
Abstract
Objectives:
Despite substantial investment by governments, the prevalence of mental health disorders in developed countries remains unchanged over the past 20 years. As 50% of mental health conditions present before 14 years of age, access to high-quality mental health care for children is crucial. Barriers to access identified by parents include high costs and long wait times, difficulty navigating the health system, and a lack of recognition of the existence and/or severity of the child’s mental health disorder. Often neglected, but equally important, are clinician views about the barriers to and enablers of access to high-quality mental health care. We aimed to determine perspectives of Australian clinicians including child and adolescent psychiatrists, paediatricians, psychologists and general practitioners, on barriers and enablers within the current system and components of an optimal system.
Methods:
A total of 143 clinicians (approximately 35 each of child and adolescent psychiatrists, paediatricians, child psychologists and general practitioners) from Victoria and South Australia participated in semi-structured phone interviews between March 2018 and February 2019. Inductive content analysis was applied to address the broad study aims.
Findings:
Clinician-identified barriers included multi-dimensional family factors, service fragmentation, long wait times and inadequate training for paediatricians and general practitioners. Rural and regional locations provided additional challenges but a greater sense of collaboration resulting from the proximity of clinicians in rural areas, creating an opportunity to develop support networks. Suggestions for an optimal system included novel ways to improve access to child psychiatry expertise, training for paediatricians and general practitioners, and co-located multidisciplinary services.
Conclusion:
Within the current mental health system for children, structural, training and workforce barriers prevent optimal access to care. Clinicians identified many practical and systemic ideas to improve the system. Implementation and evaluation of effectiveness and cost effectiveness of these ideas is the next challenge for Australia’s children’s mental health.
Introduction
Mental health disorders are a leading contributor to the global burden of disease (Vos et al., 2020). Despite increased recognition and investment by governments in treatment, the prevalence of mental health disorders in developed countries remains unchanged over the past 20 years (Jorm et al., 2017). Fifty percent of mental health disorders begin before the age of 14 years (Kessler et al., 2005). Left untreated, they can have lifelong personal and societal impacts (Bor and Bor, 2001; Bosquet and Egeland, 2006). Thus, it is crucial to ensure that children with mental health problems can readily access high-quality mental health care.
The second Australian national Child and Adolescent Survey of Mental Health and Wellbeing (known as Young Minds Matter [YMM]) reported that approximately 14% of Australian children aged 4–17 years experienced a mental health disorder within a 12-month period (Lawrence et al., 2016). The most common diagnoses were attention-deficit hyperactivity disorder (ADHD, affecting 7.8%), followed by anxiety (6.9%). Only 50% of those with a mental health disorder had received services in the previous 12 months (Johnson et al., 2016). However, among these children, few receive a sufficient dose of care that would be likely to improve their symptoms (Mulraney et al., 2020; Sawyer et al., 2019).
A nuanced understanding of barriers and enablers to service access is needed to inform the development of policies and practices that will increase access and ensure that children who do attend services receive the right treatment at the right dose. Several studies have identified barriers to care consistently reported by parents. The most commonly reported barriers include high costs and long wait times, difficulty navigating the health system, a concern with being blamed for their child’s problems, and a lack of recognition of the existence and/or severity of the child’s mental health disorder (Lawrence et al., 2016; Reardon et al., 2017; Sawyer et al., 2000). Often neglected, but equally important, is understanding clinician views about the barriers to and enablers of access to high-quality care. We could find only one study (conducted by our group, Paton and Hiscock, 2019) of Australian clinician perspectives, but this study focused on autism and ADHD and did not include the views of general practitioners (GPs). In Australia, the majority of child and adolescent mental health care is provided by GPs, psychologists, paediatricians and psychiatrists (Johnson et al., 2016). As such we aimed to expand previous research by investigating the perspectives of Australian GPs, psychologists, paediatricians and psychiatrists on:
The barriers to access and optimal care within the current health system for children and adolescents with ADHD and anxiety;
Components of an optimal system.
We chose to focus on mild to moderate mental health problems (the ‘missing middle’; Rosenberg, 2015; Victorian Government, 2019) as these are more common than severe problems and lack of timely care may lead to deterioration in the problem.
Methods
This qualitative study was nested within a larger study ‘Towards an equitable mental health system for children in Australia’ (NHMRC grant 1129957), which investigated current use of mental health care by Australian children and adolescents and how best to improve care. The qualitative methodology for this project was based on interpretative description which aims to generate an understanding of complex clinical phenomena which can lead to applied outcomes in real-world circumstances (Thorne, 2016; Thorne et al., 1997).
Approval was received from Human Research Ethics Committee at The Royal Children’s Hospital, Melbourne, Victoria, Australia, (HREC37105) prior to commencement of the project. Prior to interviews, participants were informed that their participation was voluntary and unpaid. Verbal informed consent was sought.
Recruitment
A purposive sampling strategy was used to recruit clinicians in two states of Australia (Victoria and South Australia) spanning clinicians across low and high socioeconomic settings (based on socioeconomic index for advantage [SEIFA] of clinician practice postcode), major city and regional areas and public and private work settings.
Participants were sourced via three key strategies: websites linked to professional organisations, e.g., find a Psychiatrist (The Royal Australian and New Zealand College of Psychiatrists, 2020); key informants (Marshall, 1996) from within professional networks of the clinicians; and Internet searches of the first five pages on Google.
Where recruitment strategies generated lists larger than 20 clinicians for each group, a statistician not associated with the project assigned a random number to each clinician and the clinicians were contacted in order of the numerical number assigned.
Procedures
A total of 143 (of 270 specialists and 165 GPs contacted) semi-structured phone interviews were conducted with clinicians (35 child and adolescent psychiatrists, 37 child psychologists, 35 paediatricians and 36 GPs) from Victoria and South Australia between March 2018 and February 2019.
Participants were provided with one of two alternately allocated vignettes: either a child experiencing symptoms of ADHD or a child with symptoms of anxiety (see Supplemental Material) prior to the interview, to orientate them to the population of interest. Interviews lasted approximately 45 minutes. A semi-structured interview guide was used to ensure the key questions were covered, but also allowed participants to discuss what was important to them.
Detailed field notes were kept of all interviews. Reflexivity was maintained by ongoing discussions between researchers and a reflexivity journal. Interviews were audio recorded and transcribed verbatim. Transcripts were validated, de-identified and participants assigned pseudonyms. Transcripts were then coded for analysis using NVIVO 12.0 (NVivo, 2017) software.
Analyses
The study research aims provided the broad focus for analysis but following coding more ‘interpretive’ constructs were developed using an inductive approach (Elo and Kyngäs, 2008).
Three researchers (K.P., H.W. and S.R.) developed the initial coding schema which was reviewed by senior researchers (L.G. and H.H.) and applied to all transcripts. Categories were developed in line with the primary research questions and themes were identified using the processes of content analysis. Regular discussion between members of the research team ensured a rigorous process of qualitative coding to identify similarities and differences, enabled iterative development and validation of emergent themes. The lead analyst was a female Master of Public Health (K.P.) with no clinical training. K.P. completed analysis until data saturation was achieved in relation to the research question. A further eight transcripts were then reviewed for each clinician type. Findings are reported in line with the COnsolidated criteria for REporting Qualitative research (COREQ) (Tong et al., 2007) checklist.
Results
Demographics
Characteristics of participating clinicians are shown in Table 1. There was a spread of clinician types across practice and socioeconomic settings. More respondents practised in metropolitan than rural/remote areas and more psychologists practised in private than public settings, likely reflecting workforce distributions.
Clinician characteristics by Victoria (VIC) and South Australia (SA).
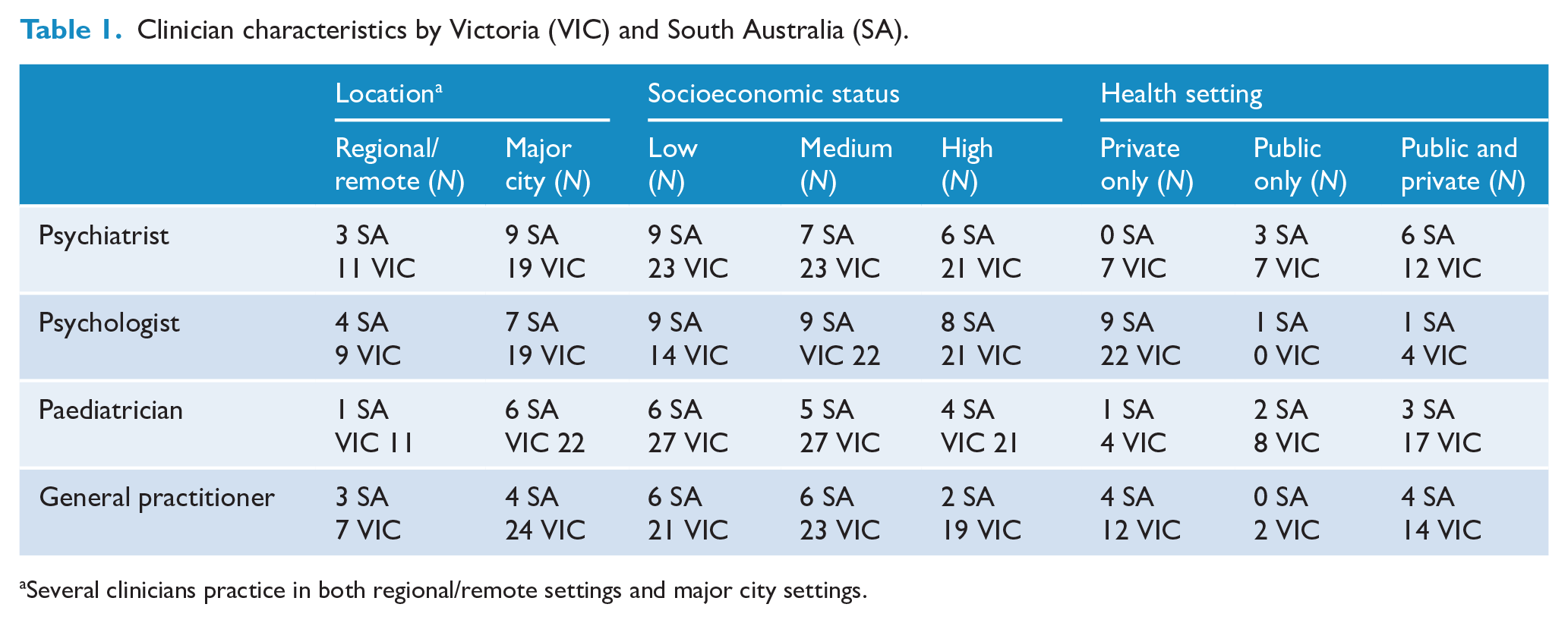
Several clinicians practice in both regional/remote settings and major city settings.
Findings
Analysis of the interview transcripts from a broad range of participants revealed important themes which are presented using verbatim quotes.
Some quotes have been truncated for space reasons without changing the meaning. This is represented by an ellipsis (...).
The overall study identified five overarching key themes. In this paper, we provide a summary of findings from one key theme: health sector challenges and components of an optimal system for child and adolescent mental health care. Other key themes included health system funding models (with some overlap of the findings in this paper); an evidence-based role for the education sector; role of emotion and perceptions about mental health; and supporting parents to support their child.
Clinician reports describing system barriers to access and optimal care
All clinician groups raised issues about access to services. Access to services is restricted by degree of severity and complexity of the condition, age ranges for specific services, fragmentation of services with no roadmap to navigate, out-of-pocket costs and lengthy waiting times.
Clinicians identified multi-dimensional interrelated individual and family factors which influence access to services, including severity and complexity of the condition, geographic location of services, age of the child/adolescent, parental factors (e.g. health literacy, mental health, capacity to pay) and individual personal circumstances such as employment status.
At the extreme ends, i.e., when a child had conditions sufficiently complex and severe to have access to publicly funded child and adolescent mental health services (CAMHS) or when families had a high degree of health literacy and were able to pay for services, services were relatively easier to access.
The term the ‘missing middle’ was used to describe those that fell outside these two extremes and described a very large group of families, children and adolescents.
The CAMHS model was identified as positive, in terms of many practitioners in one setting but clinicians also suggested that public mental health services (and specifically CAMHS) have strict criteria for accepting a referral through their intake processes and their capacity covers only a small proportion of the need.
Although long waiting times were perceived to be more likely to occur in public settings, clinicians perceived that private services also had long waiting lists in all professions. This was reflected as impacting both referral to other service providers and waiting times for clinicians’ own practices. This varied according to location and was reported to be worse in rural and low socioeconomic areas where provision of specialist services is limited.
Furthermore, clinicians identified that the need to travel long distances was challenging for families.
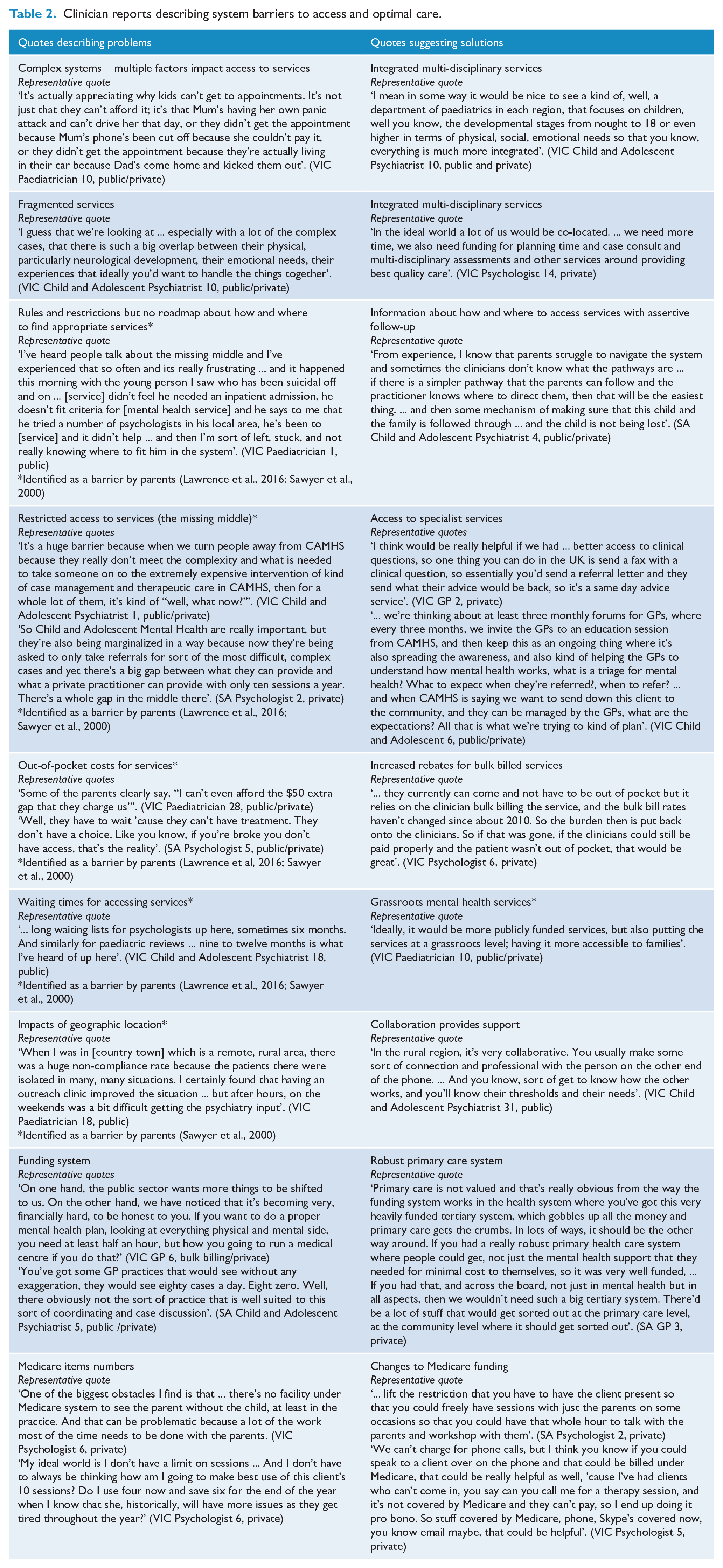
However, a greater sense of community and collaboration resulting from the proximity of clinicians in rural areas provides an opportunity to develop support networks. This was perceived to provide a mechanism for closer liaison and more coordinated care than that experienced by their metropolitan peers. Table 2 provides a detailed summary of system issues and solutions.
Clinician reports describing system barriers to access and optimal care.
Clinician reports describing workforce barriers to access and solutions towards optimal care
Limited numbers of child and adolescent psychiatrists was identified as an issue by all clinician groups including child and adolescent psychiatrists themselves. GPs and paediatricians feel they can manage some mental health conditions but expressed a desire for more support from child and adolescent psychiatrists for more complex cases. Psychiatrists see one of their roles as consultants and advisors to other professions.
A more general shortage of trained professionals for younger (<12 years) children was seen across the sample.
Publicly funded psychologists were recognised as a particularly scarce resource by all clinician groups. Combined with lengthy waiting lists this led to clinician burnout, particularly in regional areas. Clinicians expressed the view that in some cases employment contracts were short term and this led to high turnover in staff. In addition, the workload in regional areas also had an impact on recruiting new staff.
Many clinicians identified that the system of care is top heavy with a focus on specialist medical staff when some first-line mental health care management could be undertaken by other professions, provided they were trained in mental health.
Variability in the quality of services provided both at the individual clinician level and organisational level was identified.
GPs are typically considered to be generalists. Clinicians suggested that opportunities for GPs to specialise in mental health services could be valuable; however, some GPs did not have an interest in paediatrics and/or mental health and others felt they did not have the skills to treat mental health conditions.
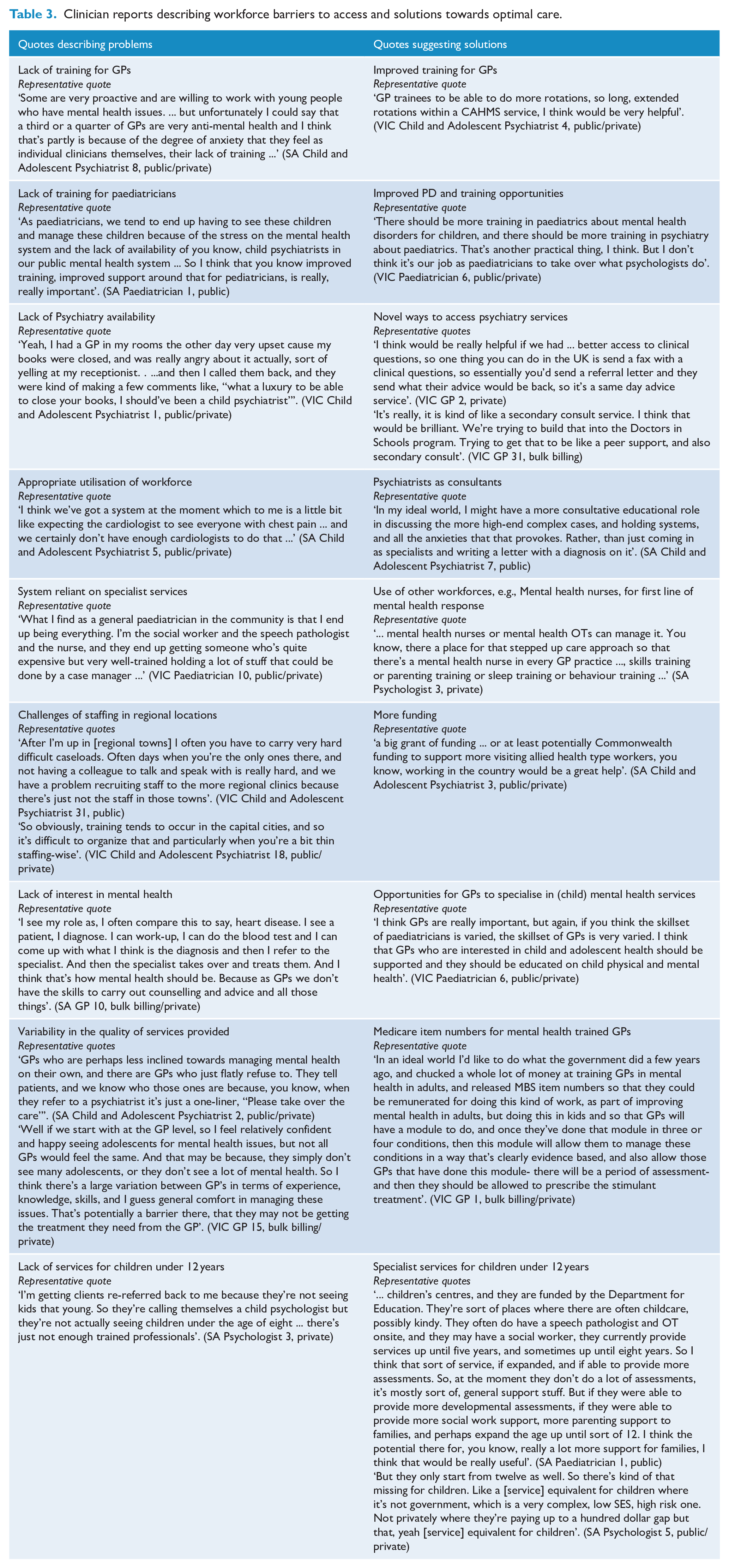
Within all clinician groups, appropriate training and professional development was identified as a challenge particularly for those in regional areas. Table 3 provides a summary of clinician identified workforce challenges and possible solutions.
Clinician reports describing workforce barriers to access and solutions towards optimal care.
Clinician reports describing the challenges of working together to improve outcomes
All clinician groups expressed the view that working together would improve care. However, the health care system is not structured for clinicians to deliver coordinated care.
Many clinicians across all clinician groups wanted clearer referral pathways and better communication between clinicians.
Effective communication between practitioners was considered an enabler for optimal care. In the absence of a systematic way of communicating, clinicians identified ad hoc arrangements they had developed which were effective in supporting children and families to receive improved care.
Some ad hoc arrangements develop from connections with colleagues.
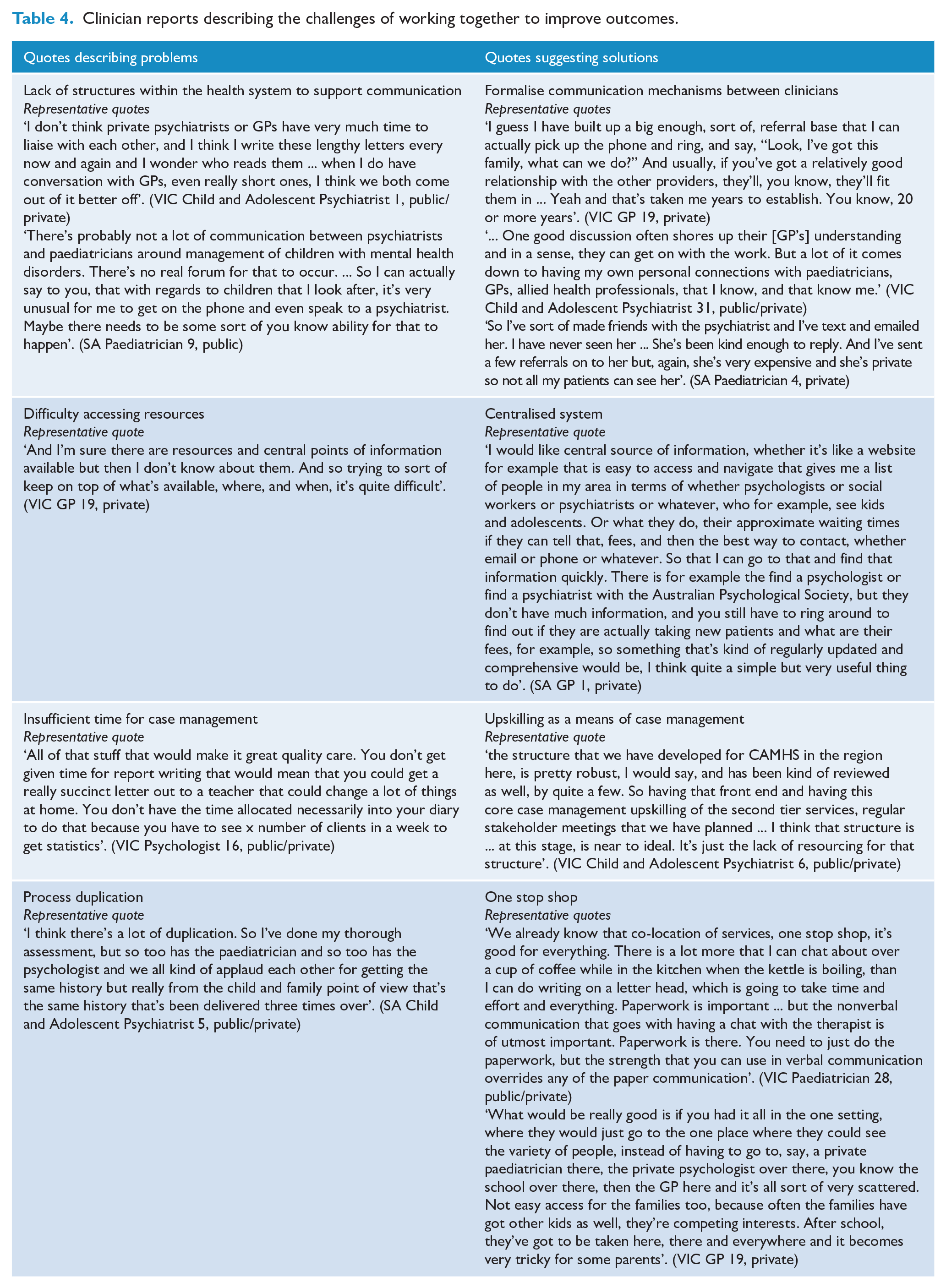
However, others developed their own support networks without a personal relationship. Co-location was a possible enabler of improved communication. Table 4 provides a summary of clinicians’ views of the challenges in communication and how to address them.
Clinician reports describing the challenges of working together to improve outcomes.
Discussion
This is the first study reporting clinicians’ perceptions of the major barriers faced by Australian young people and their parents when seeking help for common child and adolescent mental health conditions.
Clinicians identified barriers at three levels: (1) parent – poor mental health literacy, competing life stressors; (2) service – long wait times, restrictive entry criteria, large out-of-pocket costs, fragmentation of services; and (3) workforce – need for better training, need for better access to specialist support for GPs. These clinician-identified barriers are strikingly similar to those reported by parents in the two Australian child and adolescent national mental health surveys (Lawrence et al., 2015; Sawyer et al., 2000). For example, parents in both surveys also reported that not knowing where to get help, long waiting lists, high costs and geographical distance were major barriers to getting effective help for children and adolescents with mental health problems. The barriers are also similar to those reported in our smaller (n = 30) study of clinician perspectives about the care of children with complex mental health conditions using ADHD and Autism as exemplars (Paton and Hiscock, 2019). The consistency of results across these different groups suggests that these barriers should be given the highest priority in future planning for services designed to help children and adolescents with mental health problems in Australia.
This study extends previous work by including GPs as respondents. Results from GPs highlight the extent to which these clinicians want better access to secondary consultation with mental health specialists and also better training, particularly in relation to the management of acute child and adolescent mental health problems.
This study focused more specifically on mental health care than previous studies (as opposed to education and social care), purposively sampling clinicians working across diverse socioeconomic areas and including ADHD and anxiety as the two most common child mental health disorders. We could find no other study reporting on clinician views of how to improve the mental health system for children. Although the study is limited to clinicians working in one of two States in Australia, we believe results are readily generalisable to all Australian States and Territories (Paton and Hiscock, 2019).
Our findings suggest several avenues for improving the current system for children and are especially pertinent given the potential increase in mental health problems with the Covid-19 pandemic. These avenues include increasing the availability of specialist mental health support to non-specialists such as GPs and paediatricians via email, telephone or telehealth, as per successful US models (Sarvet et al., 2010). With the Covid-19 pandemic, most clinicians have pivoted to telehealth. Anecdotally, this seems to suit many families and clinicians, but rigorous evaluations are yet to be published and telehealth may not deliver effective care for children and adolescents with complex mental health problems.
Clinicians also called for a centralised service that provides information on services and pathways in a staged manner, responding to the child’s needs. While some major mental health initiatives provide this type of support for adolescents and adults (e.g. Beyond Blue, 2020), they do not provide information relevant to children under 12 years of age. Furthermore, many websites suggest patients should seek help from GPs in the first instance, but our study suggests that GPs want more effective specialised support when assessing and treating child and adolescent mental health problems.
Many clinicians in this study called for increased training in child mental health, including practical experience working in public specialist mental health services. For GPs, this would require significant changes to their current vocational training requirements for paediatrics which largely focus on medical and not mental health or behavioural problems (The Royal Australian College of General Practitioners (RACGP), 2020). Telementoring is one approach that might allow for GPs to upskill in child mental health. Project ECHO is a telementoring model which uses proven adult learning techniques and interactive video technology to connect groups of community providers with specialists at centres of excellence in regular real-time collaborative sessions (Zhou et al., 2016). Queensland Children’s Health has been using the Project ECHO model (Queensland Children’s Health, 2020) for ADHD and behavioural concerns, with positive feedback from clinicians involved (Dr Newcomb, Medical Director Integrated Care, Queensland Children’s Health, personal communication). More intensive approaches include the REsource for Advancing Children’s Health (REACH) project in the United States (The Reach Institute, 2020) which provides interactive skills building followed by a 6-month case-based distance-learning programme or the United Kingdom’s general practitioner with special interest (GPSI) model where GPSIs take referrals from other GPs and work within integrated consultant-led clinical teams in addition to specialists (Yellamaty et al., 2019). This model has been associated with superior patient satisfaction and comparable outcomes to specialists but requires appropriate training, mentoring and ongoing professional development for GPs and employers adopting this role.
Co-location of ‘private’ and ‘public’ services that provide help for the emotional, physical and social needs of children, parents and families has the potential to overcome several current service barriers identified by clinicians and parents. For example, co-location of such services has the potential to reduce current service fragmentation and to make it easier for parents to know where to get help for problems in these areas. The latter is an important issue because comorbid problems at the child, parent and family levels are common among children and adolescents with mental health problems. Co-location of services would allow children and parents to more easily access services that could address a range of such comorbid problems. The closer proximity of services would also encourage better co-ordination and information flow between staff in co-located services.
The current Medicare emphasis on funding based on the ‘fee for service’ concept limits opportunities for even co-located staff and services to work together in a coordinated and cooperative manner. This is a significant problem for the effective assessment and management of children with mental health problems, many of whose mental health problems are entwined with family, education and social issues – all of which may need addressing before a child’s mental health will improve. As recommended in the recently released Productivity Commission into Mental Health (recommendation 10.3) (Productivity Commission, 2020), funding models that encourage different clinicians and services to work together more effectively have the potential to help address this issue.
In summary, the provision of help for children and adolescents with mental health problems in Australia has often floundered as a result of major structural, training, resource and workforce issues. Clinicians in this study identified a range of barriers and potential solutions to these problems. It is notable that the issues identified by clinicians were strikingly similar to those identified by parents in the two Australian national child and adolescent mental health surveys. The challenge now is to get the Australian Government along with State and Territory Governments to use the information provided by both clinicians and parents when developing, implementing and evaluating new systems of care for Australian children and adolescents with mental health problems.
Supplemental Material
sj-pdf-1-anp-10.1177_0004867420984242 – Supplemental material for Clinicians’ perceptions of the Australian Paediatric Mental Health Service System: Problems and solutions
Supplemental material, sj-pdf-1-anp-10.1177_0004867420984242 for Clinicians’ perceptions of the Australian Paediatric Mental Health Service System: Problems and solutions by Kate Paton, Lynn Gillam, Hayley Warren, Melissa Mulraney, David Coghill, Daryl Efron, Michael Sawyer and Harriet Hiscock in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-pdf-2-anp-10.1177_0004867420984242 – Supplemental material for Clinicians’ perceptions of the Australian Paediatric Mental Health Service System: Problems and solutions
Supplemental material, sj-pdf-2-anp-10.1177_0004867420984242 for Clinicians’ perceptions of the Australian Paediatric Mental Health Service System: Problems and solutions by Kate Paton, Lynn Gillam, Hayley Warren, Melissa Mulraney, David Coghill, Daryl Efron, Michael Sawyer and Harriet Hiscock in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
We would like to thank Shea Rendall for her assistance in interviewing participants. This research project was completed as part of the ‘Towards an evidence-based and equitable mental health system for children in Australian project’.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: D.C. reports grants and personal fees from Shire, personal fees from Eli Lilly, personal fees from Medice, personal fees from Novartis, personal fees from Oxford University Press, grants from Vifor, personal fees from Servier, all outside the submitted work. All other authors have no financial relationships relevant to this article to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The project’s study design and conduct, data collection, management, analysis and interpretation were funded by National Health and Medical Research Council (NHMRC) Grant No. 1129957. H.H. is supported by NHMRC Practitioner Fellowship Award 1136222. The Murdoch Children’s Research Institute administered the grants and provided infrastructural support to its staff but played no role in the conduct or analysis of the research. D.F.’s position is funded by a Clinician Scientist Fellowship from MCRI. The Victorian Government’s Operational Infrastructure Support Program support research at the Murdoch Children’s Research Institute.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.