
Abstract
Female pigs are commonly utilized as an animal model for biomedical research and require urethral catheterization. Sixteen pigs were anaesthetized for research purposes and required the placement of a urethral catheter. Post-mortem examination of the vaginas revealed the urethral opening to be consistently halfway from the mucocutaneous junction of the vulva to the cervix. A shallow diverticulum was also observed on the ventral floor of the urethral opening. To optimize conditions for success the pig should be carefully positioned supine, a vaginal speculum and light source should be used, the pig should be adequately anaesthetized, and the anatomy of the vagina should be reviewed.
Female pigs are commonly utilized as an animal model for biomedical research and a urethral catheter is placed for a range of reasons: measurement of intra-abdominal pressure; 1 placement of pressure sensors in the urinary bladder wall; 2 serial urine sampling; 3 cystoscopy; 4 to cause injury to the urethral sphincter; 5 and intra-operative measurement of urine output and bladder drainage.6–8
The procedure for insertion of a urinary catheter is not usually described in any detail in scientific publications. In one publication the sows were conscious for placement of the catheter 3 but it is more common that the pigs are anaesthetized.4,9 The position of the animal also varies and may be prone 2 or supine. 9 Male pigs are not suitable for urethral catheterization as the tip of the penis is cork-screw shaped 10 although a suprapubic cystotomy and placement of a catheter has been utilized in males. 11
For two projects requiring prolonged (6–11 h
Large white (Sus scrofa) pigs were sourced commercially (GD Pork Pty Ltd, West Pinjarra, Western Australia) and acclimatized to the animal facility for at least one week prior to anaesthesia. During this time they were housed in communal pens (4 × 5 m), fed a maintenance diet (Pig Grower; West Feeds Pty Ltd, Welshpool, Australia) with fresh pumpkin and apples and allowed free access to water. Environmental enrichment was provided with music, various toys and daily human interaction. Prior to anaesthesia food was withheld for 12–24 h.
Anaesthesia was induced with a combination of zolazepam and tiletamine as Zoletil 100 (4 mg/kg; Virbac Australia Pty Ltd, Milperra, NSW, Australia) and xylazine (2 mg/kg, Ilium Xylazil 100 mg/mL; Troy Laboratories Australia Pty Ltd, Glendenning, NSW, Australia) by intramuscular injection in the neck. An auricular vein was cannulated and propofol (1–2 mg/kg, 1%; Norbrook Laboratories Ltd, Tullamarine, Victoria, Australia) was administered intravenously if required to achieve an adequate depth of anaesthesia for orotracheal intubation. Anaesthesia was maintained in accordance with the project protocol. The pig was positioned supine with a folded towel under the rump to raise the pelvis and lumbar spine, and the hindlegs were pulled cranially. A disposable lubricated vaginal speculum (designed for women) was inserted to visualize the external urethral opening, and blunt-tipped forceps controlled the tip of a Foley catheter French size 8 or 10 with a stylet placed in situ as described. 9 Once the catheter was inserted a closed system drainage bag was connected to the Foley catheter and secured with adhesive tape to the tail.
Urethral catheterization was attempted in 16 pigs over a five-week period. In one study (n = 10) pigs recovered from the procedure and in the other (n = 6) they were humanely euthanized at the end of the procedure in accordance with the study protocol. The total anaesthesia time was between 6 and 11 h. The mean (SD) weight of the pigs was 35.6 (4.6) kg. The catheter was removed at the end of each procedure. Following euthanasia in the six pigs the vagina was removed to examine the gross anatomy.
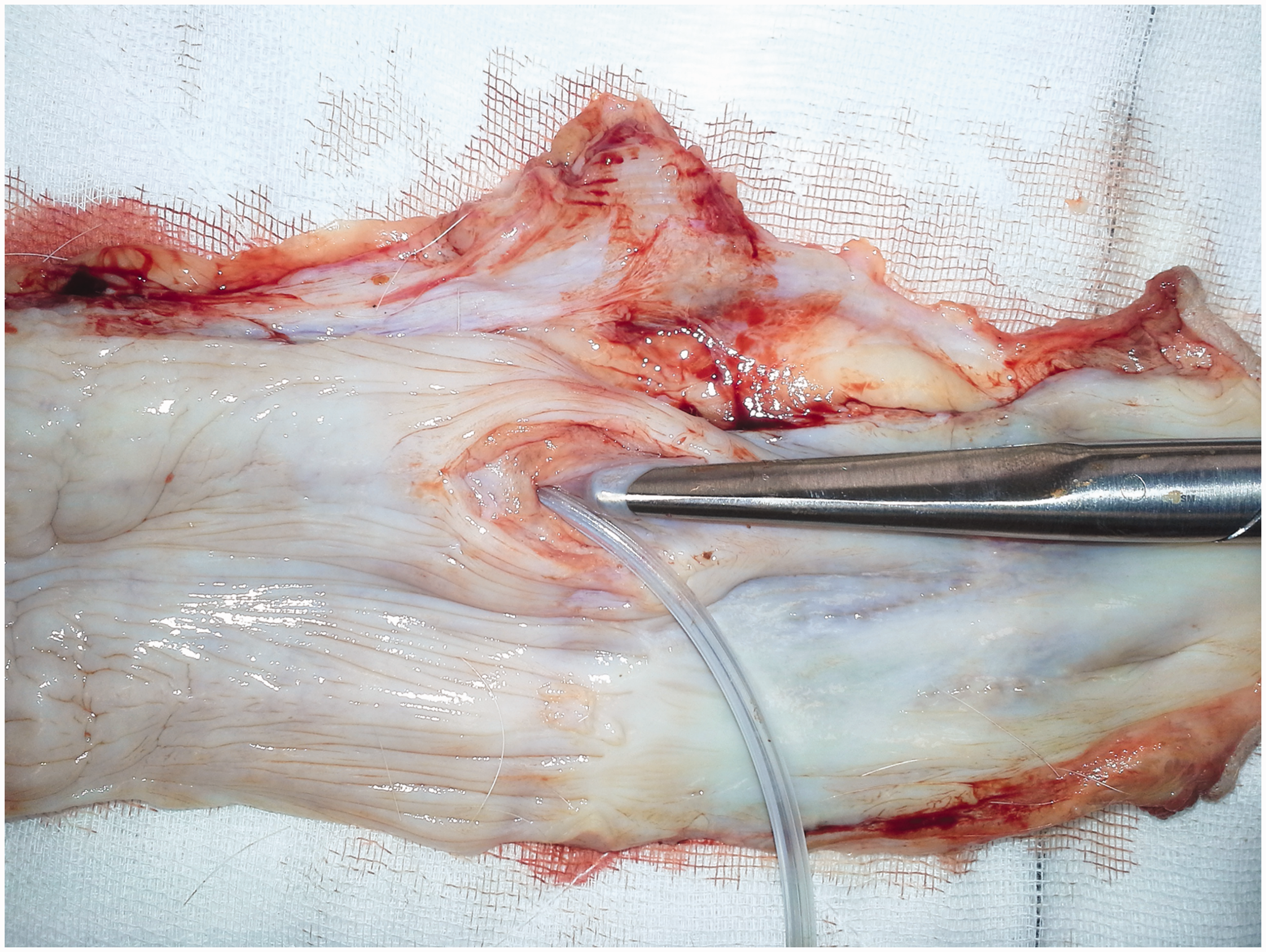
Although catheterization of the urethra was successful in 15 pigs the placement of the catheter was unexpectedly challenging and took up to 60 min in some animals. Post-mortem examination of the vaginas revealed the urethral opening to be consistently halfway from the mucocutaneous junction of the vulva to the cervix (Figure 1). A shallow diverticulum was also observed in the six pigs on the ventral floor of the urethral opening (Figure 2). This suburethral diverticulum is normal in pigs.
13
A representative example of the vagina of a pig incised along the dorsal wall to expose the urethral opening. The scissor tips mark the urethral opening and the distal border of the cervix. The urethral opening is halfway between the mucocutaneous junction of the vulva and the cervix. Vagina of a pig incised along the dorsal wall to expose the urethral opening. The urethral opening has been partially incised along its dorsal wall. The scissor tip is in the shallow thin-walled suburethral diverticulum on the ventral floor of the urethral opening. A Foley catheter is in the urethra.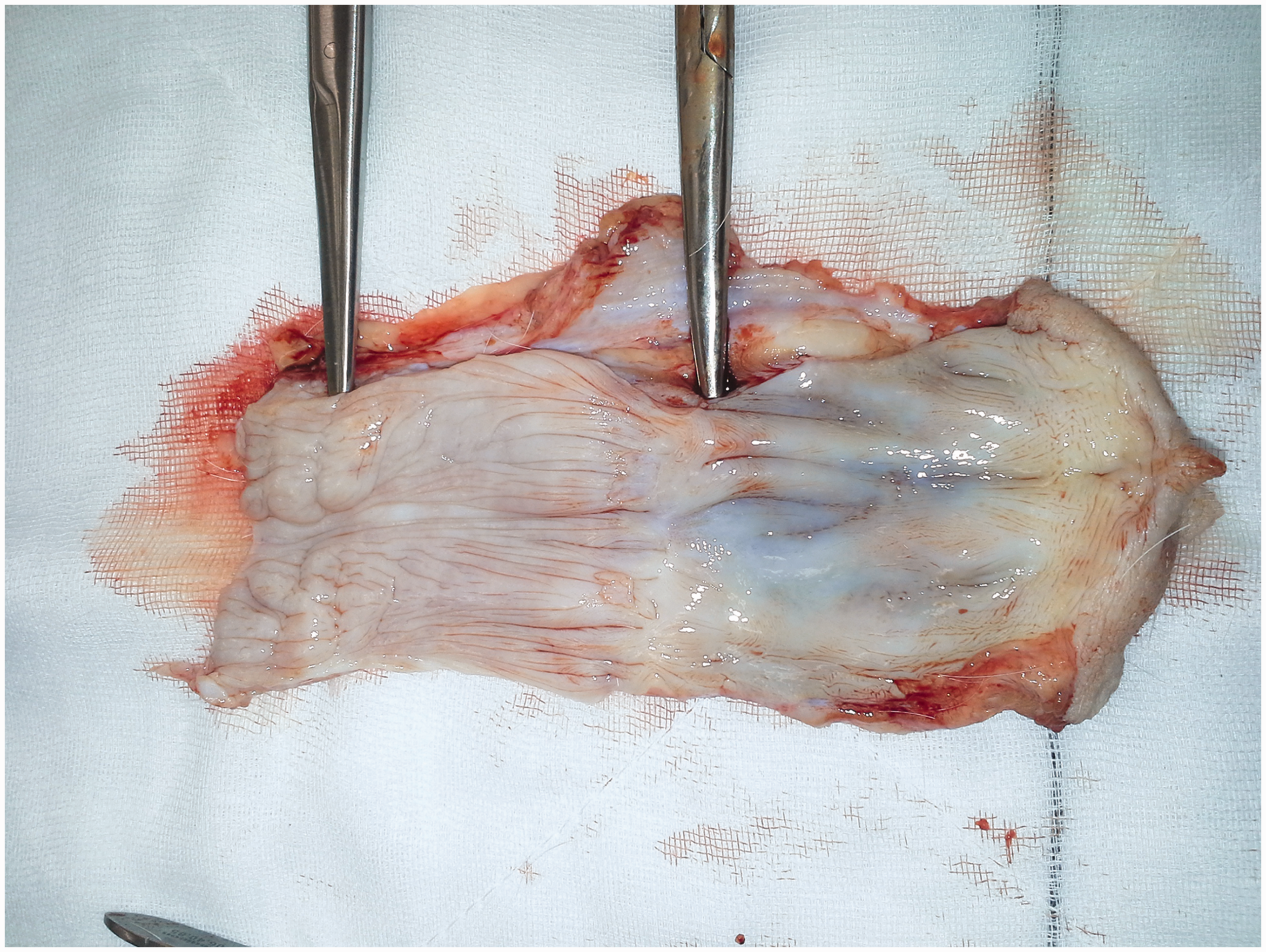
In 2011 Ettrup et al. gave a step by step account of the procedure for placement of a urethral catheter in female pigs. 9 This description is a useful starting point but does not give any indication of the difficulties the procedure may present. Despite our combined veterinary, anaesthesia and surgical experience the procedure took longer than we anticipated. If the placement of a urethral catheter is required generous time should be allocated for the procedure.
In conclusion the following practical points are intended to aid personnel placing urtheral catheters in female pigs during anaesthesia:
Pigs must be adequately anaesthetized for the procedure. The pig should be in dorsal recumbency (supine). A folded towel placed under the rump will raise the pelvis and lumbar spine and the hindlegs should be pulled cranially. Although the urethral opening is one-half of the distance to the cervix the wall of the vagina tends to fall inwards so it can be very difficult to find. Inversion of the urethral opening can make entry difficult so adjusting the angle of the pelvis and direction of the hindlimbs slightly may help to visualize the urethral opening and allow entry into it. A lubricated vaginal speculum and a focused light source should be used to visualize the vaginal wall and urethral opening. An appropriately sized Foley catheter with a stylet should be used. Blunt-tipped long forceps (e.g. Sawtell forceps) are essential to manoeuver the tip of the catheter through the long and narrow vagina towards the urethral opening. The catheter should be advanced along the ventral fold of the vaginal wall (at a 12 o’clock position in supine). If the catheter does not advance easily it may be in the suburethral diverticulum or in the cervix. Try altering the position of the pelvis and attempt again. To confirm correct placement of the catheter remove the stylet and check for the flow of urine. If there is no flow of urine commence the procedure again but be cautious to maintain asepsis.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.