
Abstract
A number of studies has examined mortality among those individuals who make suicide attempts. A recent systematic review of 26 such studies has suggested that those who make suicide attempts have a 0.5% to 2% risk of suicide within 1 year of their suicide attempt, and a suicide risk in excess of 5% after 9 years [1].
In addition to elevated rates of suicide, a series of studies has shown that those who make suicide attempts also have higher rates of death from other causes including accidents, homicide and disease [2–5]. For example, Ostama and Lonnqvist followed up, for a mean of 5.3 years, 2782 patients aged 15 years and older who had been admitted to emergency rooms in Helsinki following suicide attempts. Mortality from all causes was 15 times higher than expected in males, and nine times higher in females; mortality from accidents was 29 times higher than expected in males and 21 times higher in females; mortality from homicide was 28 times higher in males; and mortality from disease was six times higher in males and four times higher in females.
However, among the studies examining mortality following suicide attempts, few have examined mortality in those who make medically serious suicide attempts. The population of those who make medically serious suicide attempts might be expected to be at higher risk of further suicidal behaviour and mortality by suicide, than those who make less serious attempts, and would seem to provide a readily identifiable group upon which to focus efforts to prevent both further suicide attempts and mortality.
Against this background, the aims of this analysis are to examine rates of mortality, from suicide and other causes, in a consecutive sample of 302 individuals who made medically serious suicide attempts and who were followed-up for 5 years after these attempts.
Method
Participants
Participants were a consecutive series of 302 individuals aged 13–88 years (inclusive) who made medically serious suicide attempts from 1 September, 1991 to 31 May, 1994 in Christchurch (New Zealand), a mixed urban/rural region with a population of 430 000. This group has served as a case series in a multiple group case control study of suicide and serious suicide attempts, and their characteristics have been described previously [6, 7].
Medically serious suicide attempts were defined as those that required hospital admission for at least 24 h, via the sole regional emergency department (ED) at Christchurch Hospital, and met one of the following treatment criteria: (i) treatment in specialized units (intensive care unit; hyperbaric unit; burns unit); (ii) surgery under general anaesthesia (superficial cuts that did not require surgical repair were excluded); and (iii) extensive medical treatment (beyond gastric lavage, activated charcoal, or routine neurological observations) including antidotes for drug overdoses, telemetry or repeated tests or investigations.
In addition, we included individuals who attempted suicide by methods with a high risk of fatality (specifically, hanging or gunshot) who were hospitalized for <24 h but did not meet the preceding treatment criteria.
Cases were identified by daily calls to the ED, psychiatric emergency service, and relevant admitting wards. Independent communication with all locations provided a daily triple-check to ensure identification of eligible cases. Individuals who met the criteria for inclusion in the study were interviewed when medical and psychiatric staff considered it appropriate for them to be seen. Most interviews were conducted within the hospitals, but a small number were conducted in participants’ homes or in the psychiatric hospital to which some patients were transferred immediately after treatment for the physical sequelae of their suicide attempt. Each participant was interviewed as soon as practicable after their suicide attempt in order to minimize possible intervention of various factors, including contact with family or friends and commencement of psychiatric treatment.
Individuals who made more than one attempt during the study period were interviewed for the initial attempt only.
In total, 317 individuals made serious suicide attempts during the study period. Of these, 302 agreed to participate in the study, giving a response rate of 95.3%.
Measures
All subjects were studied with personal interviews conducted immediately after their index medically serious suicide attempt.
Demographic results
From interview data the following factors were available to describe the demographic characteristics of the sample at baseline: age; gender; and method of serious suicide attempt at baseline.
Mortality
The New Zealand Health Information Service (NZHIS) maintains a mortality database that holds all national death certificate details. This database was checked for each participant for the period from the date of his or her index suicide attempt to 5 years after this attempt. For participants who died, date and cause of death were established from this database. For those who died by suicide or accident, coronial inquiries had been held, and coronial records were reviewed. Method of suicide was obtained from the coronial records.
Estimation of mortality in the general population
As part of the analysis, rates of suicide were compared with expected rates from an age- and gender-matched sample. These expected rates were estimated from national mortality data for the period 1994–1998. These data were provided by NZHIS. From this information, in conjunction with population estimates subdivided by age and gender [8], it was possible to construct life-table estimates of the probability of mortality for a random sample from the general population having the same age and gender distribution as the study population. Separate estimates were produced for total mortality (from all causes), mortality attributable to suicide, mortality attributable to motor vehicle accidents, and mortality attributable to all other causes.
Results
Demographic results
The sample of subjects who made medically serious suicide attempts consisted of almost equal numbers of men (n = 140, 46.4%) and women (n = 162, 53.6%). The mean age of these subjects, at the time of their index suicide attempt, was 30.4 years (SD = 14.2) (male: mean = 30.7 years, SD = 14.8; female: mean = 29.9 years, SD = 13.4). The majority of index medically serious suicide attempts involved overdose or poisoning (n = 237, 78.5%), with other methods including carbon monoxide poisoning (n = 27, 8.9%), cutting by sharp instrument or stabbing (n = 19, 6.3%), hanging (n = 9, 3%), and gunshot (n = 4, 1.3%). The prevalence and comorbidity of mental disorders in this sample have been previously described [6].
Five year mortality following serious suicide attempt
Table 1 shows sources of mortality during the 5 years subsequent to medically serious suicide attempts for males, females and the total sample. The table also reports the percentage rates of mortality for men, women and the total sample. During the 5 year follow-up period a total of 27 participants died, representing a total mortality rate of 8.9%. Although more women than men died by suicide (11 female; 5 male) the rates of mortality for men and women were almost equal (male = 8.57%; female = 9.25%) owing to the larger number of women in the sample. Of the 27 deaths, the majority (59%) received coroner's verdicts of suicide. Other sources of death were single motor vehicle accidents (15% of all deaths), and disease (22%). One subject died by homicide. The pattern of mortality appeared to be similar for men and women although there was a trend for women to more often die by suicide and less often by motor vehicle accident.
Causes and rates of death and ages (at the index attempt) among 302 individuals making serious suicide attempts, followed for 5 years
The mean ages (at the time of the index suicide attempt) of the subjects who died by suicide (31.5 years), motor vehicle accidents (26.5 years) and homicide (29 years) were similar. By contrast, the six subjects who died from disease were much older (mean age at the index attempt, 74 years). The age difference between those who died by disease and those who died from other causes was significant (p < 0. 0001).
Among those 16 participants who died by suicide during the followup period, nine (56.25%) died by vehicle exhaust gas, five (31.3%) by hanging, and two (12.5%) by overdose or poisoning. For the majority (75%) of those who died by suicide, this represented a change from the method used for the index non-fatal attempt (predominantly, overdose or poisoning) to a method of higher lethality (vehicle exhaust gas or hanging) for the subsequent attempt that resulted in their deaths.
Figure 1 shows life-table estimates of the risk of mortality during the 5 years following a serious suicide attempt, for both deaths by suicide and deaths from all causes. The majority of deaths (62.5% of suicides; 59.3% of deaths from all causes) occurred within 18 months of the medically serious suicide attempt. However, deaths, both from suicide and all causes, continued to occur throughout the 5 year follow-up period, with one suicide occurring 59 months after the index suicide attempt.
Cumulative life-table estimates (%) of the probability of: (a) mortality by suicide; (b) mortality from all causes, during the 5 year follow-up period (n = 302).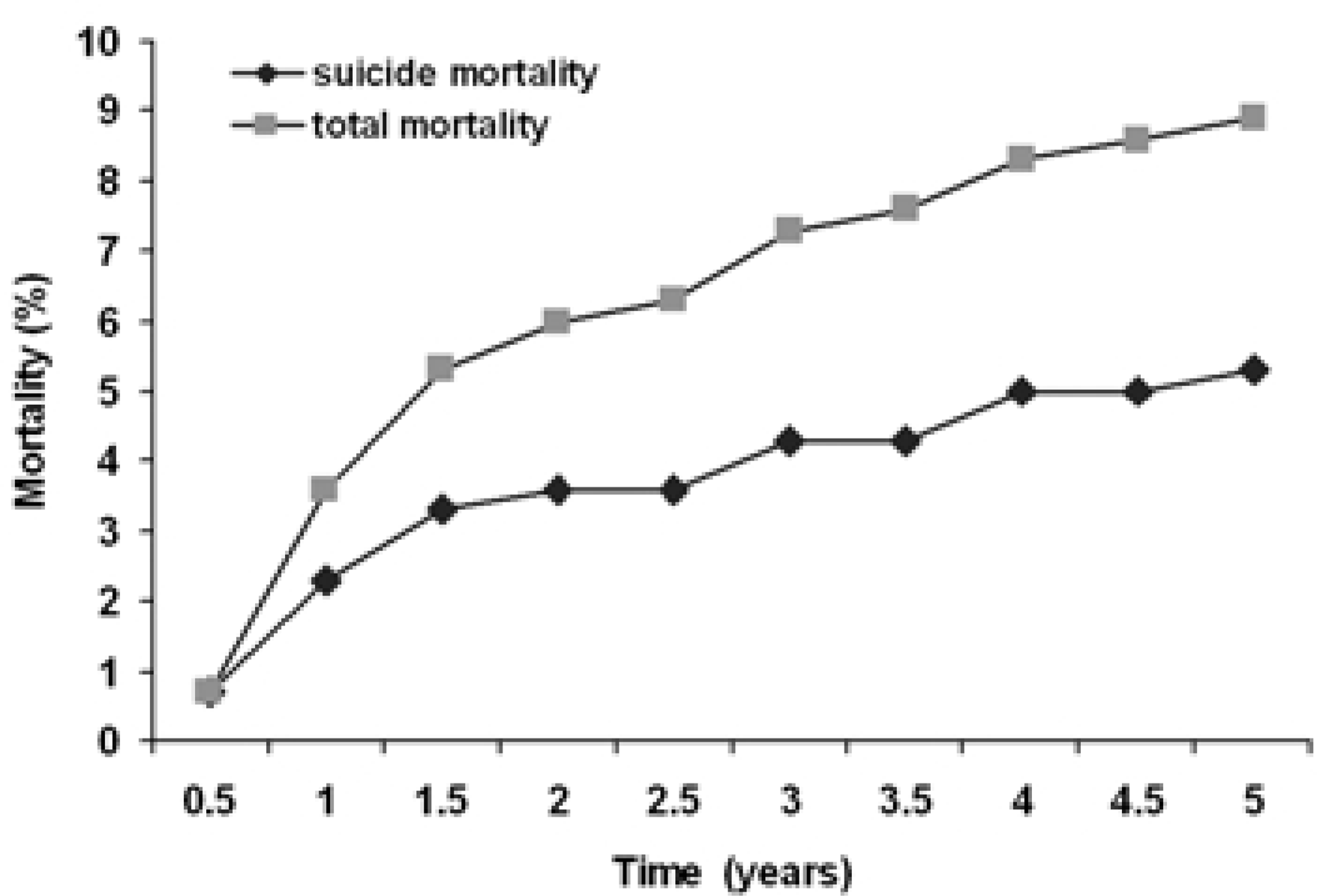
Excess mortality following serious suicide attempt
Table 2 compares the number of deaths in the study population with the number expected from an age- and gender-comparable sample from the general population. These estimates are subdivided by the source of mortality (suicide, motor vehicle accidents, other causes). The table also reports the results of a χ 2 one-sample test comparing the observed and expected deaths for each comparison.
Mortality in 5 year follow-up of medically serious suicide attempters (n = 302):observed and expected deaths
This table shows, firstly, that rates of suicide were 48 times higher than expected. Secondly, rates of mortality from motor vehicle accidents were 11.5 times higher than expected. Rates of mortality from all other causes were not significantly different from expected rates. Total rates of mortality were five times higher than expected.
From the table it is possible to estimate the contributions of various sources of death to the excess mortality (21.3 deaths). This analysis shows that of the 21.3 excess deaths 15.6 (75.2%) were accounted for by suicide. A further 3.6 excess deaths (18.8%) were accounted for by motor vehicle accidents. There was only a small excess of deaths from other causes (1.96, 6%).
Discussion
This research confirms the findings of previous studies which have shown that those making suicide attempts are an at-risk population for excess mortality, from both suicide and other causes [1, 4]. In this series just under 10% of those making medically serious suicide attempts died within 5 years of the attempt with rates of mortality in this series being over five times higher than would be expected in a comparable age- and gender-matched sample in the general population. The principal sources of excess mortality were suicide and motor vehicle accidents.
Suicide accounted for nearly three-quarters of the excess mortality, with motor vehicle accidents accounting for most of the remainder (17.2%). Rates of mortality from other causes were only marginally higher than are expected in a general population sample.
These findings are consistent with many previous studies which have found elevated rates of mortality due to suicide among those making suicide attempts [3, 4, 9–17]. However, the rate of suicide in this series (5.3%) is somewhat higher than has been typically reported. In a recent review of deaths by suicide following suicide attempts Owens et al. [1] suggested that after 4–9 years follow-up, an average of 3.4% of suicide attempters died by suicide. It seems likely that the high suicide rate in this series is accounted for by the fact that the sample consisted of people who had made medically serious suicide attempts.
The elevated rate of motor vehicle accidents in this series suggests that a number of these accidents may have been suicides that were recorded in coronial records as motor vehicle accidents. As other authors have noted, it is likely that official suicide statistics are biased downwards as a result of suicide by motor vehicle crash being classified as motor vehicle accidents [18–20]. If the four single-vehicle accident deaths that occurred in this study were included as suicides, these results would suggest an upper limit estimate of mortality from suicide in this series of 6.6% within 5 years of a serious suicide attempt.
In this series, almost equal numbers of men and women made medically serious suicide attempts. This is notable since, in most developed countries, there is usually a clear female excess among those making suicide attempts and a clear male excess in suicide deaths. The almost equal gender ratio in the present study probably reflects the fact that this was a selected sample of serious suicide attempts with severe medical consequences.
Overall, a greater number of women died in the follow-up period than men. In part, this was due to the slightly larger number of women in the sample of those making suicide attempts. When these gender differences in sample size were taken into account the rate of mortality for men and women was very similar. In addition there was a trend for women to more often die by suicide (11 of 15 female deaths) than men (five of 11 deaths). These results may reflect the fact that more men than women died by traffic accidents which, as noted above, could have been suicide deaths. When the combined numbers of deaths by suicide and traffic accidents are considered, the rates of mortality were similar for men and women.
An implication of these findings is that, for this sample of people making medically serious suicide attempts, rates of suicide and suspected/possible suicides in the follow-up period were similar for men and women. This finding suggests there are features of the population of those who make serious suicide attempts which mitigate the typical male excess observed in suicide mortality in Western societies. It seems likely that the sample making medically serious suicide attempts includes those with higher suicidal intent. This sample may include women who adopt more lethal methods with successive suicide attempts. It may also include fewer men since those with higher suicidal intent may have used more lethal methods at the index attempt, resulting in their death. The net effects of these opposing tendencies may have been to produce, for this sample, a situation in which men and women were equally vulnerable to medically serious suicide attempt and suicide mortality.
This speculation is supported by comparison of the methods used by participants for the index medically serious suicide attempt and the subsequent attempt that resulted in their suicide deaths. The majority of participants who died by suicide changed their method of suicide attempt from that used for the non-fatal index attempt. Of the 16 suicide cases, 11 made their medically serious suicide attempt by overdose or poisoning but only two subsequently died by this method. The remaining nine who used overdose at the index attempt used a method of higher lethality (vehicle exhaust gas or hanging) for the subsequent attempt that resulted in their deaths. This observation suggests that patients may learn about lethality from their failed attempts and those with high suicidal intent will change to a more lethal method.
The clinical implications of these findings relate to the high mortality in this series due to suicide or probable suicide. These findings suggest the need for adequate support and aftercare to be provided to all those who make medically serious suicide attempts to mitigate risks of further suicidal behaviour. It seems likely that this care will need to be provided to all those making medically serious suicide attempts, rather than being targeted to some portion. In particular, a companion paper has examined the extent to which those making serious suicide attempts and dying by suicide could be predicted from information collected at around the time of the suicide attempt [21]. In keeping with previous studies, this paper suggested only very modest prediction of further suicidal behaviour was possible.
It is clear that attempts to predict those suicide attempters who will eventually die by suicide is not practicable owing to the relatively low base rate of suicide. This conclusion suggests the need for intervention strategies in this area to be population-based by providing treatment, support, improved surveillance and assistance to those making suicide attempts. The results of this paper suggest that this support may need to occur over a protracted time since the suicide rate for suicide attempters remained high beyond the first year following an index serious suicide attempt.
These considerations may suggest a need to shift the emphasis in the care of suicidal patients away from short-term crisis intervention to longer-term management and surveillance. This trend is consistent with recent views on the management of other psychiatric illnesses such as depression.
Further papers from this study will examine other aspects of adjustment following serious suicide attempts including psychosocial adjustment, psychiatric morbidity, mental health treatment, and the relationships of these events to further suicidality.