
Abstract
Children in resource-constrained Global South settings face safety and mental health risk factors, often with limited access to support. Forty-four parents in South Africa and Pakistan conceptualized vulnerabilities and required support. Thematic analysis of focus group data resulted in three themes of contextual influences, child rearing practices and joint care pathways. The findings highlight the importance of integrated child protection and mental health awareness and interventions, and interdisciplinary training. In Global South countries, social workers are ideally positioned to drive partnerships between structural and informal community-based support systems, and thus continuously align policy, protocols and interventions with local sociocultural values.
Introduction
The strong association between children’s safety and their mental health is well established globally, across different sociocultural contexts (UNICEF, 2021). For example, many studies highlighted high rates of mental health problems among children who suffered abuse and neglect (Maclean et al., 2019). The large body of evidence has created a better understanding of underpinning mechanisms of risk, and their importance for social work practice. In terms of mechanisms, research shows that the onset of child mental health conditions is typically explained by interlinked risk factors such as living in socioeconomic disadvantage, disrupted attachments, recurrent exposure to trauma such as gender-based and community violence, and parental substance use or poor mental health (Green et al., 2020). Conversely, mental health problems increase vulnerability to further victimization and exploitation during young life (Skoog and Kapetanovic, 2021).
Literature review
While much of this research originates from Global North countries, there is a growing body of research in countries in the Global South, given the high rates of violence, that examines sociocultural factors influencing protection and mental health (e.g. North et al., 2020). In resource-constrained settings such as informal settlements, children are particularly vulnerable to experiencing a lack of basic needs like housing and nutrition, unsafe neighbourhoods, impaired adult supervision because of competing economic pressures for parents, experience of violence within the family and community, illegal labour, child marriage and sexual exploitation (Reza and Bromfield, 2019). Many children are exposed to multiple protection incidents (polyvictimization), which in turn increase the risk of mental health problems (Le et al., 2018). Such difficulties become sustained and more challenging, as children often do not speak out.
Several barriers have been identified in reporting and help-seeking such as a culture of adults mistrusting children’s accounts, and fear of consequences from the perpetrator or other adults (Figge et al., 2022). Crucially, there is wide variation in child protection terminology, underpinning policy, legal thresholds, structure of social services systems and positioning of social work within statutory or community systems (Crea et al., 2018). Structural social and mental health care are usually faced with overwhelming need, limited capacity and funding – especially for community-based family preservation, and because they tend to operate in silos (Strydom et al., 2020). Externally driven tensions with community cultural beliefs and practices are not uncommon, as the conceptualization of child safety, mental health and parenting are influenced by sociocultural factors. These concepts may be understood and defined according to traditional or local ‘norms’, perceptions of childhood, poverty (e.g. taking on carer role), and gender stereotypes (Khalil et al., 2020; Ramos de Oliveira et al., 2024).
Nevertheless, protection in Global South collective societies can be buffered by informal supports of extended family, community and religious networks, which may thus strengthen children’s resilience and positive mental health (Theron and Ungar, 2023). This evidence indicates the importance of joined up protection and mental health interventions, often within child development, nutrition and educational programmes, both informal and structural, and across children’s socioecology (Krishna et al., 2021). Such collaborative efforts largely rely on early detection, help-seeking and response.
Parents are central to both vulnerability and help-seeking mechanisms. In addition to the well-established risk factors of parental ill mental health and harsh parenting strategies for child safety and mental health, mothers in the Global South are more likely to be affected by multiple factors such as socioeconomic disadvantage, lack of social support and exposure to gender-based violence, which in turn increase risk for children (Burger et al., 2020). Despite the evolving knowledge on how various stakeholders perceive child safety and mental health, there has been limited research on how parents in the Global South understand this interface and appropriate support needed. This is important, because recent evidence indicates that children under ongoing threat can benefit from psychological interventions, albeit these need to be adapted to sociocultural contexts and joined up with safety measures (Yim et al., 2024). This research gap and importance for social work practice and social care services informed the rationale for this study, which is also important for other Global South contexts.
Methodology
The aim of this study was to explore the perspectives of parents and caregivers in two resource-constrained urban settings in South Africa and Pakistan on child safety and mental health, the relationship between these concepts, and the informal and structural support systems that could enhance them. A qualitative research design was selected to capture the voices and experiences of such a marginalized and seldom heard group.
Research setting and study sample
Two Global South countries were included, to provide different sociocultural contexts. Similarities between South Africa and Pakistan include high inequality, poverty and associated risk factors, an increasing child population and informal settlements characterized by inadequate service delivery (Organization for Economic Co-operation and Development [OECD], 2016). Potential differences include culture, religion, socio-political context, nature of community support, service systems and traditional sources of help for mental health issues (Pakistan Bureau of Statistics, 2018; South African Child Gauge, 2024). Although this study was not framed as a comparative research design, the inclusion of two sites could enable the identification of emerging cross-cutting or context-specific themes to inform policy and practice in other Global South settings.
In South Africa, children have high rates of child protection and mental health needs, which are both exacerbated by socioeconomic risk factors such as extreme poverty, gender-based violence, loss of parents and refugee status (UNICEF South Africa, 2025). However, only 5 percent of the healthcare budget is allocated to mental health (National Planning Commission, 2024), and there are limited specialists across the country (South African Council for Social Service Professionals, 2025; World Health Organization, 2024). The study was conducted in the City of Ekurhuleni in Gauteng Province (population 3,774,638 – COGTA, 2020).
Pakistan is similarly under-resourced in terms of overwhelming and unmet child protection and mental health needs. In recent years, 25 child protection units and 760 community-based child protection committees have been set up, although these largely rely on international partners such as UNICEF to address incidents related to child marriage, gender-based violence, regional conflicts and humanitarian disasters (UNICEF Pakistan, 2023). Services are largely adult- and hospital-based; for example, only 1 percent of out-patient clinics are child-specific, with significant specialist workforce shortages, with only 0.4 percent of the healthcare budget is being allocated to mental health (Dayani et al., 2024; World Health Organization, 2024). We included four disadvantaged areas in the city of Karachi (target population 2,262,480 – Pakistan Bureau of Statistics, 2018).
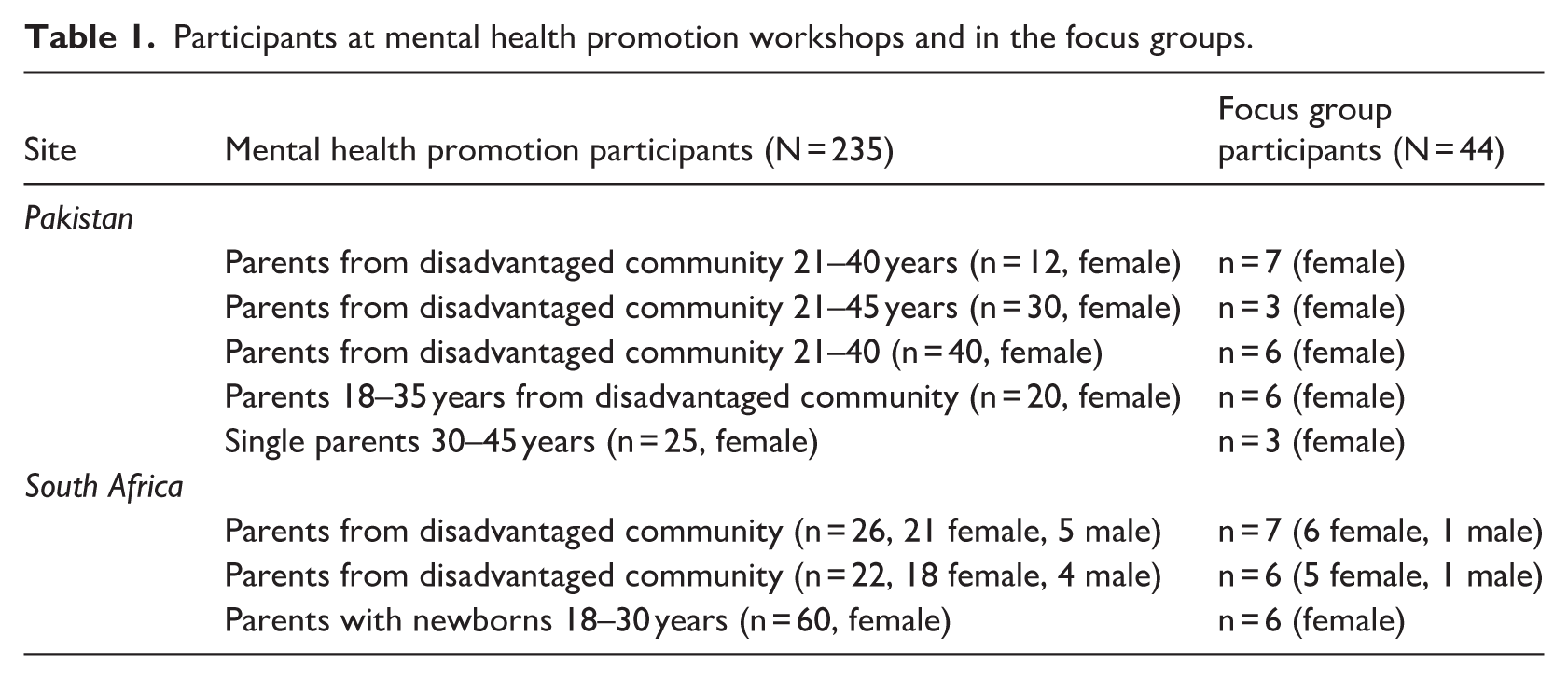
The study was hosted by two non-governmental organizations (NGOs), which provided psychosocial support to children and parents, and which acted as gatekeepers for safeguarding and recruitment. This article is based on the secondary analysis of two datasets from a larger project on parent mental health promotion in Global South resource-constrained settings. The design, implementation and perceived impact of mental health promotion workshops by various stakeholders have been published elsewhere (Vostanis et al., 2024a, 2024b). The data were revisited in relation to the above research aim. Following the mental health promotion workshops, invitations were sent to all participants to also attend focus groups. Of those, through purposive sampling, 44 parents provided informed consent and participated in this study (19 in South Africa and 25 in Pakistan). The sample within each study was selected according to thematic saturation criteria. Recruitment was completed between 2021–2022 in South Africa and 2022–2023 in Pakistan. The profile of participants attending mental health promotion workshops and of participants in this study are presented in Table 1.
Participants at mental health promotion workshops and in the focus groups.
Data collection
Focus groups engage participants in collective conversations in relation to their experiences, insights and perspectives (Adler et al., 2019). These can promote parent empowerment by confronting stereotypes and stigma, deepening our understanding of the contextual conditions promoting empowerment, shared learning and collaboration (Hall et al., 2023). Eight focus groups were facilitated by an independent researcher in each country, in isiZulu in South Africa and in Urdu language in Pakistan. The topic guide explored parents’ perspectives of child mental health needs, risk and protective factors, and required informal and structural support. Focus groups were held at community venues and were audio-recorded. Ethics approval was granted by the University of Leicester Research Ethics Committee in the UK. All participants provided written informed consent.
Data analysis
Data were audio-recorded, transcribed to isiZulu and Urdu respectively, by members of the research team, and translated to English. We utilized thematic analysis to attend to the data, engaging with a codebook approach to allow for conflation of inductive and deductive coding processes, and to ensure analyst collaboration and dialogue through a multiple coding process (Braun and Clarke, 2022). We drew on the principles of the codebook approach, template analysis, to integrate data, explore concurrently all perspectives in relation to the research aim, and allow space for coder conversations through the creation of integrative themes (Brooks et al., 2015). Data were initially coded by author 1. Author 5 independently coded one-third of the transcripts, and authors 1 and 5 met and discussed the codebook in three meetings. The research team helped resolve any discrepancies, by combining multicultural perspectives, both ‘insider’ and ‘outsider’, to the participating countries, thus minimizing potential bias to data collection and interpretation. Subject confidentiality was ensured through anonymized and coded transcripts, and exclusion of quotes that could indirectly identify participants.
Results
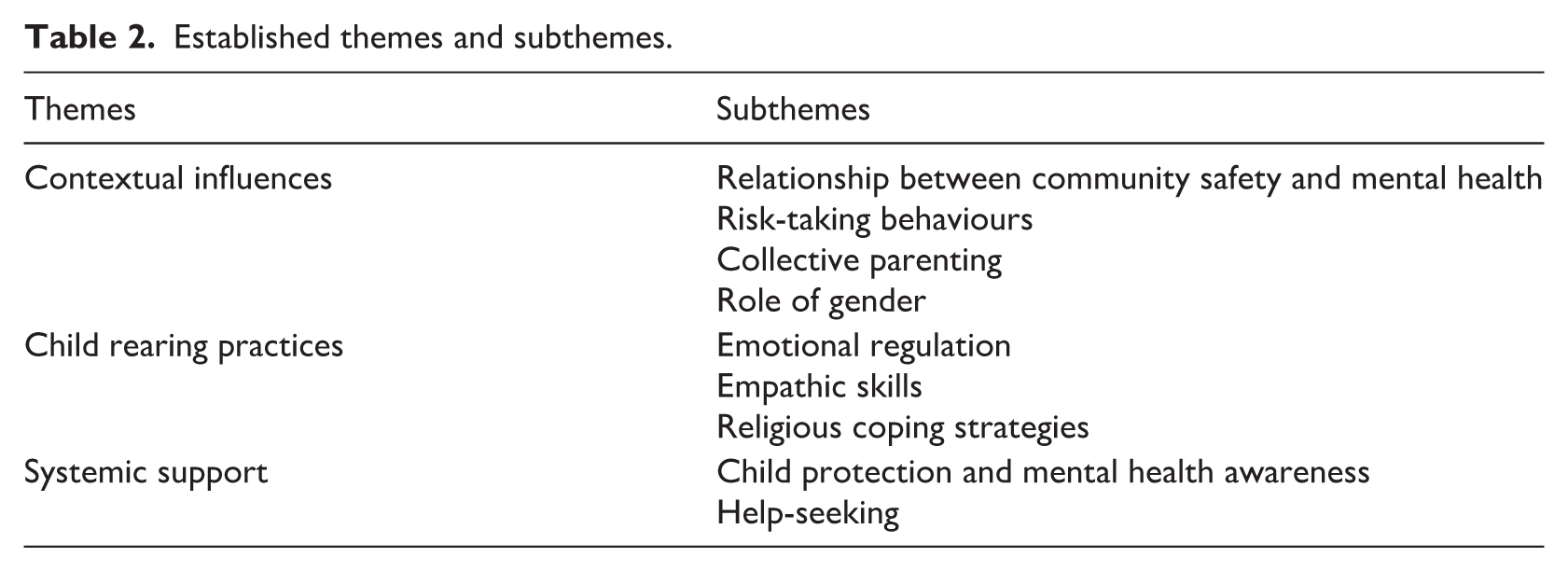
The created themes and subthemes, which outline perceived factors or mechanisms that relate to child safety, mental health and wellbeing, as well as end users’ views on support systems, are summarized in Table 2. These are subsequently described in more detail, with supporting excerpts. The themes were interlinked, as participants reflected on various contextual factors in their communities that compromised child safety and mental health, the impact of both negative and positive parenting strategies, and the role of support systems in enhancing community awareness and help-seeking.
Established themes and subthemes.
Theme 1: Contextual influences
Contextual influences, such as exposure to or experiences of abuse, and mental health stigma were interconnected and viewed as important by participants, as they navigated the challenges faced by children in their community. Initially, parents referred to ‘abuse’ as extra-familial incidents, although further during the conversations they provided examples of intra-familial maltreatment (Theme 2 below).
Child abuse is a topic which always scares me, and it is scarier that it can happen to anyone, and it can happen to any child. (Pakistan, FG3, Parent 4) We often feel shy talking to the children and then we see increasing cases of abuse. Our area is especially vulnerable in this case. Day-by-day we see increasing number[s] of child abuse cases. (Pakistan, FG3, Parent 1)
Participants recognized that individual and environmental vulnerabilities were often closely associated along a child’s life trajectory. For example, they connected mental health with youth risk-taking behaviours such as alcohol and substance use, which were often attributed to peer pressure.
I don’t know what to say, these 2000s need serious lessons, and when you look at the age when these children start using nyaope [street drug]. This is the age. (South Africa, FG7, Parent 2) Maybe not that we are sick, but that we have challenges. (South Africa, FG8, Parent 2)
For caregivers and communities, the stigma of mental illness often posed safety concerns. Notably, participants recognized that fear and knowledge were conflated, and that the ‘stigma mindset’ perpetuated a view of those with mental health needs in a negative light, as ‘crazy’.
I am scared of them, because I still don’t understand their mental health. So, that is the hardest idea, because I cannot accept them as someone who has mental health . . . yes, I still have that stigma mindset. I still see them as crazy because of my experience. (South Africa, FG6, Parent 7)
Living in collective societies, parents were actively involved in their neighbourhoods and communities and often observed abusive or other violent incidents that involved children and reflected on how lack of safety impacted mentally on both children and adults. Such examples were largely reported from South Africa.
It is not easy raising a child that doesn’t have parents. When you want to see mental disorder, take and raise a child that doesn’t have parents. You will raise them well, but you are abusing them to others. So, I feel like you should approach them and teach them. (South Africa, FG6, Parent 3)
Within the South African community, it appeared that it was more acceptable for participants to intervene and guide parents and children directly, rather than access external assistance.
Now I try to talk to their parents and tell them to talk politely with the kids. I advise not to hit the child, rather teach them right and wrong. I will try to make it my habit to spread positivity. (Pakistan, FG1, Parent 3) I spoke to my neighbours about beating the children. They should not abuse the children, because if they hit the children too much, then they are disturbing their minds. So, beating is abuse, and it disturbs them a lot. (South Africa, FG6, Parent 3)
One parent even reported that she took up such a role with a local teacher. For those reasons of holding unique knowledge and being better placed than external services to engage communities, parents considered they had a valuable role to play alongside professionals.
I had a situation where the children complained that their teacher was always shouting at them. I then approached the teacher and explained that in such situations, she should take the time to hear from the children what was happening before she shouted at them. (South Africa, FG7, Parent 7)
Both vulnerability to victimization and perpetration of violence were related to gender, with some acknowledgement of the importance of involving males in awareness and interventions, in addition to women-only spaces. Thus, the notion of child safety was not only bound up in parental roles and identity, but in the role of the father and the gendered identity of the mother.
So, I think we, as in us men, that we as men should also be in the position to attend these sessions. We need to be aware to mitigate the issue of abuse. (South Africa, FG6, Parent 4) Elders used to say women shouldn’t show their anger and answer back. That was somewhere stuck in my mind, and then we got [a] platform to channel our anger and make our energies travel in [a] positive direction. (Pakistan, FG2, Parent 2)
Theme 2: Child rearing practices
Parents acknowledged that children and themselves often had difficulties in regulating their emotions, and this was putting them in unsafe situations. Hence, they reflected on circumstances such as living in poverty, being isolated and lacking support, that led to dysregulated responses.
The most difficult thing for me was to reduce my anger at everyone, because I was very angry at everyone, because the situation had come to me in such a way that there was no one to support me. (Pakistan, FG5, Parent 2)
Parents reflected how difficulties in controlling their anger were projected onto their children through physically or verbally harsh parenting. They identified lacking support and facing multiple stressors, thus not paying attention to children’s emotional needs.
We get angry with family for many things, and if we take our anger out on the children, it creates a bad impression. I did this many times. (Pakistan, FG5, Parent 2) I, being single mother, was always afraid what if children go to the wrong path, so I behaved strictly with them, always. (Pakistan, FG5, Parent 1)
Children’s mental health and wellbeing was also adversely affected indirectly, through inter-parental or inter-sibling conflict. Children could then re-enact such behaviours in school or the community, and parents expressed concerns that their own anger and reactions towards the child might be mirrored against others.
Younger sister wants to hit the eldest sister . . . they won’t forget that she hit her older sister. Once you let people hit each other in your home, your house will become where people hit each other. Please speak to her about not doing that. (South Africa, FG6, Parent 2)
Some parents reflected on strategies that had enabled them to regulate their anger and emotions without resorting to verbal or non-verbal responses, especially towards their children. They further acknowledged that this learning was iterative and developing, rather than an isolated implementation of understanding.
I have learned to control my anger. I have gained the confidence and learned [a] way of communication in [name of NGO] that now I am able to communicate in this manner, because I belong from the background where manners are not visible in communication, and I also taught my kids about the way of better communication. (Pakistan, FG2, Parent 3)
Some parents described how negative parenting attitudes and practices adversely affected their children’s mental health.
The issue is with their mind, which disturbs them. Even as parents, we get angry, shout, and use harmful words when talking. And when we shout, we shout, we hurt them. That is why we need to find a way to communicate with them. It would be best to have a soft spot when you speak to them but also keep their mental health in mind, because they need to see a professional. (South Africa, FG3, Parent 3) Parents should not fight in front of the children. The mind of the children gets disturbed. (Pakistan, FG3, Parent 3)
Those parents who shifted their responses to positive strategies reported several interlinked reasons such as disentangling their own from their child’s needs, listening and interacting accordingly. Gradually, they would observe changes in their child’s behaviour too.
I then think about how I can discipline them. Hitting or punishing them might not work. (South Africa, FG6, Parent 5) If they can’t say anything to you, it doesn’t mean that you should take all your anger out on them. (Pakistan, FG5, Parent 3)
Developing more empathic skills was perceived as leading to both a better understanding of children’s needs and a safe space for children to disclose concerns, which was argued to be effective in encouraging them to ‘open up’.
. . . trying to take my child in confidence, so that if anything happens, he should report that to me. (Pakistan, FG3, Parent 1) So, I’ll say come, my boy. Let’s sit down . . . and then I will say, ‘come, let’s drink some tea and tell me what the problem is because, as a family, we need to be able to solve it’. (South Africa, FG6, Parent 3)
Parents reflected that, when they instilled positive parenting strategies and broke the conflict cycle, this also protected their own, as well as their children’s, mental health.
But when they were together, they started to fight, so I told them they would make me crazy, and I was not crazy. So, before it gets to that, I tell them to sit down and speak to each other appropriately . . . so, when you sit down and speak to them as friends, they will calm down and tell you their problems. (South Africa, FG7, Parent 2)
Nevertheless, such awareness was not always translated to positive parenting.
So, instead of hitting them, I am now punishing them. So, I will ask, who did one, two, three, then one will say it’s not me . . . I will ask again; if no one responds, I will not cook. (South Africa, FG7, Parent 2) Like I said, I am a mother, so being a mother, I always try to be the one who is always available for her child, but sometimes unintentionally I hit my child when she does something wrong. Now she is growing, and she demands a lot. I felt like she is spoiled but I was wrong. (Pakistan, FG4, Parent 1)
Religious beliefs and coping strategies were perceived by some parents as moderating both internal mechanisms and external responses in relation to children’s behaviours.
Even if that’s passed, we impose it on our children that everything that happened to us happened from God, but we often use bad words with children. (Pakistan, FG5, Parent 1) You must also keep God in mind when speaking to the social worker, because you’re also doing this for the child’s benefit. (South Africa, FG7, Parent 3)
Theme 3: Systemic support
As child mental health and parenting styles are more widely related to systemic influences, participants valued the importance of awareness and education on child protection and mental health that was provided to their communities. Some parents also made the link between the two.
Here mothers are illiterate, some of them never been to school, so it’s highly needed to educate them on child abuse. They often leave their children with relatives and cases of child abuse happen, and they don’t find it wrong if a male relative is kissing on a child’s lips. The mother says nothing, because she thinks it’s not wrong. (Pakistan, FG3, Parent 4)
The need for awareness, education, and promotion of safety and mental health for different stakeholder groups, that is, children, youth, parents, teachers and the police, was emphasized.
Useful was the idea of arranging such workshops for parents and teachers about important information for child abuse. This one thing can bring big change. (Pakistan, FG3, Parent 6)
Participants also spoke of the need to educate and include police officers and other professionals in awareness campaigns; particularly as police officers worked with youth who misuse substances that impact on their behaviour.
You’ll find that once a person is affected, they will start using nyaope and stuff like that. So, I think the police should be included when doing such things as the mental health event. (South Africa, FG6, Parent 7)
There was lack of clarity on when and how to seek help from services on potential cases of child or gender-based abuse. The interplay between safety and mental health sometimes led to ambivalence on the preferred route to services.
You can call and report that the husband is beating up his wife, and they will come quickly, but only to see if she is the right fit for them. Then with [name], you can ask her about orphans. You treat them well, and then they accuse you of abuse. You raise them well, and then they will say that you treat others better. (South Africa, FG6, Parent 5)
Parents from South Africa mainly focused on youth and the risk of extensive substance use in disadvantaged areas. Hence, they considered reasons related to inequalities, lack of legislation and implementation of policies.
They use corruption to obtain these visas because of greed and money, all of which are hurting our children. They know what is in the bag when it comes, but they don’t open it, which ends up killing our kids. (South Africa, FG6, Parent 7)
Participants did not confine interventions to the community and victims. Understanding welfare issues and addressing safety for perpetrators were perceived as being interconnected.
Also, I think we should make sure that we work on those who do child abuse. Because we never know what circumstances that person has gone through, which made him do this. We should start taking safety measures and also plans to work on the abusers as well. (Pakistan, FG3, Parent 4)
Discussion
This study sought to understand how parents living in socioeconomic disadvantage in South Africa and Pakistan experience and comprehend mechanisms that compromise child safety and mental health within their communities, and to identify the types of informal and structural support that can enhance child protection and mental health, thus to contribute to the literature and inform social work practice in similar Global South contexts. The findings align with international, including Western, literature on the connection between child safety and mental health. Parents identified both shared and interconnected risk factors, including poverty, exposure to family and community violence, substance misuse, harsh parenting practices, and lack of social support (Le et al., 2018; Maclean et al., 2019).
The findings highlight certain contextual issues that apply to similar collectivist societies, and which need to be taken into consideration in informing social work practice and social care policy. A major barrier is due to structural inequalities in terms of statutory skilled professionals, supporting policies and budgets. Social services may not be autonomous, with limited legislative powers and staffing levels, instead child protection responsibilities are often designated to or shared with NGOs. This balance should be redressed by national and local governments, with increasing devolution of authority to statutory services, while working in partnership with non-statutory, community- and faith-based organizations that focus on awareness and first-level psychosocial response. In particular, religion and culture play a central role in shaping perceptions, coping strategies and treatment-seeking behaviours for mental health, while also offering social support, moral guidance and resilience-promoting resources (Sikrweqe et al., 2024). Social worker posts can thus be positioned on the interface between communities, informal and statutory structures in Global South contexts, to lead this transformative process. Social workers are ideally placed, because of their unique knowledge of support systems, expertise in holistically meeting child and parent needs, and skills in coordinating agencies on the ground.
As demonstrated by the findings, concepts of child safety and mental health vary and are negatively influenced by stigma and taboo of child and gender-based abuse within families and communities, and the widely documented negative attitudes and beliefs towards mental health and illness. Misperceptions between cultural ‘norms’ of, for example, corporal punishment, and statutory definitions, can be blurred and hinder recognition, reporting and help-seeking. The design of awareness and psychosocial interventions should thus be informed by evidence-based cultural influences on child rearing and reframe attitudes. Social workers could coordinate and increasingly integrate social care and mental health services underwritten by children’s rights (Cuartas, 2021), while maintaining ongoing dialogue with communities in negotiating and linking rights-based frameworks with existing processes and traditional mechanisms (Ellermeijer et al., 2023). Interdisciplinary training between social care, mental health, education and community-based practitioners can facilitate integrated and collaborative care.
The findings need to be interpreted in the context of sociocultural and systemic differences between the participating countries, and how these influence parenting practices and child outcomes (Bornstein, 2023). In Pakistan, parenting is largely shaped by collectivist values, strong extended-family networks and traditional gender roles, where obedience and respect for elders are emphasized, often leading to authoritarian styles and limited child autonomy. Conversely, South Africa’s post-apartheid context and diverse multicultural society have fostered a growing emphasis on children’s rights, individual expression and collective responsibility for children’s wellbeing (Ubuntu), supported by formal child protection and social protection systems, like the Child Support Grant assisting families in need. Nevertheless, the family system is negatively impacted by high levels of poverty, unemployment and community violence. While poverty and trauma affect children in both countries, Pakistan’s limited access to support services contrasts with South Africa’s more structured community-based interventions.
The findings indicate opportunities and benefits in the intersection between community awareness and education on child protection and mental health, with the initiation of positive parenting initiatives. Preventive and responsive interventions for parents are clearly important in promoting awareness, protective knowledge and skills. In Global South countries, there is emerging evidence of such innovative and socioculturally sensitive programmes, which can reduce harsh parenting and child maltreatment (Zhang et al., 2021).
Fathers were notably absent from the study. This was related to lack of engagement in both sites, and additional cultural reasons for opting for single-gender groups in Pakistan. Although this gender pattern is not uncommon in children’s services and research, fathers have been shown to hold different beliefs in relation to child safety, for example on corporal punishment, which are significantly associated with gender-based violence (Lansford et al., 2020). When fathers have, however, been included in psychosocial interventions through targeted strategies, their input predicted adaptive early childhood developmental and health outcomes (Jeong et al., 2023).
As their theoretical frameworks and techniques are broadly similar, it is important to combine child protection and mental health interventions and integrate those into existing local support systems, so that solutions are owned and co-driven by communities (Krishna et al., 2021; Yim et al., 2024). Participants shared several examples of collective parenting, which were more commonly used as a first-line response rather than approaching external structural services. Parents could hence utilize such local knowledge and acceptance as peer educators, mentors or support workers (paraprofessionals). Indeed, there is positive evidence of parents adopting awareness, support and advocacy functions for their peer group in relation to children’s welfare, physical and mental health (Atif et al., 2019). Youth peers were also found to encourage child participation in psychosocial support groups, which facilitated the reporting of legal issues such as beatings, and resulted in improved access to education, health and social care (Muriuki and Moss, 2016). Such integrated initiatives are pertinent in humanitarian post-conflict settings (Metzler et al., 2023). It is also important to involve perpetrators in responsive and preventive programmes, as such policy and interventions are not well developed in many countries.
Parents in this study widely reflected on social factors affecting their emotional self-regulation, which in turn impacted on their parenting capacity and children’s mental health. Parenting interventions should thus incorporate self-regulatory activities, rather than only focus on behavioural techniques. Haslam et al. (2019) noted the limited evidence of this therapeutic component in Global South parenting programmes, which might be explained by self-regulation being perceived as associated more in individualistic rather than collectivist cultures. Rather than adopting an either-or position, the authors propose an interesting concept of promoting self-regulation in conjunction with collective efficacy and regulation. This is supported by our participating parents’ perspectives, and is consistent with the collectivist values of solidarity, vigilance and morality (Ubuntu-based social work model of ‘I am a person through other people’ – Mulumba and Carvalho, 2024).
The findings need to be considered in the context of the limitations of the research design. The two settings are not necessarily representative of the respective countries, or indeed other Global South sociocultural contexts. As the sample included parents who already had some exposure to mental health promotion, their views may have been positively biased. For example, parents without such prior exposure may have held more negative attitudes towards mental health and/or not associated it with safety issues. Capturing the perspectives of children, youth, practitioners and policy makers would provide a holistic perspective on how to integrate child protection and mental health in future awareness, interventions and service provision. Data on barriers to help-seeking merit more in-depth analysis. A mixed-methods design could complement the qualitative component with activity data on child protection and mental health referrals and interventions in the participating areas. Recruitment challenges were anticipated and partly addressed by working through host NGOs and holding community consultation meetings, while methodological decisions were driven by pragmatic issues such as resources. Nevertheless, the strength of the study was that it addressed parent perspectives on child protection and mental health in conjunction and across two Global South resource-constrained settings.
Conclusion
The reported perspectives of parents living in resource-constrained settings provide an important platform to inform social work across the Global South. To this effect, social workers could play a leading role in improving structural services, legislation and child protection, while bridging gaps with psychosocial support, and engaging informal community systems through awareness and peer involvement. Strategies should be linked to child-sensitive social protection, that is, policies and programmes aimed at preventing or protecting against poverty, vulnerability and social exclusion (Cirillo et al., 2024). Social workers could also drive the co-production, design and delivery of interdisciplinary and culturally sensitive training, supervision, mentoring and advocacy in community-based organizations such as early childhood development centres (Ronaasen and Engelbrecht, 2023; van Wijk et al., 2021). End-users, that is, children, youth, parents and other caregivers, should be actively involved in the contextualization, uptake and implementation of interventions.
Footnotes
Acknowledgements
We thank all participating parents and the two host community-based organizations for facilitating this study.
Ethical considerations
Ethical approval was granted by the University of Leicester Sociology Research Committee, reference numbers 29296 (approval date 16.2.2021, recruitment period 1.6.2021-31.5.2022) for the South Africa and reference number 34318 (approval date 27.4.2022, recruitment period 1.9.2022-28.2.2023) for the Pakistan projects, respectively. All ethical considerations are explored in detail in the main article.
Funding
The two integrated datasets are based on research projects funded by Economic and Social Research Partnership Grants.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Patient consent statement
Informed consent was obtained from study participants as is detailed in the main article.
AI statement
No AI tools were used at any stage of the project, including analysis and dissemination.
Author biographies
![]() ), which provides capacity-building in such contexts.
), which provides capacity-building in such contexts.