
Abstract
Introduction:
Deliberate self-harm and suicide attempts share common risk factors but are associated with different epidemiological features. While the rate of suicide after deliberate self-harm has been evaluated in meta-analyses, the specific rate of death by suicide after a previous suicide attempt has never been assessed. The aim of our study was to estimate the incidence of death by suicide after a nonfatal suicide attempt.
Method:
We developed and followed a standard meta-analysis protocol (systematic review registration—PROSPERO 2021: CRD42021221111). Randomized controlled trials and cohort studies published between 1970 and 2020 focusing on the rate of suicide after suicide attempt were identified in PubMed, PsycInfo and Scopus and qualitatively described. The rates of deaths by suicide at 1, 5 and 10 years after a nonfatal suicide attempt were pooled in a meta-analysis using a random-effects model. Subgroup analysis and meta-regressions were also performed.
Results:
Our meta-analysis is based on 41 studies. The suicide rate after a nonfatal suicide attempt was 2.8% (2.2–3.5) at 1 year, 5.6% (3.9–7.9) at 5 years and 7.4% (5.2–10.4) at 10 years. Estimates of the suicide rate vary widely depending on the psychiatric diagnosis, the method used for the suicide attempt, the type of study and the age group considered.
Conclusion:
The evidence of a high rate of suicide deaths in the year following nonfatal suicide attempts should prompt prevention systems to be particularly vigilant during this period.
Introduction
Suicide is a leading cause of avoidable death worldwide, with approximately 800,000 deaths per year (World Health Organization, 2014). Suicide rates have been declining annually throughout the world since 2000 (Fazel and Runeson, 2020). Moreover, with at least 16 million per year, suicide attempts (SAs) are estimated to be 25–50 times more common than deaths by suicide (Fazel and Runeson, 2020). For several decades, many efforts have been made to highlight the risk factors involved in suicidal risk to reduce suicidal behavior, to protect those exposed to it and to implement suicide prevention programs (Demesmaeker et al., 2021; Hill et al., 2020; Zalsman et al., 2016).
In this context, deliberate self-harm (DSH), including SAs, has been particularly investigated, as they are more frequent, as the data on DSH are routinely collected at admission to hospital. Moreover, DSH are supposed to share risk factors for death by suicide (Knipe et al., 2019; Runeson et al., 2016). DSH is defined as an act of intentional injury or damage to the body, including nonfatal SA and all other injuries (e.g. self-poisoning, cutting or burning), irrespective of the suicidal intent to die or not (NHS Inform, n.d.). Moreover, DSHs have been the subject of more research because they do not require the researcher to establish the suicidal intent of the act (Huang et al., 2017; Wilkinson et al., 2011).
The scientific literature has already focused on the risk of death by suicide after a nonfatal DSH episode and the risk of suicides after discharge from nonpsychiatric settings through three literature reviews and meta-analyses (Carroll et al., 2014; Owens et al., 2002; Wang et al., 2019). First, in 2002, a systematic review estimated the suicide rate after a nonfatal DSH episode at 1.8% at 1 year, 3.4% between 4 and 9 years and 6.7% over 9 years (Owens et al., 2002). A more recent meta-analysis, in 2014, estimated the risk of suicide after hospital discharge for DSH to be 1.6% within the first year and 3.9% within 5 years (Carroll et al., 2014). Third, a meta-analysis on participants who presented with suicidal thoughts and behaviors in nonpsychiatric settings found that the pooled suicide rate was 483 suicide deaths per 100,000 person-years (Wang et al., 2019). The first two studies cited above included all studies exploring DSH episodes whether the suicidal intent for the episode was investigated or not and even whether self-injury leading to healthcare contact was a habitual nonsuicidal behavior (Carroll et al., 2014; Owens et al., 2002). The latest review explored suicidal thoughts and behaviors after discharge from nonpsychiatric settings and therefore excluded a large number of subjects consulting for suicidal acts.
Interestingly, while the rate of suicide after a nonfatal DSH has been evaluated in systematic reviews and meta-analysis, the specific rate of death by suicide after an SA after discharge from psychiatric or nonpsychiatric healthcare services has never been assessed through a meta-analysis or other statistical analysis pooling multiple-source databases. Indeed, nonsuicidal self-injury, generally covered by the term ‘self-harm’, may be distinct from suicidal behavior; therefore, several authors have suggested establishing the suicidal purpose of a DSH episode to appropriately classify attempts into suicidal or nonsuicidal (De Leo et al., 2006; Fazel and Runeson, 2020; Nock, 2010; Oquendo and Courtet, 2015). Some authors have also suggested distinguishing these two terms since they are associated with different epidemiological features, providing more consistency in nomenclature and improving research on suicide prevention programs (Fazel and Runeson, 2020; Oquendo and Courtet, 2015).
The aim of our study was to estimate the incidence of death by suicide after a nonfatal SA. Therefore, we performed a systematic review and meta-analysis of published aggregated data. We hypothesized that the rate of death by suicide after a previous nonfatal SA must be higher than that after any DSH episode.
Methods
We developed and followed a standard meta-analysis protocol (systematic review registration—PROSPERO 2021: CRD42021221111).
Types of participants
We reviewed studies involving patients with a history of a previous SA. Definitions by Beck ‘a situation in which a person has performed an actually or seemingly life-threatening behavior with the intent of jeopardizing his life, or to give the appearance of such an intent, but which has not resulted in death’ (Beck et al., 1972) and O’Caroll ‘a potentially self-injurious behavior with a nonfatal outcome, for which there is evidence that the person had the intent to kill him/herself, but failed, was rescued or thwarted, or changed one’s mind’ were used to define a nonfatal SA. A serious SA is defined as ‘an attempt that would have been fatal had it not been for the provision of rapid and effective emergency treatment’. Inclusion criteria were a history of SAs or a history of DSH or self-poisoning if a suicidal intent of the episode was mentioned. We excluded studies including participants with a history of DSH, self-poisoning or any self-injury if no suicidal intent was evaluated or reported.
Types of interventions
Studies were eligible if they followed participants for at least 1 year and if they focused on the rate of subsequent death by suicide after a nonfatal SA.
Types of outcomes
We considered as a primary outcome the 1-year rate of deaths by suicide after a nonfatal SA. Secondary outcomes were the rate of suicide at 5 and 10 years after SA.
Types of studies
Our review was restricted to cohort studies and randomized controlled trials (RCTs), regardless of the inclusion location (consultation, liaison services, hospital presentation or admission). For RCTs, only information from the control arm was considered exempt from any effect of the treatment studied. Studies focusing on specific age groups or specific psychiatric disorders were also included.
Search strategy
We searched PubMed, PsycInfo and Scopus to identify all English- or French-language papers published between 1970 and 2020 using the following term combinations: ‘suicide attempt*’ AND ‘mortality’. Personal collection of the authors and then the reference sections of all included papers were also browsed to identify any additional relevant studies.
Study selection
The eligibility assessment was performed independently in a blind standardized manner by two reviewers (A.D. and A.H.). Disagreements were resolved by consensus or in consultation with a third reviewer (A.A.). We checked for multiple papers published with the same cohort of patients and avoided duplicates.
Assessment of methodological quality
All studies were assessed for methodological quality prior to inclusion in the review using an appropriate tool from the Joanna Brigs Institute (critical appraisal tools for prevalence studies and RCTs, which can be found in https://jbi.global/critical-appraisal-tools) for assessing the risk of bias. Each question was scored from 0 to 2 (0: no, 1: unclear, 2: yes).
Data collection
For the included studies, the following data were extracted: characteristics of the study (year, design, country), characteristics of the participants (number of patients, specific age group, specific clinical context), duration of follow-up and rate of suicide mortality.
Data analysis
Aggregated data were used. First, we performed a qualitative analysis describing each study, its design and the outcomes observed. A quantitative synthesis of all evidence available from the cohort studies and RCTs was then performed.
The incidence of death by suicide was calculated as the number of participants who died by suicide within a given time frame. The duration of follow-up can vary for participants in a study. If participants were recruited and followed up over different periods of time, the mean duration of follow-up was taken into consideration, and the estimated risk of death was investigated.
The rate of deaths by suicide at 1, 5 and 10 years after a nonfatal SA was calculated and pooled using a random-effects model, and the proportions were transformed into logits. All estimates are reported with their 95% confidence intervals (95% CIs). Second, subgroup analyses were performed investigating the relationship between different types of studies (i.e. cohort studies or RCTs), continents, specific age groups, year of publication, the characteristics (e.g. first SA, serious SA) and methods used for the SAs and the assessment of psychiatric disorders, and the rate of suicide. Third, we evaluated potential moderators: year of publication, mean age of participants and the total number of participants at baseline through meta-regression analysis.
Statistical heterogeneity was visually inspected on the forest plots and evaluated with the I2 index and the Q statistic. Studies introducing substantial heterogeneity (I2 > 50% and/or p value of the Q test > 0.10) were identified and described. Then, sensitivity analysis without these studies was performed. The existence of a small study effect, suggestive of possible publication bias, was investigated graphically using a funnel plot.
All analyses were performed using R and the Metafor package (Viechtbauer, 2010). The results are presented according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement (Page et al., 2021).
Results
Studies included
A total of 2642 papers were screened, and 41 were included in the meta-analysis (25 for 1-year suicide rate estimation, 14 for 5-year suicide rate and 11 for 10-year suicide rate) (see Table 1 and Figure 1).
Description of studies in the meta-analysis.
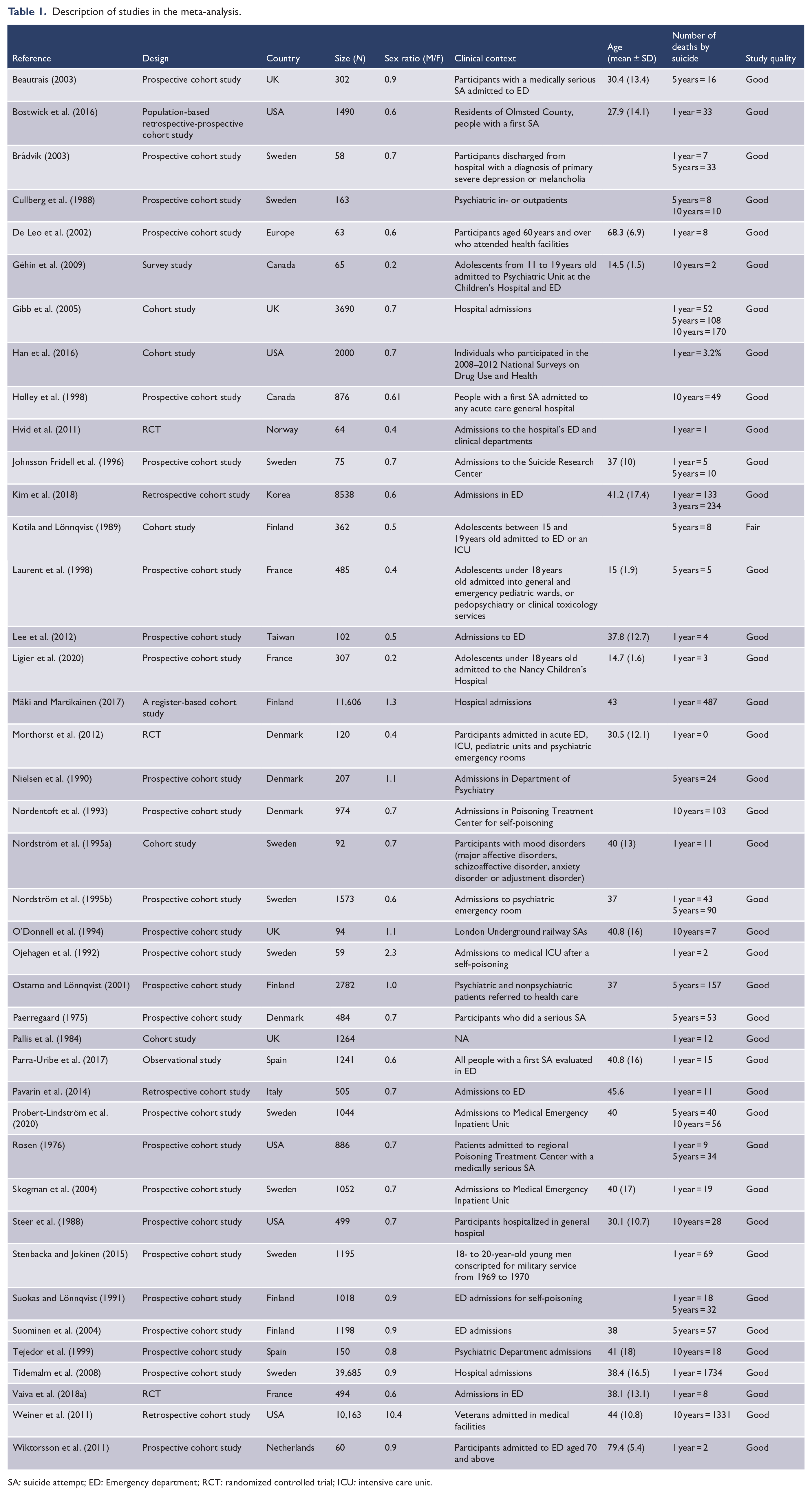
SA: suicide attempt; ED: Emergency department; RCT: randomized controlled trial; ICU: intensive care unit.
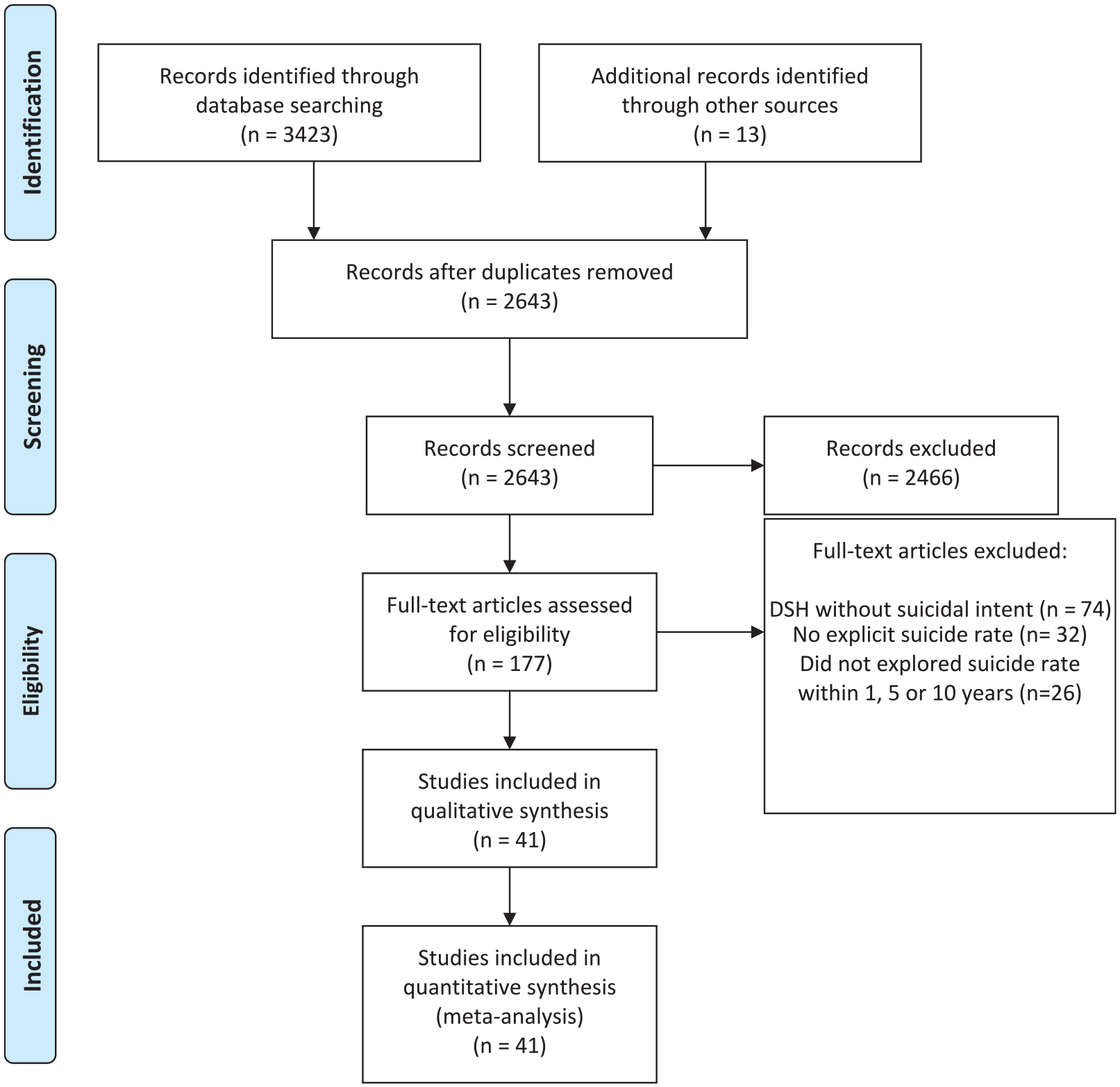
Literature review flow chart.
Study characteristics, risk of bias within studies and qualitative analysis
Study characteristics
Among the studies included in the quantitative analysis, 38 (92.7%) were cohort studies and 3 (7.3%) were RCTs. Among the studies, 32 (78%) were undertaken in Europe, 7 (17%) in North America and 2 (4.9%) in Asia. In addition, two studies focused specifically on mood disorders (one study on primary severe depression or melancholia and one study on inpatients suffering from major affective disorders [unipolar or bipolar depression], anxiety disorders, schizoaffective disorder or adjustment disorders) or on specific age groups (four on adolescents and two on the elderly). Six studies (15%) took only a single method or characteristic of SA into consideration: four studies on self-poisoning and two of all serious SAs. Finally, two studies specifically included participants with a first SA.
Description of the RCTs
Three RCTs were considered for the qualitative analysis evaluating interventions for the prevention of a suicide reattempt (Hvid et al., 2011; Morthorst et al., 2012; Vaiva et al., 2018a). Hvid et al. (2011) conducted an RCT involving 133 participants (64 in the control group) admitted to the emergency department and clinical departments after an SA in Norway. Patients with major psychiatric diagnoses (schizophrenia, bipolar disorder, severe/psychotic depression) were not included. Vaiva et al. (2018a) conducted an RCT on 1040 patients (494 in the control group) recruited in French emergency departments. Morthorst et al. (2012) included 234 participants (120 in the control group) admitted to the acute emergency department, intensive care unit, pediatric units and psychiatric emergency rooms. They excluded patients diagnosed with schizophrenia spectrum disorders and patients living in institutions. For these RCTs, the risk of bias was high due to not blinding the participants and personnel (see supplementary materials, Table 2).
Description of the cohort studies
Bias was heterogeneous from low to high for the cohort studies (see supplementary materials, Table 2). The sample size was less than 100 participants for 9 (22.5%) cohort studies (see Table 1). The participants were not described in detail for seven (17.5%) studies and were included from different care settings (emergency departments, psychiatric departments, poisoning centers, etc.). Moreover, the definition of an SA was heterogeneous across studies and constituted a risk of bias. In several studies, the definition used to characterize an SA was not specified or was imprecise (De Leo et al., 2002; Han et al., 2016; Ojehagen et al., 1992). All details are available in Table 1 and supplementary material Table 1.
Incidence of suicide at 1 year after an SA
The pooled estimated incidence of death by suicide within 1 year after a nonfatal SA was 2.77% (2.22–3.46) (see Table 2 and Figure 2). Heterogeneity among the studies was high (I2 = 93.5% and Q test: p < 0.01).
Subgroup analysis exploring the incidence of death by suicide after SA on different continents, psychiatric diagnoses and age groups.
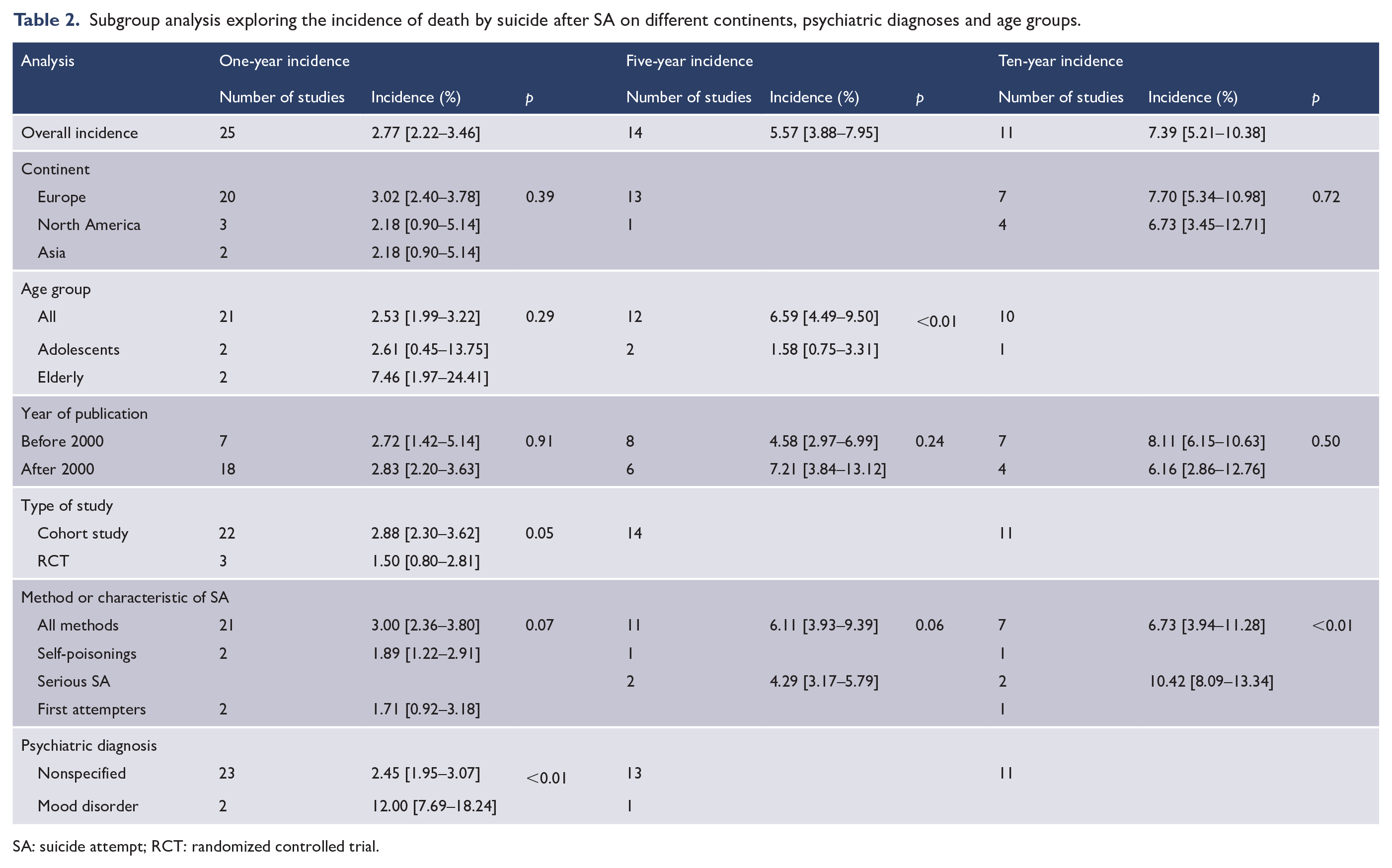
SA: suicide attempt; RCT: randomized controlled trial.
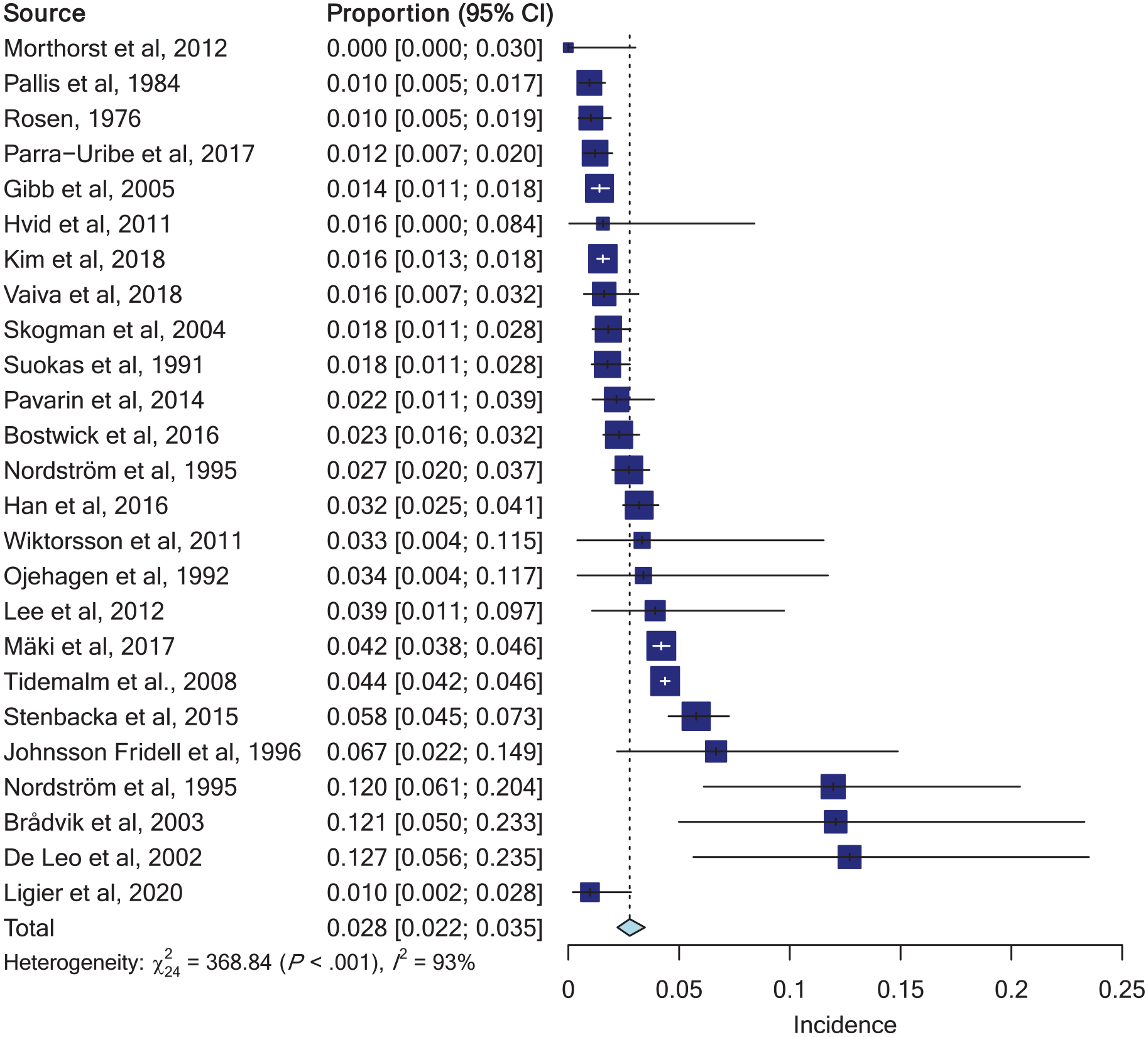
Forest plot of 1-year suicide rates.
Subgroup analysis showed different suicide rates when the psychiatric diagnosis and the type of study were taken into consideration (p < 0.05). Indeed, participants with a mood disorder had a higher estimated incidence of subsequent suicide after an SA (12.00% [7.69–18.24]) compared to participants included regardless of a psychiatric disorder. Higher suicide rates were also found in cohort studies (2.88% [2.30–3.62]) than in RCTs (1.50% [0.80–2.81]). Subgroup analysis of studies focusing on self-poisoning and on people with a first SA showed nonsignificantly lower suicide rates (1.89% [1.22–2.91] and 1.71% [0.92–3.18], respectively).
Finally, meta-regressions did not highlight any effect of the year of publication, mean age of the participants or the total number of participants at baseline on the 1-year suicide rate (p > 0.05) (see supplementary materials, Table 1).
Incidence of suicide at 5 years after an SA
The pooled estimate of the 5-year suicide rate after an SA was 5.57% (3.88–7.95) (see Table 2 and Figure 3). The studies showed significant heterogeneity (I2 = 94.7% and the heterogeneity chi-square test: p < 0.001).
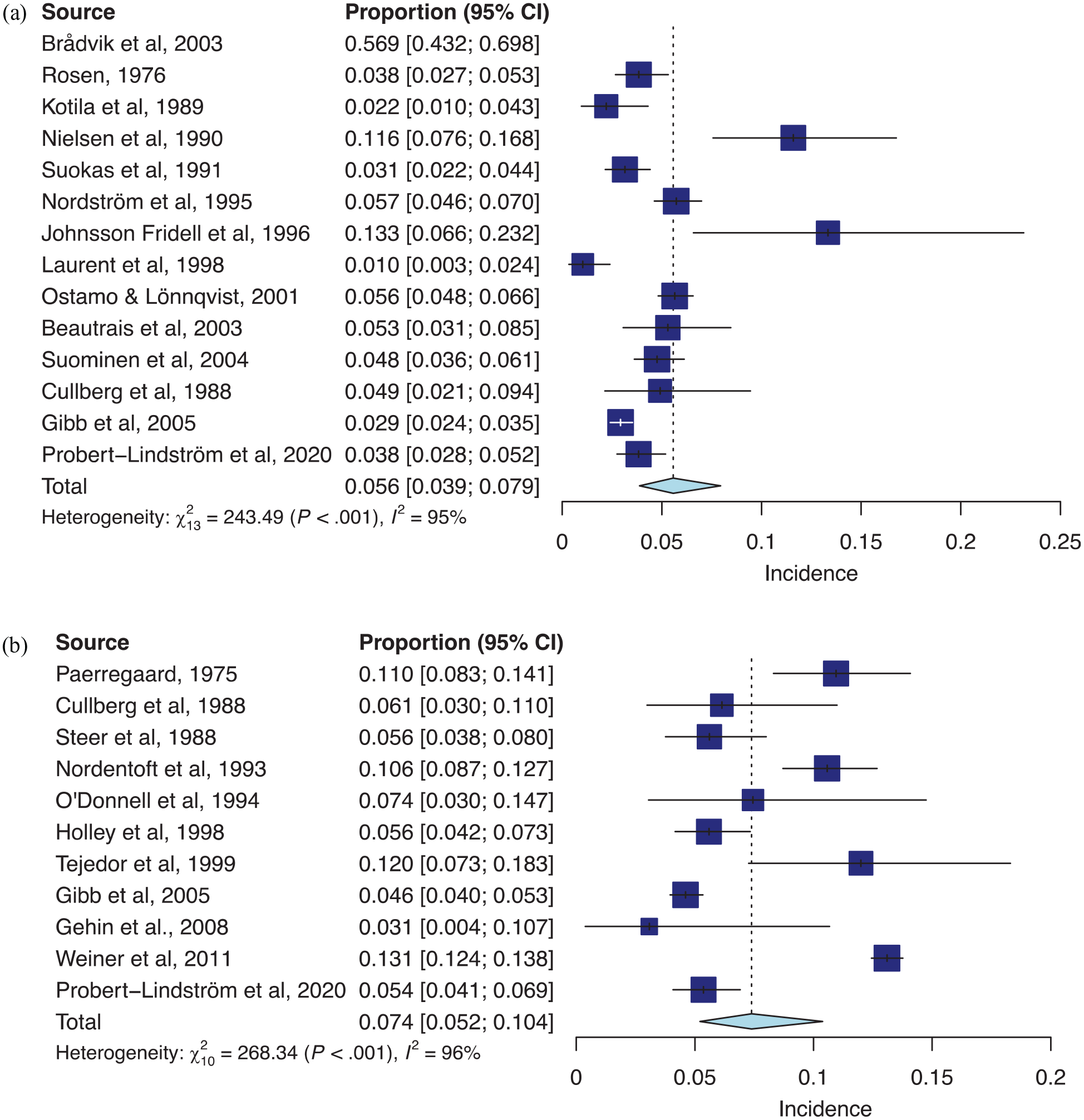
Forest plot of (A) 5-year suicide rates and (B) 10-year suicide rates.
Subgroup analysis highlighted significantly different estimates of 5-year suicide risk according to specific age groups. Studies evaluating adolescents had a significantly lower incidence of suicide death at 5 years (1.58% [0.75–3.31]).
Finally, univariate meta-regressions showed an effect of the mean age of the participants on the 5-year suicide rate with an increase in the incidence of subsequent death with age (p = 0.02) and the findings suggested that the mean age of the participants explained 48% of the between-study variance in the estimates.
Incidence of suicide at 10 years after an SA
The pooled estimate of the 10-year suicide rate after a nonfatal SA was 7.39% (5.21–10.38) (cf. Table 2 and Figure 3). Important heterogeneity existed among the studies with I2 = 96.3% and the heterogeneity chi-square test (p < 0.001).
In the subgroup analysis, different rates of deaths by suicide were found according to the method used for the SA or characteristic of SA (p < 0.01). People with a first SA had a lower incidence of subsequent deaths by suicide (5.59% [4.25–7.32]), whereas patients who used self-poisoning or who did a serious SA had a higher incidence of subsequent deaths (10.57% [8.79–12.67] and 10.42% [8.09–13.34], respectively).
Meta-regressions did not highlight any effect of the year of publication, mean age of the participants or the total number of participants at baseline on the 10-year suicide rate (p > 0.05).
Sensitivity analysis
According to the forest plot, two studies focusing on mood disorders and a study on the elderly were introducing substantial heterogeneity when estimating the suicide incidence at 1 year after an SA (Brådvik, 2003; Nordström et al., 1995a). The 1-year suicide rate estimate was 2.34% (1.85–2.95) after exclusion of these studies. Nonetheless, heterogeneity remained high (I2 = 93.8%). In addition, two studies with small sample sizes appeared to be outliers when estimating the 5-year suicide rate (Johnsson Fridell et al., 1996; Nielsen et al., 1990). Sensitivity analysis without these studies showed a 5-year incidence of 5.20% (3.45–7.77). Finally, no study seemed to be an outlier when estimating the 10-year suicide rate after an SA. Thus, sensitivity analysis was not performed for the estimates of the 10-year suicide rate.
Assessment of publication bias
The investigation of the funnel plots did not show any evidence of publication bias.
Discussion
Our literature review and meta-analysis based on 41 publications estimated the 1-year suicide rate after a nonfatal SA at 2.8% (2.2–3.5), the 5-year suicide rate at 5.6% (3.9–7.9) and the 10-year rate at 7.4% (5.2–10.4). Interestingly, the results of our subgroup analysis showed that the estimates of suicide rate vary widely depending on the psychiatric diagnosis, the method used for the SA, the type of study and the age group considered. Moreover, our results suggested that the incidence of death by suicide was the highest during the first year after a nonfatal SA.
Notably, our study is the first meta-analysis to explore the rate of death by suicide after a nonfatal SA. Hence, two previous meta-analyses exploring the rate of suicide after any DSH episode found lower estimates (i.e. 1.6% [1.2–2.4] at 1 year and 3.9% [3.2–4.8] after 5 years) (Carroll et al., 2014; Owens et al., 2002). Thus, the risk of subsequent death by suicide seems to be higher where there is suicidal intent. They also noticed a higher risk of death by suicide during the first year after a nonfatal SA. These results are of major importance in suicide prevention, as the key challenge is to determine which patients are at higher risk of death by suicide and when they are at highest risk.
In the subgroup analysis, a higher rate of deaths by suicide at 1 year was found for participants suffering from mood disorders compared to studies including participants regardless of the psychiatric diagnosis. These results are consistent with the scientific literature, as depression or bipolar disorder and a history of a previous SA are well-known risk factors for death by suicide (Arsenault-Lapierre et al., 2004; Chesney et al., 2014; Christiansen et al., 2007; Large et al., 2011). The interaction between these two factors may increase the risk of future death by suicide. Moreover, patients with major affective disorders and a history of previous SA were also associated with a higher risk of long-term suicide in a cohort of 954 participants (Fawcett et al., 1990).
Interestingly, our findings also indicated great variations in the rates of subsequent death by suicide in specific age groups in comparison to studies where all age groups were investigated. Concerning the adolescents, we found significantly lower suicide rates at 5 years after an SA. Therefore, the risk of death by suicide for adolescents appears to be high during the first year after an SA and then it seems to decrease. Nonetheless, the 1-year rate was estimated according to a study on Swedish young men and may be affected by selection bias (Stenbacka and Jokinen, 2015). In a previous meta-analysis on suicide rates among people discharged from nonpsychiatric settings after presenting for suicidal behaviors, lower rates of future suicides were found for adolescents (Wang et al., 2019). Moreover, in long-term cohort studies on adolescents, almost twice as many deaths occurred due to violent causes (i.e. substance abuse, road accident, drowning, homicide) rather than from suicide after an SA (Granboulan et al., 1995; Kotila and Lönnqvist, 1989).
In addition, we estimated nonsignificantly higher 1-year suicide rates for the elderly according to two European studies (De Leo et al., 2002; Wiktorsson et al., 2011). Nonetheless, the sample sizes of these two studies were small, and wide confidence intervals were therefore estimated. The results of our meta-regression also noticed an association between age and death by suicide. Indeed, we found an increase in the incidence of death by suicide at 5 years with increasing age. Our results are consistent with international literature, as it has been shown that suicide rates were also high for the elderly at 3 and 6 years after an SA and that older age is a risk factor for suicide among suicide attempters (Hepple and Quinton, 1994; Lebret et al., 2006; Parra-Uribe et al., 2017). Interestingly, while neurocognitive disorders, physical illnesses, and physical and psychological pain are well-known risk factors for suicidal behavior among the elderly (Conejero et al., 2018; Conwell, 2014; Conwell et al., 2011), in the years following an SA, the elderly had higher rates (from 3- to 7-fold) of deaths from causes other than suicide (Hepple and Quinton, 1994; Wiktorsson et al., 2011).
According to our results, a lower 1-year rate of death by suicide was found when participants were people with a first SA. It has been demonstrated in several cohort studies of suicide attempters that having more than one previous SA was a risk factor for a suicide reattempt (Irigoyen et al., 2019; Suokas and Lönnqvist, 1991).
Moreover, we found that the 1-year suicide rates was almost half when the method used for the index SA was self-poisoning. The lower rates could be explained by a lower risk of repetition after self-poisoning compared to other methods, as has been found in a Swedish study (Runeson et al., 2010).
Finally, for serious SAs, the rate of subsequent death by suicide was higher at 10 years than for nonserious SAs. In the current literature, violent and serious SAs were also more likely to be associated with a higher risk of repetition (Giner et al., 2014; Runeson et al., 2010).
Strengths and limitations
Our study is, to our knowledge, the first meta-analysis on suicide mortality after a nonfatal SA. Whereas other meta-analyses took into consideration all DSH attempts, we focused on studies specifically analyzing SAs for more consistency in epidemiology. One of the strengths of our study is the inclusion of studies that focused on specific age groups, specific psychiatric diagnoses and the inclusion of studies regardless of the method used for the index attempt and the participant inclusion setting. Second, we performed subgroup meta-analysis to take into consideration these specificities and to assess their weight in the suicide rate estimates. Moreover, another strength is the absence of publication bias assessed through funnel plots.
One of the limits of our results is the small number of studies found, the small sample sizes of the studies and the high between-study heterogeneity. Therefore, we performed sensitivity analysis, but heterogeneity was persistent after removing the outliers from the analysis at 1 and 5 years. The high level of heterogeneity between the included studies is a significant limitation to the interpretation of the results and particularly to the estimation of the suicide death rate. Nevertheless, a random-effects meta-analysis was used to reduce this bias, and we did not find any impact of sample size or year of publication in our meta-regression analysis. Second, subgroup meta-analyses were based on a small number of studies rather than two for the assessment of the specific age group rates, psychiatric diagnosis and index methods of SA. We still chose to perform these analyses to encourage future research, but results must be interpreted with caution. Third, meta-regression on the mean age of the participants did not find a significant effect on the 1-year suicide rate according to our results. This could be explained by the nonlinearity of the mean ages of the participants and the heterogeneity of the results. Fourth, the risk of bias was heterogeneous from low to high for the cohort studies. Notably, the definition used to characterize the index SA was not specified or was imprecise in several studies and this constituted a bias. Nevertheless, the study quality was fairly high for the majority of the studies included. Finally, the interaction between risk factors was not examined as we did not have access to individual data from the primary studies and we used summary data provided in the included publications.
Conclusion
In conclusion, while half of patients die during their first suicide attempt, those who survive are a group of subjects with a well-known high risk of suicide (Isometsä and Lönnqvist, 1998; Jordan and McNiel, 2020). Hence, the risk of death by suicide after a failed SA remains very high, especially during the first year and seems to persist for many years. The evidence of a high rate of suicide deaths in the year following nonfatal SAs should prompt prevention systems to be particularly vigilant during this period, especially for people with chronic mood disorder. Moreover, little is known about suicide mortality after SA in specific populations, such as adolescents and the elderly, or according to specific psychiatric diagnoses, and further research is needed. Future studies may more accurately identify participants with higher death rates to improve the current prevention programs.
Supplemental Material
sj-docx-1-anp-10.1177_00048674211043455 – Supplemental material for Suicide mortality after a nonfatal suicide attempt: A systematic review and meta-analysis
Supplemental material, sj-docx-1-anp-10.1177_00048674211043455 for Suicide mortality after a nonfatal suicide attempt: A systematic review and meta-analysis by Alice Demesmaeker, Emmanuel Chazard, Aline Hoang, Guillaume Vaiva and Ali Amad in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-docx-2-anp-10.1177_00048674211043455 – Supplemental material for Suicide mortality after a nonfatal suicide attempt: A systematic review and meta-analysis
Supplemental material, sj-docx-2-anp-10.1177_00048674211043455 for Suicide mortality after a nonfatal suicide attempt: A systematic review and meta-analysis by Alice Demesmaeker, Emmanuel Chazard, Aline Hoang, Guillaume Vaiva and Ali Amad in Australian & New Zealand Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.