
Abstract
Recently there has been increasing international interest in the epidemiology and outcomes of those making suicide attempts [1–4]. One aspect of this interest has focused on the extent to which suicidal behaviours are repetitive. Two lines of evidence suggest that suicidal behaviours are repetitive: many of those who die by suicide have made a previous suicide attempt [5]; and many of those who make a non-fatal suicide attempt will make subsequent attempts [4], [6], [7].
For example, in a 5 year follow-up of a consecutive series of 302 individuals admitted to Christchurch Hospital (New Zealand) for medically serious suicide attempts, Beautrais [4] found that 37% made at least one further attempt and 6.7% died by suicide. However, a limitation of this study is that it considers only medically serious suicide attempts occurring during a particular time period.
Against this background, this study reports an extension of Beautrais' study, examining suicide attempts of all types of severity admitted to Christchurch Hospital during the 10-year period 1993–2002. The specific aims of this study were: (i) to estimate mortality from suicide, and for all causes, in all individuals admitted to Christchurch Hospital for suicide attempts during the 10-year period from 1993 to 2002; and (ii) to examine the risk of further admissions to Christchurch Hospital for attempted suicide in this group.
Method
Participants
Participants were a consecutive series of 3690 individuals (1467 males; 2223 females; age range 9–90 years) admitted to Christchurch Hospital, New Zealand, for suicide attempts during the 10-years period from 1993 to 2002. Christchurch City has a population of approximately 330 000 and the Canterbury region (including Christchurch City) has a population of approximately 450 000. Christchurch Hospital is the sole entry point for suicide attempts from the Canterbury region.
Data sources
Data on hospital admissions for suicide attempts were obtained from the Canterbury District Health Board which routinely collects these data for the New Zealand National Minimum Data Set. National Health Index (NHI) numbers reported with each admission provided a unique identifier for each individual in the study and allowed multiple attempts to be linked to an individual. The first admission for each individual within the study period was defined as the index attempt.
Measures
From the database of the study, the following measures were available for each participant: date of birth; gender; dates of admission; length of the study period (from the index attempt to 31 December 2002); total number of hospital admissions for attempted suicide during the study period.
Method of suicide attempt was classified according to ICD-9 [8] and ICD-10 [9] causes of injury codes for intentional self-harm (X60-X84 and E950-E959). Where more than one method of suicide was used in a specific attempt, the method of highest lethality was recorded as the principal method, using Card's classification of lethality of method of suicide attempt [10]. The index suicide attempt method was available for 3686 of 3690 (99.9%) participants.
Mortality
The New Zealand Health Information Service (NZHIS) holds all national death certificate details in a mortality database (National Mortality Database). This database was checked for each individual up to 31 October 2003. From this database, date and cause of death were established for those individuals who died.
Results
Mortality after an index suicide attempt
The cumulative risk of death from all causes and by suicide was determined for the 10 years study period. By the end of the study period, 12.4% of those making attempts had subsequently died.
Table 1 shows the risk of subsequent death by suicide for males, females and the total sample for the 10-year study period. Gender differences in risks of suicide were tested using a log-rank test.
Cumulative risk of suicide (%) during the 10 years following an index suicide attempt
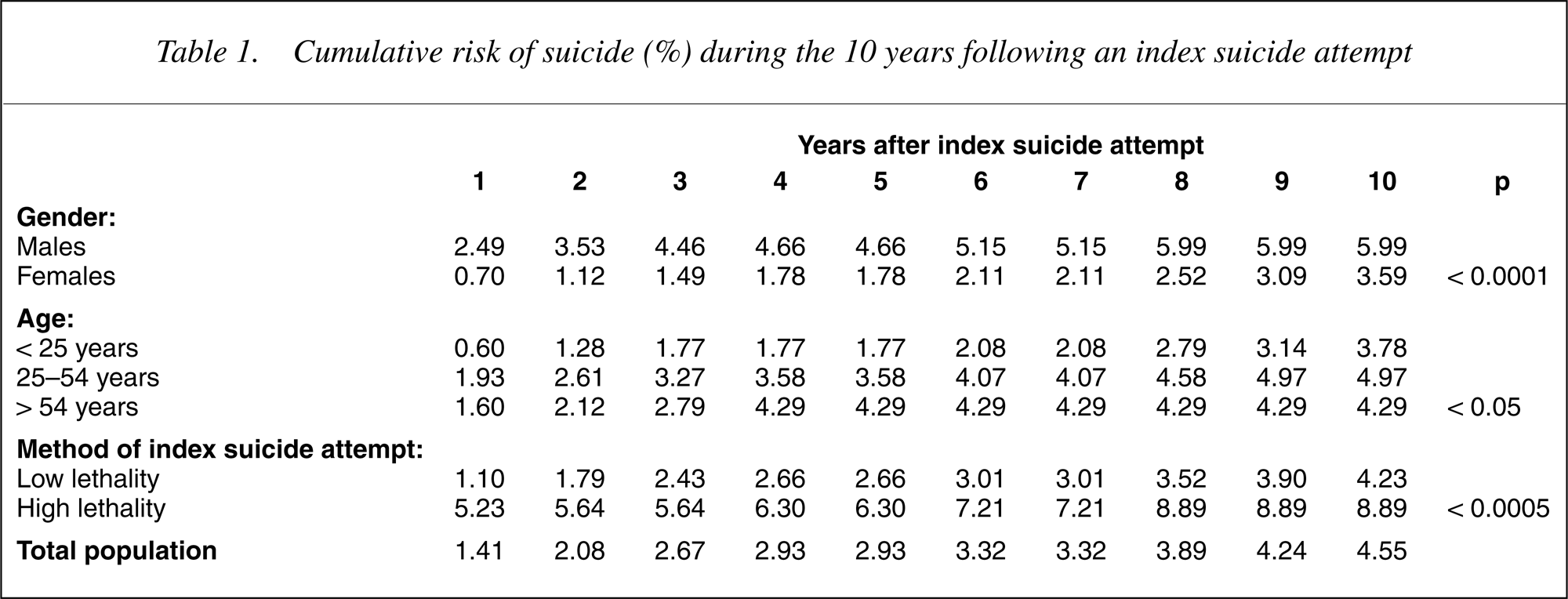
The table shows: (I) By the end of the 10-year study period, 4.6% of those making a suicide attempt had subsequently died by suicide; (ii) Risks of death by suicide were significantly higher for males than for females (p < 0.0001) (χ2 = 1: 22.44).
Table 1 also compares risk of death by suicide across three age groups: < 25 years (n = 1378), 25–54 years (n = 2047) and < 54 years (n = 265). There is a significant trend for risks of suicide to be higher in those aged 25 years and over than those aged less than 25 years (p < 0.05) (χ2 = 2: 7.48).
Finally, 10]. The table shows that the risk of subsequent death by suicide was significantly higher in those using an index attempt method of high lethality than in those using an index attempt method of low lethality (p < 0.0005) (χ2 = 1: 16.58).
Risk of further suicide attempts
Using survival analysis, the cumulative risk of first readmission to hospital (following an index suicide attempt admission) over the study period was determined.
Table 2 shows the risk of readmission to hospital for attempted suicide for males, females and the total sample for the 10 years study period. Gender differences in risks of suicide were tested using a logrank test. Table 2 shows: (I) by the end of the study period, 28.1% of those making index suicide attempts had been readmitted at least once for attempted suicide; (ii) risks of readmission for attempted suicide were significantly higher for females than for males (p < 0.0001) (χ2 = 1: 14.5).
Cumulative risk of readmission (%) to Christchurch Hospital for attempted suicide during the study period
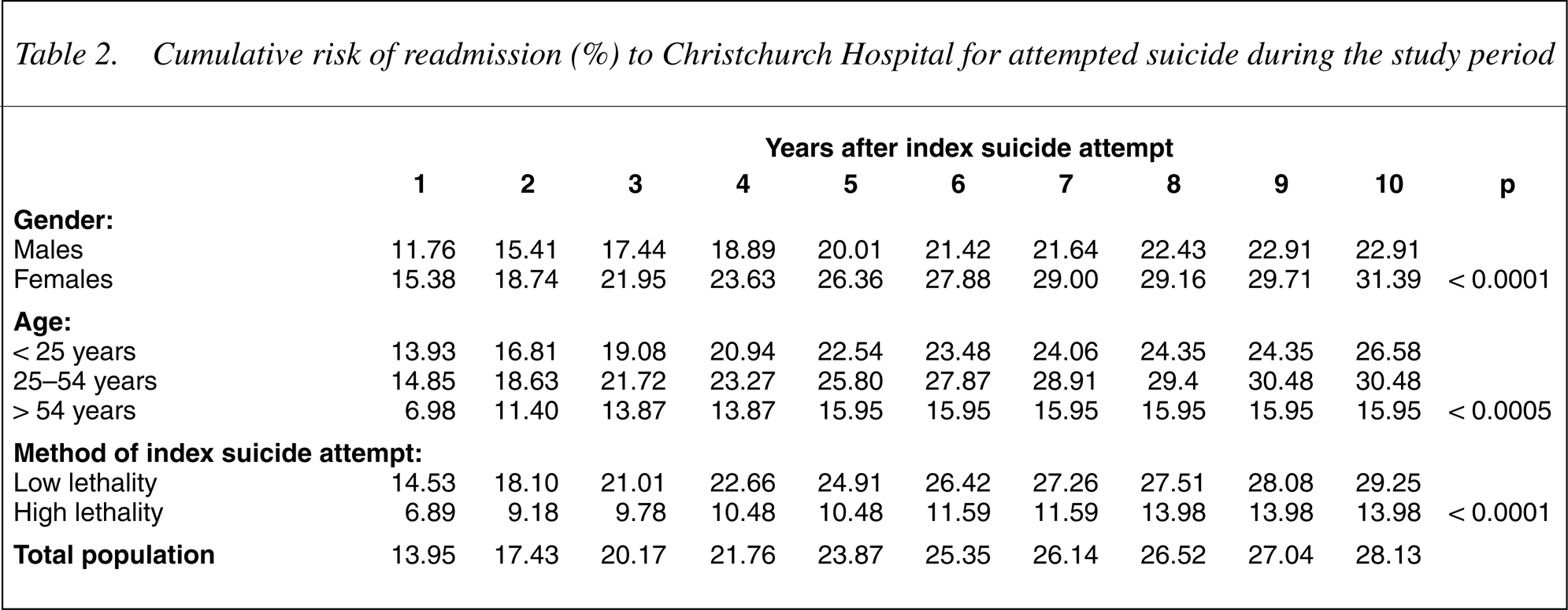
Table 2 also compares overall risks of readmission for attempted suicide by age group. The table shows that there is a significant trend for risks of readmission to be higher for those aged less than 55 years than for those aged over 54 years (p < 0.0005) (χ2 = 2: 15.0).
Finally, Table 2 also shows the risks of readmission for attempted suicide by the lethality of the index suicide attempt method. The table shows that the risk of readmission for attempted suicide was significantly higher in those with an index attempt method of low lethality than in those with an index attempt method of high lethality (p < 0.0001) (χ2 = 1: 21.0).
A limitation of the analysis in Table 2 is that it does not take into account multiple readmissions for attempted suicide. Many participants had multiple readmissions for attempted suicide with the number of readmissions ranging from 1 to 56. To address this issue, the data were reanalysed to estimate the mean number of admissions for attempted suicide, by gender and age group, in each year of the study. This analysis produced similar trends to those in Table 2: (I) the overall rate of readmissions per year for attempted suicide (excluding the index attempt) during the study period was 0.23; (ii) the rate of readmissions per year for females (0.27) was 1.8 (95% confidence interval [CI] 1.4, 2.2) times that of males (0.16); (iii) the rate of readmissions per year for older adults (< 54 years) (0.16) was 0.5 (95% CI = 0.3, 0.8) times that of adults (25–54 years) (0.25), and 0.5 (95% CI = 0.3, 0.9) times that of youth (< 25 years); (iv) the rate of readmissions per year during the first 2 years after an index suicide attempt (0.37) was 2.6 (95% CI = 2.1, 3.1) times higher than that over the rest of the study period (0.14).
Summary of results
The major findings from this study may be summarized as follows:
Total mortality during the 10 years after an index suicide attempt was 12.4%, and the risk of death by suicide was 4.6%. The risk of death by suicide was: higher in males than females; lower in youths than in adults or older adults; and higher after an index attempt method of high lethality than after an index attempt method of low lethality. The risk of readmission for a further non-fatal suicide attempt was relatively high (28.1%). The risk of readmission was: higher in females than males; lower in older adults than in youths or adults; and higher after an index suicide attempt method of low lethality than after an index suicide attempt method of high lethality. The overall rate of readmissions per year for attempted suicide during the study period was 0.23. The rate of readmissions was highest in the first 2 years following an index suicide attempt. The rate of readmissions was higher amongst females, and higher amongst youth and adults than older adults.
Discussion
This paper has examined subsequent suicide attempts, total mortality and death by suicide in a consecutive sample of 3690 individuals admitted to Christchurch Hospital for attempted suicide. This sample includes all individuals admitted for suicide attempts irrespective of the severity of the attempt. During the study period risks of mortality and readmission to Christchurch Hospital for attempted suicide were determined. The main conclusions and findings from this study are discussed below:
Risk of further suicidal behaviour and death
The risk of further suicidal behaviour during the 10 years following a non-fatal suicide attempt is high, with an estimated 28.1% of the sample making at least one further non-fatal suicide attempt which required hospital admission during the study period, and 4.6% of the sample dying by suicide. These results are consistent with findings reported by Beautrais [4] for outcomes following index suicide attempts of high medical severity and suggest that the risk of subsequent suicide and further suicide attempts following an index suicide attempt is high for all who attempt suicide, regardless of the medical severity of the index attempt.
Risks of readmission and death by suicide varied with the following.
Gender
Overall, there were more index admissions for women than men. This is consistent with previous studies which have found overall higher rates of suicide attempts in women [3], [11]. The consistently higher rates of suicide attempts in women in this and other studies may be due to higher risks of depression in women [12].
During the study period, the risk of death by suicide was higher for males than females. On this matter, the findings of previous studies are mixed, with some reporting higher risks for males [2], [13], and some finding no difference [4]. In contrast, the risk of a further non-fatal attempt was higher for females than males. This is consistent with findings from previous follow-up studies [3]. The higher number of female non-fatal suicide attempts and the lower number of female suicide deaths may reflect the tendency for females to use less lethal methods of suicide [11].
Age
During the study period, the risk of death by suicide was lower in youth than adults or older adults. While some studies have found older adults to be at increased risk of death by suicide after a non-fatal suicide attempt [14], others have found no differences between age groups [3], [4]. The failure of some studies to find age differences in the risk of further suicide attempts may reflect insufficient sample size. Because older adults account for only a small proportion of non-fatal suicide attempts, a large sample size would be needed to contain a sufficient number of older adults to detect any differences in the risk of death by suicide between age groups.
The risk of readmission for a further non-fatal suicide attempt was lower in older adults than in adults or youth. This is consistent with previous studies that have found lower risks of further non-fatal suicide attempts in older adults [14].
Adults aged 25–54 were the most at-risk age group, with high risks of both further non-fatal suicide attempts and subsequent death by suicide. Cross-sectional surveys support this finding [15].
Lethality of index attempt
The risk of subsequent suicide was higher in those who used index attempt suicide methods of high lethality, while the risk of readmission for a further non-fatal suicide attempt was higher in those who used index suicide attempt methods of low lethality. This pattern has been observed in other studies [14] and probably reflects the fact that those using index attempt methods of high lethality are likely to continue using these highly lethal methods, and are therefore more likely to die by suicide, and less likely to survive an attempt, than those using less lethal methods.
Rates of readmission for further suicide attempts
Further hospital admissions for attempted suicide were common in the study population. While more than one in four people were readmitted for at least one further suicide attempt, a significant number of people were readmitted for several further attempts, with the maximum number of readmissions being 56.
The overall rate of readmissions per year for attempted suicide over the 10 years study period was 0.23. The highest rate of readmission was during the first 2 years after the index attempt (0.37).
In summary, these trends suggest that those most likely to be readmitted for suicide attempts are female and less than 55 years old, while those most likely to die by suicide are male and aged over 24.
A limitation of this study is that it reports only those further suicide attempts that resulted in admission to Christchurch Hospital. Attempts that did not require hospital admission, or were admitted to another hospital, were not analysed. As a result, the rates of further suicide attempt found in this study underestimate the true rates of further suicidal behaviour. A further limitation is the use of an artificial cohort of people making suicide attempts within a given time period (1993–2002). The analysis of only those admissions occurring within a given time results in the index attempts in the sample being a mixture of first attempts and subsequent attempts. Furthermore, because participants entered the study throughout the entire 10-year period, the lengths of follow-up vary considerably between participants. However, this has been controlled for in the analysis by the use of survival analysis and by adjusting rates in order to reflect the number of people studied at a given time. Despite these limitations, the findings from this study provide useful information about the regional burden of suicide attempt admissions and subsequent risk of readmission and of mortality. These risks are distressingly high and a matter of concern.
Although age, gender and lethality of index suicide attempt are associated with the risk of further suicide attempts and death by suicide, these associations are not strong enough to allow for ready identification of individuals who will make a further attempt or die by suicide [4]. Since a high-risk group within the population of those making suicide attempts cannot be reliably identified, intervention strategies should be targeted at all individuals admitted to hospital for attempted suicide. The risk of further suicide attempts and death by suicide is highest in the first 2 years after an index attempt, suggesting that support and monitoring of those who have made suicide attempts should be concentrated in this period. However, the risk of reattempt remains high 10 years after an index attempt, indicating a concomitant need for longer-term support and management.
The high risk of further suicide attempt amongst those who are hospitalized for an index suicide attempt suggests the need for improved and enhanced assessment, treatment and management of all individuals in this readily identifiable high risk group. There are a number of ways in which the treatment needs of these patients might be met: a series of clinical practice guidelines for managing people at risk of suicide have recently been developed for emergency departments [see, for example, 16,17–20]. However, the extent to which the effective implementation of these guidelines might reduce risks of further suicidal behaviour has yet to be determined. Secondly, there are a series of psychopharmocotherapeutic and psychotherapeutic approaches which appear promising but which require further evaluation. Thirdly, given the well recognized poor attendance rate of the suicide attempt population (between 30% and 60% attend follow-up appointments after suicide attempts [20]) there may be merit in trying to develop intervention strategies which place minimal demands on these patients. There are promising findings from a range of systematic programmes which aim to maintain contact with patients who have made suicide attempts, but are difficult to engage in treatment [see, for example, 21–23]. These promising minimal-cost interventions require further evaluation to determine the extent to which they might be effective in reducing subsequent suicidal behaviour in those who have made an index suicide attempt.
Footnotes
Acknowledgements
We acknowledge funding provided by a Health Research Council of New Zealand Summer Studentship to Sheree Gibb. We thank Kevin Huang (Canterbury District Health Board), Chris Lewis (NZHIS), Jeff Chuter (Department of Courts), and Kirk Newman (New Zealand Police) for their assistance with data collection, and John Horwood (Christchurch Health and Development Study) for statistical advice.