Brazil. 52
This study presented some limitations, particularly concerning the generalizability of the results to the MSM population, as participants were recruited using the snowball sampling technique. It is noteworthy that this method was chosen due to the difficulty in accessing the population. To ensure a more representative outcome, seeds from different social contexts were selected to minimize the risk of bias related to income, age, education level, and other factors. Another limitation was related to resistance to HIV testing, which was mitigated through clarifications and relevant information, as well as by offering a safe and confidential location.
Nevertheless, the study presents important strengths, particularly due to the absence of prior national data on predisposition to PrEP use among MSM in Teresina, Piauí, Brazil, thus addressing a relevant gap in the literature. Furthermore, the study provided participants with knowledge of their HIV serological status, fostering engagement with health education initiatives. In addition, it enabled the investigation not only of predisposition to PrEP use but also of the factors associated with this predisposition. In this sense, the study could be expanded to other similar geographic regions, both in Brazil and in other South American countries.
Conclusion
There was a high predisposition to PrEP use among MSM in the sample. Factors associated with PrEP predisposition included higher education levels (college degree), satisfactory knowledge about PrEP, and having experienced signs and symptoms of STIs in the past 12 months. Additionally, high rates of non-condom use during oral sex and unsatisfactory HIV risk perception were observed.
It is recommended that future studies adopt methodological approaches that allow for the generalization of results, such as longitudinal studies and more robust sampling techniques like Respondent-Driven Sampling, as well as qualitative approaches to more effectively explore individual motivations. Moreover, this study encourages reflections on the development and implementation of public policies related to PrEP access, particularly in the state of Piauí, where availability remains limited and concentrated in a few municipalities. This centralization poses significant challenges for raising awareness, increasing knowledge, and initiating this preventive strategy.
Footnotes
ORCID iDs
Ethical Approval and Informed Consent Statements
The study was submitted to and approved under protocol no. 6.415.820 by the Research Ethics Committee (CEP in Portuguese) of the Federal University of Piauí (UFPI in Portuguese). Eligible participants who agreed to participate signed the Free and Informed Consent Form (TCLE in Portuguese), ensuring the confidentiality and privacy of MSM during data collection.
Ethical Aspects
This study complied with the principles established by Resolution No. 466/2012 of the Brazilian National Health Council, which addresses the ethical aspects of research involving human subjects (Brazil, 2012). The study was first submitted for institutional approval by the CTA and subsequently reviewed and approved by the Research Ethics Committee (CEP) of the Federal University of Piauí (UFPI), under opinion No. 6.415.820 and Certificate of Presentation for Ethical Consideration (CAAE) 73169023.6.0000.5214.
Participants were asked to sign the Informed Consent Form (ICF), at which time they were informed about the study objectives, data collection procedures, assurance of anonymity, the right to withdraw at any time, and the confidentiality of all data obtained.
Authors Contributions
Conceptualization was done by YKCS, CPBV, LTN, RLBM, PTMB, and TMEA. Data curation was done by YKCS, ÁFLS, APMF, LAC, TMF, CPBV, LTN, RLBM, PTMB, and TMEA. Formal analysis was done by YKCS, ÁFLS, APMF, LAC, TMF, AGSJ, WDDO, CPBV, LTN, RLBM, PTMB, and TMEA. Funding acquisition was done by YKCS, AGSJ, and AFLS. Investigation was done by YKCS, CPBV, AGSJ, WDDO, LTN, RLBM, PTMB, and TMEA. Methodology was done by YKCS, CPBV, AGSJ, WDDO, LTN, RLBM, PTMB, and TMEA. Project administration was done by YKCS, CPBV, LTN, RLBM, PTMB, and TMEA. Resources was done by YKCS, CPBV, LTN, RLBM, PTMB, and TMEA. Software was done by YKCS, CPBV, LTN, RLBM, PTMB, and TMEA. Supervision was done by YKCS, ÁFLS, APMF, LAC, TMF, AGSJ, WDDO, CPBV, LTN, RLBM, PTMB, and TMEA. Validation was done by YKCS, ÁFLS, APMF, LAC, TMF, CPBV, AGSJ, WDDO, LTN, RLBM, PTMB, and TMEA. Visualization was done by YKCS, CPBV, LTN, RLBM, PTMB, and TMEA. Writing–original draft was done by YKCS, ÁFLS, APMF, LAC, TMF, AGSJ, WDDO, CPBV, LTN, RLBM, PTMB, and TMEA. Writing–review & editing was done by YKCS, ÁFLS, APMF, LAC; TMF, AGSJ, WDDO, CPBV, LTN, RLBM, PTMB, and TMEA.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES) – Finance Code 001; Universidade Federal de Mato Grosso do Sul- Brasil (UFMS) - Finance Code 001 and Fundação de Apoio ao Desenvolvimento do Ensino, Ciência e Tecnologia do Estado de Mato Grosso do Sul (FUNDECT).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are not publicly available due to ethical restrictions involving human participants.