
Abstract
Parents with intellectual and developmental disabilities (IDDs) are at an increased risk of having their children placed in foster care. A group intervention to provide support was developed in Australia and applied in Sweden to help mothers with children in foster care deal with the grief of having a child removed and their new parenting role. An evaluation found that the intervention could contribute to maturing and developing the insights and skills of the mothers. This study aimed to explore the long-term process and outcomes of the intervention in terms of the mothering role, visits with their children and the need for support. An explorative and qualitative single-case design was used. Three mothers with IDDs were interviewed before participating in the intervention, directly after the intervention and between nine and 14 months later. Interviews were analysed with qualitative content analysis. The intervention helped the mothers to come to a broader and shared experience with new insights and acceptance of help, improved contact with social services and better strategies in their relationships with their children. The feelings of grief and loss lasted over time. The study concluded that despite the history of mothers with IDDs whose children are in care (e.g., life crises, the trauma of placement), an intervention adapted to meet their needs can contribute to long-lasting experiences of wellbeing and reconciliation, which also benefit their children.
Plain Language Summary
This study looked at how a special support programme helped mothers with disabilities whose children were taken into foster care. The programme aimed to help these mothers cope emotionally and adjust to their new parenting role. Researchers talked to three mothers with disabilities before, immediately after and about one year after they joined the programme. They wanted to see how helpful the programme was in the long run, focusing on how the mothers felt about being parents with children in foster care, how they experienced collaboration with social services and foster homes around visits and their need for support.
The study found that the programme was helpful. It made the mothers feel less alone and more willing to get help and work with social services. They also learned better ways to parent during visits. But even after the programme, the mothers still felt sad about not having their children with them.
This research suggests that programmes tailored like this can help mothers with disabilities feel better and be better parents. This means it’s important for social services to offer such support programmes. They can make a big difference in the lives of mothers with disabilities, helping them to feel happier and more confident as parents.
Keywords
Introduction
Parents with intellectual and developmental disabilities (IDDs) constitute a heterogeneous group and are overexposed to factors that convey the risk of inadequate caregiving (Pacheco et al., 2022). Yet, support for parents with IDDs is limited and rarely adapted to the individual needs of the parents (Azar et al., 2012; Janeslätt et al., 2019). Thus, their children are more likely to be taken into foster care (LaLiberte et al., 2017; McConnell et al., 2021; Tøssebro et al., 2017). Having children in care entails grief for mothers and a need for adaptive support (Janeslätt et al., 2019; Mayes and Llewellyn, 2012). This study focuses on the process and long-term outcomes of a group intervention that was offered in Sweden.
Parents With Idds And Parenting Skills
IDDs is an umbrella term for diagnoses of cognitive difficulties, including intellectual disability (ID), borderline intellectual functioning, attention-deficit/hyperactivity disorder (ADD/ADHD) and autism. Parents with IDDs frequently need support (Feldman, 1994; Johnston et al., 2012; Starke, 2005) and rate their parental competence significantly lower than parents without these disabilities (Roshanai et al., 2019). Research confirms that parents with ADHD symptoms or autism can benefit from support in their parenting role (Chronis-Tuscano et al., 2008; Dugdale et al., 2021; Johnston et al., 2012; van Steijn et al., 2013). For instance, many parents with ADHD report high parental stress and low confidence in their abilities (Banks et al., 2008; Chronis-Tuscano et al., 2008; Lowry et al., 2018; Theule et al., 2011). People with ADHD or autism often have comorbidities (e.g., dyslexia, borderline ID and learning disabilities). It has been increasingly established that the caregiving of parents with IDDs depends on complex interactions between factors beyond their cognitive difficulties. Capturing this complexity, Feldman and Aunos (2020) developed a contextual–interactional model emphasising the impact of life crises, parental traumatic experiences, psychological ill health, insufficient social and professional support, and child heredity. Such factors explain a large proportion of the variance in these parents’ caregiving abilities and in their children’s development (Meppelder et al., 2015; Schuengel et al., 2017; Wade et al., 2015). The model also underlines that parents with IDDs are subject to discriminatory practices from social services. Stereotypical assumptions and low expectations of parents with IDDs can influence social workers’ decisions regarding child risk and their general willingness to help. A parent’s diagnosis can significantly affect a professional’s perception of their fitness to parent and their ability to change and can then potentially be used to justify the permanent removal of their child(ren) (Aunos and Pacheco, 2021; Lightfoot and DeZelar, 2016; Proctor and Azar, 2013; Tefre, 2017). Stigmatisation and discrimination can lead to parents masking their cognitive difficulties and being apprehensive to ask for and/or rejecting support when it is offered. Because caregiving-based support can be crucial for ‘good-enough’ caregiving, this may further reduce the likelihood of successful caregiving for these parents (Feldman and Aunos, 2020). Mothers with IDDs report low levels of social support and are often isolated in society (Llewellyn and McConnell, 2002). Social disconnection is associated with high-stress levels, poorer mental health, and adverse parenting and child outcomes (McConnell et al., 2009). This research concludes that many parents with IDDs may need a broad spectrum of support addressing not only parenting skills.
The Difficult Process Of Parents Dealing With Children In Placement
Out-of-home care is sometimes essential for child protection. Still, child–caregiver separation constitutes intrusive, life-changing events for parents and children (Forslund et al., 2022). In these cases, striving for continuous contact between the children and their birth parents is important. Haight and colleagues (2003) and Schofield and colleagues (2011) also emphasise that the engagement of parents through contact is likely to impact children’s stability and security in the foster family.
In general, mothers whose children have been removed find themselves renegotiating their identity, trying to reconcile being a mother in an ‘in-between’ state and dealing with a loss (Memarnia et al., 2015). At the same time, the mothers remain in contact with their children during brief and often strained visits (Memarnia et al., 2015). There is also a stigma attached to being labelled ‘unfit’ as a parent, and the grief associated with having ‘lost’ a child who has been removed is less accepted by society than the grief of parents deprived by the death of a child (Charlton et al., 1998). Therefore, such losses have been described as ambiguous (Boss, 2009) and lacking legitimacy (Memarnia et al., 2015).
It is no less challenging for parents with IDDs to deal with their child being in foster care than it is for any other parent. Mayes and Llewellyn (2012) found that mothers with IDDs whose children had been removed described feelings of sadness, emptiness and powerlessness, leading to a complicated and extended grieving process.
Additionally, mothers with children in care experience a threat to their identity and feel forced to alter their maternal role (Janeslätt et al., 2019; Schofield et al., 2011). Dealing with child removal may be more difficult for mothers with IDDs as they often have diminished internal coping resources for understanding and managing grief (Mayes et al., 2011). Parents with IDDs also tend to have low social support and thus limited external coping resources (Feldman et al., 1992). Because grieving after the fostering of a child is a long-term process, an attendance to the psychological and physical health of the mothers is needed (Mayes and Llewellyn, 2012). Depression and anxiety are frequent in parents with IDDs (Jones, 2013). It has also been proposed that individuals with IDDs should be seen as more susceptible to traumatic grief based on an increased risk of secondary loss, communication barriers and difficulty finding meaning in the loss (Brickell and Munir, 2008). Thus, parents with IDDs often need adapted professional support to cope effectively with their grief (Brickell and Munir, 2008).
Support For Parents With Idds And Children In Placement
There is an urgent need to attend to the psychological health of mothers with IDDs whose children are taken into care. According to the United Nations Convention, article 23 (United Nations, 2008), parents with disabilities must get adapted support to manage their crisis and adjust to their new parenting role. Yet, mothers with IDDs either do not receive the support they need or receive it only on a small and arbitrary scale (Azar et al., 2012; Janeslätt et al., 2019).
Group interventions, which flexibly apply adult learning principles, can positively affect wellbeing and self-worth and improve parenting skills in mothers with IDDs (Booth and Booth, 2003; May and Harris, 2020; McConnell et al., 2009). Group interventions with parents whose children are in care can also build relationships and empower participants (Thomson and Thorpe, 2004). In addition, group interventions can enhance social skills and trust in relationships with social workers (Gustavsson and Starke, 2017; McConnell et al., 2009). Booth and Booth (2003) concluded that key components of successful group activities include focusing on real-life situations, developing self-advocacy skills and being flexible enough to cope with other issues affecting the mothers’ time and attention.
Preliminary evidence also indicates that group interventions for parents whose children have been removed can improve parent–child relationships and interactions at visits (Bullen et al., 2017). Furthermore, the benefits of social support provided in group interventions to parents with IDDs have been found to influence parents’ wellbeing (Adolfsson et al., 2021).
In Sweden, most children in care will have a regulated relationship with their biological parents. A regulated form of control usually implies only being in contact at pre-specified intervals (e.g., every third week) and for a limited time (e.g., a few hours). Naturally, the parents long for their children, worrying about their wellbeing and the child–caregiver relationship. This situation will increase the need for support to help the parents find strategies to handle their grief and cooperate with social workers for the sake of their children. Parents with IDDs need adapted support, which involves an extra challenge for professionals who often lack the knowledge to adapt support to cognitive deficits (Janeslätt et al., 2019). People with IDDs need individually adapted support to understand the decisions made and facilitate cooperation with child protection services and the foster home (Janeslätt et al., 2019).
Group Intervention For Parents With Idds And Children In Placement
In Australia, a group intervention called Parents on the Outside was developed due to the identified lack of support and concern for meaningful engagement of parents with their children after they have gone into care. More specifically, it was created to support mothers with IDDs to deal with grief and their new parenting role (Mayes et al., 2011). The intervention model was translated into Swedish, culturally adapted and named After all, I Am a Mother (hereafter ‘MTA’). A manual was developed (Adolfsson et al., 2021), and Adolfsson and colleagues (2021) evaluated the intervention for mothers with IDDs (n = 11) and children in care. The authors found that the support group could contribute to maturing and developing mothers in a reconciliation process when their children are in care. However, the long-term effects of participating in the intervention have not yet been investigated. As such, this study aimed to explore the longer-term process and outcomes of the intervention in terms of the mothering role, visits with their birth children and support in the parenting role.
Method
An explorative and qualitative single-case design was used (Kazdin, 2003; Todman and Dugard, 2001). The study design was approved by the Regional Ethical Review Board in Uppsala (ref. no. 2014/369). By investigating similar and contrasting cases, it is possible to understand the findings further, grounding them by specifying similarities in the process of the mothers at different time points (Merriam and Tisdell, 2015). When analysing similarities and differences between cases across time, the approach also enables insight into processes associated with stability and change.
Participants
Three mothers with IDDs were interviewed before participating in the group intervention, directly after the intervention and between nine and 14 months later. The mothers had one or more children in care. Information on the participants is provided in Table 1. Pseudonyms (Anna, Britta and Catherine) are used to preserve their anonymity. Details have also been changed, and their children’s genders/sexes are not revealed. The contexts described are the mothers’ situations before participating in the MTA support group activities.
Participant details.
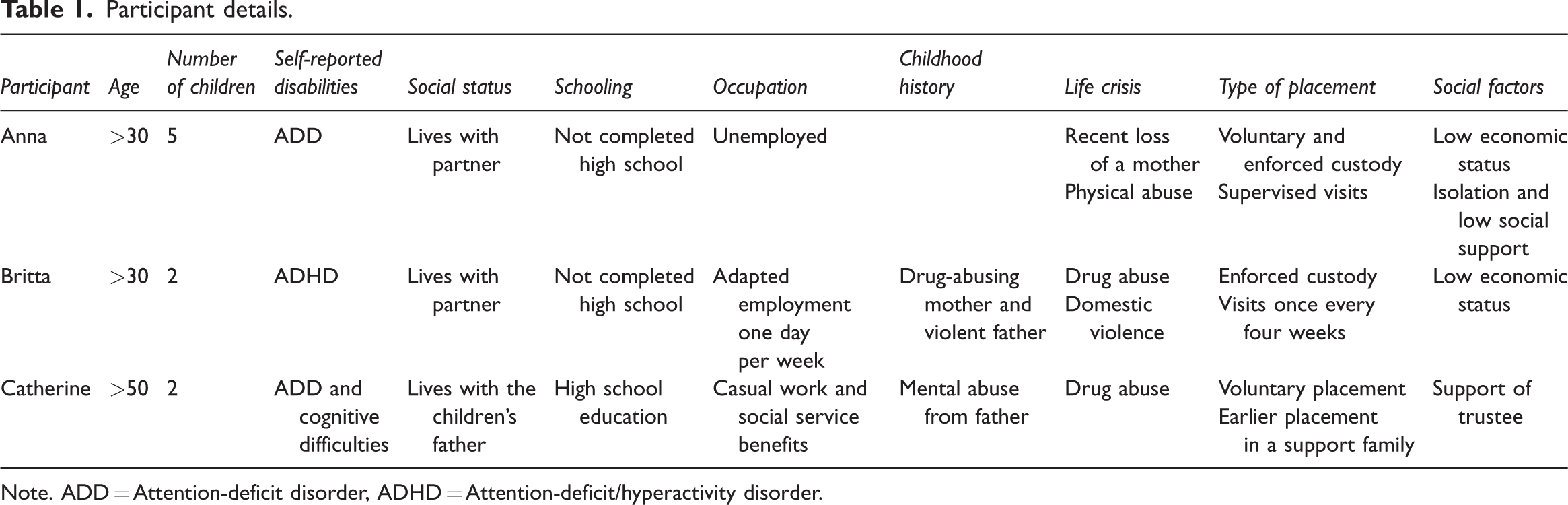
Note. ADD = Attention-deficit disorder, ADHD = Attention-deficit/hyperactivity disorder.
Data Collection
The recruitment was done in one support group of four participants receiving the intervention in the spring of 2015. Three of the four participants gave informed consent to participate in the research and took part in a series of three interviews each over time. The interviews were recorded and transcribed verbatim. 1
An interview guide used in earlier studies contained demographic and semi-structured questions about the experience of the parenting role, parental visits and support needs (Adolfsson et al., 2021; Janeslätt et al., 2019). The same interview guide was used on all three occasions. However, five questions about the mothers’ experiences of participating in the intervention were added to the interviews at the second two time points (i.e., directly after the intervention and at the nine- to 14-month follow-up). Interviews were conducted by three of the four authors, all of whom had extensive experience interviewing people with IDDs (KJ, GJ, PA).
Respondents received reminders before each interview. The interviews were conducted in an undisturbed environment. Adaptations were applied to compensate for the IDDs, and after each interview a gift card was offered (Janeslätt et al., 2019).
Demographic information was obtained at the beginning of each interview (age, social status, number of children at home or in care, level of education and type of disability). Semi-structured questions about the participants’ experiences of their role as a parent, visits with their children and the support they felt they needed to parent were asked at each time interval.
Group Intervention
The translation and cultural adaption of the MTA were described in an earlier study and mothers with IDDs were involved in the process (Adolfsson et al., 2021). The intervention followed the original programme, which includes eight one-and-a-half-hour to two-hour sessions, provided once a week, with set themes for each session. The group intervention was tailored to parents with IDDs. Because it is known that the tailoring of an intervention is important for a parent’s ability to benefit from group interventions, the Swedish version was adapted further. Throughout the intervention, there was an openness about cognitive functions to raise awareness of the consequences of cognitive limitations, to verbalise different functions and discuss coping strategies. Mothers with IDDs were involved in several stages of the development and research of the intervention, including viewing and providing feedback on the interview guide. They also contributed to sharing their experiences to new group leaders about the importance of the intervention and helped to recruit new participants by making a video to demonstrate their experiences of the intervention, including their initial fears of participation which they had subsequently overcome.
Data Analyses
Qualitative content analysis inspired by Patton (2014) and Graneheim and Lundman (2004) was used. First, all authors read the nine transcripts (three participants at three time points). Meaning units covering matching content were collected and distributed in a joint document to respond to the study’s aims. Following this, the content was sorted in correspondence with three major areas: (1) The mothering role; (2) Parental visits; and (3) Support needed in the parental role. This was a preliminary qualitative content analysis performed by the first author (SM). The meaning units were colour-coded in three colours relating to the three major areas. The collected meaning units were double-checked to certify that all relevant data were included in the first analysis. While the important content of the meaning units was preserved, they were shortened and condensed into codes while retaining the essential meaning of the text. Authors SM and KJ then discussed and reviewed the meaning units and corresponding codes until a consensus on interpretation was reached.
The nine interviews were then labelled with two types of code for the three participants (A, B, C) and three time points (1–3) (Table 2). The unit of analysis was then divided into three domains according to the time points (Graneheim and Lundman, 2004), structured according to the study’s aims (mothering role, parent visits and support needed in being a parent). All texts in each domain were divided into meaning units. These were condensed and coded by SM and KJ as described by Graneheim and Lundman (2004).
Interview codes for participants.
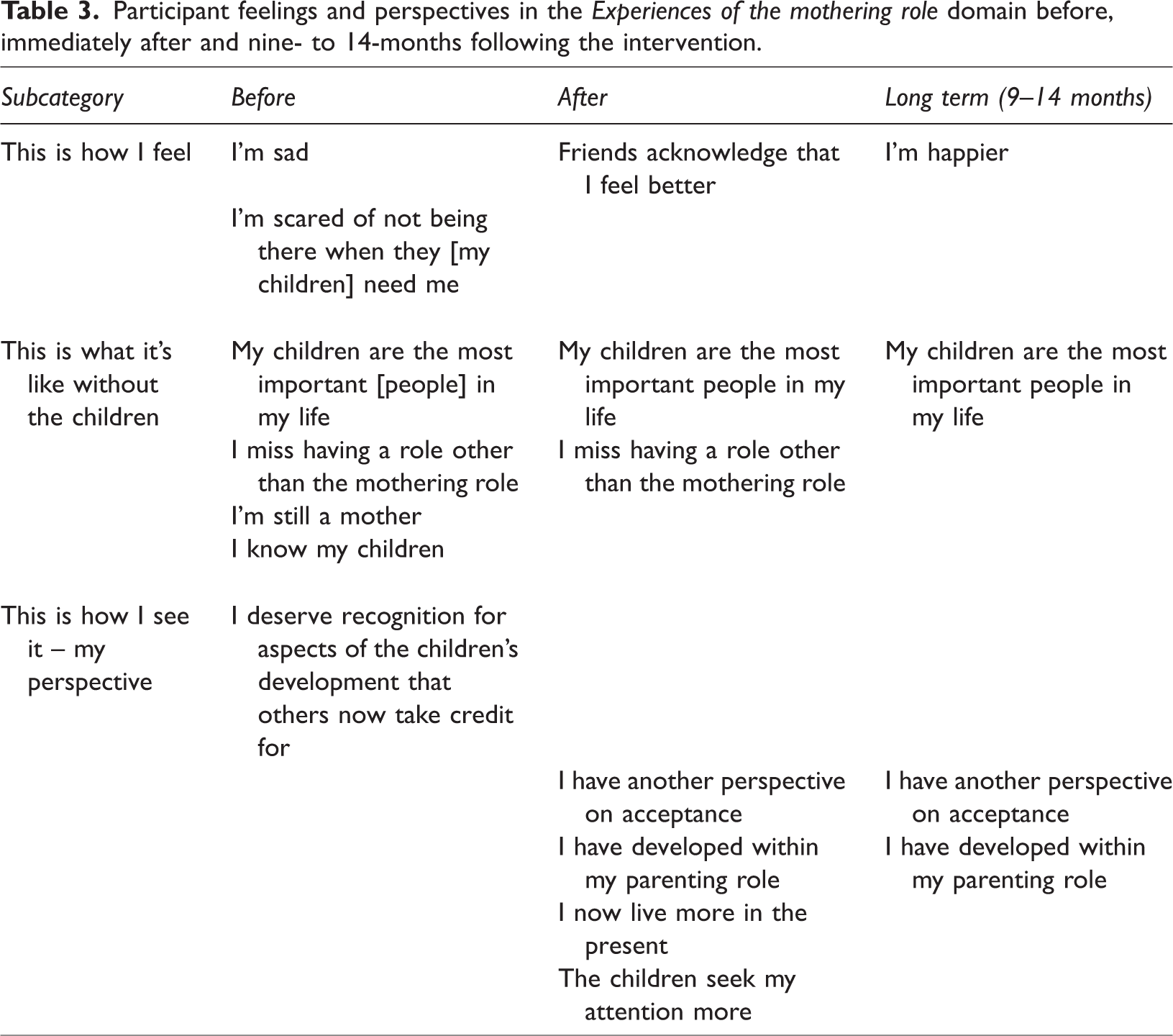
Next, the data were regrouped (using previous codes) for each participant in order to understand their process over time. The codes were then sorted into subcategories and categories within the three major areas. All authors then combined categories with similar content to obtain fewer categories. The new categories were given broader labels, which contained the earlier categories but were sorted in a more general manner. Broader labels allowed us to recognise similarities and differences more easily (Table 3). Hereafter, comparisons were made between all three study participants.
Participant feelings and perspectives in the Experiences of the mothering role domain before, immediately after and nine- to 14-months following the intervention.
Findings
The findings show common experiences for the three mothers. These similarities pertain to experiences that persisted across the three time points and those that changed over time. Because the changes seen after the intervention are typically present (also in the long-term follow-up interview), they are presented as one category.
The Process Over Time
The process over time is presented in Figure 1. Here, the three domains are presented alongside categories before and after the group intervention, the latter including data collected directly after the intervention and after nine to 14 months.
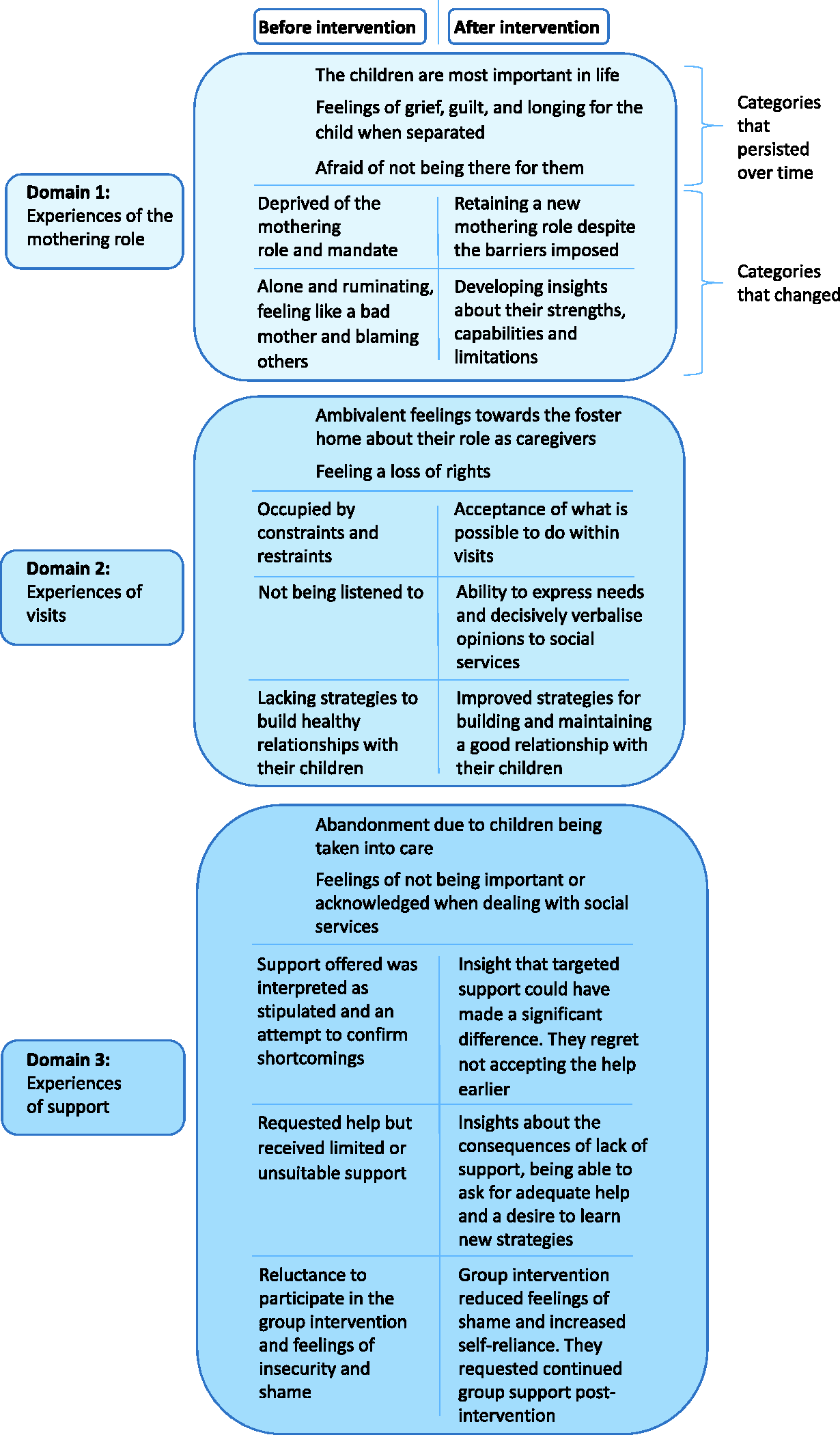
The process and outcomes before and after the intervention.
Experiences Of The Mothering Role
Categories That Persisted Over Time
Within the Experiences of the mothering role domain, some experiences and feelings were present at all three time points. The three mothers stressed that their children are most important in life, and this description persisted for the entire study period. Their identities and roles as mothers were characterised by separation from their children. They described the difficulty of no longer having daily contact with their children. Therefore, separation implies the loss not only of their children but also of their role as a mother.
Separation was expressed in the interviews as feelings of grief, guilt and longing for the child when separated. Afraid of not being there for them. These feelings also persisted over time. The mothers’ narratives contained feelings of guilt and shame about their shortcomings and recounted experiences of how their children were negatively influenced during their upbringing. The narratives also described things that children should not have to experience. Finally, mothers feared losing touch with their children with the passage of time.
Categories Changing Over Time
Two categories changed over time within the Experiences of the mothering role domain. The first category to change was their sense of being deprived of the mothering role and mandate. Before the intervention, the mothers felt deprived of their role or mandate as a parent and no longer knew who they were in relation to their children. After the intervention, the category indicates a continuing process of refining their image of a parent’s role, retaining a new mothering role despite the barriers imposed. Others were raising their children, but this situation appears to be more accepted and meaningful to them: … all I can feel about the one who is on a voluntary placement is that we have a better relationship, and I can put my foot down. [My child] has tried to push me around a bit, but I can see that I put my foot down and I’m a stronger person now. And I work with the foster home more and have had their support and encouragement, so I’ve grown as a person as regards [my child]. (A2, Anna)
The mothers also expressed insights into their value as a mother even if their children did not live at home. For example, Catherine felt that the intervention helped her to reflect on her situation and accept that the children were not coming home: Anyway, MTA has helped me to think and accept that the kids sort of aren’t coming home. That they are simply too old for that. I mean, [my older child] only has one more year and [my younger], well … first of all we have to have a decent relationship before even thinking about [this child] coming home. (C3, Catherine)
The mothers’ feelings of deprivation and dejection were not as strong after the intervention. The mothers believed their wellbeing improved and noted that significant others perceived them as better: [My child] must have felt that I’ve been struggling and wondered how I’ll be and no, all of that stuff that [my child] shouldn’t need to do … so I think [my child] is relieved now that things are all a lot better. (A2, Anna) Yes, my husband [thinks my wellbeing has improved]. He says you’re much happier and more positive and look at things differently. And he thinks it’s great that I’ve been able to be a support for some of the other participants. And that’s nice to hear. (B2, Britta)
Through intervention, the perception of being alone and ruminating, feeling like a bad mother and blaming others also changed toward developing insights about strengths, capabilities and limitations. Before the intervention, the mothers felt they were not good enough as parents. Such feelings also caused an emotional strain, leading to a strategy of creating distance from their children to protect themselves against feelings of anguish. Still, much of what had happened was perceived as the fault of others. The experience involves being without control and having no one to turn to when they have to solve problems.
After the intervention and at the nine- to 14-month follow-up, the mothers’ responses indicated that they had gained insights about strengths, capabilities and limitations. The narratives became more nuanced, including shortcomings and insights into accomplishing good things. For instance, the mothers could express pride in themselves, they could recognise that they asked for help when the situation became unbearable for their child and they noticed that their experiences as parents were called on by the foster carers. The mothers reflected on their strengths and potential positive outcomes for their children: The feeling is sort of … just that you know … what kind of Mum am I to opt out of my kids, like … at the same time, well, you understood that you couldn’t manage them. And then it’s better to ask for help even if it kind of hurts. (C3, Catherine)
The insights gained by the mothers appeared to be partly indirect through the peer support afforded by the group-based approach. For example, the support helped the mothers to understand acceptance and atonement and to know that they were not alone. According to the participants, listening to other mothers and helping one another was enlightening for their relationship with one other and created a sense of belonging: At MTA you could find out that just because you have a diagnosis that doesn’t make you any worse as a mother. You just need a lot of extra help. So, this Mama thing [MTA] is spot on. (B3, Britta)
Sharing experiences of asking for help or having support from the foster home with the others in the group bolstered the mothers’ capabilities. With group support, the mothers expressed a strengthened awareness of their abilities: To start with I didn’t ask for help. But I have actually done that later. Actually started asking for help. Because that’s been the hard part, not asking for help. You want to manage it all by yourself. (A2, Anna)
Experiences Of Visits
Categories Persisting Over Time
Within the Experiences of visits domain, one category enduring over time is ambivalent feelings towards the foster home about their role as caregivers. On the one hand, the foster carers were regarded as taking over the mothers’ parental roles. On the other hand, the mothers accepted this assistance and were grateful for its importance to their children. Although the ambivalent feelings towards the foster carers continued, the sense of gratitude was more pronounced after the intervention, having listened to mothers in the group who had an even more difficult situation with their children’s foster home but also due to exploring and expressing feelings and insights about the consequences of a lack of support.
Another category that persisted over time was feeling a loss of rights. This category includes termination of parental rights by the foster home and social services. The mothers experienced little or no opportunity to influence their children’s upbringing and did not feel their competence and knowledge about their children were taken seriously. They felt undermined in their parental roles and without rights in a system they found incomprehensible: I’m the mum after all – I’m the guardian, so this is really important. If anything happens, I have to know about it. And that’s where there’s a problem if it turns out that someone has to go to hospital, am I allowed to go or not? That’s the big issue for me, it’s about my child after all. (A1, Anna)
They did not feel that the social workers were receptive when they tried to contribute and thought they had to struggle to gain attention at the foster home: And now I had, I had to put on pressure here now, I have worked like a dog for them to assess my [child], you know. Because [my child] is like me, but … [suffers] 10 times worse. (B1, Britta)
Categories Changing Over Time
One category that changed over time within the Experiences of visits domain was the mothers’ sense of being occupied by constraints and restraints. Before the intervention, mothers were occupied by the visits, which they considered to be under the control of a system that imposed limitations. For example, they felt their children’s suggestions concerning activities were blocked by practicalities such as pre-defined schedules.
After the intervention, the category changed into acceptance of what it is possible to do within visits. This acceptance was partly grounded in realising their importance to their children: that they are most important during visits, not the activities. Thus, the mothers’ focus shifted to what they could do within the social framework. This shift was in part characterised by making plans together with their children: Me and the kids plan what we do together. I can’t influence when or how long. [We get] Four hours every fourth week. (B2, Britta)
The second category to change was not being listened to. Although the relationship with the foster families could vary with placement conditions, there was a general feeling of not being heard. Two mothers reported having little influence on planning the visits. They could only bring requests but not influence decisions. For instance, they tried to increase the frequency of the visits but had to contend with a few hours every third or fourth week. One mother felt that her children became shy because of the long gaps between the meetings. After the intervention, the mothers explained their ability to express needs and decisively verbalise opinions to social services. The mothers referred to the support group as having helped them confront the foster homes and social service staff.
The third category in the domain of Experiences of visits concerns experiences of lacking strategies to build healthy relationships with their children. One striking example presented in the interview before the intervention is a situation of rejection from the child during visits. The reaction from the child was reasonable but resulted in the mother feeling hopeless, without strategies to manage the situation. Help was given in MTA to build on the mother–child relationship step-by-step and in a respectful way. The change included improved strategies for building and maintaining a good relationship with their children, meaning learning strategies to become more responsive to their children’s needs and discovering alternative ways to build relationships with them, such as contact via social media (e.g., Facebook, Instagram) and letters: MTA has affected our contacts; it has made me able to handle visits differently … What I think has made [my child] so positive is that I find it easier to put things into words. I find it sort of easier than before to show when I’m sad or happy or things like that. (C3, Catherine)
Experiences Of Support
Categories Persisting Over Time
Within the Experiences of support domain, one perception found to last over time was abandonment due to children being taken into care. The mothers felt alone without support from relevant authorities in society. All three mothers had a shared feeling of being left on their own when their children were taken into care. This dramatic event affected their daily life long after the separation took place. They described an unmet need for personal support to oversee their crisis. They had to rely on informal help from friends, the church or other support groups. Support from the foster home and family care centre was more apparent for Catherine, since she and the children’s father consented to the placement.
Also persistent over time were feelings of not being important or acknowledged when dealing with social services. The mothers felt disregarded as parents and that their needs were neglected, especially after the children were placed into care.
Categories Changing Over Time
The first category that changed with time in the Experiences of support domain was that the support offered was interpreted as stipulated and an attempt to confirm shortcomings. Before the intervention, support from social services was sometimes construed as demanding and stipulating limitations. The mothers viewed it not as an opportunity but as an attempt by social services to gather more information about their shortcomings. For example, contact with a psychologist was interpreted as an attempt to probe into an individual’s past.
After participating in the support group, a common factor for the mothers was the development of insights that targeted support could have made a significant difference. They regret not accepting the help earlier. There are indications that they misunderstood the intentions of the support provider. They also noted their inability to be understood in what they were trying to convey.
The second category to change over time was the view that they had requested help but received limited or unsuitable support. In the first interviews, the mothers expressed a lack of support in parenting and wanted better support for themselves. They reported an absence of guidance in parenting and dealing with their feelings. After the intervention, there were indications of insights about the consequences of lack of support, being able to ask for adequate help and a desire to learn new strategies. The mothers learned how earlier guidance could have helped them to feel better earlier on and that their wellbeing impacts their children’s wellbeing: Because I think that if they had listened to us and given us support earlier on, we wouldn’t have been stuck in this situation now. So it wouldn’t have gone as far with [my child] and we wouldn’t have hurt each other as much. (C2, Catherine)
Later in the intervention, the mothers could verbalise their needs and increased their ability to ask for help (e.g., using strategies such as anger management and working on relationships). Another example is that they could connect the need for structure and routines with ADHD/ADD diagnoses and the ensuing importance of accepting support in this area.
Another category in the Experiences of support domain that changed over time is participation in the group intervention. In the first interviews before the group intervention the mothers expressed reluctance to participate in the group intervention and feelings of insecurity and shame. The mothers felt that attending group meetings could be challenging, as it was experienced as taboo and intensely distressing. The group meeting also brought up feelings of inadequacy, powerlessness or embarrassment. After the intervention, the mothers said that the group intervention reduced feelings of shame and increased self-reliance. They requested continued group support post-intervention. They portrayed the support, in the form of group meetings, as resulting in new and valuable friendships. Sharing thoughts and experiences with others in similar situations contributed to the offloading of guilt and shame. As the mothers got to know each other and shared their experiences, they could gradually express strong emotions (such as joy, enthusiasm and anger). They described the pleasant feeling of listening, sharing and understanding one another. Participating in the support group also contributed to increased self-reliance. One of the mothers mentioned that whilst she had the support of her husband, in the group she did not need to worry about hurting his feelings when she expressed herself: Yeah, my hubby has said that I can kind of think more clearly somehow. That, you know, my supervisor at work has said the same. That it’s kind of easier. Somehow, I see ‘Why’ more clearly, or can accept in a different [way], that afterwards we could talk about it and such. Like, you know, the thing that sort of, before you could really feel like a failure as a mum, like you couldn’t manage your kids, but when you could hear from the others like then it turned into that I’m not alone. (C3, Catherine)
The situation the mothers were in with their children was hugely complex. They had a unanimous wish for continued support provided by the support group activities. They found the sessions too few and too short. The support group can be understood to have been empowering for them, therefore: Because I’ve found friends in this group. And made contacts through this group. And I’ve been able to share lots of my experience with the others and be a support for them. (B2, Britta)
Discussion
These findings show that the intervention helped the mothers to attain a broader perspective and a sense of shared experience. The mothers felt enabled to recognise their emotions, found mutual support and reached new insights through discussion with their peers. This finding aligns with the Feldman and Aunos (2020) interaction contextual model and the importance of enhancing parental mental health and social support while counteracting a sense of isolation for parents with IDDs. This study shows that change achieved in a group intervention can still be present for up to nine to 14 months, indicating positive long-term outcomes from participation.
Main Findings Of The Mothering Role
The findings of this study support and contribute to the existing evidence in the literature. The importance of the children to the mothers above all else in their lives was long lasting. The experience of grief was also present in all interviews but of variable intensity. A similar phenomenon, that is, a gradual process of acclimatisation, was shown by Baum and Negbi (2013), who interviewed fathers of children in care. In the current study, mothers stressed that their identity and role as a mother were tainted by being separated from their children; a comparable observation was reported by Memarnia and colleagues (2015). Furthermore, feelings of grief, guilt and longing for their children when separated were also reported by Charlton and colleagues (1998). Related sentiments were shown in studies with mothers with IDDs and children in care (Janeslätt et al., 2019; Mayes and Llewellyn, 2012). Our study reveals that the group intervention, including peer support, can help the mothers better manage their grief and separation from their children. In Adolfsson and colleagues’ (2021) study, mothers reported feeling relieved and comforted during the MTA intervention. The current study adds that longing for the child and grief still remain nine to 14 months afterwards. It cannot be expected, nor is it an aim, that an eight-week intervention can eliminate the grief entirely; rather, the aim is to manage it on a long-term basis.
Being deprived of a mothering role and mandate was one of the main experiences observed in the mothers before the intervention that was subject to change through time. Previous studies have reported a need for mothers with IDDs to alter their maternal role (Janeslätt et al., 2019; Schofield et al., 2011). The loss of legitimacy of parenting due to placement and the necessity for social workers to acknowledge and address these issues are described by Schofield and colleagues (2011). The mothers’ feelings of being deprived of their mothering role could have been influenced by beliefs or fears of being treated with prejudice, also affecting their collaboration with and trust of social services (Aunos and Pacheco, 2021; Mayes and Llewellyn, 2009). It is especially destructive for mothers with IDDs to feel deprived of the mothering role because of the strong normative view that the role is natural, expected of you and desirable (Franklin et al., 2022; Janeslätt et al., 2019; Theodore et al., 2018). Höglund and colleagues (2012) highlighted that the limited choice of other positive social roles may be a reason for young women with IDs to be particularly attracted to the role of parenthood. Adolfsson and colleagues (2023) found that fathers with IDDs whose children were in foster care experienced vulnerability and frustration too, but they also emphasised the value of their work outside of the home. Their parenting role was characterised by being accepting of the living arrangements of their child while feeling frustrated. This contradiction seemed to be related to the substantial support offered in the child’s upbringing due to the placement and the fathers taking a pragmatic strategy of focusing on what works best in daily life, alongside a sense of their own shortcomings due to their cognitive limitations and being excluded from child-rearing and parenting, with little or no support. This feeling of exclusion is essential since disappointment with the authorities undermines trust and confidence – a finding also in line with the experiences of the mothers in our study.
In McGaw and colleagues’ (2002) study, the sample included parents with borderline or mild IDs with children living at home. The results demonstrated that self-concept improved significantly for the parents participating in a group intervention. They made new friends in addition to other positive social and practical changes within their families. The present results are similar, signalling an improved self-concept. Our study adds to the literature that the mothers experienced a new view of their role, despite the barriers imposed, which helped them to accept their situation better. Through participation in the MTA, they also gained insights into their strengths, capabilities and limitations, a finding also reported by Adolfsson and colleagues (2021) when they applied the same intervention.
Main Findings Concerning Visits
Two categories in the domain of Experiences of visits were constant throughout the interviews. Ambivalent feelings about their caregiver role in relation to the foster home were present over time. Also, the loss of rights was observed in all the interviews, with feelings of being undermined in the parental role in a system seen as incomprehensive. Comparable findings were observed by Adolfsson and colleagues (2021). This study adds that the feeling of a loss of rights remains over a one-year period.
However, there were multiple changes. Even within the limited frame of the study, there was a shift in the mothers from focusing on the limitations of visits with their children to concentrating on the possibilities as a result of the intervention. This was also found in Adolfsson and colleagues’ (2021) study. Notably, therefore, an appreciation of what it is still possible to achieve in visits endures even a year after intervention.
The second category to change was the experience of not being listened to. In the post-intervention interviews the mothers described an ability to express needs and decisively verbalise opinions about social services. They felt that they could voice their opinions more confidently. This attitude could be related to what was found by Adolfsson and colleagues (2021) and described as an outcome of transparency, as participants articulated the consequences of various IDDs. The possibility that group intervention can affect social skills and trust in relationships with social workers has been described elsewhere (Gustavsson and Starke, 2017; McConnell et al., 2009). It is also possible that ‘not being listened to’ might be an indicator of discrimination.
Research has shown that when analysing care assessments concerning the involuntary removal of children from parents with IDs, it is sometimes impossible to know whether earlier support measures failed because the parents’ caring abilities could not be improved or because the support was not sufficiently adapted to their needs (Alexius and Hollander, 2014). This may have been an underlying factor in the mothers’ reported trust issues with social workers and their feelings of a loss of rights in our study.
The third category to change in the domain of Experiences of visits entailed moving from lacking strategies to build relationships with their children to developing improved strategies for building and maintaining a good relationship with their children. These could include strategies to facilitate responsiveness to their needs and to discover alternative ways to construct mother–child relationships. Improved parent–child relationships correspond with the suggestions of Bullen and colleagues (2017) who indicate that group programmes have the potential to improve parent–child relationships and the quality of contact visits. The present study shows that this is also true for people with IDDs. The new strategies from the support group may involve long-term improved social relationships and psychological wellbeing for the mothers, as described by McConnell and colleagues (2008).
Main Findings Of Support To Parents
The sense of abandonment and insufficient support lasted over time for the mothers. The mothers felt that they lacked an important role in relation to social services and expressed feelings of desertion and worthlessness – a phenomenon described previously (Mayes and Llewellyn, 2012; Memarnia et al., 2015). Lack of support and acknowledgement as a parent can contribute to anger and the struggle to maintain their identity as a parent (Schofield et al., 2011). Schofield and colleagues (2011) have presented recommendations on how social workers can support parents in managing their parental identity and encourage their involvement. Similarly, our findings with mothers with IDDs show that the experiences of lacking support as well as not being acknowledged by society often remain over time, suggesting the importance of social workers having a strategy to meet these needs. Engaging independent advocates could support parents with IDs in contact with social workers and help them have their voices heard (Atkin and Kroese, 2022).
Experiences of support that changed over the course of the interviews include the previous refusal of support or asking for support but being rejected by the authorities. Experiences of unsuitable or even disruptive support developed into insights about the consequence of not getting tailored and relevant support in time, awareness that support can make a difference and the emergence of skills to express needs and wanting to learn new strategies. New insights and skills could be interpreted as resulting from the intervention’s tailored support. The value of offering tailored support has been underscored elsewhere (Babinski et al., 2012; Chronis-Tuscano et al., 2011; Jans et al., 2015). The present study shows that mothers with IDDs and children in care can benefit from the MTA intervention. McConnell and colleagues (2009) showed that group interventions could affect social skills, which are essential for strengthening social inclusion. This finding was also observed in the present study.
Our findings showed that attitudes towards support changed following the intervention. Overall, the process entailed a change towards accepting help. Asking for and accepting support is protective (Meppelder et al., 2015). Accepting support plays a key role in the practice of parenting and in child development outcomes (Feldman and Aunos, 2020). The altered attitudes and acceptance of support can create new possibilities for collaborative alliances with social workers.
The findings of this study indicate that the MTA group intervention can support mothers with IDDs in their mothering role, with improved insights into helping them cope with their children being in care. In general, people with IDDs need professional support to manage grief, restore self-confidence and engage in daily life (Brickell and Munir, 2008). Strategies for managing grief may contribute to the reduced anxiety and depression often seen in the participants of these groups (Wade et al., 2015). Considering the increased risk of children being in care (LaLiberte et al., 2017; McConnell et al., 2021; Tøssebro et al., 2017) and the vulnerability of parents with IDDs, our study confirms the importance of providing adapted support (Azar et al., 2012; Banks et al., 2008; Chronis-Tuscano et al., 2008; Feldman, 1994; Johnston et al., 2012; Minde et al., 2003; Starke, 2005; van Steijn et al., 2013). Also, this position is consistent with the United Nations Convention (article 23): parents with disabilities must get adapted support to manage their crisis and adjust to their new parenting role. In all, the results of this study support the findings of Schofield and colleagues (2011), who showed that social workers need to meet parents with awareness, provide frequent information about the child and involve them as often as possible. Additionally, tailored group interventions should be offered to help mothers maintain a legitimate and reasonable parenting role.
Methodological Issues
The sample size of this study was small, and all three participants were recruited from the same group. However, we used a single-case design in the interviews with the mothers to better capture the complexity of their experiences over time. Further, the participants varied in characteristics. The interviews were performed by researchers with extensive experience of interviewing people with IDDs. Two of the authors were involved in further developing and culturally adapting the method. The other two authors contributed extensive competence of the target group and methods for parenting support.
All the participating mothers self-reported their ADHD or ADD diagnoses. The recruitment was conducted by professionals in social services and adult rehabilitation, who identified the mothers as having an IDD and thereby being likely to benefit from the adapted support group. The invitation to the support group was explicit in inviting mothers with IDDs, indicating that the mothers were aware of having an IDD.
Conclusion
Despite their previous circumstances (e.g., life crises, the trauma of placement and lack of support), this study demonstrated that an intervention adapted to the needs of mothers with IDDs contributed to a change towards long-lasting experiences of greater wellbeing and engaging mothers in a process of reconciliation with their children in care. Further research is needed on prejudice in the social care system and group interventions for parents with IDDs whose children are in care in Sweden and other countries.
Clinical Implications
The findings of this study support the existing literature on the vulnerability of parents with IDDs whose children are in care and their need for targeted interventions. As part of their role, social workers can support these parents by acknowledging the need for advocacy and ensuring that the system treats families justly. Professionals should be aware of the value of providing adapted support to parents with IDDs. This includes support for family preservation and, if children have to be placed in out-of-home care, support to process the life changing circumstances. Intervention can support a process of empowerment for these parents, who can develop a greater understanding of and ability to cope with the realities of their parenting role and the grief of their children being in care. This can ultimately affect the parent–child relationship, as well as the collaboration between the parent, the social worker and the family home. This study showed that the benefits could last for at least a year following intervention.
Footnotes
Acknowledgments
The authors would like to express their gratitude to the participants.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Erik och Carola Tengströms fond and Stiftelsen Allmänna Barnhuset.