
Abstract
Keywords
Caring for a child with a disability can be stressful. According to the 2003 Australian Bureau of Statisitics Survey on Disability, Ageing and Carers, there were around 2.2 million families in Australia with children aged between 0 and 14 years. One in eight of these families had a child with a disability [1]. The majority of these parents were primary carers, providing most of the informal help (e.g. assisting with mobility, communication, or self-care), and lived with and cared for their child. Over half of these parents spent more than 40 h a week providing care for their child, and many received little or no asistance. Psychologically, more than half of them reported feeling weary or lacking in energy. Others felt worried and depressed or angry and frustrated. Socially, these carers stated that their caring role had placed great strain on their relationship with their spouse or partner, and that they were losing touch or spent less time with other co-resident family members and existing friends. Indeed, 18% of these carers had been diagnosed with a stress-related illness.
A review of the literature suggests that elevated parenting stress can disrupt the parent–child relationship and negatively affect parenting practices in families with children with disabilities [2]. Parenting stress has also been linked to disruptions in parent psychological functioning, including depression, reduced parenting efficacy, and more punitive and less responsive parenting [3,4]. A higher level of parenting stress is also associated with more problem behaviour in children with disabilities [5,6]. Among the various disabled categories, the parents of children with autism appear to have a higher level of stress than the parents of children with developmental problems other than autism or with special health care needs but without developmental problems [7]. Caring for a child with a disabilty is clearly stressful, and affects the psychological health of carers, the quality of care given to a disabled child, the child's behavioural or emotional health, and the carer's relationships with others.
Research evidence on CBT
Several studies have tested the efficacy of CBT in helping parents with disabled children to better manage their emotions and symptoms of depression and anxiety. Singer et al. conducted a meta-analysis of the effects of parenting and stress-management interventions for parents of children with developmental disabilities [8]. Six of the studies used CBT to teach coping skills to parents to directly reduce the psychological distress associated with parenting stress. The results suggested that CBT has relatively small but consistent benefits in reducing parenting stress and distress. A closer look at the programme content reveals that the programmes reviewed focused on teaching coping skills and muscle relaxation to handle stressful situations, and on cognitive strategies to modify dysfunctional thoughts. However, as Singer et al. point out, many of these interventions lack ‘adequate responsiveness to cultural differences’ (p. 359). Another meta-analysis of stress interventions for parents of children with intellectual disabilities suggested that ‘the strongest evidence base is for cognitive behavioural group interventions, especially for the reduction of stress in mothers’ [9]. However, the researchers highlighted several limitations of these clinical trials. First, the clinical significance of the treatment effects was rarely addressed. Second, in terms of process measures, few of the studies included measures to show that unhelpful cognition was remedied or that problem-solving skills improved as a result of the intervention. Third, only a narrow range of outcome measures was reported in the studies under review.
There is a lack of clinical outcome studies in the literature that use CBT to reduce parenting stress for parents with children with developmental disabilities in Asian societies, except for one study conducted in South Korea. In that study, Ha and Oh found that the participants of their CBT group reported significantly lower scores for depressive symptoms, self-reported parent–child problems, negative automatic thoughts, and fewer behaviour problems in their children compared with a waiting list control group [10]. Positive results were also found at the three-month follow-up assessment. However, to the best of the authors’ knowledge, no study has tested the efficacy of CBT treatment for Chinese parents with children with developmental disabilities. This study attempted to fill this research gap by testing a culturally attuned CBT group treatment for Chinese parents with children with developmental disabilities and who were at risk of developing mental health problems in Melbourne, Australia. This clinical trial improved on previous studies by including a process variable (dysfunctional attitudes and values), two outcome variables (mental health and quality of life), and an analysis of clinical significance. The hypotheses of the study were that the participants in the experimental group would have less parenting stress and fewer dysfunctional attitudes, rules, and values and better mental health and quality of life than the participants in the control group post-treatment, and that changes in dysfunctional attitudes, rules, and values would be linked to changes in mental health and quality of life in the experimental group.
Method
Participants
Potential participants (n = 68) were recruited through advertisements posted at the Chinese Community Social Services Centre, which has offices in four regions in Melbourne, Victoria. The inclusion criteria included: (i) age 18–60 years; (ii) suffering from poor mental health and at risk of developing mental health problems as indicated by a score of at least four symptoms on the GHQ-12. Individuals who had psychosis or severely acute depressive symptoms at the time of interview, or had attempted suicide or had suicidal ideation in the three months before the interview were excluded from the study and were referred to other places for psychiatric assessment and intervention. After the pre-group interviews, five potential participants who had less than four symptoms on the GHQ-12 (i.e. not at risk of developing poor mental health) were excluded from the waiting list (n=5). Two others who had severely acute depressive symptoms (n = 1) and psychosis (n = 1) were similarly excluded and referred to psychiatric services for follow-up. A total of 61 participants were thus included in the study after the pre-group interview. A colleague at the Chinese Community Social Service Centre who had no affiliation with the research team was invited to randomly select participants into the experimental and waiting list control groups.
Group content
Lin argues that cognitive behavioural therapy is highly compatible with Chinese culture because the therapy is structured and solution focused [11]. However, Wong et al., and Kwan and Wong suggest that it is necessary to modify CBT for Chinese people with emotional problems [12–14]. This suggestion is based on the understanding that Asians (including Chinese) tend to have less tolerance for ambiguity and prefer structured counselling sessions that give practical and immediate solutions to their problems [15]. Furthermore, Chinese people prefer therapists to employ a directive rather than a non-directive approach, and expect them to play an active role in providing suggestions and advice in the counselling process [11].
Based on this information we designed and implemented a CBT group for treating Chinese parents in Melbourne, Australia with poor mental health who were at risk of developing mental health problems. The group was culturally attuned to fit the cultural characteristics of Chinese people. First, all of the technical terms in the group manual were translated into colloquial expressions. For example, ‘automatic thoughts’ were renamed ‘thought traps’ and the cognitive distortion of ‘personalization’ was rephrased as ‘putting all the blame and responsibilities onto oneself’. Second, several worksheets and exercises were written in Chinese to facilitate the understanding of the cognitive and behavioural processes and the learning of cognitive and behavioural skills. Third, the format of the group was structured, and the group leaders were active in structuring and facilitating the group processes, particularly in the initial stages of group development. Finally, when exploring the dysfunctional rules and values held by the group participants, the group leaders put great emphasis on helping the participants to identify their own rules through an exploration of their family and interpersonal relationships. Clinical experience and a literature review both suggest that Chinese people have many family and interpersonal relationship rules that can become a potential source of stress [16]. For example, Chinese mothers may hold the belief that “It is my responsibility to take care of my child, particularly the disabled one, from cradle to grave”.
Each group comprised ten sessions, with each session lasting three hours. In the main the content was modified from the content of a Chinese CBT group manual developed by D.F.K. Wong for Chinese people with depressive symptoms [17]. In the first session the participants were helped to understand the patterns of their physiological, cognitive, behavioural, and emotional responses to external stressful life events. The second and third sessions aimed to help the participants to understand their own types of negative automatic thought patterns (i.e. cognitive distortions) and dysfunctional coping behaviour in relation to their depressed mood. We categorized these negative automatic thoughts into nine types and collectively called them ‘thought traps’. In sessions four and five the participants learned various cognitive and behavioural strategies to manage their depressed mood. We introduced five cognitive and behavioural strategies for managing depressed emotions, which we collectively termed the ‘five strategies’. These included (i) recognizing one's specific physiological responses (i.e. alarm signals), (ii) thought stopping, (iii) disputing questions (e.g. What is the worst that can happen? What evidence is there to support this idea?), (iv) distraction, and (v) positive self-statements and cue cards. In the fourth to ninth sessions the participants were encouraged to come up with a pleasurable activity that they would try to accomplish during the coming week. As parents with children with developmental disabilities tend to spend a great deal of time taking care of their disabled children, this exercise was part of a strategy to help the participants to learn to attend to their own needs and to develop a more balanced social life.
The sixth session focused on helping the participants to understand their dysfunctional attitudes, rules, and values by asking them to identify and examine how these rules and values might place too much expectation on themselves and others. Culturally relevant values and rules such as ‘It is shameful to have a child with a disability’, ‘As a mother, it is my sole responsibility to take care of my disabled child’, and ‘It is a family responsibility to take care of disabled children, from cradle to grave’ were brought up and discussed by the participants. In the seventh and eighth sessions the participants were introduced to various strategies for challenging and modifying their dysfunctional rules and values, such as the cognitive continuum, identifying the advantages and disadvantages of holding on to rules, and behavioural experimentation. The participants were also encouraged to learn to apply these techniques both during and outside of the group sessions. In the ninth session the participants had the opportunity to examine their priorities in life through an activity called ‘the auction game, the game of life’. Essentially, the participants were given one million dollars. They were asked to put the million dollars into 9 domain of life activities (e.g. having more friends and spending more time with families) according to individual preference. They then went on an auction. Whoever put the highest bid in a certain life activity would win the item. This was followed by a discussion to let the participants talk about their life priorities. They were also encouraged to set short- and long-term goals to work towards their new priorities. In the final session the participants were asked to recount and capitalize on their group experiences.
It is worth noting that the group session content did not focus on helping parents to develop coping skills to manage their children's behavioural and emotional issues. We made this decision because there are already many skills training programmes that have been developed to help parents to acquire these skills. Through the CBT group treatment, we aimed to promote the message that parents with disabled children ought to attend to their own needs as well as the needs of their children. This is particularly relevant for Chinese parents, who are culturally more inclined to engage in self-sacrificing behaviour for their children. According to Phillips and Xiong, most Chinese people consider ‘self-sacrificing and devoted behaviour’ the responsibility of parents with ill children, particular when the children are young or unmarried adults [18]. Another reason for not choosing to focus on coping skills training for parents was that our clinical practice suggests that although parents may learn the necessary coping skills, they are often unable to effectively apply them because they are overwhelmed by their emotions when trying to manage their children's behavioural and emotional problems. Unless they can develop skills to manage their own emotions, they will continue to feel frustrated by their seeming lack of ability to handle their children's problems.
Procedure
Each participant was asked to fill out a questionnaire at the beginning and end of the treatment. A structured CBT group was designed and run for the participants in the experimental group between the times of measurement, whereas no treatment was given to the participants in the control group. Three CBT treatment groups were run between October 2008 and September 2009. Each group comprised 10 sessions and was attended by 9 to 10 participants. The individuals in the control group were asked to fill out a questionnaire at around the same times as the participants of the experimental group (the beginning and end of the treatment), and were given group treatment after the study had finished.
The three group leaders were two experienced mental health social workers and a clinical psychologist. One of them was a member of the teaching staff of a university and was a qualified cognitive therapist trained at the Beck Institute. Two independent observers reviewed the videotapes from sessions 2, 6, and 8 of a randomly selected experimental group. The content of the three sessions revolved around ‘understanding the relationships among cognitive, behavioural, physiological, and emotional responses’ (session 2) and ‘identifying and modifying dysfunctional rules’ (sessions 6 and 8). As the group content was written up in a manual, it was easy for the research team to develop a checklist of the tasks to be completed in the three sessions. The two reviewers were asked to check each of the items on the checklist to see whether the group leaders had completed the prescribed tasks. There was no disagreement between the two reviewers over the tasks to be completed by the group leaders.
Instruments
General Health Questionnaire-12 (GHQ-12)
The General Health Questionnaire-12 (GHQ-12) is a commonly used screening instrument. It detects a wide range of psychological disorders, mainly on the anxiety/depression spectrum, and has been shown to be a valid and reliable instrument across cultures [19]. For this study the Chinese version of the GHQ-12 was employed to measure the mental health outcomes of the participants. The GHQ-12 rates the frequency of occurrence of distress symptoms. A decrease or increase in the mean scores between pre-treatment and post-treatment signifies a worsening or improving, respectively, of a person's mental health. The GHQ-12 (0-0-1-1) method was also used to classify the participants into at-risk or not at-risk cases. As different studies have recommended different cut-off scores ranging from 2/3 to 3/4 [20–22], we decided to adopt 4 as the cut-off score, with individuals registering four or more symptoms being classified as having poor mental health and being at risk of developing mental health problem. In this study the scale achieved a high level of internal consistency, with a Cronbach's alpha of 0.91.
Parenting Stress Index – Parent Domain
The Parenting Stress Index aims to tap the sources of difficulties and the level of parenting stress experienced by parents [23]. The scale is divided into the parent domain and the child domain. The parent domain examines the perceived social and psychological costs of parenting, and includes sub-scales such as feelings of attachment, depression, restriction of roles, sense of competence, social isolation, relationship with spouse, and parent health. The child domain attempts to explore parents’ perceptions of stress stemming from the demands of the child, and includes the sub-scales of child adaptability, acceptability, demandingness, moodiness, distractibility, and reinforcement by the parent. In this study four of the subscales in the parent domain were adopted: restrictions of roles (7 items), sense of competence (13 items), social isolation (6 items), and relationship with spouse (7 items). The content of the other three subscales appeared to be similar to that of other instruments such as the GHQ-12 and Q-LES-Q-18, and were thus not included. The Index is measured on a five-point Likert scale, where 1 denotes ‘strongly agree’ and 5 ‘strongly disagree’. It is assumed that the higher a person's score, the greater his or her disagreement with the statement. The scale has been translated and used among Chinese populations, and has shown good validity and reliability [24]. In this study, the Cronbach's alpha of the instrument was 0.84.
Abbreviated Quality of Life Enjoyment and Satisfaction Questionnaire (Q-LES-Q-18)
This scale was developed by Endicott et al. and later validated for use among schizophrenic, schizoaffective, and mood disordered patients [25]. The scale attempts to tap the level of life satisfaction of a person in the five dimensions of physical health, subjective feelings, leisure activities, social relationships, and medication. The scale has been translated and used among Chinese populations [13]. It is a five-point scale where 1 denotes not at all and 5 all the time. It is assumed that the higher a person's total score, the greater his or her satisfaction. The scale and its subscales achieved a high internal consistency in this study, with Cronbach's alpha of 0.82 for the total scale, 0.7 for physical health, 0.71 for subjective feelings, 0.73 for leisure activities, and 0.78 for social relationships. The medication subscale had only one item and no reliability test was performed.
Dysfunctional Attitude Scale (DAS)
The 40-item Form A version of the Dysfunctional Attitude Scale (DAS-A) was adopted and translated from Weissman and Beck's original scale [26] for use in this study. The scale attempts to tap dysfunctional beliefs, and is supposed to reflect the content of a person's cognitive schema [27]. It is assumed that the fewer dysfunctional beliefs that a person holds, the more functional that person's cognitive processes. The scale achieved a high level of internal consistency in this study (Cronbach's alpha = 0.9).
Data analyses were conducted for all of the participants who completed the treatment or the waiting period. The differences between the treatment and control groups were examined by using analysis of covariance (ANCOVA) with the pre-treatment score of each outcome measure being treated as the covariate so that the post-group outcome could be adjusted with respect to the baseline severity. The effect sizes were calculated using Cohen's d (the difference between the adjusted means divided by the pooled standard deviation) to examine the size of the differences between the experimental and control groups at post-treatment [28]. To examine the clinical significance of the study we adopted a cut-off score of 4 on the GHQ-12 to identify at-risk and not at-risk participants at post-treatment. Essentially, those participants who had four or more symptoms were classified as having poor mental health and to be at risk of developing mental health problems. Finally, regression analyses were performed to examine the relationship between the DAS scores and the GHQ-12 and Q-LES-Q-18 scores for both groups.
Results
The mean age of the participants was 47 years, and ranged from 37 to 60 years. About 95% (n = 55) were female, 81% were married (n = 47), and 19% were separated or divorced. About 40% had a college or university education, and 53% had a secondary education. Over 88% of the participants were housewives, and the rest were unemployed, retired, or had part-time jobs. About 12% of the participants had consulted a psychiatrist in the six months before the pre-group interview, and 9% were on medication. Unfortunately, the study did not ask for details of their psychiatric diagnoses or medication. About 57% of the participants came from mainland China, 17% were from Hong Kong, and 22.4% were from south-east Asian countries such as Singapore, Malaysia, and Vietnam. About half of the participants had an annual family income below the range of AU$20,000 to AU$30,000. Over 72% had one to two children, and about 64% of the children were below the age of 11. There were more male than female children, and over 80% had autism or autism and learning difficulties. The rest of the children had learning difficulties, speech delay, anxiety disorders, or ADHD.
The demographic data of the experimental and control groups were compared using analyses of variance (ANOVAs) for the continuous variables and Chi-squared tests for the categorical variables. The analyses found no significant differences between the experimental and control groups for any of the demographic variables (all p >0.3), indicating that the two groups shared similar characteristics before treatment began for the experimental group. ANOVAs were also used to compare the pre-treatment scores for the dependent variables between the experimental and control groups. Again, no significant differences were found between the two groups (all p > 0.3). Three participants dropped out of the study. One dropped out of the control group because she could not arrange childcare (n = 1). The other two attended the first few sessions of the treatment group and decided to discontinue because they did not feel comfortable sharing in the group setting (n = 2). This left 58 participants who completed the post-treatment questionnaire, 29 of whom were in the experimental group and 29 in the control group. Of the 29 participants in the experimental group, all completed at least eight group sessions.
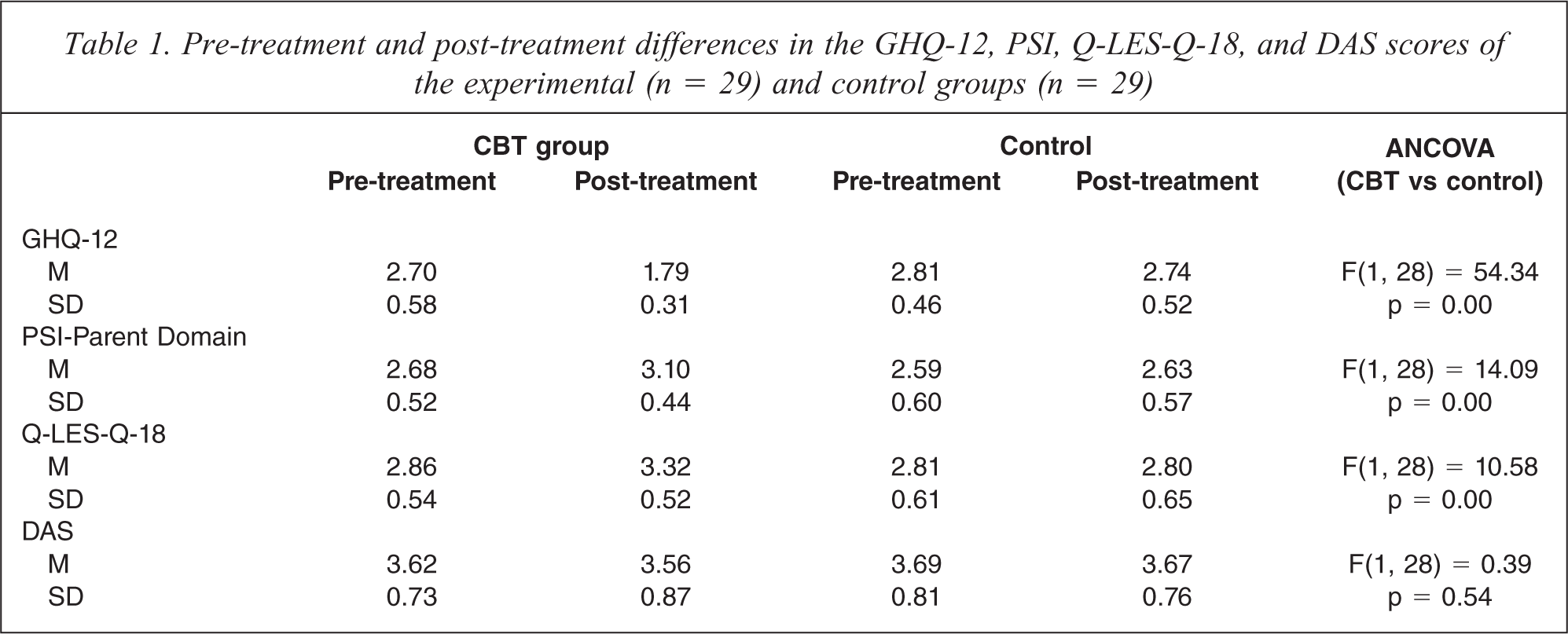
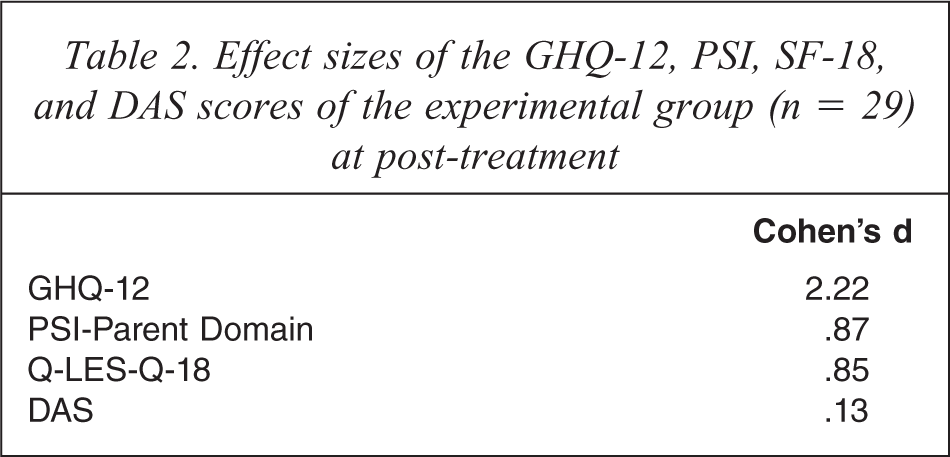
Table 1 presents the pre-treatment and post-treatment results for the experimental and control groups. The ANCOVAs show that there were significant between-group differences in the GHQ-12 (F(1, 28) = 54.34, p = 0.00), PSI-Parent Domain (F(1, 28) = 14.09, p = 0.00), and Q-LES-Q-18 (F(1, 28) = 10.58, p = 0.00) scores, but not in the DAS (F(1, 28) = 0.39, p = 0.54) scores. Compared with the control group, the experimental group showed significant improvements in general mental health, quality of life, and parenting stress. Slight improvements in dysfunctional attitudes were also noted among the participants in the experimental group at post-treatment, and between the participants of the experimental and control groups. The effect size statistics using Cohen's d (Cohen, 1988) revealed large differences in the GHQ-12 (Cohen's d = 2.22), PSI-Parent Domain (Cohen's d = 0.87), and Q-LES-Q-18 (Cohen's d = 0.85) scores between the participants of the experimental and control groups at post-treatment (Table 2).
Pre-treatment and post-treatment differences in the GHQ-12, PSI, Q-LES-Q-18, and DAS scores of the experimental (n = 29) and control groups (n = 29)
Effect sizes of the GHQ-12, PSI, SF-18, and DAS scores of the experimental group (n = 29) at post-treatment
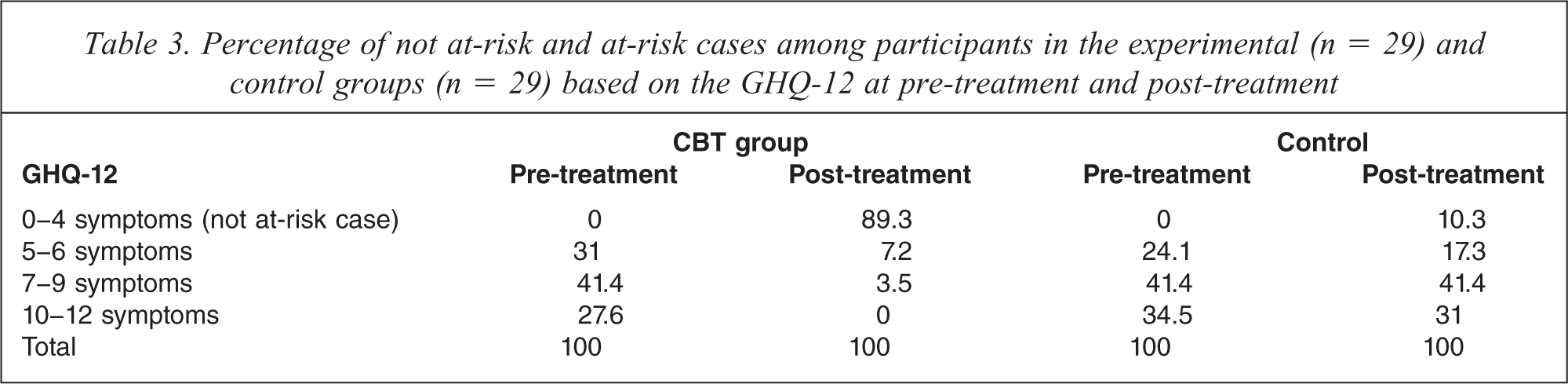
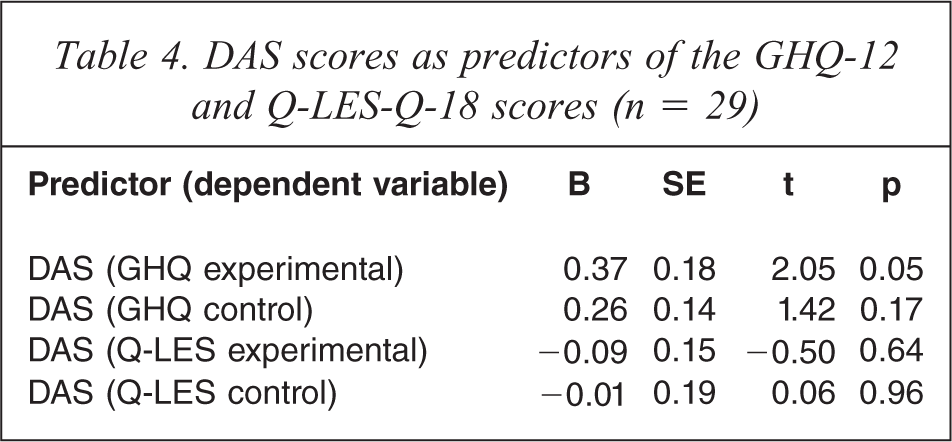
Based on the cut-off score of 4 on the GHQ-12 to identify at-risk cases and not at-risk cases, about 89% and 10% of the participants in the experimental and control groups, respectively, were classified as not at-risk at post-treatment (GHQ-12 = <4) (see Table 3). These figures contrast markedly with those taken at pre-treatment when all of the participants were classified as at-risk cases so that they met the selection criteria to participate in the CBT groups (GHQ-12 = >4). Regression analyses were performed to establish the link between changes in the DAS scores and the GHQ-12 and Q-LES-Q-18 scores. The results suggest that changes in the DAS only predicted changes in the GHQ-12 in the experimental group (Table 4).
Percentage of not at-risk and at-risk cases among participants in the experimental (n = 29) and control groups (n = 29) based on the GHQ-12 at pre-treatment and post-treatment
DAS scores as predictors of the GHQ-12 and Q-LES-Q-18 scores (n = 29)
Discussion
The participants in the experimental group showed a substantial decrease in parenting stress and improvement in mental health and quality of life compared with the participants in the control group at the end of the treatment. It is also fairly impressive that as many as 89% of the participants in the experimental group were not at-risk cases at post-treatment, whereas only 10% were not at risk in the control group. The results of this study provide preliminary support for the efficacy of our CBT group for Chinese parents with children with developmental disabilities in Melbourne, Australia. A substantial proportion of the content of the treatment groups focused on helping the participants to identify, challenge, and modify their negative automatic thoughts and dysfunctional rules and assumptions that might be associated with heightened levels of parenting stress. By changing these negative thought patterns it is possible that the participants acquired a more positive attitude toward themselves and their role in taking care of their children. The development of a Chinese group manual that contained group exercise worksheets, homework worksheets, and easy text extracts, and the translation of CBT terminology into colloquial Chinese expressions (in both Cantonese and Mandarin) may have helped the participants to understand their own patterns of negative automatic thought and dysfunctional attitudes much more easily. However, the positive changes in parenting stress, mental health, and quality of life among the participants in the experimental group may also have been due to the group effect, in that the participants were able to express their emotions and found support from the other participants in the group and felt less stressed as a consequence. Future research should include a control condition that eliminates the non-specific effects of contact with other group participants, such as the introduction of a social group, in the research design.
The positive outcomes of this CBT group for Chinese parents in Melbourne may also have been influenced by the mediating effect of the level of acculturation of the participants. Simply put, Chinese parents who have lived in Australia for a certain length of time may be more receptive to psychotherapy, whereas those recently arrived from China or living in China, for examples, might not benefit in the same way from this CBT group treatment, as they might not be as readily open to psychotherapeutic treatments. As we did not ask the participants in this study to give us information about their duration of residence in Melbourne, it was not possible to test this hypothesis. Further investigation concerning the mediating effect of acculturation in cross-cultural clinical trials should thus be conducted to clarify this issue.
There was no significant difference in the DAS scores of the participants in the experimental and control groups. However, a modest improvement was noted in the DAS scores of the participants of the experimental group between pre-treatment and post-treatment. There are two possible reasons for this result. First, it may be genuinely the case that the participants failed to experience a marked improvement in dysfunctional attitudes, rules, and values. Given that a person's dysfunctional attitudes, rules, and values have been formulated through many years of life experience and become rather entrenched, it is reasonable to assume that it would take more than a few group sessions for a person to be able to examine and relax his or her rigid dysfunctional attitudes, rules, and values. Another plausible explanation is that a generic scale such as the DAS may not be sufficiently sensitive to tap the specific dysfunctional attitudes, rules, and values associated with parenting children with development disabilities. Indeed, a careful look at the items in the PSI-Parent Domain reveals that several of the items pertain to attitudes toward parenting, and that the scores of the participants in the experimental group for these items had changed significantly at post-treatment. Examples of these items are ‘I expected to have closer and warmer feelings for my child than I do and this bothers me', and ‘When I think about the kind of parent I am, I often feel guilty or bad about myself’. As parenting attitudes, rules, and values are situation-specific and culture-specific, there is a need to develop or adopt a more culturally sensitive scale for parenting attitudes and values to measure specific cognitive changes associated with Chinese parents with children with developmental disabilities.
Our findings suggest that changes in the DAS scores only predicted changes in the GHQ-12 scores for the experimental group. This result echoes the findings of other studies conducted by DeRubeis et al. and Lamberton and Oei [29,30]. One of the therapeutic goals of CBT is to help participants to examine and relax their dysfunctional attitudes so that they can place more realistic demands on themselves, their children, and others in the family. The present CBT programme attempted to help participants to acquire an attitude of letting go of certain things that they could not change and to learn to place realistic demands on themselves and others. During the treatment process a substantial proportion of the group content focused on helping participants to identify, challenge, and modify their dysfunctional rules and assumptions. Through these activities the participants may well have achieved better self-acceptance and may have improved their interpersonal relationships with others. It is thus unsurprising that changes in dysfunctional attitudes, values, and rules can bring about a reduction in mental health symptoms.
Researchers such as Jacobsen and Gortner and Oei et al. have raised the argument that cognitive therapy may not be the primary change agent in reducing mental health symptoms, and that an identified reduction in symptoms may be the result of receiving positive reinforcement from the environment [31,32]. In addition, as Oei et al. suggest, positive post-therapeutic changes may also depend on certain non-specific factors such as the effect of the therapist's communication skills or support from other members if the treatment is delivered in a group format [32]. Indeed, the current literature offers mixed results on the causal relationship between cognition and emotion, and appears to suggest a bidirectional relationship between the two variables [32]. Further studies are clearly needed to examine the nature of the relationship between changes in cognitive processes and changes in depressive symptoms among Chinese people with mental health symptoms.
This study has several major limitations. First, it did not measure the longer-term effect of CBT for Chinese parents with children with developmental disabilities. A follow-up study would be necessary to ascertain whether the effects of the CBT are maintained in this group of parents. Second, we cannot rule out the possibility that positive changes in the various measures may have been due to group effects such as emotional support and advice provided by others. To better ascertain the therapeutic values of the cognitive and behavioural skills taught in the CBT group, it would be useful to introduce a social group as a control condition in the study design. Finally, we introduced dysfunctional attitudes, rules and values as a cognitive process variable in this study. Although it may be the case that there is a need to adopt a more sensitive measure to tap parents’ dysfunctional attitudes, rules and values associated with the care of children with developmental disabilities, it is certain that there is room to introduce and test other process variables that may be associated with changes in the outcome variables for this group of parents. One such process variable that is widely used in the literature is parenting self-efficacy.
Conclusion
This study endeavoured to examine the efficacy of CBT groups for Chinese parents with children with developmental disabilities. The initial findings suggest that after ten weeks of treatments, the participants in our culturally attuned and structured CBT group displayed significant improvements in parenting stress, general mental health, and quality of life, whereas no significant changes in these measures were observed among the participants in the control group.
Footnotes
Acknowledgements