
Abstract
Objective
The COVID-19 pandemic required mental health clinicians globally to transition to the delivery of care via telehealth. This study aimed to gain an understanding of clients’ satisfaction with and attitudes towards telehealth mental health services.
Method
Seventy adults who had attended a clinic for mood and anxiety disorders, and participated in at least one telehealth consultation with a psychologist or psychiatrist, completed an anonymous online survey.
Results
The majority of participants (81.5%) reported satisfaction with telehealth mental health care provided during the COVID-19 pandemic. However, satisfaction overall was significantly higher amongst participants who had received both telehealth and face-to-face mental health care, compared to participants who received care via telehealth only. Advantages of telehealth care reported included convenience and increased access to mental health clinicians. However, disadvantages of telehealth care included greater difficulty developing a rapport with a clinician and expressing oneself via telehealth.
Conclusions
Whilst client satisfaction with telehealth mental health care for mood and anxiety disorders is generally high, clinicians should consider the limitations of telehealth from clients’ perspectives. In particular, strategies to enhance therapeutic connection during telehealth sessions may be needed, and client preferences for mode of delivery should be taken into consideration when possible.
Globally, mental health conditions are not only highly prevalent but also severely underserviced. 1 The COVID-19 pandemic not only led to an increase in anxiety and depressive disorders but also created a severe disruption to mental health services. 1 However, one opportunity that has arisen from the COVID-19 pandemic is the recognition of the potential role of telehealth to improve access to mental health care.2,3 In Australia, as with many other countries, mental health clinicians were required to rapidly transition to the delivery of services via telehealth.4,5 Worldwide, there is now increasing recognition of the need to understand how to best utilise telehealth for mental health services beyond the COVID-19 pandemic.
Several studies have described the experiences and attitudes of clinicians delivering telehealth mental health services.4,6 However, it is also important to gain an understanding of clients’ experiences and their satisfaction with and attitudes towards telehealth mental health services. For example, the limited research to date has identified that whilst client satisfaction with telehealth mental health services is high overall, those participating in video-conferencing were more likely to consider continuing remote treatment than those participating in telephone consultations. 7
This study aimed to explore the perspectives of clients of an outpatient clinic for mood and anxiety disorders regarding telehealth mental health care. Specifically, the study aimed to examine clients’ satisfaction with the care they received overall, and with telehealth services in particular. Clients’ perspectives of the advantages and disadvantages of both telehealth and face-to-face mental health care were also investigated.
Methods
Participants
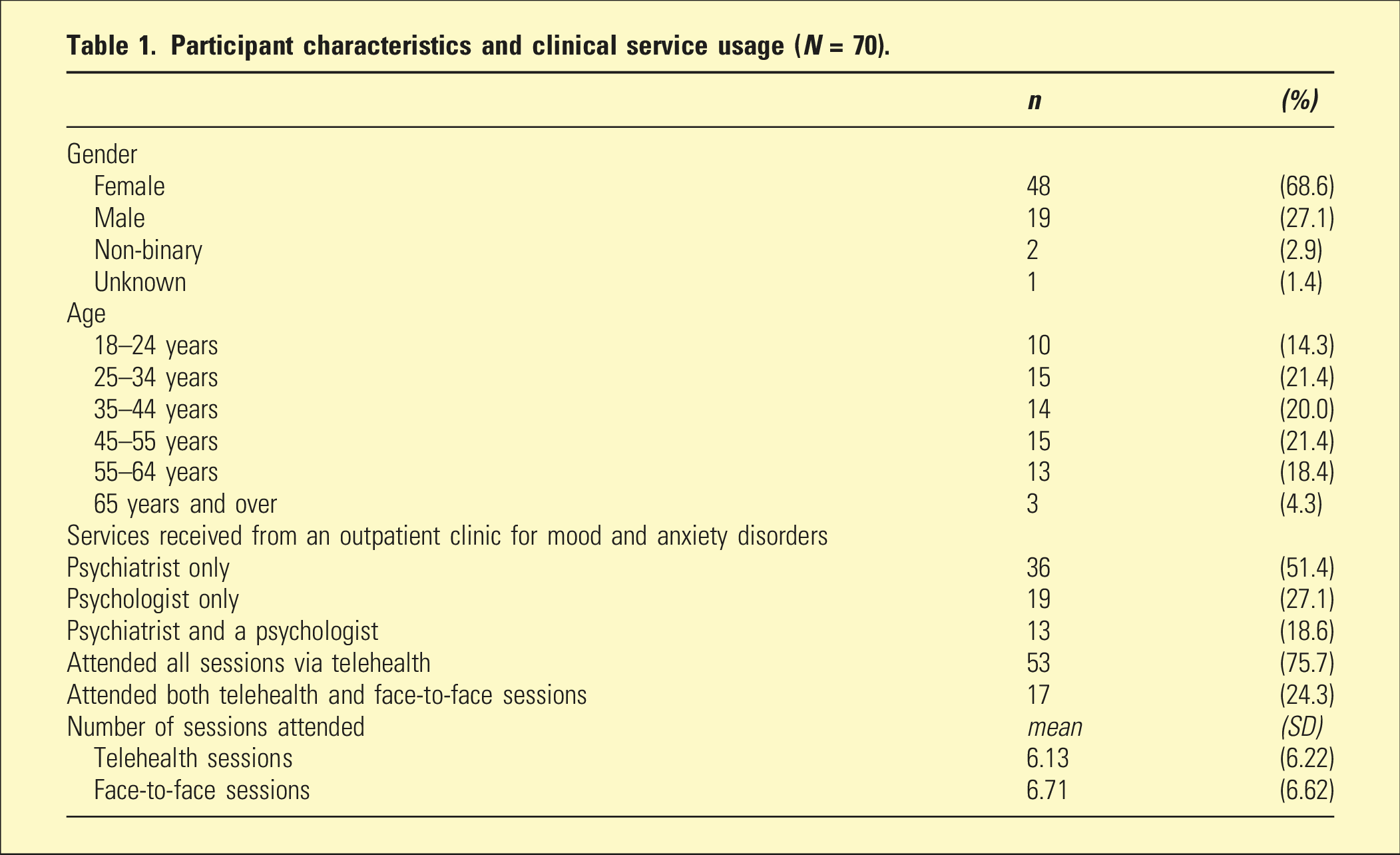
Participant characteristics and clinical service usage (N = 70).
Procedure
Data was collected in April 2022. Eight hundred and two adults who had attended the clinical service in 2020 or 2021 were emailed an invitation to participate in an anonymous online survey. The mixed-methods survey included measures of satisfaction and open-ended questions regarding telehealth and face-to-face mental health services. The sample of N = 70 participants included in analyses (who had attended at least one of their consultations via telehealth and completed measures of satisfaction) was thus 8.7% of past clients invited to complete the survey.
Measures
The survey included three measures of client satisfaction. Two were measures of overall satisfaction: (i) the Yes Survey 8 and (ii) the Client Satisfaction Questionnaire-8 (CSQ-8). 9 The third measure specifically assessed clients’ satisfaction with the telehealth mental health consultations they had received from the service: (iii) Telehealth Usability Questionnaire (TUQ). 10 The TUQ asks respondents to rate 21 items on a 7-point scale ranging from 1 (strongly disagree) to 7 (strongly agree). A response of 5 to 7 indicates an agreement with a statement. 10
The survey also included questions regarding demographics, the number of consultations with a psychiatrist and with a psychologist, the number of consultations via telehealth and via face-to-face and barriers to both telehealth and face-to-face mental health care. Open-ended questions in the survey asked participants about their experiences with telehealth and face-to-face mental health consultations with the service, including the advantages and disadvantages of both telehealth and face-to-face consultations.
Statistical analyses
Quantitative data were analysed using IBM SPSS program (version 24). Descriptive analyses and independent t-tests were conducted to examine for any differences in client satisfaction scores between clients who had telehealth sessions only and those who had both telehealth and face-to-face sessions. Statistical significance was defined as p < .05. The qualitative survey data was analysed using an inductive thematic analysis (i.e. allowing the data to determine the themes) with a semantic approach (i.e. analysing the explicit content).11,12 Two researchers independently conducted coding across the whole dataset and reviewed the data again once a structure of themes, sub-themes and codes was agreed upon. Any differences in categorisation were discussed until an agreement was reached.
Results
Satisfaction
Satisfaction scores in participants receiving mental health care via (i) telehealth only and (ii) telehealth and face-to-face.
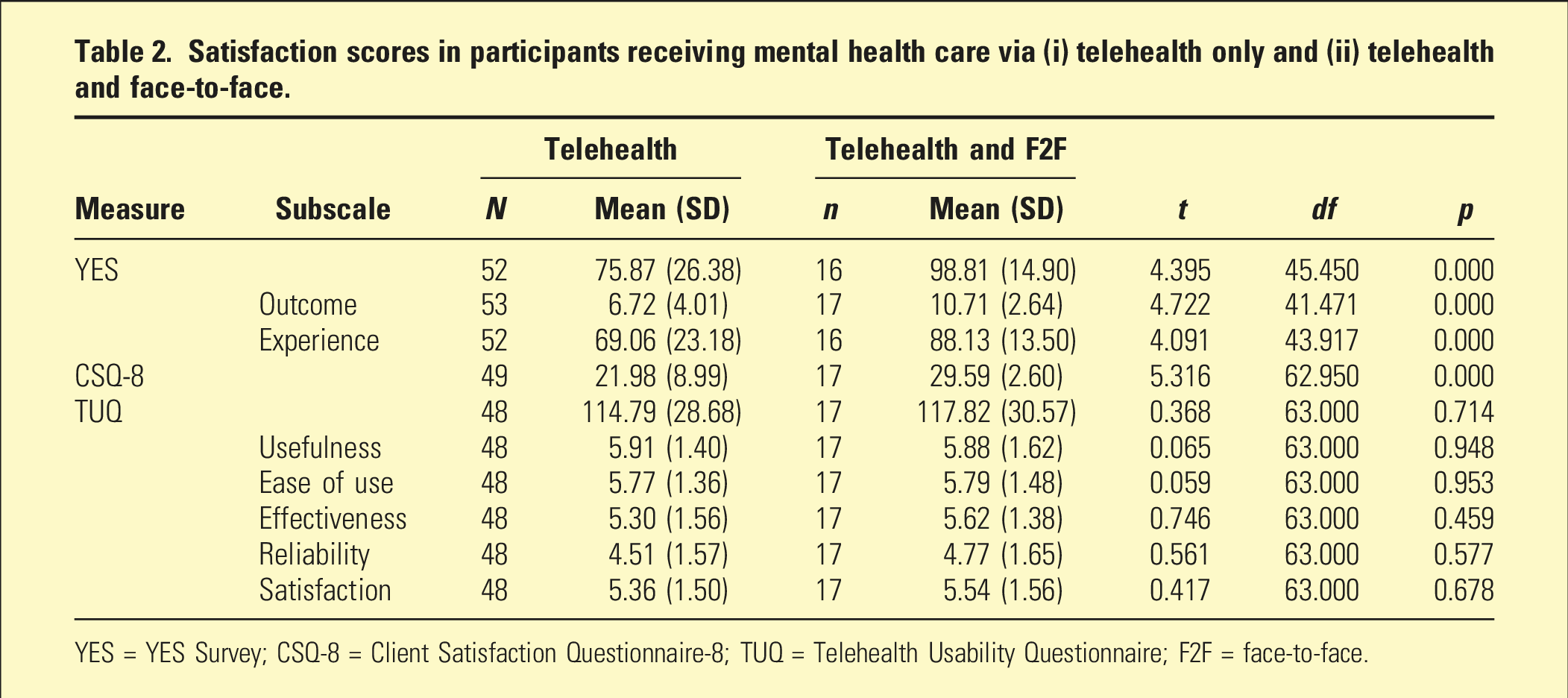
YES = YES Survey; CSQ-8 = Client Satisfaction Questionnaire-8; TUQ = Telehealth Usability Questionnaire; F2F = face-to-face.
On the TUQ, 81.5% of participants agreed that they were satisfied overall with the telehealth services provided by the mental health service and 80.0% reported that they would use such telehealth services again.
Barriers to telehealth and face-to-face mental health care
Barriers to telehealth and face-to-face mental health care.
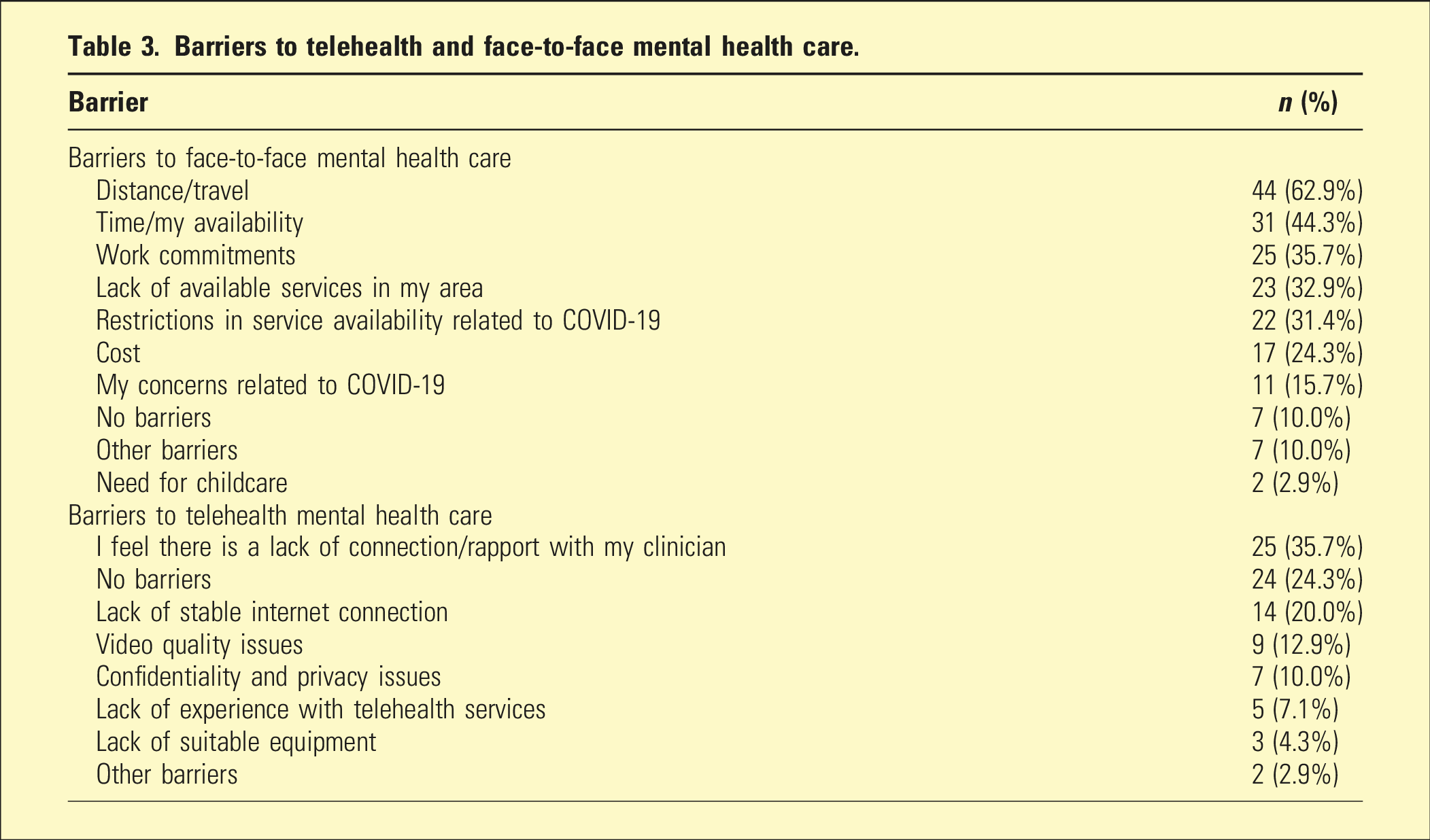
The most frequently reported barriers to face-to-face mental health care were distance/travel (reported by 62.9% of participants) and time (44.3%), whereas the most frequently reported barrier to telehealth mental health care was a feeling of a lack of connection or rapport with the clinician, which was reported by over a third (35.7%) of participants.
Qualitative results: Advantages of telehealth and face-to-face mental health services
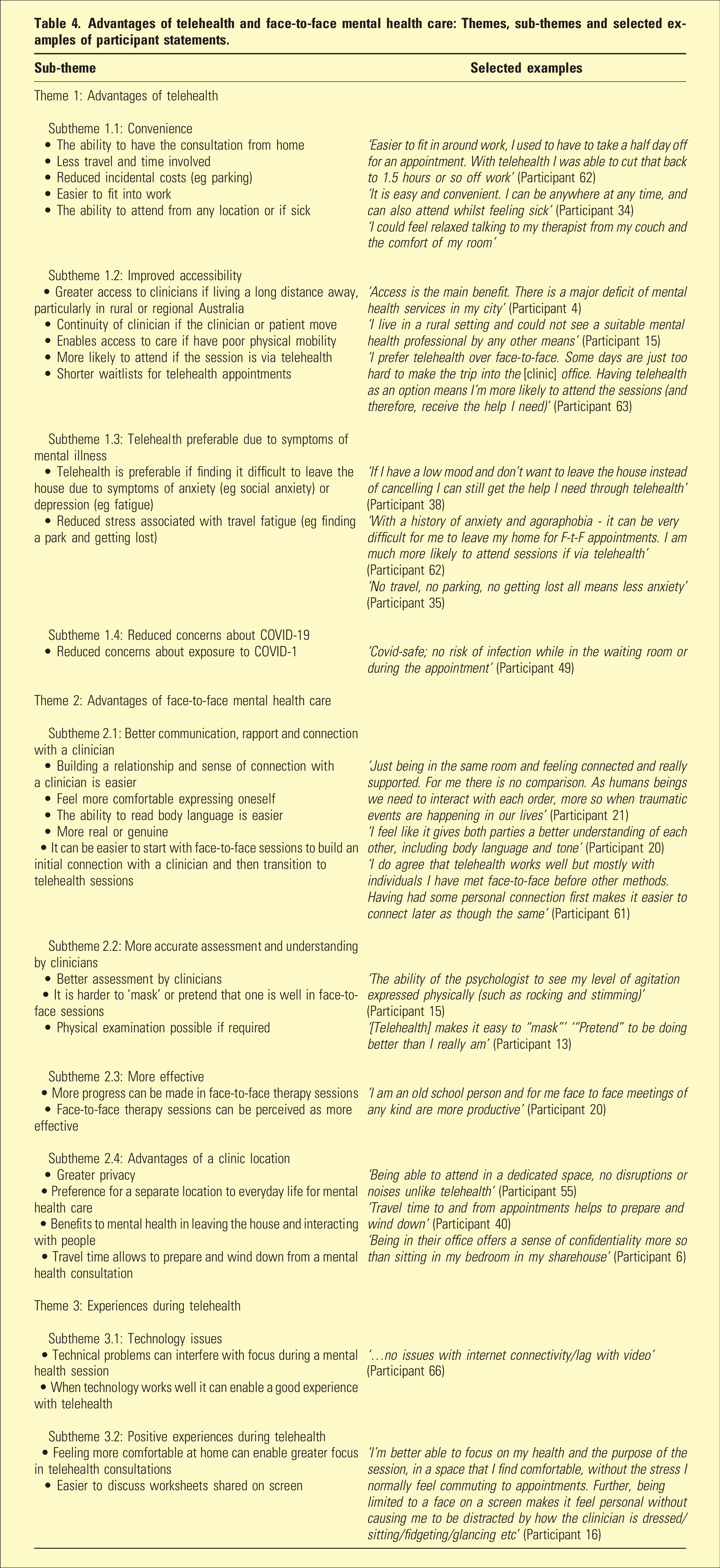
Advantages of telehealth and face-to-face mental health care: Themes, sub-themes and selected examples of participant statements.
Discussion
This study aimed to gain an understanding of clients’ satisfaction with and attitudes towards telehealth mental health services for mood and anxiety disorders. The findings have implications for the integration of telehealth into routine mental health care. Firstly, the majority (81.5%) of adult clients who completed the study survey reported satisfaction with telehealth delivery of mental health care during the COVID-19 pandemic. Importantly, for some participants, telehealth enabled them to access mental health care when they would not have been able to otherwise, due to geographical location, COVID-19 restrictions, or symptoms of mental illness.
However, satisfaction with clinical services received overall was significantly lower amongst participants who had received mental health care via telehealth only, compared to those who had received both face-to-face and telehealth care. Clinicians should be aware of the limitations of telehealth mental health care. In particular, many participants described greater difficulty developing a rapport with a clinician via telehealth, along with difficulties with expressing themselves and non-verbal communication. This is consistent with the observations of psychiatrists in Australia,13,14 as well as the findings of surveys of mental health professionals in Australia and New Zealand 4,15 and clients in the US. 7 For a small number of participants in our survey, this extended to a sense that less progress was made during telehealth therapy sessions.
The clinical implications are clear. In circumstances where a mixed mode of delivery is possible, it may be beneficial for initial mental health appointments to be face-to-face, in order for a client to develop a relationship with a new clinician. Further, the preferences of clients should be taken into account when possible. However, when telehealth delivery of mental health care is the only option, mental health clinicians should be mindful that it may take longer to develop a rapport with clients and for clients to feel comfortable expressing themselves. Strategies that clinicians may use to enhance therapeutic alliance when delivering mental health care via telehealth may include more regular check-ins with clients and consideration of voice and body language to convey empathy and understanding. 15
The limitations of this study should be noted. There was a possible bias in recall and reporting, given that participants completed the survey between 4 months and 2 years and 4 months after their sessions with the clinical service. This, along with the low survey response rate (of 8.7%), may have impacted the validity of the data. Nevertheless, these findings regarding client perspectives were consistent with previous reports of observations by mental health clinicians, as described above. It should also be noted that whilst our survey was conducted amongst adults with the most common mental health problems, depression and anxiety, it is not known if people with different mental illnesses would report different perspectives. For example, clients experiencing psychosis may report different needs. 16 Further, clients with different demographic characteristics may report different preferences. For example, Indigenous clients of mental health services in remote Australian communities are more likely than non-Indigenous clients to prefer face-to-face consultations to telehealth beyond the COVID-19 pandemic. 17 In addition, limited access to technology may be a barrier to telehealth for clients with socioeconomic disadvantage. 14
Conclusions
The majority of adult clients with mood and anxiety disorders reported satisfaction with telehealth mental health care provided during the COVID-19 pandemic. Telehealth provides a significant opportunity to improve access to mental health services by overcoming barriers such as geographical location and symptoms of mental illness. However, clinicians should consider the limitations of telehealth from clients’ perspectives when integrating telehealth into routine mental health care. In particular, strategies to enhance communication and a sense of connection during telehealth sessions may be needed, and client preferences for mode of delivery should be taken into consideration when possible.
Footnotes
Acknowledgements
We would like to thank the clients of the Black Dog Institute (BDI) Clinical Services who participated in this survey and Dr Claire McAulay for her assistance with data collection and analysis. S.B.H is supported by an NHMRC Investigator Grant (grant no’ 1178666). The BDI Clinical Services are supported by NSW Health.
Disclosure
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Informed consent
All participants provided informed written consent online.