
Abstract
Objective:
To identify the percentage of 4–17 year olds with mental disorders in Australia who attended health professionals for single or repeat visits to get help for emotional and behavioural problems during a 12-month period. To identify factors associated with single and repeat visits, and the average length of time between visits. To compare the number of parent-reported visits with visits recorded in the Medicare Benefits Schedule.
Method:
The study used data from the national survey of the mental health and wellbeing of 4–17 year olds conducted in 2013–2014 (n = 6310). Participants were randomly selected from all 4 to 17 year olds in Australia. Information about visits was available from face-to-face interviews with parents, the Medicare Benefits Schedule and self-reports from 13 to 17 year olds. Mental disorders were assessed using the Diagnostic Interview Schedule for Children Version IV completed by parents.
Results:
Parents reported that 51.1% of 4–17 year olds with mental disorders had attended a health professional during the previous 12 months. However, 13.6% of these children had attended on only a single occasion, most commonly with a general practitioner. With the exception of occupational therapists, 2–4 visits was the most common number of repeat visits. Children with comorbid disorders and severe functional impairment and those aged 12–17 years were more likely to have repeat visits. Among those with linked Medicare Benefits Schedule data, more children were reported by parents to have attended Medicare Benefits Schedule-funded health professionals (47.9%) than were recorded in Medicare Benefits Schedule data (38.0%).
Conclusion:
The typical number of visits to health professionals by children with mental disorders during a 12-month period is relatively small. Furthermore, parent-reports may overestimate the number of visits during this time. It seems unlikely that current patterns of attendance are of sufficient duration and frequency to allow full implementation of evidence-based treatment programmes for child and adolescent mental disorders.
Introduction
Child and adolescent mental disorders have a significant adverse impact on children, families and the community (for brevity, the term ‘children’ will be used to describe children and adolescents in this manuscript) (Institute for Health Metrics and Evaluation (IHME), 2017; Kessler et al., 2005; Knapp et al., 2011). To successfully address this problem at a population level, it is essential that universal, targeted and clinical services are employed in the most effective manner possible. This is particularly important for services provided by health professionals because such services are expensive to provide and often relatively scarce.
Accurate information about the proportion of children with mental disorders in the general community who have contact with health professionals and the nature of this contact is an essential prerequisite to determine the effectiveness of clinical interventions at a population level. While more recent studies have reported that a higher proportion of children with mental disorders in the community have contact with health professionals, a significant limitation of almost all previous studies is lack of information about the extent to which this contact is comprised of a single visit or includes sufficient ongoing contact to allow delivery of evidence-based treatment programmes (Farmer et al., 1999; Green et al., 2013; Johnson et al., 2016). This is an important issue because interventions recommended in treatment guidelines for the management of childhood mental disorders such as major depressive disorder (MDD), attention-deficit hyperactivity disorder (ADHD), conduct disorder (CD) or anxiety disorders (AD) uniformly require multiple contacts with service providers (National Institute for Health and Care Excellence, 2016, 2017a, 2017b). In contrast, there is no evidence of which the authors are aware that demonstrates a single visit with a health professional is sufficient to effectively treat these disorders. A further limitation of previous studies is lack of information about the frequency of visits (e.g. weekly, monthly or annually). This is a significant omission because of the potential adverse impact that long gaps between visits can have on the quality of therapeutic relationships required for effective delivery of treatment programmes.
Four previous studies have reported the number or frequency of service attendances by children with mental disorders in population samples (Farmer et al., 1999; Lawrence et al., 2015; Meltzer et al., 2000; Merikangas et al., 2011). In Australia, Lawrence et al. (2015) reported that over a 12-month period, 41.7% of visits to general practitioners, 31.7% to paediatricians, 21.3% to psychiatrists and 17.2% to psychologists by children with mental disorders seeking help for emotional and behavioural problems consisted of single visits (Lawrence et al., 2015). However, the extent to which these children had also attended other health professionals on repeated occasions during this time was not reported. This makes it difficult to interpret the meaning of the results as access to psychiatrists and paediatricians, and commonly psychologists, for the treatment of mental health problems requires a referral from a general practitioner in Australia. As such, a single visit with a general practitioner may have been for the purpose of obtaining a referral to a specialist. It is also possible that a child who had a single consultation with one health professional may have attended another on several occasions.
In Great Britain, Meltzer et al. (2000) reported that over a 12-month period 25% of 5–15 year olds with a mental disorder had attended their general practitioner >2 times compared to 13% of children without a disorder. However, the authors indicated that these visits could be for any health problem rather than specifically for management of mental health problems. In the United States, in a 1-year prospective study of 1007 children aged 9, 11 or 13 years at baseline, approximately 30% of those who used a health or education service to address a mental health problem during a 3-month period continued to use services during a subsequent 3-month period. However, less than 10% used services during multiple 3-month periods across the year of the study (Farmer et al., 1999). For mental health services, the most common pattern was 1–2 visits over a 3-month period. Using data from the National Comorbidity Survey, Merikangas et al. (2011) reported that 68% of 13–18 year olds with mental disorders in the United States had less than six ‘service contacts’ (p. 38) across their life time. The authors described this as a very small number of lifetime visits for young people with disorders typically associated with high service needs.
This study had three main aims: (1) to identify the percentage of 4–17 year olds with mental disorders in Australia who attended health professionals for single or repeat visits during a 12-month period, (2) to identify factors associated with single and repeat visits and (3) to identify the typical length of time between repeat visits. To assess the accuracy of parent-reported service use, for 13–17 year olds we also compared the number of parent-reported visits to health professionals, visits recorded in the Medicare Benefits Schedule (MBS) and self-reported visits over the 12-month period.
Methods
Participants
The participants were children identified as having a mental disorder in the second Australian Child and Adolescent Survey of Mental Health and Wellbeing (Lawrence et al., 2015). The survey was conducted during 2013–2014 and the dataset is available to research professionals (Zubrick et al., 2014). Participants were a nationally representative sample of 6310 4–17 year olds and their parents/carers (for brevity referred to as parents; response rate = 55%). Young people aged 11–17 years (89% of those eligible, n = 2967) completed their own questionnaire. Details of the survey methodology have been described elsewhere (Hafekost et al., 2016).
Participation in the survey was voluntary and all participants gave written consent to participate. The research protocol for the study was approved by the Australian Government Department of Health Human Research Ethics Committee and The University of Western Australia Human Research Ethics Committee.
Measures
Mental disorders
Mental disorders were assessed using the Diagnostic Interview Schedule for Children–Version IV (DISC-IV) completed by parents (Fisher et al., 1993; Shaffer et al., 2000). The DISC-IV implements the criteria for mental disorders set out in the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (American Psychiatric Association, 2000). Seven DISC-IV modules were completed by parents in relation to their children’s symptoms and the impact of these over the previous 12 months: AD (including social phobia, separation anxiety disorder, generalised anxiety disorder, obsessive–compulsive disorder); MDD; ADHD; and CD. For the purpose of this study, we report visits to health professionals by those who met criteria for a disorder during the previous 12 months.
Functional impairment
Detailed information about the measure used to assess children’s level of functional impairment is available in a technical report (Zubrick et al., 2015). In brief, the measure consists of 17 items that rate the extent to which AD, MDD, ADHD or CD adversely affect children’s schooling, friendships, family and the children themselves. For the purpose of this study, we used tertiles from the total functional impairment score to categorise children into one of three impairment groups described as mild, moderate and severe impairment. If a child had an impairment score for more than one diagnosis, the most severe level of functional impairment was utilised in this study.
Parental psychological distress
The Kessler-6 (K6) scale was used to assess parental psychological distress in the past 4 weeks. For the purpose of this study, recommended cut-off scores were used to categorise parents into one of two distress levels described as ‘high’ and ‘normal’ (Furukawa et al., 2003).
Family functioning
A short version of the General Functioning Scale of the Family Assessment Device completed by parents was used to assess family functioning. Recommended cut-off scores were used to categorise families into one of two groups described as ‘unhealthy’ and ‘healthy’ (Boterhoven de Haan et al., 2015).
Parent-reported service use
Parents were asked whether their child had attended a general practitioner, paediatrician, psychologist, psychiatrist and/or another health professional (i.e. social worker, occupational therapist, counsellor/family therapist) to get help for emotional or behavioural problems during the last 12 months. Parents who responded positively were asked for the location of this service (e.g. ‘doctor’s rooms or other private practice’, Child and Adolescent Mental Health Service and hospital emergency). They were also asked whether their child had attended 1, 2–4, 5–9 or ⩾10 times during the 12 months. Children aged 13–17 years (n = 2314) were also asked whether they had attended any of these professionals but were not required to identify the number of visits.
For the purpose of this study, the number of visits with health professionals during the 12 months before the survey were categorised as follows:
One visit. The child had only one visit with a health professional. Note that this category includes a small number of children (n = 14) who had one visit with more than one health professional during the 12 months.
One visit plus ⩾2 visits with another health professional. The child attended a combination of single and repeat visits with health professionals in different disciplines. For example, if a child had one visit with a general practitioner and ⩾2 visits with another health professional, they would be included in this category.
Number of visits. The number of visits to health professional during the previous 12 months as specified in the parent survey questionnaire (i.e. 1 visit, 2–4 visits, 5–9 visits, or ⩾10 visits).
Data from MBS
Consent to access MBS data was obtained from children aged ⩾14 years and from their parents for 78.1% (n = 4817) of children in the survey. Information about visits with general practitioners, paediatricians, psychologists, psychiatrists, social workers and occupational therapists was available from MBS data. The MBS items used to identify visits with each of these health professionals are shown in Supplementary Appendix A. For general practitioners, occupational therapists and social workers, we limited visits to those relating to mental health support. There are no specific MBS items relating to the assessment or treatment of AD, MDD, ADHD or CD for paediatricians. However, paediatricians generally use MBS items 110 and 132 for new cases related to mental health, and items 116 and 133 for any mental health treatment and reviews (Hiscock et al., 2017).
Sociodemographics
Family type, household income and household location (metropolitan vs non-metropolitan) were collected using the Australian Bureau of Statistics standard formats (Australian Bureau of Statistics, 2014).
Statistical analyses
Statistical analyses used parent responses to the national survey to identify the percentage of children with mental disorders who had single and/or repeat visits with health professionals during the 12 months prior to the survey. In all the analyses, survey data were weighted to represent the full Australian population of 4–17 year olds and to adjust for patterns of non-response. Visits to nurses or health professionals whose professional discipline was unknown were not included in these analyses.
Logistic regression was then used to examine the strength of the relationship between number of visits (single and repeated), and child and family demographic characteristics, children’s level of functional impairment, family functioning, parental distress and the presence of comorbid disorders. All analyses were conducted using the Stata software ‘svy’ procedure to account for the clustered nature of the sample design and use of survey weights (StataCorp, 2017). In these analyses, two sets of logistic regression models were fitted. Initially bivariable logistic models were used to assess the strength of the relationship between service use and each predictor variable. Subsequently, a single multivariable model was produced in which all the predictor variables were included in the model to identify the strength of the relationship between service use and each predictor variable, after adjusting for the effect of the other predictor variables. The analyses using parent-reported visits were all repeated using MBS data.
Throughout the presentation of results, the percentages are weighted to represent the full Australian population of 4–17 year olds while the number of participants shown is the number in the survey sample.
Results
As previously reported, 13.9% (n = 870) of the children in the second Australian Child and Adolescent Survey of Mental Health and Wellbeing had problems that met the criteria for AD, MDD, ADHD or CD (American Psychiatric Association, 2000; Lawrence et al., 2015). No information about service use was available for seven of these children and due to missing data it could not be determined if an additional 17 children had ⩾2 visits with a health professional. The majority of these 17 children had visited a general practitioner. This left 846 children with mental disorders for whom relevant service use data were available. Within this group, some information about their repeat visits was missing for six participants. They were included in the analyses of results where the missing information was not required.
Percentage of children attending health professionals
Of the 846 children with mental disorders for whom information was available, parents reported that 51.1% (n = 448) had attended a health professional on one or more occasions during the previous 12 months. Among these children, 10.8% (n = 44/448) had a single visit with only one health professional while a further 2.8% (n = 14/448) had single visits with two or more health professionals. The remaining children had attended ⩾2 appointments with at least one health professional during the previous 12 months (Table 1). The most common pattern among these children was for 2–4 visits (32.5%, n = 142/442).
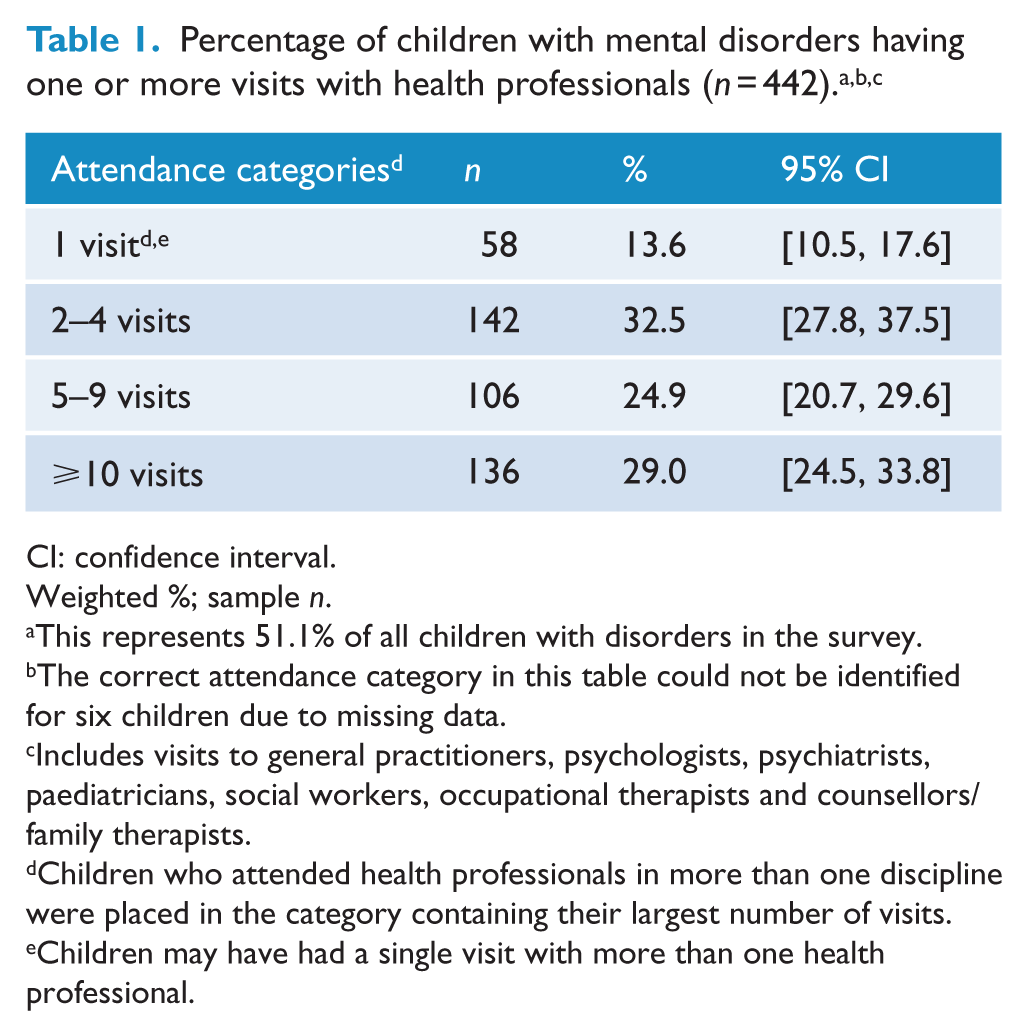
CI: confidence interval.
Weighted %; sample n.
This represents 51.1% of all children with disorders in the survey.
The correct attendance category in this table could not be identified for six children due to missing data.
Includes visits to general practitioners, psychologists, psychiatrists, paediatricians, social workers, occupational therapists and counsellors/family therapists.
Children who attended health professionals in more than one discipline were placed in the category containing their largest number of visits.
Children may have had a single visit with more than one health professional.
General practitioners (67.2%, n = 309/445), psychologists (52.8%, n = 242/446), paediatricians (41.1%, n = 170/447) and counsellors/family therapists (40.2%, n = 183/445) were the professionals most commonly attended by children with mental disorders (Table 2). Among those who attended general practitioners, 41.1% (n = 119/309) had only one visit during the 12-month period (Table 2). Of these, 29.6% (n = 84/119) of the children had also attended another professional for ⩾2 visits during this time (Table 2). Among those who attended general practitioners for ⩾2 visits, 40.0% (127/309) attended 2–4 times, 13.8% (44/309) attended 5–9 times and 5.0% (19/309) attended ⩾10 times (Table 2).
Percentage of children with mental disorders who had 1 and/or ⩾2 visits with health professionals (n = 442). a
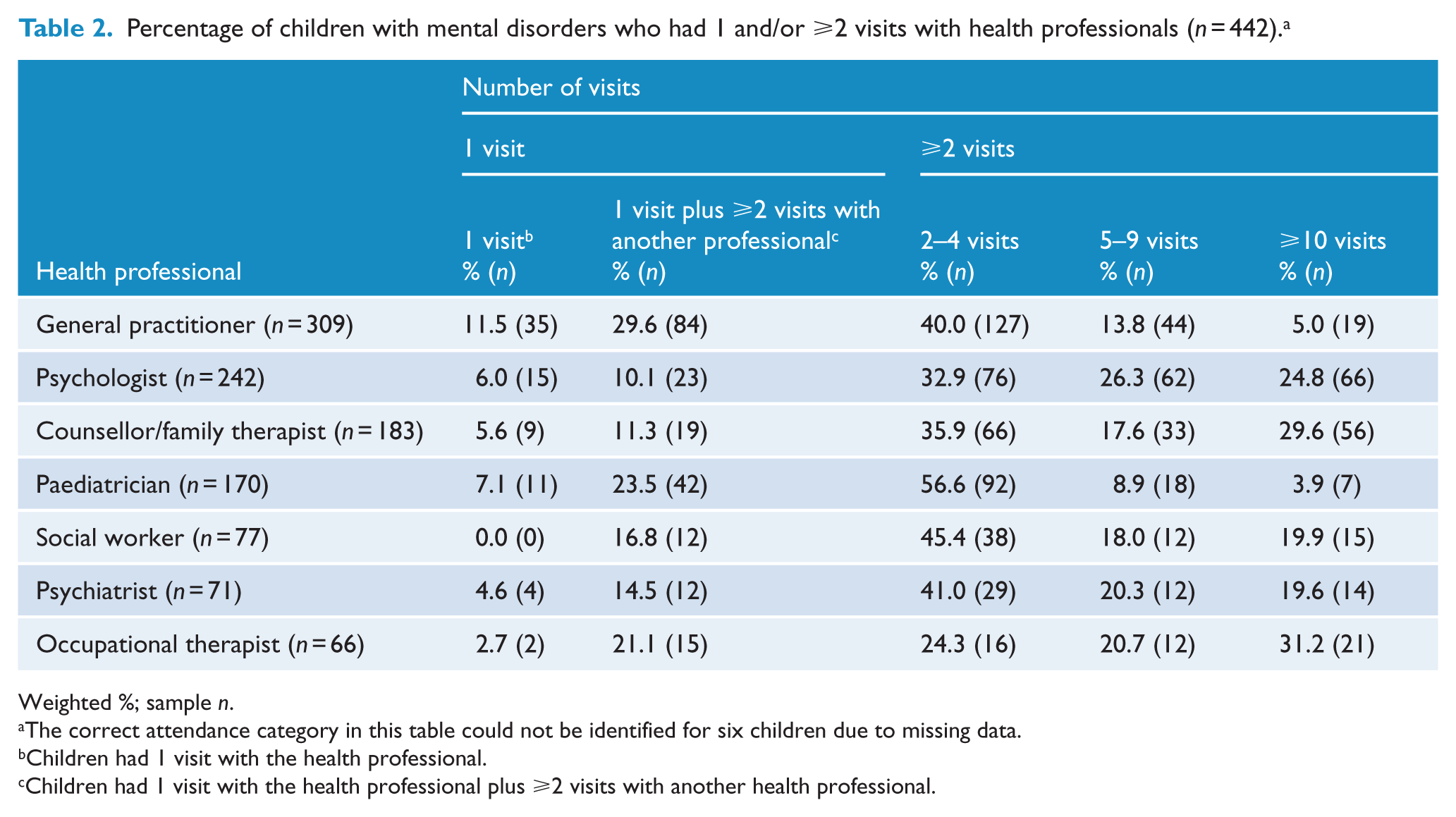
Weighted %; sample n.
The correct attendance category in this table could not be identified for six children due to missing data.
Children had 1 visit with the health professional.
Children had 1 visit with the health professional plus ⩾2 visits with another health professional.
A single visit was also a common pattern with several other health professionals (Table 2). For example, 30.6% (n = 53/170) of the children had only one visit to a paediatrician, 19.1% (n = 16/71) to a psychiatrist and 16.1% (n = 38/242) to a psychologist. The percentage of children who had one visit to these health professionals and who also had ⩾2 visits with a health professional in another discipline was 23.5% (n = 42/170) for paediatricians, 14.5% (n = 12/71) psychiatrists and 10.1% (n = 23/242) for psychologists. With the exception of occupational therapists, 2–4 visits was the most common number of repeat visits by children with each of the health professionals shown in Table 2.
Factors associated with visits to health professionals
To identify the strength of the relationship between the number of visits with health professionals reported by parents and the demographic and psychosocial characteristics of children with disorders, children were grouped into one of three categories: (1) no visits, (2) 1 visit and (3) ⩾2 visits. There was little difference in the demographic and psychosocial characteristics of children with no visits versus single visits with health professionals (Table 3). As well, none of the multivariable coefficients in the logistic regression models testing the strength of the differences across the two groups were significant at the level of p < 0.05 (Table 4).
Demographic and psychosocial characteristics of children and families, by number of visits with health professionals (n = 846). a
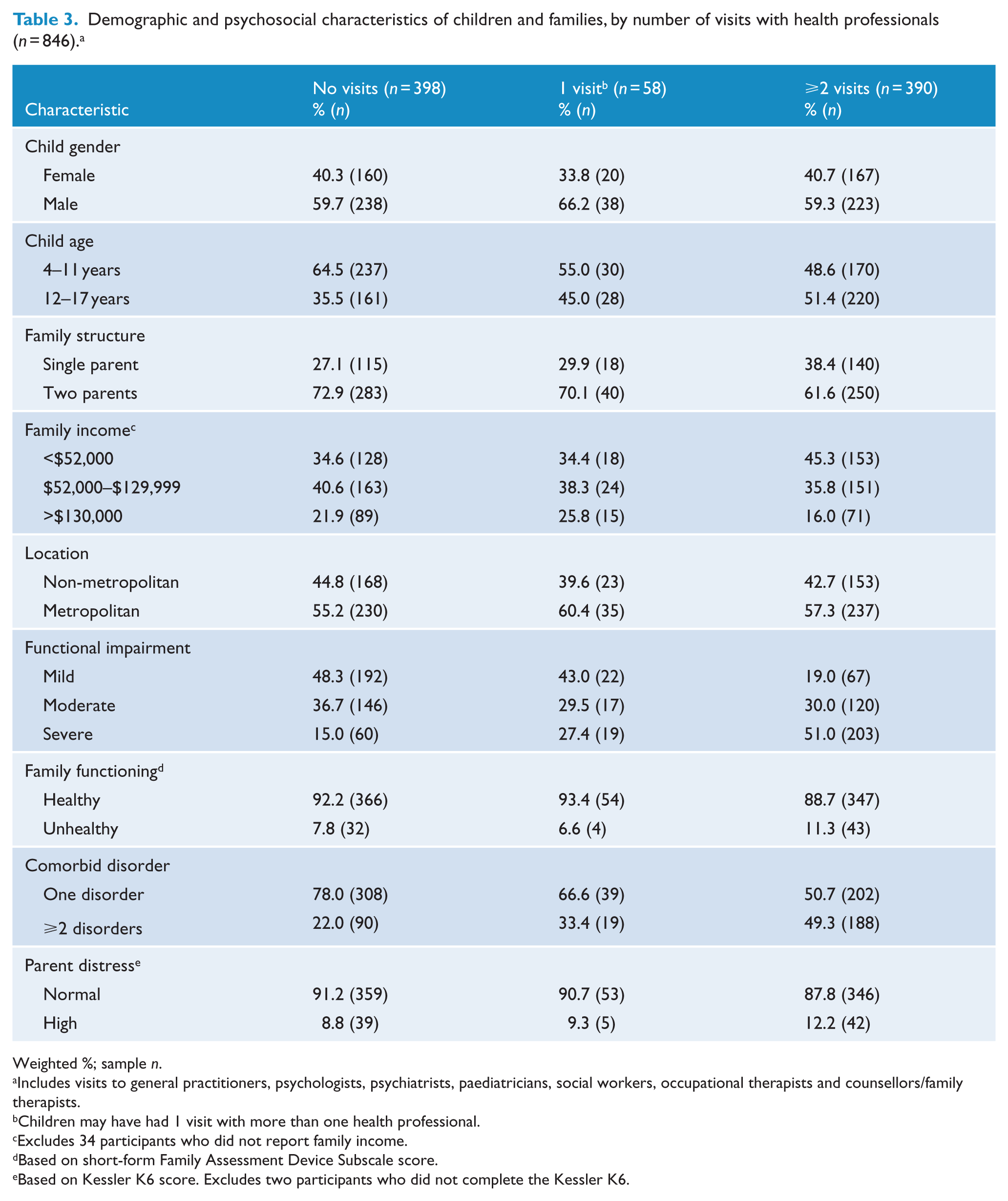
Weighted %; sample n.
Includes visits to general practitioners, psychologists, psychiatrists, paediatricians, social workers, occupational therapists and counsellors/family therapists.
Children may have had 1 visit with more than one health professional.
Excludes 34 participants who did not report family income.
Based on short-form Family Assessment Device Subscale score.
Based on Kessler K6 score. Excludes two participants who did not complete the Kessler K6.
Odds ratios (95% CI) for visits (vs no visit) with health professionals. a
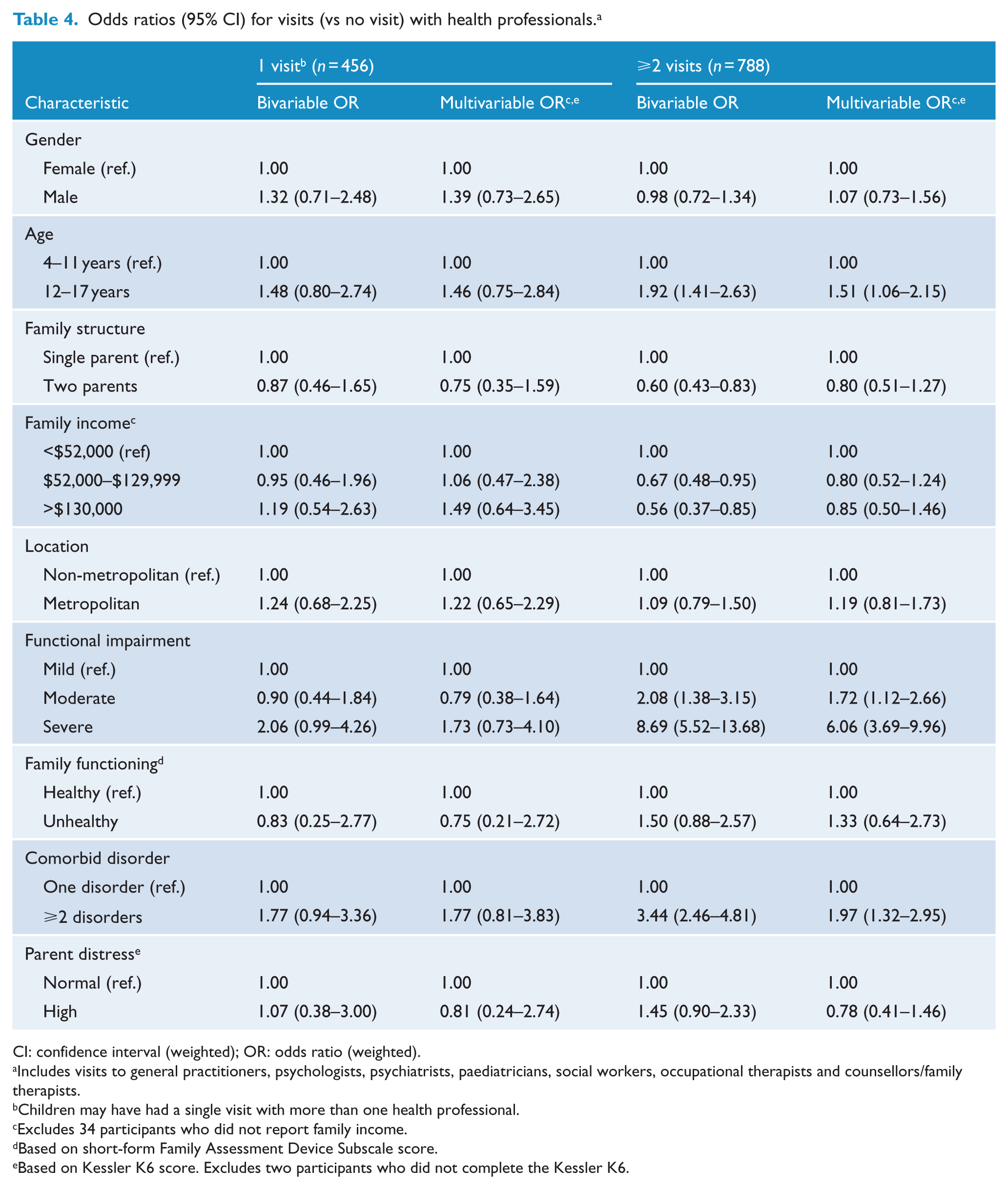
CI: confidence interval (weighted); OR: odds ratio (weighted).
Includes visits to general practitioners, psychologists, psychiatrists, paediatricians, social workers, occupational therapists and counsellors/family therapists.
Children may have had a single visit with more than one health professional.
Excludes 34 participants who did not report family income.
Based on short-form Family Assessment Device Subscale score.
Based on Kessler K6 score. Excludes two participants who did not complete the Kessler K6.
As compared to those with no visits to health professionals, a higher percentage of children who had ⩾2 visits were 12–17 year olds, had severe functional impairment, a comorbid disorder and lived in lower income and single-parent families (Table 3). In the multivariable logistic regression models, children with ⩾2 visits were 6.1 times more likely to have severe functional impairment, 2.0 times as likely to have a comorbid disorder and 1.5 times more likely to be in the 12–17 year age group than children with no visits to health professionals (Table 4).
Time between visits to health professionals
Information about the time between visits for children with ⩾2 visits was available for 181 of the children with linked MBS data (Table 5). This showed that repeat visits with general practitioners had a median gap of 75 days (IQR = 33–153 days) (Table 5). The median gap for psychologists was 14 days (IQR = 9–28 days), for psychiatrists it was 31 days (IQR = 15–54 days) and for paediatricians it was 70 days (IQR = 29–125 days).
Median number of days between visits for children with mental disorders who had ⩾2 visits reported in MBS data (n = 181).
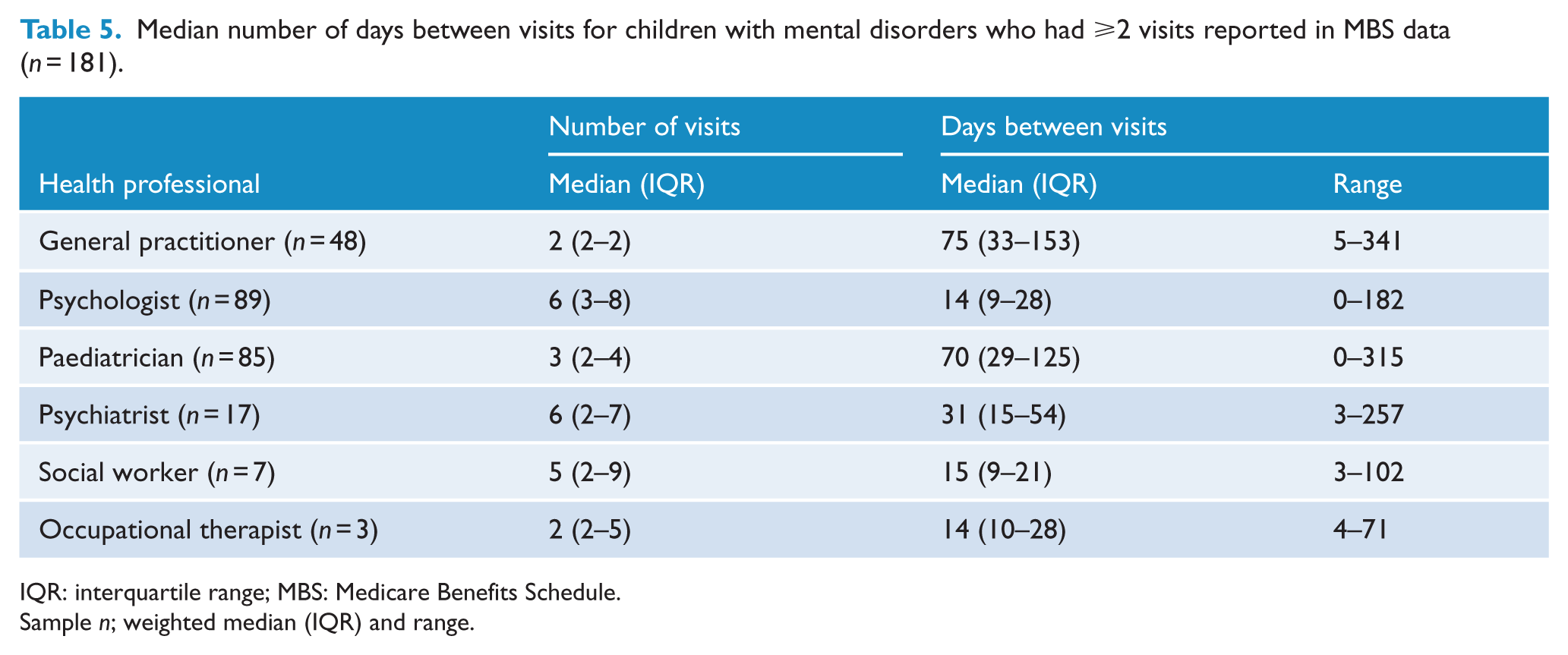
IQR: interquartile range; MBS: Medicare Benefits Schedule.
Sample n; weighted median (IQR) and range.
Sensitivity analyses
MBS-recorded visits. Consent for MBS data access was provided for 80.2% (n = 657/846) of the children. With the exception of child age, there was little difference in the demographic and psychosocial characteristics of children, and parent-reported service use, for children for whom consent was provided versus those for whom it was not provided. However, consent from 14 to 17 year olds as well as parents was required for MBS data linkage for children aged 14 years and older. As a result of a lower rate of consent by 14–17 year olds, there was a smaller proportion of 12–17 year olds in the group for whom MBS data were available (38.4%, n = 283/657) versus those for whom data were not available (62.2%, n = 126/189).
In total, 47.9% (n = 323/657) of the parents who consented to MBS access reported that their child had attended a MBS-funded health professional during the previous 12 months. This included visits to general practitioners, paediatricians, psychologists, psychiatrists, social workers and occupational therapists (counsellors/family therapists were not included in these analyses as they cannot be identified in MBS data). However, only 38.0% (n = 245/657) of these children had an attendance recorded in the MBS data. Unlike other MBS-funded health professionals, paediatricians have no specific MBS items with which to bill the MBS for provision of mental health services to children with AD, MDD, ADHD or CD. As a result, it is not possible in MBS data to distinguish between these services and those provided by paediatricians for other health problems. In light of this, we repeated comparisons between parent-reported and MBS-recorded service use after dropping paediatricians from the analyses. When this was done the difference between parent-reported service use and MBS-recorded service was somewhat larger (parent-reported = 44.8%, n = 305/657 vs MBS-recorded = 23.3%, 163/657).
Parents reported that a smaller percentage of children (16.7%, n = 52/323) had a single visit with health professionals than was recorded in MBS data (27.6%, n = 64/245). They also reported that a larger percentage of children (23.5%, n = 79/323) had ⩾10 visits than was recorded in the MBS data (7.3%, n = 22/245; Table 6). Both sources of information indicated that 2–4 visits was the most common number of repeat visits. To reduce the possibility that differences between parent and MBS results were due to health professionals providing care in settings such as schools or community health services where they did not seek payment from MBS, these analyses were repeated for visits that were specifically identified as taking place in ‘doctor’s rooms or other private practice’. The results of these analyses were very similar to those obtained using all the contacts with health professionals and do not change the study’s conclusions (data not shown).
Percentage of children with mental disorders attending a health professional according to parent report and MBS records. a
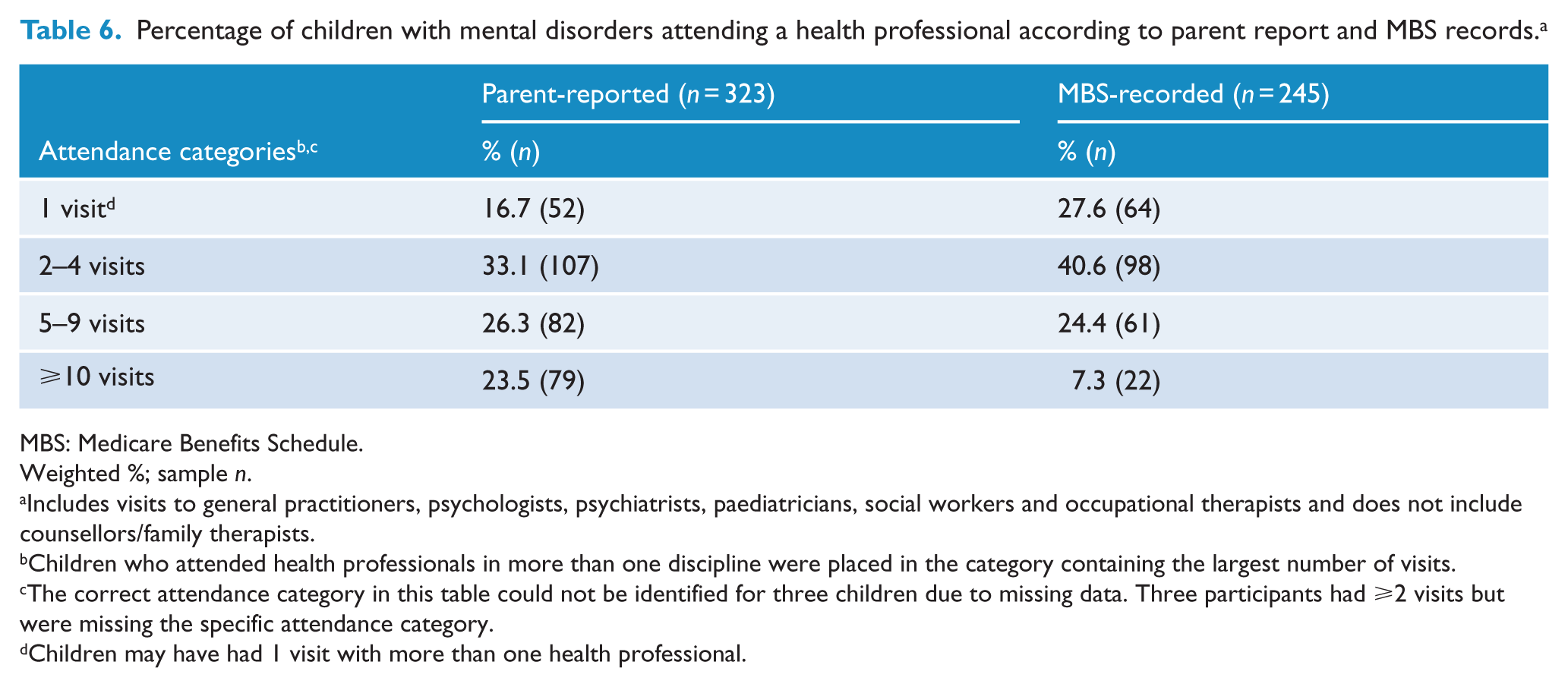
MBS: Medicare Benefits Schedule.
Weighted %; sample n.
Includes visits to general practitioners, psychologists, psychiatrists, paediatricians, social workers and occupational therapists and does not include counsellors/family therapists.
Children who attended health professionals in more than one discipline were placed in the category containing the largest number of visits.
The correct attendance category in this table could not be identified for three children due to missing data. Three participants had ⩾2 visits but were missing the specific attendance category.
Children may have had 1 visit with more than one health professional.
Consistent with results obtained from parent-reports, there was little difference in the demographic and psychosocial characteristics of children with no visits versus single visits with health professionals (see Supplementary Appendix B, Table 1). In the multivariable logistic regression analyses, only the multivariable coefficient describing the relationship between single visits and severe functional impairment was significant at the level of p < 0.05 (see Supplementary Appendix B, Table 2). In contrast, as compared to children with no visits to health professionals, a higher percentage of children who had ⩾2 visits were 12–17 year olds, had severe functional impairment, a comorbid disorder, lived in metropolitan regions and lived in lower income and single-parent families (see Supplementary Appendix B, Table 1). In the multivariable logistic regression model, children with ⩾2 visits were 3.8 times more likely to have severe functional impairment and 2.6 times more likely to have comorbid disorders than children with no visits to health professionals. They were also 1.7 times more likely to live in metropolitan regions (see Supplementary Appendix B, Table 2).
2. Parent-reported and self-reported versus MBS-recorded visits. Information about visits by 13–17 year olds to MBS-funded health professionals was available from parent-reports, MBS records and self-reports for 232 children. We included the later reports in this comparison because of the possibility that older children had visits to health professionals of which their parents were unaware. Among these children, 56.2% (n = 131) had parent-reported visits, 42.3% (n = 99) MBS-recorded visits and 37.4% (n = 90) self-reported visits (see Supplementary Appendix B, Table 3).
Discussion
Several findings are evident from this study. First, parents reported that 51.1% of the 4–17 year olds with mental disorders in the study had contact with a health professional during the 12 months prior to the national survey. However, 13.6% of these contacts were for a single visit, most commonly with a general practitioner. Single visits were also relatively common with other health professionals ranging from 16.1% of visits with psychologists to 30.6% of visits with paediatricians. With the exception of occupational therapists, 2–4 visits was the most common number of visits with each of the health professionals over the 12 months assessed in this study.
Second, none of the demographic and psychosocial factors examined in the study had a strong relationship with single visits. In this area, the absence of a relationship between family functioning and service use is consistent with results of previous studies (Ryan et al., 2015). However, as compared to children with no visits to health professionals, children with ⩾2 visits were six times more likely to have severe functional impairment, twice as likely to have comorbid disorders and 1.5 times more likely to be aged 12–17 years old.
Third, there was a sizable gap in time between visits with most health professionals. For example, the median number of days between appointments with psychiatrists was 31 days and for paediatricians it was 70 days. For psychologists, the median number of days between visits was 14 days. For all these health professionals, there was also a very wide range in the length of time between visits.
Finally, comparisons of parent-reports and MBS records suggest that parent-reports may overestimate the number of 13–17 year olds who attend health professionals for help with mental health problems. They also suggest that parent-reports may overestimate the number of repeat visits 13–17 year olds have with health professionals.
The results suggest that although the number of children having contact with health professionals appears to have increased in Australia over the last 20 years (Lawrence et al., 2015; Sawyer et al., 2000), the number of repeat visits to health professionals remains small. Saloner et al. (2014) have suggested that ⩾4 visits are required for minimally adequate treatment for mental disorders involving a psychotropic medication and ⩾8 visits for treatment without medication. While it was not possible to identify the nature of children’s treatment in this study, it is notable that among the children with mental disorders, less than 30% (n = 242/840) had ⩾5 visits with a health professional and only 15% (n = 136/840) had ⩾10 visits during the 12 months of the study. It was also notable that there was often a substantial gap in time between repeat visits. The latter is important because long gaps between visits have the potential to both hinder the implementation of evidence-based treatment programmes and adversely affect the quality of therapeutic relationships that are a key element of many such programmes.
Relatively little is known about how long children with mental disorders stay enrolled in services and what influences ongoing use of services. The results from this study suggest that somewhat different factors influence single versus repeat visits with health professionals. Specifically, the characteristics of those with single visits were not significantly different from those with no visits. However, those with ⩾2 visits had higher levels of functional impairment and comorbidity and were also more commonly older than those with no visits. This is consistent with one of the few previous studies to examine this issue which reported that higher symptom levels among children, greater parental psychopathology and higher parent education were associated with persisting service use over a 12-month period (Farmer et al., 1999). In this study, level of functional impairment and presence of comorbid disorders had a stronger association with participation in ongoing treatment than other demographic characteristics such as family income and family structure. This suggests that it is the clinical characteristics of children’s problems, rather than their demographic characteristics that are playing the key role in decisions about the provision of ongoing care and support.
The low percentage of children with mental disorders receiving minimally adequate treatment is similar to that reported in a recent national study of adults with affective and/or anxiety disorders in Australia where only 16% of participants were receiving minimally adequate treatment, defined in a similar way to this study (Harris et al., 2015; Saloner et al., 2014). This frequent pattern of inadequate care cannot be identified in studies where level of service use is described using a dichotomous indicator that simply records service contact versus no contact. However, it is an important issue because epidemiological studies conducted during the last decade have demonstrated that the prevalence of child and adult mental disorders is not decreasing in Australia and other industrialised countries (Collishaw, 2015; Collishaw et al., 2010; Jorm et al., 2017; Lawrence et al., 2015; Sawyer et al., 2000). Jorm et al. (2017) have suggested that a potential reason for the lack of change in prevalence of mental disorders among adults is that much of the treatment provided may fail to meet minimal standards of clinical practice guidelines. The results from this study suggest that similar problems may exist with much of the treatment provided to children with mental disorders.
Problems with service systems, health practitioner issues, and parental knowledge and attitudes all have the potential to adversely affect the dose of treatment received by children with mental disorders. Service system issues include problems with service access, the cost of services (including incidental costs such as travel costs, lost work time and costs of child care for siblings) and lack of availability of ongoing appointments (Lawrence et al., 2015; Sawyer et al., 2000). Health care provider issues include failure to deliver evidence-based treatments, variations in clinical practice and insufficient time or remuneration for delivery of evidence-based treatments. Parent issues include uncertainty about whether children need help, a preference to handle problems themselves and difficulties getting children to attend appointments (Lawrence et al., 2015; RCH National Child Health Poll, 2017). It is notable that in both Australian national surveys, practical problems of this kind were more commonly identified as barriers than issues related to stigma (Lawrence et al., 2015; Sawyer et al., 2000). This suggests that while it is important to continue addressing issues of stigma, doing this without addressing the significant practical problems experienced by parents seeking help for children with mental disorders will not improve treatment outcomes.
Finally, the results highlight the value for population-level service planning of combining information collected in epidemiological studies with that available in electronic health records, such as MBS. As noted by Angus (2015), electronic health records have the advantages of being inexpensive to access, specific to individuals and also descriptive of entire populations. The value of this information is evident in this where it appears that parents may overestimate the number of visits children with mental disorders have with health professionals as compared to data collected contemporaneously at the time of the visit. It is possible that this occurred because parents were reporting visits to health professionals funded through private health insurance schemes or for services based in schools or in public health services. However, when comparisons were limited to services provided in doctor’s rooms or other private practice settings, the gap remained.
Limitations
Strengths of this study include its national scope, the quality of its sampling methods, and its use of well-established diagnostic criteria and methods. However, it also has some limitations. These include a response rate of 55% and diagnostic information limited to parent-report. Extensive checking showed that the participants were highly representative of the national population of 4–17 year olds (Hafekost et al., 2016; Lawrence et al., 2015). However, it is possible that inclusion of children who did not participate in the survey may have changed population estimates. It is also possible that additional information from other informants such as children or teachers may have altered the proportion of children who were considered to meet the criteria for one or more of the disorders in the study. Finally, it was beyond the scope of this study to investigate use of school-based services, but previous work has shown that these are also an important source of support for children with mental disorders (Lawrence et al., 2015).
Conclusion
This study demonstrates that while slightly more than 50% of children with mental disorders have contact with health professionals during a 12-month period, many of these children will have insufficient visits to allow for the delivery of interventions that meet minimum recommended clinical practice guidelines (National Institute for Health and Care Excellence, 2016, 2017a, 2017b).
The results highlight an urgent need to better understand why so few children with mental disorders receive minimally adequate care. There is also a continuing need to develop, implement and evaluate new interventions delivered in routine clinical practice that can benefit larger numbers of children than is possible with traditional face-to-face treatment approaches. Achieving these goals will require changes to service systems to optimise access to care, upskilling of existing workforces in evidence-based mental health care and greater use of Internet-based services to reach larger numbers of children with disorders. It will also require ongoing monitoring and feedback to health care professionals about both the care they provide and its effectiveness in providing help for children with mental disorders. Finally, success in these areas will only be achieved by working in partnership with parents and children to help facilitate early recognition of mental health problems and reduction of practical barriers that currently impede effective engagement with mental health systems of care.
Supplemental Material
Appendix_A – Supplemental material for Access to health professionals by children and adolescents with mental disorders: Are we meeting their needs?
Supplemental material, Appendix_A for Access to health professionals by children and adolescents with mental disorders: Are we meeting their needs? by Michael G Sawyer, Christy E Reece, Alyssa CP Sawye, Sarah E Johnson, Harriet Hiscock and David Lawrence in Australian & New Zealand Journal of Psychiatry
Supplemental Material
Appendix_B – Supplemental material for Access to health professionals by children and adolescents with mental disorders: Are we meeting their needs?
Supplemental material, Appendix_B for Access to health professionals by children and adolescents with mental disorders: Are we meeting their needs? by Michael G Sawyer, Christy E Reece, Alyssa CP Sawye, Sarah E Johnson, Harriet Hiscock and David Lawrence in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors wish to express their gratitude to the 6310 families who participated in the survey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The second Australian Child and Adolescent Survey of Mental Health and Wellbeing was funded by the Australian Government Department of Health. H.H.’s position is funded by an Australian National Health and Medical Research Council career development award (No. 607351). Murdoch Children’s Research Institute is supported by the Victorian Government’s operational infrastructure support programme.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.