
Abstract
Objective:
Mental health disorders are a major health concern in older people and are associated with a higher risk of disability, frailty and early mortality. This study aimed to conduct a contemporary population-based assessment of the prevalence, trends and factors associated with mental health disorders in individuals who are living in permanent residential aged care (PRAC) in Australia.
Methods:
A retrospective cross-sectional study was conducted using national data from the Registry of Senior Australians, a national cohort of older Australians who had aged care eligibility assessment and entered PRAC between 2008 and 2016. Stepwise multivariate logistic regression modeling was applied to identify factors associated with mental health disorders.
Results:
Of 430,862 individuals included in this study, 57.8% had at least one mental health disorder. The prevalence of depression, phobia/anxiety and psychosis were as follows: 46.2% (95% confidence interval = [46.0%, 46.3%]), 14.9% (95% confidence interval = [14.8%, 15.0%]) and 9.7% (95% confidence interval = [9.6%, 9.8%]), respectively. The likelihood of having a mental health disorder was higher for those who were (adjusted odds ratio [95% confidence interval]) relatively younger, specifically for every 10-year increment in age, the odds of having mental health disorders was 44.0% lower (0.56, [0.55, 0.56]); female (1.33 [1.32, 1.35]); having increasing numbers of physical health comorbidities, 6–10 (1.26 [1.24, 1.29]) or 11–15 (1.48 [1.45, 1.51]) or more than 15 (1.64 [1.58, 1.71]) compared to people having less than five comorbidities; having limitations related to health care tasks (1.05 [1.04, 1.07]), meals (1.04 [1.02, 1.05]) or social and community participation (1.10 [1.08, 1.12]).
Conclusion:
The burden of mental health disorders in older Australians living in PRAC was high and individuals with these conditions tend to be younger, with several physical comorbidities and/or functional limitations. Understanding the profile of individuals with mental health disorders at entry into PRAC can be used as evidence for baseline resource allocation for this population and evaluation of future needs of mental health services.
Introduction
Mental health disorders are of major public health concern worldwide, contributing to 13–32% of the global diseases burden (Collins et al., 2011; Prince et al., 2007), 1.5 million suicides and 15–30 million suicidal attempts (Collins et al., 2011). The World Health Organization estimated that over 15% of adults, aged 60 and over, suffer from mental illness, and the rapidly growing older population has implications for providing appropriate care for this population (World Health Organization, 2019).
In the 2016–2017 financial year, 3.8 million (15%) of Australians were aged 65 years or over (Department of Health, Commonwealth of Australia, 2016) and this proportion is projected to increase to 8.7 million (22%) by 2056 and to 12.8 million (25%) by 2096 (Australian Institute of Health and Welfare [AIHW], 2018). Current estimates indicate that 7% of older Australians over 65 years are receiving aged care services at permanent residential aged care (PRAC) facilities, account for 41% of the hospitalisations in Australia, 48% of the days spent in hospital, utilise ambulance services at a much higher rate than younger people (Lowthian et al., 2011) and are at high risk of medical complications (Roughead et al., 2013).
Older people experience a higher level of psychological distress than the general population (Phongsavan et al., 2013) and they are more vulnerable to mental health disorders (Boorsma et al., 2012; Brown et al., 2014; Creighton et al., 2016; De Mendonca Lima and Ivbijaro, 2013; Soysal et al., 2017). Reduced cognition, having comorbid physical health problems, reduced activity, poor living conditions, loneliness, isolation from social networks, change in living arrangements and experiencing loss of family and friends are risk factors predisposing older people to a mental health disorder (Brown et al., 2014; Scott et al., 2016; Soysal et al., 2017; Steptoe et al., 2013) and many of these factors contribute to a reduced quality of life and poor health outcomes. For example, a feeling of social isolation increases the risk of mortality by 26% compared to people who have regular contact with families and friends (Steptoe et al., 2013). Equally, poor quality of life, poor physical health and polypharmacy are often considered to be consequences of poor mental health (Barnett et al., 2012). Having a mental health disorder affects an individual’s ability to carry out basic activities of daily living, exacerbates the negative consequences of physical medical illnesses and increases the use of health care resources (De Mendonca Lima and Ivbijaro, 2013). Multimorbidity (presence of multiple health conditions) is common in older people; thus, understanding the complex comorbidity profile of physical and mental health conditions in older people is important for providing appropriate care (Agustini et al., 2020).
There is growing recognition that an increasing number of older people with mental health conditions have poor access to mental health care and emotional support, and yet there is limited research concerning the long-term impact of living with a mental health disorder (De Mendonca Lima and Ivbijaro, 2013; Medicine et al., 2012; Ohrnberger et al., 2017). Thus, clarifying the pattern and risk factors of mental health disorders in older people is a first step to identify individuals who require intervention and determine where resources should be invested. Understanding the prevalence of mental health conditions in older people will help develop and inform mental health service provision in the aged care setting.
Using a population-based cohort of older Australians receiving aged care services, our study estimated the prevalence and individual factors associated with mental health disorders in older people living in a residential aged care setting. Our project aims to inform targeted mental health quality improvement initiatives in the aged care setting that can ultimately improve the lives of older Australians with mental illness.
Methods
Study setting, design and data sources
A retrospective cross-sectional study using data from the National Historical Cohort of the Registry of Senior Australians (ROSA) (Harrison et al., 2019; Inacio et al., 2019; Visvanathan et al., 2019) between 1 July 2008 and 30 June 2016 was conducted. ROSA is comprised of linked de-identified national data from the AIHW’s National Aged Care Data Clearinghouse, the Pharmaceutical Benefits Scheme (PBS) and the Medicare Benefits Schedule (MBS) datasets (Inacio et al., 2019). Specifically, this study used datasets from the Australian Commonwealth Aged Care Assessment Program (ACAP), Aged Care Funding Instrument (ACFI), residential aged care service details and PBS (AIHW, 2002; AIHW, Australian Government, 2016; Australian Government Department of Social Services, 2015). The ACAP dataset includes every assessment performed by an Aged Care Assessment Team (ACAT) when determining eligibility for aged care services in Australia. The ACAP dataset contains information on sociodemographic characteristics, activity limitations and health conditions, including mental health disorders of older people being assessed for aged care services. The ACFI dataset contains the needs assessment performed at PRAC when a person first enters into residential aged care and is used as a resource allocation tool. Health conditions in these datasets are coded using the ACAP health condition codes which can be mapped to the International Statistical Classifications of Disease (ICD) codes (Australian Consortium for Classification Development, 2017). The PBS dataset contains all medications for which the Australian Government provides a subsidy. Data in the PBS are captured using PBS item codes, which can be mapped to the Anatomical Therapeutic Chemical (ATC) Classification System to identify medication use according to their therapeutic characteristics (WHO Collaborating Centre for Drug Statistics Methodology, 2018).
Ethical approval for this study was obtained from the University of South Australia (ID: 200489), the AIHW Human Research Ethics committee (Ref.: EO2018-1-418) and South Australian Department for Health and Wellbeing Human Research Ethics Committee (HREC/18/SAH/90).
Study sample
The study sample comprised people aged 65 years and older who had an aged care eligibility assessment approval for and entered a PRAC between 1 July 2008 and 30 June 2016.
Definition of outcomes
The presence of at least one mental health disorder was the primary outcome of interest. This was defined as having at least one of the following conditions: depression, mood or affective disorders, psychosis or schizophrenia, phobia/anxiety disorder, nervous tension/stress, obsessive-compulsive disorder, somatoform disorders, intellectual and developmental disorders, mental retardation/intellectual disability, mental and behavioural disorders due to alcohol and other psychoactive substance use, or adult personality and behavioural disorders. These conditions were ascertained using health information collected at the time of the first aged care eligibility assessment using the ACAP dataset (AIHW, 2002), mental and behavioural disorders checklist at the time of entry into permanent residential care using the entry into care assessment from the ACFI dataset (Australian Government Department of Health and Ageing, 2013) or based on medication use history for mental health disorders within 6 months prior to their aged care eligibility assessment using the medication-based Rx-Risk-V Comorbidity Index (Pratt et al., 2018) (Supplementary Appendix A).
Covariates
Variables evaluated were age, sex, preferred language (English or other), country of birth (Australia or born overseas), marital status (never married, divorced, married/registered de facto, separated or widowed), state (SA, ACT, NSW, NT, QLD, TAS, VIC or WA), living arrangements (lives alone, with family or with other relatives) prior to PRAC, usual accommodation (private owned, temporary shelter, retirement village, hospital or other institution) prior to PRAC entry, carer availability prior to PRAC entry, carer co-residency status prior to PRAC, carer relation prior to PRAC, having an activity limitation (communication, domestic assistance, health care tasks, home maintenance, meals, movement activities, moving around places at/or away from home, self-care, transport or social and community participation), remoteness (major cities, inner regional, outer regional, remote or very remote) prior to PRAC, calendar year of entry in to PRAC (2008–2016), having comorbid physical health conditions (Supplementary Appendix A), number of comorbid physical health conditions (⩽5, 6–10, 11–15 or >15 conditions ascertained using the Rx-Risk-V, ACAT health conditions and ACFI health conditions) and frailty index score (0–0.3 or >0.30) (Khadka et al., 2020).
Statistical analysis
The prevalence of mental health disorders was calculated as the proportion (in percentage) of individuals who had a mental health disorder (any), depression, phobia/anxiety, psychosis or a combination of these disorders out of the total number of individuals in care. Prevalence and 95% confidence intervals (CIs) are reported. To identify factors associated with mental health disorders, logistic regression models were fitted using mental health disorders (yes, no), depression (yes, no), phobia/anxiety (yes, no), psychosis (yes, no) as outcome variables and covariates as exposures. Covariates that showed a statistically significant association with the outcome (alpha = 0.05) in the univariate analysis were selected to be included in the final multivariable logistic models. A stepwise variable selection was applied to identify covariates associated with mental health disorders and model fit was checked using the Akaike information criterion. To check multicollinearity, a correlation matrix was examined and a generalised variance-inflation factor below 5 was considered acceptable. Both adjusted and unadjusted odds ratios (ORs) and 95% CI were calculated. All tests were two-sided and alpha = 0.05 was considered statistically significant. The analysis was performed using R programming language version 3.5.1.
Sensitivity analysis
To evaluate whether the burden of mental health disorders varied by dementia status, we compared the disease prevalence between those with and without dementia. We also stratified our models to examine the role of dementia status as an effect modifier in the statistical associations of individuals characteristics with mental health disorders.
Results
Characteristics of individuals in PRAC
During the study period, 430,862 individuals entered PRAC. The mean (standard deviation [SD]) age of the cohort was 82.4 (7.0) years. The majority were female (61.9%), widowed (50.5%), born in Australia (69.5%), lived with family prior to aged care entry (48.4%), had a carer before entering care (81.6%), were residing in a privately owned or rental accommodation before entering care (85.1%) and had at least one activity limitation (98.4%). Forty-eight percent of the study participants had dementia (Table 1, Supplementary Table 1).
Prevalence of mental health disorders by sample characteristics: 2008–2016 (N = 430,862).
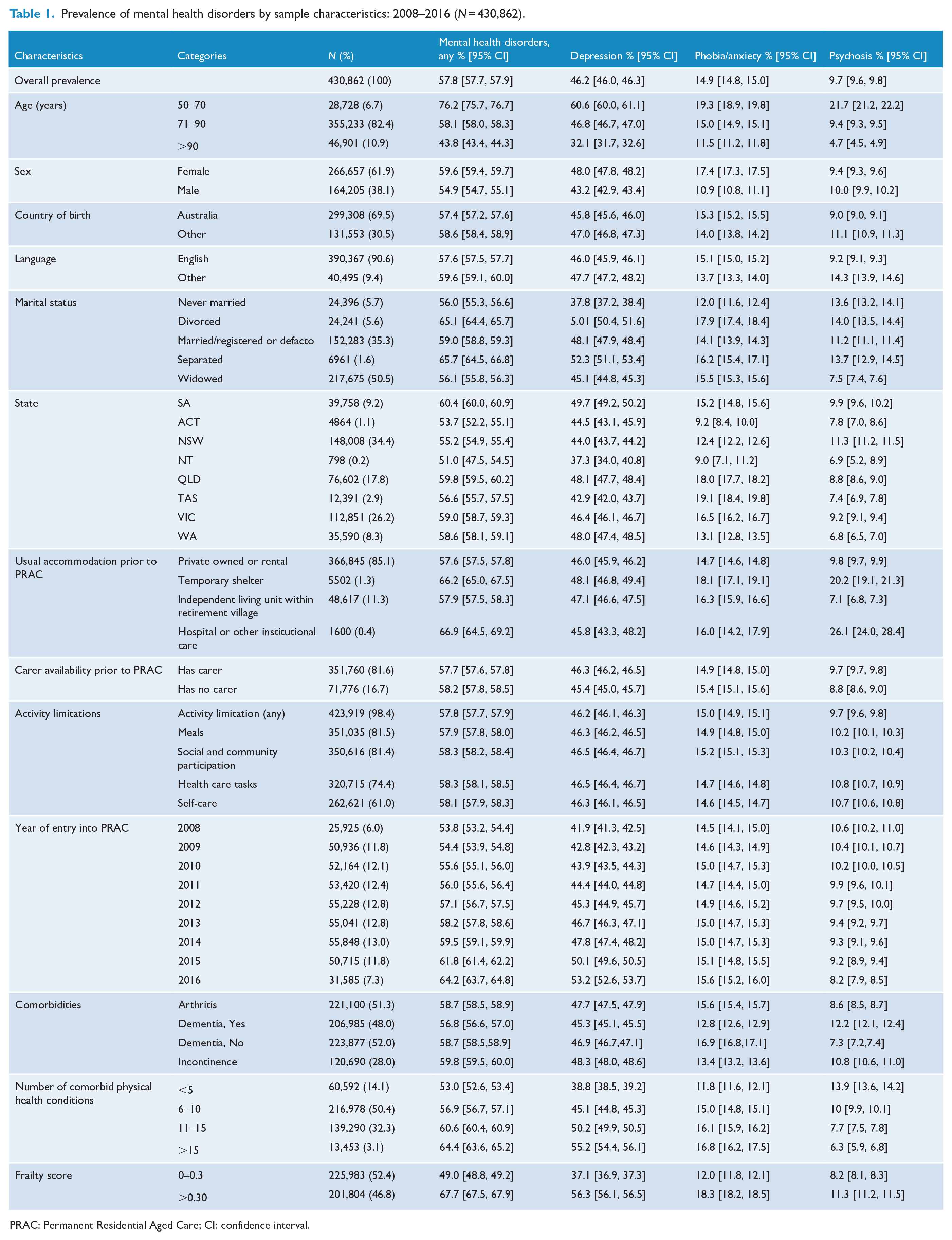
PRAC: Permanent Residential Aged Care; CI: confidence interval.
The prevalence of mental health disorders in PRAC
Of the 430,862 individuals in our cohort, 57.8% (95% CI = [57.7%, 57.9%]) had at least one mental health disorder. The most common mental health disorder was depression 46.2% (95% CI = [46.0%, 46.3%]), followed by phobia/anxiety 14.9% (95% CI = [14.8%, 15.0%]) and psychosis 9.7% (95% CI = [9.6%, 9.8%]). Of those with a mental health disorder, 10.2% (95% CI = [10.2%, 10.3%]) had both depression and phobia/anxiety, 6.8% (95% CI = [6.8%, 6.9%]) had both depression and psychosis, 2.4% (95% CI = [2.3%, 2.4%]) had phobia/anxiety and psychosis and 2.0% (95% CI = [1.9%, 2.0%]) had depression, phobia/anxiety and psychosis reported together. During the 8-year study period, the prevalence of mental health disorder increased significantly from 53.8% (95% CI = [53.2%, 54.4%]) in 2008 to 64.2% (95% CI = [63.7%, 64.8%]) in 2016. While the proportion of people with depression increased from 41.9% (95% CI = [41.3%, 42.5%]) in 2008 to 53.2% (95% CI = [52.6%, 53.7%]) in 2016, the prevalence of phobia/anxiety and psychosis remained constant during this period (Figure 1, Table 1, Supplementary Table 2).
Factors associated with the likelihood of having a mental health disorder in older Australians in permanent residential aged care.
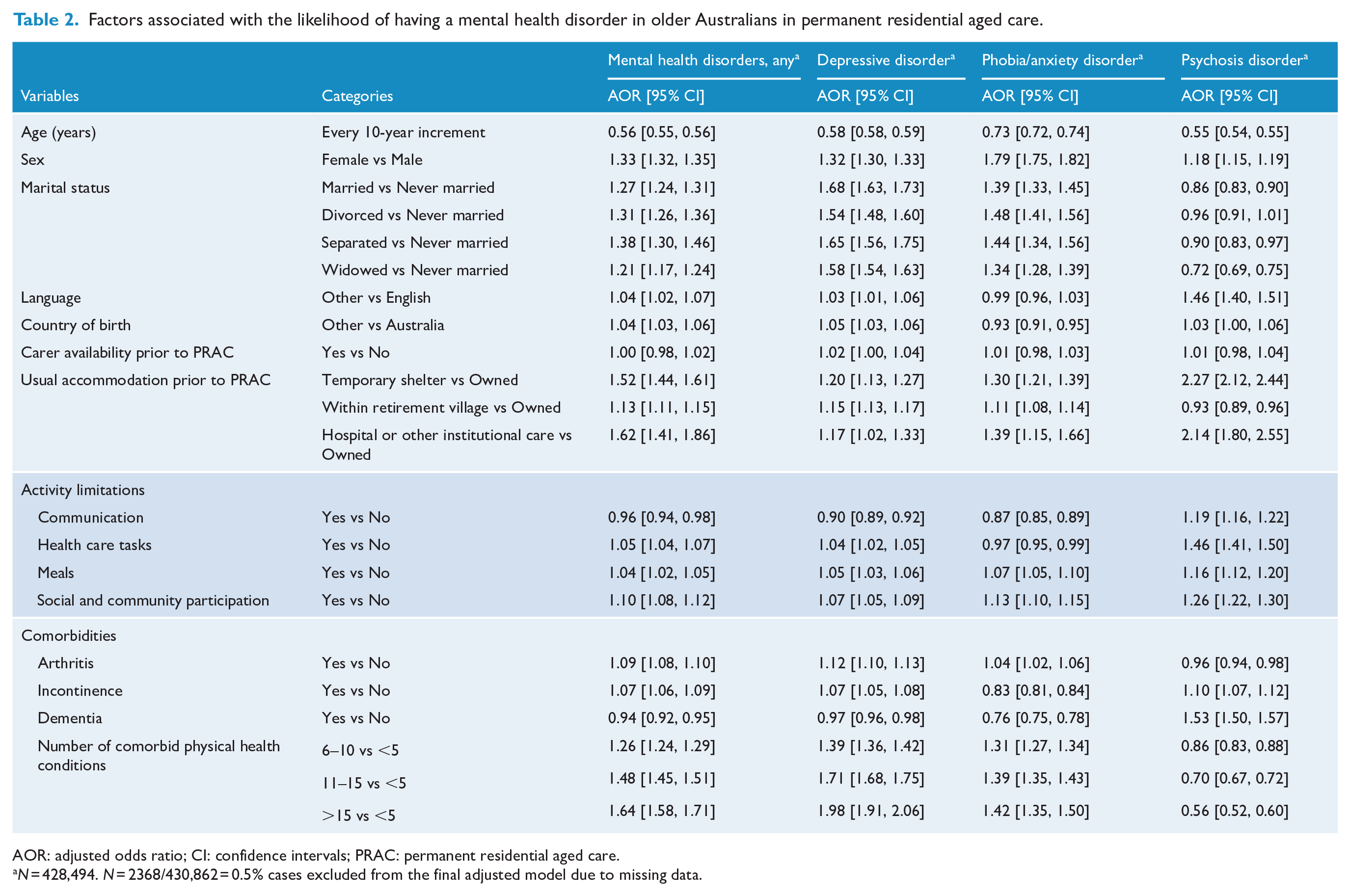
AOR: adjusted odds ratio; CI: confidence intervals; PRAC: permanent residential aged care.
N = 428,494. N = 2368/430,862 = 0.5% cases excluded from the final adjusted model due to missing data.
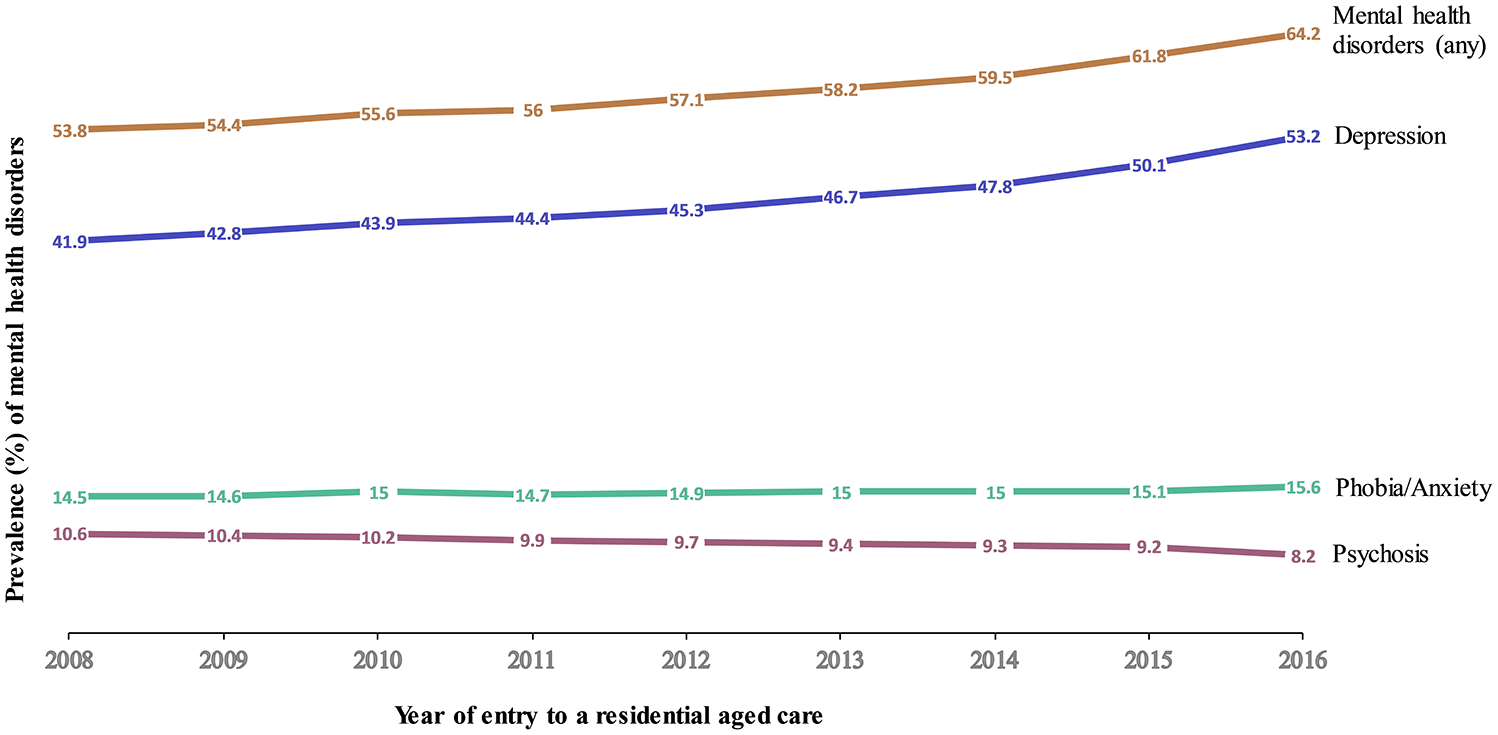
Prevalence and 95% confidence intervals of mental health disorders in older Australians living in permanent residential aged care between 2008 and 2016.
The prevalence of mental health disorders in those with physical health comorbidities or activity limitations
Of those individuals with a mental health disorder, 57.7% had physical health comorbidities.
Mental health conditions were reported most in individuals with musculoskeletal disorders 60.4% (95% CI = [60.1%, 60.8%]), incontinence 59.8% (95% CI = [59.5%, 60.0%]), arthritis 58.7% (95% CI = [58.5%, 58.9%]), diabetes 58.8% (95% CI = [58.5%, 59.2%]), malnutrition 58.5% (95% CI = [57.7%, 59.3%]), breathing difficulties 58.0% (95% CI = [57.3%, 58.7%]), falls 57.8% (95% CI = [57.5%, 58.1%]), injuries 57.7% (95% CI = [57.1%, 58.2%]), hypertension 57.6% (95% CI = [57.4%, 57.8%]) and dementia 56.8% (95% CI = [56.6%, 57.0%]) (Table 1 and Figure 2).
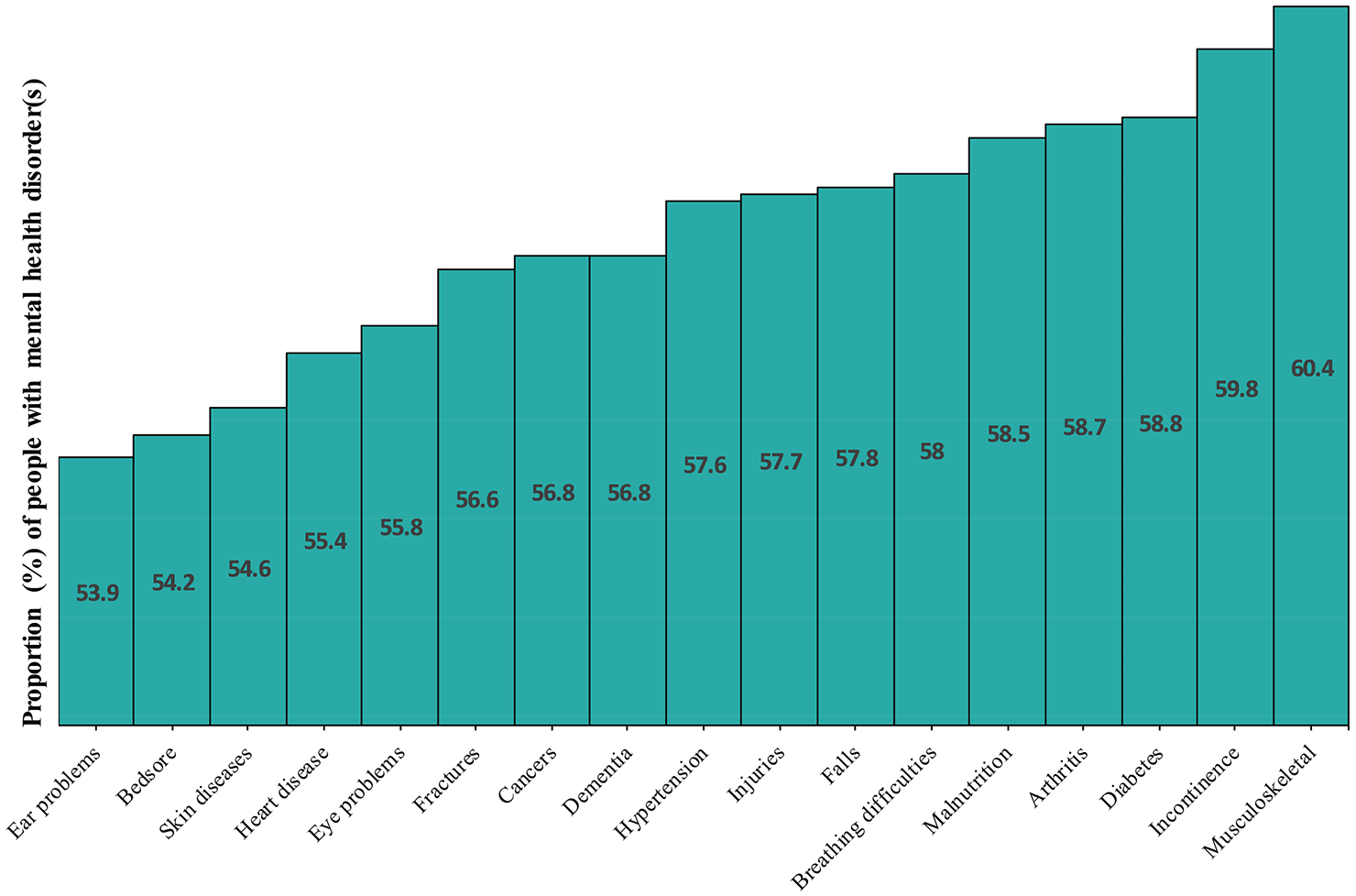
The prevalence of mental health disorders in those who had physical medical health conditions in older Australians living in permanent residential aged care between 2008 and 2016. In the x-axis are a list of top physical medical health conditions that are comorbid with mental health disorders (depressive disorder, phobia/anxiety disorder, psychosis disorder). The y-axis represents the proportion of people who had at least one of the common mental health disorders (depressive disorder, phobia/anxiety disorder, psychosis disorder) in those with physical medical health conditions.
Of the 423,919 (98.4%) people with an activity limitation, which includes limitation for communication, domestic assistance, health care tasks, home maintenance, meals, movement activities, moving around places, self-care, transport and/or social and/or community participation, 57.7% of them had at least one mental health disorder (Supplementary Table 2).
Factors associated with having a mental health disorder
Individuals who had mental health disorders were more likely to be (adjusted OR [95% CI]) younger, for every 10-year increment in age, the odds of having mental health disorders was 44.0% lower (0.56 [0.55, 0.56]); female (1.33 [1.32, 1.35]); married (1.27 [1.24, 1.31]), divorced (1.31 [1.26, 1.36]), separated (1.38 [1.30, 1.46]), widowed (1.21 [1.17, 1.24]) compared to being not married; speak languages other than English (1.04 [1.02, 1.07]); born overseas (1.04 [1.03, 1.06]); having 6–10 physical health comorbidities (1.26 [1.24, 1.29]) or 11–15 (1.48 [1.45, 1.51]) or more than 15 (1.64 [1.58, 1.71]) compared to people having less than five physical health comorbidities; having an activity limitation for health care tasks (1.05 [1.04, 1.07]), meals (1.04 [1.02, 1.05]) or social and community participation (1.10 [1.08, 1.12]). Individuals who had dementia were also less likely to report mental health disorders (0.94 [0.92, 0.95]). Table 2 provides details on the characteristics that were associated with depression, phobia/anxiety or psychosis.
Sensitivity analysis
In our cohort, the prevalence of mental health disorders (any), depressive disorder and phobia/anxiety disorder was slightly higher in individuals with no dementia compared to those who had dementia, with an estimated variation of 1.9%, 1.6%, 4.1%, respectively. For instance, the prevalence of overall mental health disorders in people with dementia versus in those with no dementia was 56.8% (95% CI = [56.6, 57.0]) and 58.7% (95% CI = [58.5, 58.9]), respectively (Table 1). The prevalence of psychosis in people with dementia in our cohort was 12.2% (95% CI = [12.1%, 12.4%]), which was higher than the prevalence in those without dementia 7.3% (95% CI = [7.2%, 7.4%]) (Table 1). This higher association of dementia with psychosis was also observed in the multivariable models (OR = 1.53, 95% CI = [1.50, 1.57]) (Table 2).
Moreover, we showed that dementia status was not an effect modifier of the association between the examined variables and mental health conditions. As shown in Supplementary Table 3, the association between the factors examined and mental health disorders was consistently similar between those with and without dementia. The only exceptions was for the association of marital status with psychosis and language with phobia/anxiety disorder. Specifically, individuals with psychosis and dementia were more likely to be married than not married (1.14 [1.06, 1.22]) while those with psychosis who had no dementia were less likely to be married (0.67 [0.63, 0.71]). Also, individuals with phobia/anxiety disorder and dementia were more likely to speak languages other than English (1.07 [1.02, 1.13]), while in individuals with phobia/anxiety disorder who had no dementia, this estimate was lower (0.91 [0.87, 0.96]) (Supplementary Table 3).
Discussion
In this comprehensive analysis of older individuals in Australia who live in PRAC facilities, the prevalence of mental health disorders was high, with 58% having at least one disorder. We have shown that the prevalence of mental health disorders has steadily increased over time from 53.8% in 2008 to 64.2% in 2016. Depression was the most commonly reported mental health disorder (46.2%), followed by phobia/anxiety (14.9%) and psychosis (9.7%). This estimate of mental health disorders in older Australians living in PRAC facilities is higher than the national 12-month and lifetime prevalence estimates, which were 20% and 45%, respectively, in Australians aged 16–85 years (The Australian Bureau of Statistics, 2007). Studies in other developed countries have also reported a high burden of mental health disorders, yet the current estimate for the Australian PRAC population was higher. For instance, in the United States, the prevalence of depression in newly admitted nursing home residents was 26% (Ulbricht et al., 2017), while the prevalence of the same disorder in older Australians in PRAC was 46.1%. A European-wide study, which involved older people aged 65–84 years from Germany, Italy, England, Spain, Switzerland and Israel, found a 47% lifetime prevalence of any mental health disorder (Andreas et al., 2017).
The higher burden of mental health disorders in people living in PRAC facilities may reflect the impact of age-related disease comorbidities, disabilities and a change in living environment on older people’s mental health wellbeing. It can also be anticipated that the overall number of older people with mental health disorders will continue to expand as the population is ageing, creating a challenge for the aged care system, given the lack of specific areas of focus on targeted interventions and the extensive care requirements of mental health disorders. Aged care oriented mental health services are, therefore, required to address the high burden of mental health disorders in older people.
Among several factors that we examined, age, sex, marital status and living conditions prior to residential aged care entry, having co-existing physical health conditions such as dementia or functional limitations, were associated with having a mental health disorder while living in PRAC. Studies in the general population report a consistent, higher likelihood of having a mental health disorder associated with ageing (Schaakxs et al., 2018) and within an older population, mental health problems were higher at an earlier age than later (Byers et al., 2010; McDougall et al., 2007). In our study cohort, a higher prevalence of mental health problems at an earlier age, around the time of entry to PRAC, partially reflects the mental health impact of moving into residential aged care facilities, and care providers should be aware of this period to make the transition more positive. Being placed into a new environment, leaving their homes, spouses and possessions may cause older people to experience grief, which may in turn likely contribute to or result in mental health illness (Coyle and Dugan, 2012; Domenech-Abella et al., 2017; Ong et al., 2016).
Women continue to carry a greater burden of mental health disorders even at an older age, and the gap in the burden of mental health disorders between women and men is significant. Consistent with findings from a general population (Kuehner, 2017; Seedat et al., 2009), our study found a 35% excess odds of having a mental health disorder in women compared to men.
While the burden of mental health disorders alone is substantial and complex, a significant proportion of the people with mental health disorders had co-existing physical health conditions, and/or activity limitations, and were using a large number of medicines. Over half of individuals with mental health disorders had at least one comorbid physical health condition, and one in every two individuals had six or more physical health conditions. The most common comorbid physical health conditions were musculoskeletal disorders excluding arthritis, incontinence, arthritis, diabetes, malnutrition, breathing difficulties, falls, injuries, hypertension and dementia. In general, the presence of co-existing physical health conditions was significantly associated with having a mental health disorder and as the number of co-existing physical health conditions increases, the odds of having a mental health disorder rises. This finding is consistent with previous epidemiological evidence that showed the association of mental health disorders with physical medical diseases (Barnett et al., 2012; Gum et al., 2009; McDougall et al., 2007) or polypharmacy (O’Connell et al., 2019; Qato et al., 2018). Unlike previous studies (Andreasen et al., 2013; Byers and Yaffe, 2011), our study found a lower risk of depression or phobia/anxiety associated with dementia. This might be due to several reasons. First, older people with dementia have a functional limitation on communication that could inhibit their ability to report symptoms related to depression or anxiety. Second, because older people with dementia have multiple chronic medical comorbidities, depression and anxiety may not be included in the list of diseases reported during individuals health assessment (Curran and Loi, 2013). Third, depression and anxiety may present differently in people with comorbid dementia, particularly when the dementia is at an advanced stage. In such conditions, the clinical symptoms of depression and anxiety might be hidden by psychotic symptoms (Curran and Loi, 2013). However, in our assessment of whether the presence of dementia was an effect modifier for the associations of individual characteristics with mental health disorders, we showed that most estimates were similar (indeed very close) for those with and without dementia.
This complex co-existence of physical and mental health disorders makes resource allocations challenging, as policymakers are often biased to addressing physical chronic diseases. Studies found that investing in mental health care and ensuring appropriate interventions has a substantial return by reducing disability, delaying the transition to high-level aged care packages and improving life expectancy (Chisholm et al., 2016; Rockwood, 2016). In older people with mental health disorders and co-existing physical health conditions, an integrated and holistic health care approach is appropriate. Maintaining a collaborative effort between aged care consumers/residents, aged care facilities and institutions providing mental health services could lead to better mental health outcomes. In addition, the quality and quantity of mental health services should be a major clinical and policy issue.
Implications of our findings
Without a clear understanding of the prevalence and factors associated with mental health disorders, it is challenging to design targeted effective interventions for this vulnerable population who require quality and timely care. Our study provides a comprehensive assessment of the prevalence and trends of mental health disorders and further investigated the factors associated with the disorders in a national cohort of older Australians. The results are of particular importance for policymakers, aged care providers and consumers, and the evidence presented here can be used to inform resource allocation regarding national mental health interventions in the aged care sector. This study has implications for future mental health research in the aged care sector by highlighting variations of disease prevalence across the different aged care services. For instance, the prevalence of depression in those receiving community care packages is 16% (Visvanathan et al., 2019); however, this estimate is tripled in individuals living in residential aged care. Thus, in the future, it is important to identify the critical period of change in disease prevalence and provide the right health interventions while older people are transiting across the different pathways in the aged care spectrum.
Strength and limitations of the study
This study captured the national cohort of individuals in Australia who accessed PRAC between 2008 and 2016, making our findings generalisable to older individuals accessing PRAC in Australia. We also have used three data sources, including two aged care assessments performed by trained assessors and individuals’ medication records, to ascertain the mental health conditions examined in this study. This ensures that our measure of mental health disorders was comprehensive and sensitive.
A limitation of this study is the observational nature of our data, from which causal inferences cannot be drawn. Because of our sample size, we have also reported statistically significant associations with small effect sizes, which may be considered clinically irrelevant; therefore, it is important to consider effect sizes while interpreting significant findings. We also recognise that our study relied on data collected for the purpose of aged care service eligibility assessment and resource allocation; therefore, our data could suffer from certain limitations. For instance, in individuals with dementia and/or other cognitive impairment, tools such as the Cornell scale, which involves direct observation of the individuals’ behaviour and interview with care providers to screen for depression (Snowdon et al., 2011), may be more appropriate. This could potentially have influenced the results of our study, which showed a lower risk of depression or anxiety in those individuals with dementia or functional limitations on communication. Although the Cornell scale has been used as part of permanent care assessments, 114,512 (26.6%) individuals did not complete this information and it is unknown whether it was because those individuals were too impaired to complete the assessment or did not have signs of mental health illness (Snowdon et al., 2011). In our study, we used a medication-based comorbidity index to ascertain the disease conditions examined. Antipsychotics are commonly used to manage the behavioural symptoms of dementia, and it is likely that some of the individuals in our cohort were classified as having psychosis when in fact these medications were used for the management of behavioural symptoms of dementia.
Conclusion
This population-based study of older Australians in PRAC showed that the prevalence of mental health disorders was high and has increased annually over the study period. Age, sex, activity limitations and having a high number of comorbid physical conditions were associated with the presence of mental health disorders. This has important implications for planning interventions to address mental health problems in the aged care setting. Thus, our results can be used as evidence for baseline resource allocation and evaluation of future mental health services. Future research is needed to investigate existing services and recommend optimal strategies for addressing mental health problems in the aged care setting.
Supplemental Material
Appendix_A_Supplementary_file – Supplemental material for The prevalence, trends and determinants of mental health disorders in older Australians living in permanent residential aged care: Implications for policy and quality of aged care services
Supplemental material, Appendix_A_Supplementary_file for The prevalence, trends and determinants of mental health disorders in older Australians living in permanent residential aged care: Implications for policy and quality of aged care services by Azmeraw T Amare, Gillian E Caughey, Craig Whitehead, Catherine E Lang, Sarah CE Bray, Megan Corlis, Renuka Visvanathan, Steve Wesselingh and Maria C Inacio in Australian & New Zealand Journal of Psychiatry
Supplemental Material
Supplementary_Table_1 – Supplemental material for The prevalence, trends and determinants of mental health disorders in older Australians living in permanent residential aged care: Implications for policy and quality of aged care services
Supplemental material, Supplementary_Table_1 for The prevalence, trends and determinants of mental health disorders in older Australians living in permanent residential aged care: Implications for policy and quality of aged care services by Azmeraw T Amare, Gillian E Caughey, Craig Whitehead, Catherine E Lang, Sarah CE Bray, Megan Corlis, Renuka Visvanathan, Steve Wesselingh and Maria C Inacio in Australian & New Zealand Journal of Psychiatry
Supplemental Material
Supplementary_Table_2 – Supplemental material for The prevalence, trends and determinants of mental health disorders in older Australians living in permanent residential aged care: Implications for policy and quality of aged care services
Supplemental material, Supplementary_Table_2 for The prevalence, trends and determinants of mental health disorders in older Australians living in permanent residential aged care: Implications for policy and quality of aged care services by Azmeraw T Amare, Gillian E Caughey, Craig Whitehead, Catherine E Lang, Sarah CE Bray, Megan Corlis, Renuka Visvanathan, Steve Wesselingh and Maria C Inacio in Australian & New Zealand Journal of Psychiatry
Supplemental Material
Supplementary_table_3 – Supplemental material for The prevalence, trends and determinants of mental health disorders in older Australians living in permanent residential aged care: Implications for policy and quality of aged care services
Supplemental material, Supplementary_table_3 for The prevalence, trends and determinants of mental health disorders in older Australians living in permanent residential aged care: Implications for policy and quality of aged care services by Azmeraw T Amare, Gillian E Caughey, Craig Whitehead, Catherine E Lang, Sarah CE Bray, Megan Corlis, Renuka Visvanathan, Steve Wesselingh and Maria C Inacio in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
We would like to acknowledge the Healthy Ageing Research Consortium Investigator Team and the ROSA’s South Australian Health and Medical Research Institute Research Team for ensuring the success of the ROSA and support with this study. We also acknowledge the South Australian Government who provide us with support (2017–2021) through the Department for Innovation and Skills, and the Australian Institute of Health and Welfare for the provision of the raw data used in ROSA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the South Australian Government Department for Innovation and Skills and the National Health and Medical Research Council Centre of Research Excellence Scheme – APP 1102208. Dr Amare has received 2020-2022 NARSAD Young Investigator Grant from the Brain & Behaviour Research Foundation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.