
Abstract
Self-harm is a major public health concern in New Zealand because it is common [1], it is associated with suicide [2] and it has a high overall mortality and morbidity rate [3]. Reducing self-harm attempts is a priority in the New Zealand Health Strategy [4]. Presentations to hospital for self-harm are important, not only because they place a significant burden on health-care resources, but also because a history of intentional self-harm is a strong predictor of future suicidal behaviours [5]. Between one-third and half of people who complete suicide have a history of intentional self-harm [6]. Approximately 1% of people who self-harm will complete suicide over the next year and this increased risk continues for at least the next 10 years [5].
Until recently, New Zealand official data showed that there were >5000 episodes of self-harm presenting to hospital emergency departments with intentional self-harm each year [7]. It was recognized, however, that these data were likely to be an underestimate because of two problems related to data collection. First is the problem of recognition. Intentional self-harm may be recorded by clinical coders as the effect of the harm rather than the action, for example, paracetamol poisoning may be recorded as ‘abdominal pain’. Second is the difficulty of recording what a ‘hospitalization’ is. The rules for this are unclear and differ between different district health boards (DHBs), resulting in inconsistencies and difficulties interpreting the data. For example some DHBs record everyone who presents to hospital, usually the emergency department of a hospital, with intentional self-harm, while others record only those who are subsequently admitted to an inpatient ward. Further, the status of those people admitted to a short stay or observation ward in different DHBs is unclear. A final problem with official figures is that they refer to episodes rather than people, and record only a limited number of variables. The current New Zealand Ministry of Health document Suicide facts: deaths and intentional self-harm hospitalizations 2006 tries to manage these difficulties by restricting the definition of intentional self-harm to episodes in which patients were admitted for intentional self-harm via an emergency department and had a length of stay (either in a medical ward or inpatient mental health unit) of ≥48 h or longer [8]. Using these criteria official figures show that there were 2868 hospitalizations for intentional self-harm in 2006. It is important to have accurate measures of important public health issues such as self-harm to monitor the effect of policy and to make decisions about allocation of resources.
There have been few previous studies describing the epidemiology of self-harm in New Zealand. Those that have been published have restricted themselves to only one DHB [9, 10], or one particular age group [11] or ethnicity [12].
We have recently completed a large multi-centre randomized controlled trial of problem-solving therapy following self-harm in New Zealand. Identifying eligible people for this study has provided us with an opportunity to record in detail everyone who presented with intentional self-harm to the general hospitals of four DHBs. In the current paper we present these data and compare them with official figures.
Methods
Definition of self-harm
Self-harm was defined as intentional self-poisoning or self-injury, irrespective of motivation. Self-poisoning included the intentional ingestion of more than the prescribed amount of any drug, whether or not there was evidence that the act was intended to result in death. This also included poisoning with noningestible substances (e.g. pesticides or carpet cleaner), overdoses of recreational drugs and severe alcohol intoxication, such cases of which the clinical staff considered to be an act of intentional self-harm. Self-injury was defined as any injury that had been intentionally self-inflicted [13]. In practice the people identified for the study were all recognized by clinicians as needing an assessment by a mental health professional, and includes all people who presented to the hospitals regardless of whether they were admitted.
Settings
We collected data on every person who presented for self-harm from four DHBs Waitemata, Counties Manukau, Northland and Capital Coast. Waitemata District Health Board is the largest of New Zealand's 21 DHBs, serving a population of 481 611 (all population figures are from the 2006 census) in the North and West of Auckland. Counties Manukau District Health Board serves a population of 433 086 in South Auckland. This DHB has high numbers of Maori people (17%), Pacific people (21%), Asian people (16%) and a relatively youthful population (25% of the population under 15). One-third of the Counties Manukau population live in areas that are very deprived, (based on the NZ Deprivation Index 2006). Northland District Health Board serves a population of approximately 148 500 in the north of New Zealand. Northland is characterized by a large Maori population (29%), widely dispersed rural communities and a disproportionately high level of socioeconomic deprivation. The Capital and Coast District Health Board provides health services for 266 658 people in the central Wellington area. Between them these four DHBs contain one-third of the population of New Zealand.
In this paper we present data on presentations to Waitemata and Counties Manukau for one calendar year, 2006; for Northland for the 12 months between 1 August 2006 and 31 July 2007; and for Capital and Coast for the year between 6 November 2006 and 5 November 2007.
Identification of cases of intentional self-harm
Research staff identified people presenting with an episode of intentional self-harm using several different computerized and written methods including electronic databases and liaising with the specialist teams responsible for providing psychosocial assessments. They used over-inclusive criteria to be sure that all presentations were identified. At least two different electronic databases and one manual method were used at each site to ensure that all presentations were identified. These are described in more detail for each DHB, as follows.
Waitemata District Health Board
Waitemata has two emergency departments in its area at North Shore and Waitakere Hospitals. During office hours people who presented with self-harm were seen by the Liaison Psychiatry team, out of hours they were seen by the on-call psychiatric registrar. Research therapists identified people presenting to these two sites by looking at the triage descriptions on the emergency department lists available in the electronic patient information management system (PIMS). Once an episode of self-harm had been identified, further investigation of the discharge summary available on the electronic system, called Concerto, was required. If no discharge summary had been completed the research therapists looked at the paper patient file. The research therapist also checked all referrals to the Liaison Psychiatry service within Waitemata DHB. Mental health services within Waitemata use an electronic system call (Health Care Community; HCC) and this system was used to assist with the location of patients following discharge, the circumstances of their self-harm episode and previous contacts with the service.
Counties Manukau District Health Board
People who presented with self-harm were seen by the Liaison Psychiatry service during the day and weekday evenings; outside these times they were seen by the on-call psychiatric registrar. The PIMS and Concerto patient management systems are also used by this DHB, with research therapists identifying patients using the triage description on the electronic emergency department list and matching this with the Concerto discharge summary if available. They also used the written systems kept by the Liaison Psychiatry service.
Northland District Health Board
The emergency departments are located at Whangarei, the main base hospital, with small units at Kaitia, Bay of Islands, and Rawene. In Northland patients who present with self-harm were seen by the crisis team. The research therapist identified those people presenting with intentional self-harm to Whangarei Hospital by visiting the emergency department and scrutinizing the written list maintained by the emergency department staff. This was cross-checked with Alpha, the electronic system used by the Whangarei emergency department, which provides basic information on current and previous admissions. There is also a system for electronic discharge summaries called i:health, and when a discharge summary was available this could be used in conjunction with Alpha and the manual system to clarify reasons for admission. Alpha and i:health could also be used to identify whether people had had previous admissions to the emergency departments. Northland mental health services use a system called Jade to electronically record patient notes. To identify those people presenting to emergency departments in Northland other than Whangarei, any assessments created by staff out of the Whangarei area were examined to see if they involved intentional self-harm presenting to a general hospital.
Capital and Coast District Health Board
This DHB uses a medical applications portal, which includes Concerto, similar to the system used at both Waitemata and Counties Manukau, and IBA. Concerto gives general information on hospital admissions and outpatient appointments, with IBA giving more detail. Clinical Records was another application used to look at notes of previous emergency department admissions and discharge summaries. The research therapist mainly relied on the written systems of the crisis team to identify study participants. The crisis team are required to provide a psychosocial assessment for all self-harm presentations. Information regarding previous history was also gathered from the manual assessment forms.
Data collected
We collected information on age, sex, ethnicity, method of self-harm and past history of self-harm.
Ethics approval
Ethics approval was obtained from the Northern Regional Ethics Committee X and the Multi-region Ethics Committee.
Results
Demographic characteristics
Characteristics of intentional self-harm vs DHB over 12 months
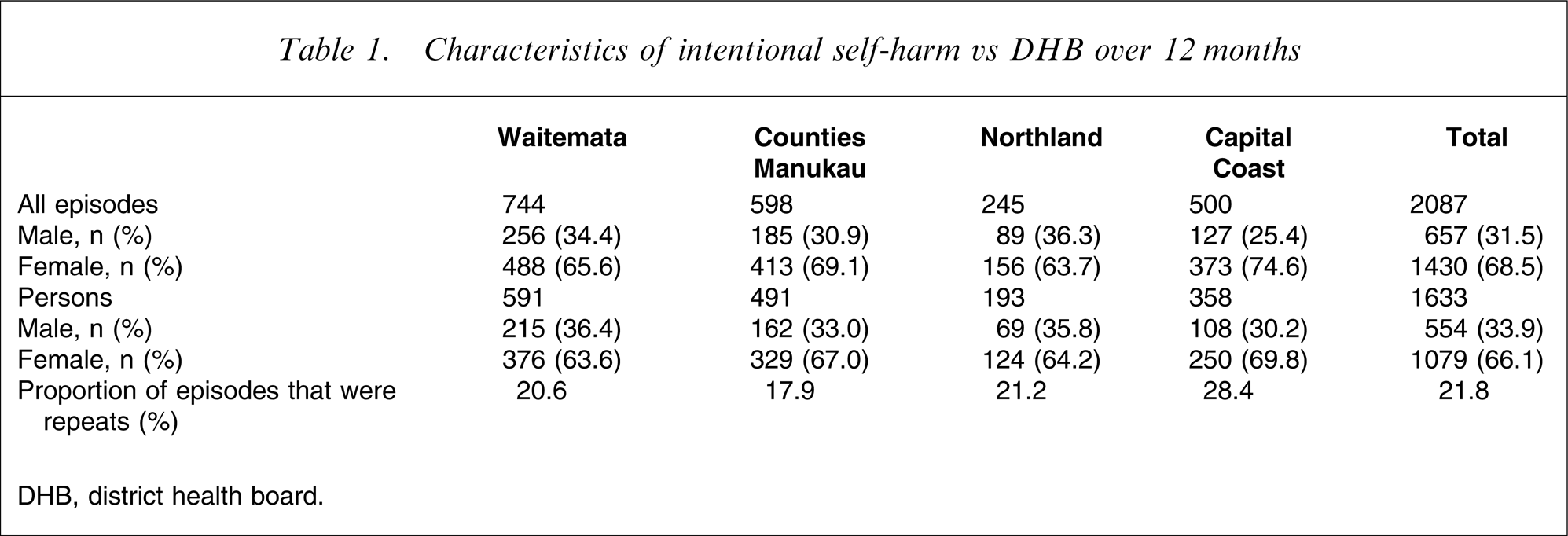
DHB, district health board.
The age range of subjects at the four DHBs was 12–92 years, with a median age of 29. The distribution of patients showed a marked skew towards younger age groups, with 62.7% of the population being under the age of 35 years, although there is some evidence of a bimodal distribution, with the greatest numbers under 20 and a smaller peak in the mid 30s (Figure 1). This is reflected in the distribution of the two sexes, with the largest numbers of female subjects in the 15–19 year age group (276, 25.6% of female subjects), 20–24 year age group (159, 14.7%) and 30–34 year age group (131, 12.1% of total). The largest numbers of male subjects were in the same age brackets: 15–19 year age group (105, 19% of male subjects), 20–24 year age group (80, 14.4%) and 30–34 year age group (70, 12.6%). Those >64 years of age comprised 3.1% (n = 51) of the total.
Age distribution of people presenting with intentional self-harm to four district health boards. (▪) Female; (□) male.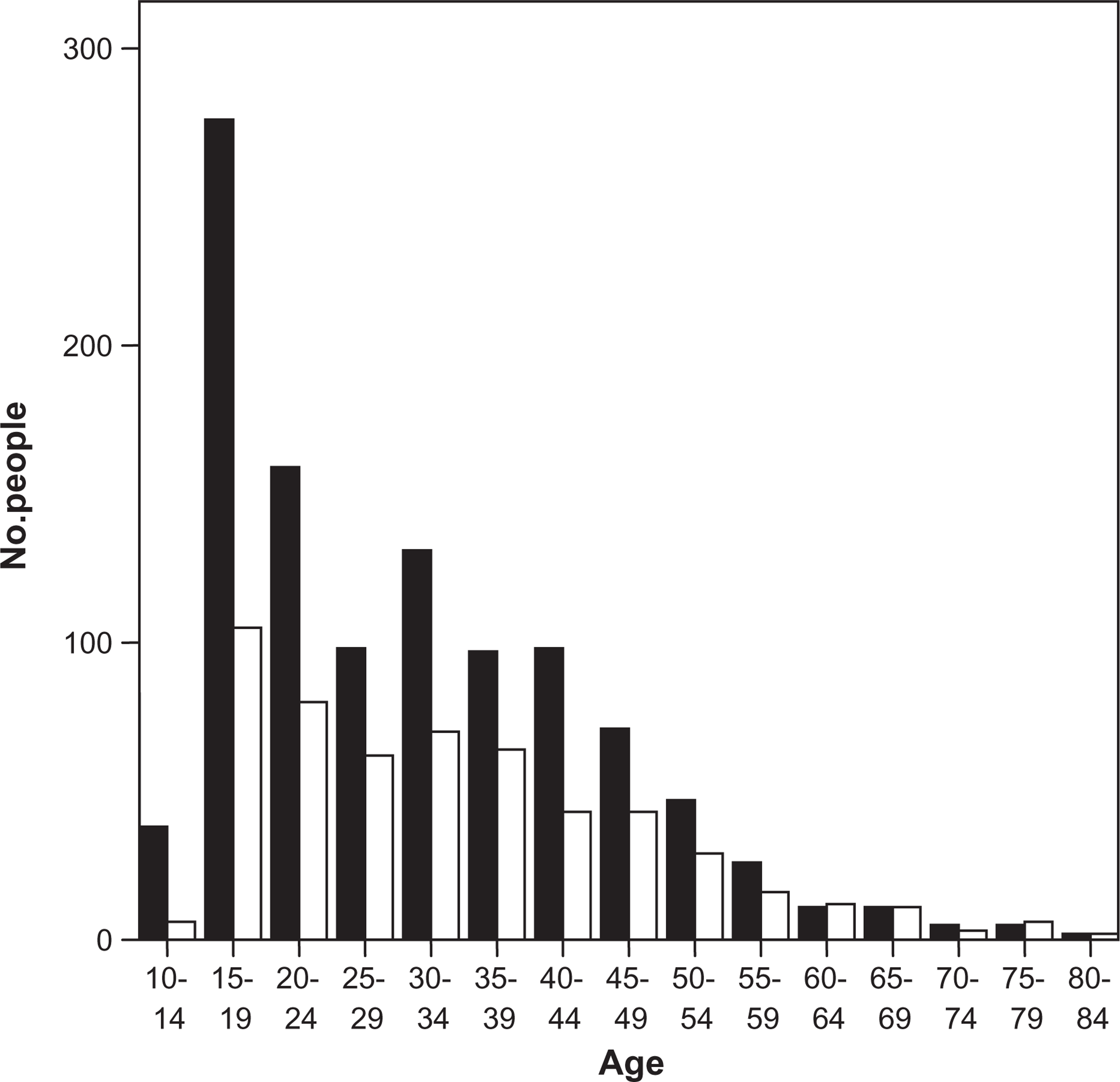
Comparing the different DHBs, people who presented in Northland were significantly younger (median age 27, F = 2.668, df = 3, p = 0.046) with 35.2% of presentations being for patients 20 years old compared to 27.1% in Waitemata (median age 31), 26.8% in Capital Coast (median age 27.5) and 18.5% in Counties Manakau (median age 30).
Intentional self-harm vs ethnicity and DHB according to 2006 census
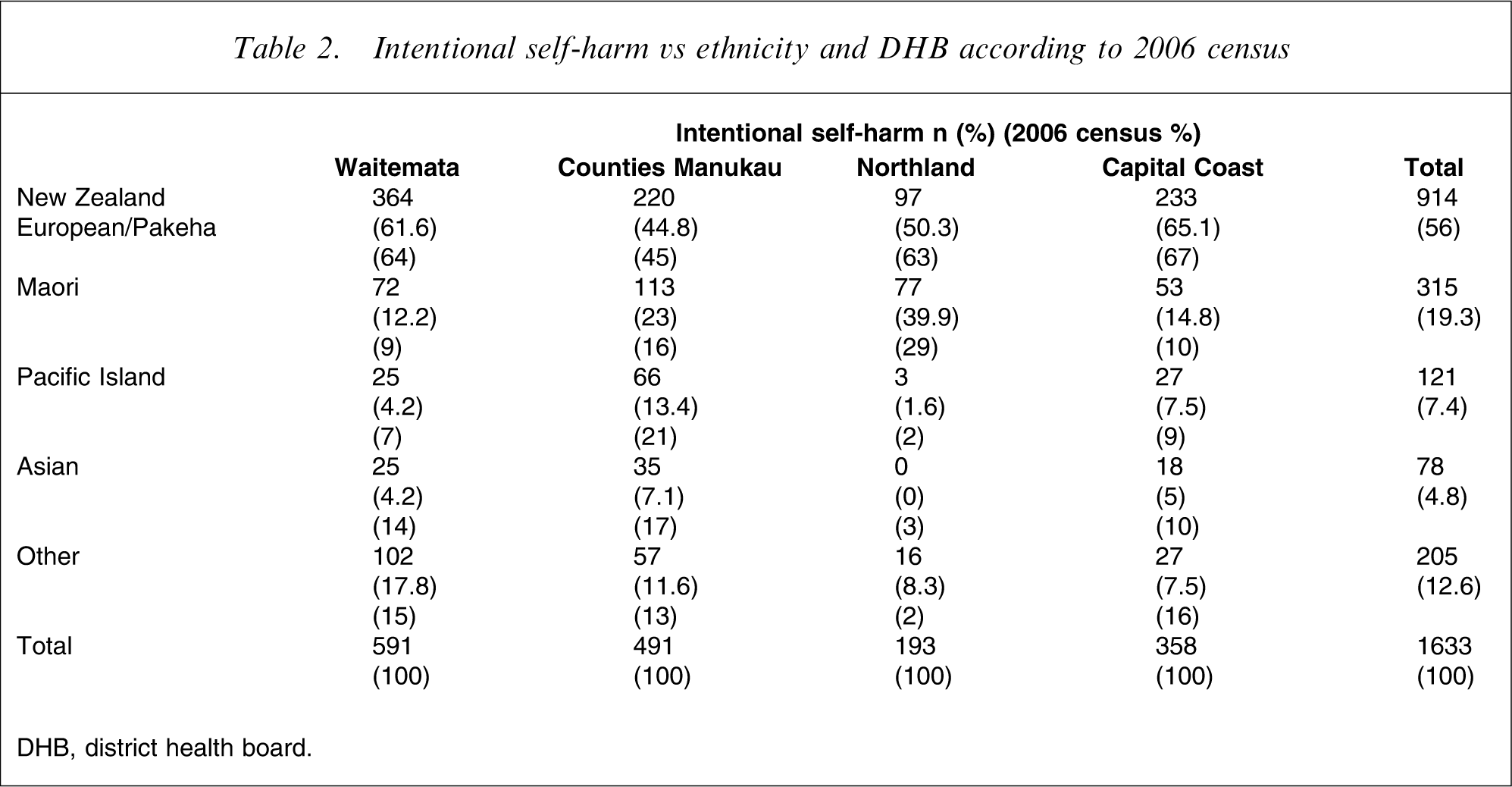
DHB, district health board.
Most NZ European/Pakeha patients were in the 15–19 year age group (210, 23% of NZ European/Pakeha people), the 20–24 year age group (113, 12.4%) and the 30–34 year age group (107, 11.8%). Maori people were most common in the 15–19 year age group (82, 26% of Maori), the 20–24 year age group (42, 13.3%) and the 25–29 year age group (42, 13.3%). Pacific Islanders were most common in the 20–24 year age group (33, 27% of Pacific Islanders), the 15–19 year age group (28, 23%) and 20–29 year age group (18, 14.8%). There were only three people over the age of 65 who identified as Maori who presented to the four DHBs. The median ages of the different ethnicities who presented with intentional self-harm were significantly different (F = 8.921, p = 0.000, df = 4) with Pacific Islanders (median age 23) and Maori people (median age 27) being younger than NZ European/Pakeha (median age 32) and Asian people (median age 27.5).
More than 95% of people who presented received some sort of assessment by a mental health professional. Of those who presented 6.8% were admitted to a psychiatric inpatient unit following their episode of self-harm (Waitemata 8% admitted; Counties Manukau 7.1%, Northland 8.8% and Capital Coast 3.4%).
Most people who presented to hospital with intentional self-harm did so because of an overdose of drugs (n = 1262, 77.3%) followed by self-injury of some sort (generally cutting, carbon monoxide poisoning or hanging; n = 293; 17.9%) and both an overdose and self-injury (n = 77, 4.7%). There were some significant differences between the DHBs, with people being significantly more likely to present to Capital Coast with an overdose (n = 302; 84.6% of presentations to Capital Coast, χ2=13.79, df = 3, p = 0.003) than to Northland (n = 156, 80.8% of presentations), Waitemata (n = 454, 76.9% of presentations) or Counties Manukau (n = 366, 74.5% of presentations). Carbon monoxide poisoning accounted for 2.8% (n = 46) of all presentations to the DHBs while cutting occurred in 17.4% (n = 282) of people and hanging in 4% (n = 66). Comparing method of self-harm between ethnicities, NZ European/Pakeha people were more likely to take an overdose (n = 737, 80.6% of NZ European/Pakeha presentations chi-square = 15.49 p = 0.004) than Maori (n = 238; 75.6% of Maori presentations) or Pacific Islanders (n = 80; 66.1% of Pacific Island presentations). Maori and Pacific Islanders were more likely to present with hanging (Maori n = 28; 8.9% of Maori presentations. Pacific Islanders n = 9; 7.4% of Pacific Island presentations) than NZ European/Pakeha (n = 24, 2.6% of NZ European/Pakeha presentations, χ2=32.715, df = 8, p = 0.00). Half of all cases of self-injury (51.9%) occurred in those under the age of 25.
Most people (n = 974, 59.7%) had no history of previous self-harm attempts. The proportion of people presenting for the first time was not affected by ethnicity, gender or method of self-harm. Nearly one in 10 people (9.2%) had a history of five or more self-harm attempts.
Intentional self-harm per 100 000 age standardized to WHO standard world population vs DHB
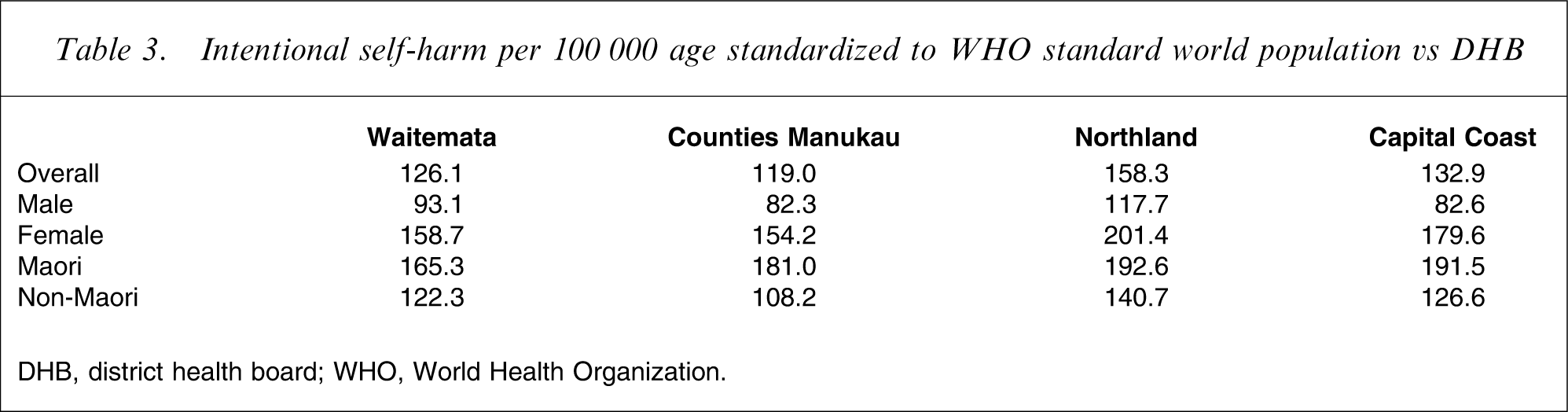
DHB, district health board; WHO, World Health Organization.
Study data vs Ministry of Health figures [7]
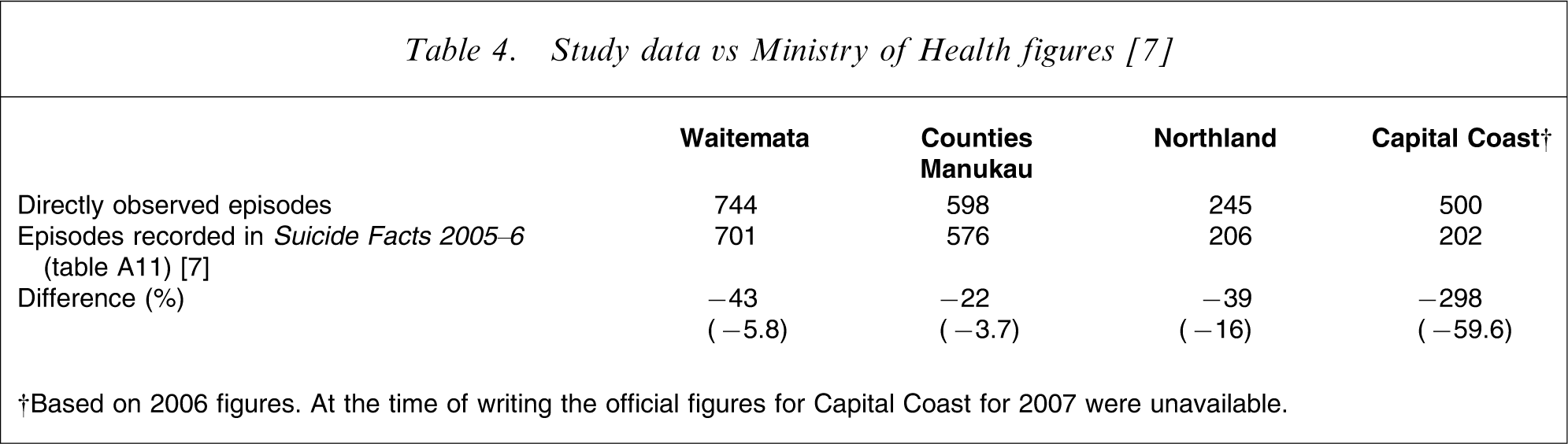
†Based on 2006 figures. At the time of writing the official figures for Capital Coast for 2007 were unavailable.
Discussion
The principal findings of this study are that in these four DHBs approximately 1600 people present a total of 2000 times over 12 months. Extrapolating this to the whole country, this means that the number of episodes of self-harm nationally is approximately 6200 per year involving 4900 people. The highest rates were in Northland, young women and Maori people. Official figures from the Ministry of Health substantially underestimate the size of the problem. From Te Rau Hinengaro: the New Zealand Mental Health Survey we know that approximately 0.4% of the population make a suicide attempt over 1 year, that is approximately 16 000 people. It seems that less than one-third of them present to hospitals.
The strength of the study is that it was done within emergency departments using a variety of methods within each DHB to ensure that people who presented with intentional self-harm were not missed. Using this method we were able to describe both episodes and people presenting with intentional self-harm. The official figures describe only episodes and provide no information on individuals. The figures collected in this paper are the first time that this information is available for a large proportion of the New Zealand population. The weakness is that despite efforts to identify everyone who presented, we may still have missed some people, which will lead to an underestimate of the size of the problem.
It is hard to know whether self-harm is changing in frequency. According to official figures it is declining but this is based on a narrow definition, flawed data collection and episodes only. A previous study that looked at self-harm presentations to Waitemata in 2001–2002 found 452 people presented 633 times over 1 year [9]. The current study found that these numbers had increased in Waitemata by 31% and 18% respectively over 4 years. It is unlikely that this magnitude of increase will have been accounted for by population changes alone, and this change is consistent with an older study that noted an increase in admissions for attempted suicide at Christchurch Hospital over 10 years [10].
The present study overcomes the weaknesses of previous studies by counting both people and episodes of intentional self-harm. It is recognized by the Ministry of Health that there is a difficulty with the collection of official data on intentional self-harm. Langley et al. have criticized the analysis of trends in the official figures by examining secondary data and different definitions of intentional self-harm [15]. The current study is the first that has used direct observation of admissions for self-harm in a large proportion of the New Zealand population to provide accurate data on the size of the problem. This paper also gives some idea of the magnitude of the underestimate of the size of the problem, but it also demonstrates that it is possible to accurately count the number of people who present to hospital with intentional self-harm.
There are two ways to address the problem of underestimating the number of people who present to hospitals with intentional self-harm. The first is to improve routine data collection and reporting on intentional self-harm from the DHBs. Attempts to address this problem in the past, however, have been unsuccessful. The other way is to set up monitoring sites in a few representative DHBs to accurately count and describe intentional self-harm presentations. This approach is the one that has been adopted overseas [13] and is one we would recommend. Without this it is impossible to know whether one of the key goals of the New Zealand health strategy is being met.
Footnotes
Acknowledgements
The study was funded by the Accident Compensation Corporation of New Zealand. We would like to thank the staff in the different DHBs for their cooperation in obtaining the data.