
Abstract
Social phobia (fear and avoidance of being the centre of attention in case of embarrassment or shame) is a disorder that does not come to the attention of primary practitioners even though it begins in adolescence and is often chronic. In the Australian Burden of Disease study, social phobia was associated with a similar burden to that of schizophrenia (approx. 18 000 disability adjusted life years lost) but only one in five people with the disorder sought treatment, and only 8% of the burden was averted by current treatment [1]; therefore maximizing access to effective treatment is important. There is strong evidence for the effectiveness of cognitive behavioural therapy (CBT) in the treatment of social phobia 2–4. Recent studies indicate that clinician-assisted computerized cognitive behavioural therapy programmes can significantly reduce social phobia in the short and long term 5–10. These studies also indicate that such Internet therapies may reduce barriers to treatment seeking [11].
More than half of individuals who meet criteria for one mental disorder endorse symptoms that satisfy criteria for one or more additional mental disorders [12]. This is clinically important because comorbid patients experience greater disability and distress, decreased quality of life compared to non-comorbid patients, and are more difficult to treat [13]. Rates of comorbidity are especially high in individuals meeting criteria for social phobia. For example, 78% of Australians suffering from social phobia had a comorbid condition, usually another anxiety or affective disorder [14]. Studies have shown that a comorbid diagnosis of depression or generalized anxiety disorder (GAD) may range from having a minimal to a severe impact on treatment outcomes for social phobia 15–19.
The present study examined the impact of an Internet-based treatment programme for social phobia, the Shyness programme, on comorbid symptoms of depression and GAD in 211 patients. The two alternative hypotheses were as follows: (i) consistent with the view that short-term therapies such as CBT would be inappropriate in chronic mental disorders that were comorbid with other disorders [20], the diagnosis-specific Shyness treatment programme would have minimal impact on comorbid symptoms; and (ii) consistent with an increasing body of evidence indicating the potential of so-called unified or transdiagnostic treatment approaches [21], it was expected that significant reductions would also be seen in comorbid symptoms following the Shyness programme.
Method
Selection and diagnoses
Data on 211 participants in three randomized controlled trials (RCTs) of the Shyness programme were reanalysed 5–7. All had been recruited using the same techniques and inclusion criteria, and all were treated using the same treatment procedures and materials, and by the same therapist 5–7. The original analyses reported results from participants in the treated groups only, but this reanalysis also includes the results from participants in the waitlist control groups, who subsequently received treatment.
Applicants were recruited via a website (www.climateclinic.tv). Applicants in the first two RCTs who met the inclusion criteria were telephoned to determine whether they met DSM-IV criteria for social phobia using the social phobia section of the Composite International Diagnostic Interview version 3·0 (CIDI v3·0) [22]. The social phobia section of the Mini International Neuropsychiatric Interview Version 5·0·0 (MINI) [23] was used in the third RCT. Eligible participants were sent an informed consent form that they printed, completed and returned.
Sixty per cent of participants were female, mean age was 38 years (SD = 11.37), 35% had never married, 56% were in full-time employment, and 29% were taking medication for their mental disorder. All participants met DSM-IV criteria for social phobia.
Comorbidity with depression
The Patient Health Questionnaire nine-item (PHQ-9), a nine-item questionnaire with items that correspond to criterion A for depression in DSM-IV, was used to identify participants with elevated symptoms of depression [24]. The PHQ-9 distinguishes DSM-IV depressed individuals from healthy individuals in the general population [24]. A total score ≥10 indicates the likelihood of meeting diagnostic criteria for depression. This measure has demonstrated acceptable validity when compared with the DSM-IV Structured Clinical Interview for DSM, Symptom Checklist-20 depression scale and Beck Depression Inventory [25].
Comorbidity with generalized anxiety disorder
The severity of symptoms of GAD was measured by administering the Generalized Anxiety Disorder–7-Item Scale (GAD-7) [26]. This questionnaire consists of seven items that each correspond to diagnostic criteria for GAD from the DSM-IV. Scores ≥10 indicate a likelihood of meeting diagnostic criteria for GAD [26, 27].
Other outcome measures
The Social Phobia Scale (SPS) and Social Interaction Anxiety Scale (SIAS) are widely used, 20-item measures of performance and social interaction anxiety, respectively [28]. Internal reliabilities for the SPS (α = 0.89) and SIAS (α = 0.93) are high and they are sensitive to change [29]. The 12-item version of the World Health Organization Disability Assessment Schedule–2nd edition (WHODAS-II) [30] was used to measure disability. Each item is rated on a 5-point scale, with higher scores indicating increased disability. Changes over treatment in the SIAS and SPS were evidence of changes in symptoms of social phobia, while changes in the PHQ-9 and the GAD-7 were evidence of change in depression and anxiety, respectively.
Treatment procedure
The Shyness programme consists of four components: six online lessons; homework assignments; participation in an online discussion forum; and regular email contact with a therapist. Each lesson is in the form of an illustrated story about the treatment response of a young man with social phobia. Lessons 1 and 2 provide education about symptoms and treatment of social phobia; lesson 3 provides instructions on how to develop an exposure hierarchy; lessons 4 and 5 demonstrate principles of cognitive restructuring in the setting of exposure; while lesson 6 includes information about relapse prevention.
Each lesson included a printable summary and homework assignment. Participants were expected to complete homework tasks prior to completing the next lesson. Participants were also expected to regularly post messages and homework assignments on a secure and confidential online discussion forum, using an alias. The therapist moderated the treatment group forum and responded to postings within 24 h. After completing each lesson participants were emailed by the therapist. The themes of the therapist's emails varied from reinforcement for continued participation to encouragement to practise the relevant treatment skills including graded exposure. The therapist time commitment was <3 h per patient.
Group assignment
To examine the impact of comorbid symptoms of depression and/or GAD, participants were divided into one of four groups: (i) social phobia without significant symptoms of depression or GAD (SP only; n = 86); (ii) social phobia with PHQ-9 scores ≥ 10 (SP + DEP; n = 28); (iii) social phobia with GAD-7 scores ≥ 10 (SP + GAD; n = 46); and (iv) social phobia with both PHQ-9 and GAD-7 scores ≥ 10 (SP + DEP + GAD; n = 51).
Statistical analysis
Univariate analyses of variance (ANOVAs) followed by post-hoc Bonferroni-corrected t-tests were used to determine whether severity of pre-treatment SIAS, SPS, PHQ-9, GAD-7, and WHODAS-II scores differed between groups. Paired samples t-tests were conducted to determine whether changes occurred over treatment on those dependent variables. Univariate ANOVAs followed by post-hoc Bonferroni-corrected t-tests were then calculated on change scores to compare magnitude of changes over treatment between the groups. All reported statistics are based on intention-to-treat analysis and effect sizes are Cohen's d, using pooled standard deviations.
Results
Before treatment
The mean pre-treatment scores and change scores (before treatment minus after treatment), and effect sizes for the SIAS, SPS, PHQ-9, GAD-7, and WHODAS-II are reported for each of the four groups in Table 1 and in Figure 1. As expected, univariate ANOVAs indicated significant between-group differences on pre-treatments scores on the SIAS (F(3,207) = 16.65, p < 0.001), SPS (F(3,207) = 13.45, p < 0.001), PHQ-9 (F(3,207) = 167.13, p < 0.001), GAD-7 (F(3,207) = 172.82, p < 0.001), and WHODAS-II (F(3,207) = 27.04, p < 0.001). Post-hoc Bonferroni-corrected t-tests (Table 1) showed that at pre-treatment assessment, the SP + DEP + GAD group consistently reported more severe symptoms than the other three groups.
Pre- and post-treatment scores on the SIAS, SPS, PHQ-9, and GAD-7. GAD-7, Generalized Anxiety Disorder 7-Item; PHQ-9, Patient Health Questionnaire 9-item; SIAS, Social Interaction Anxiety Scale; SPS, Social Phobia Scale; WHODAS-II, World Health Organization Disability Assessment Schedule – 2nd edition. SP only, social phobia only; SP + Dep, social phobia and significant symptoms of depression; SP + GAD, social phobia and significant symptoms of generalized anxiety disorder; SP + Dep + GAD, social phobia + significant symptoms of depression and generalized anxiety disorder.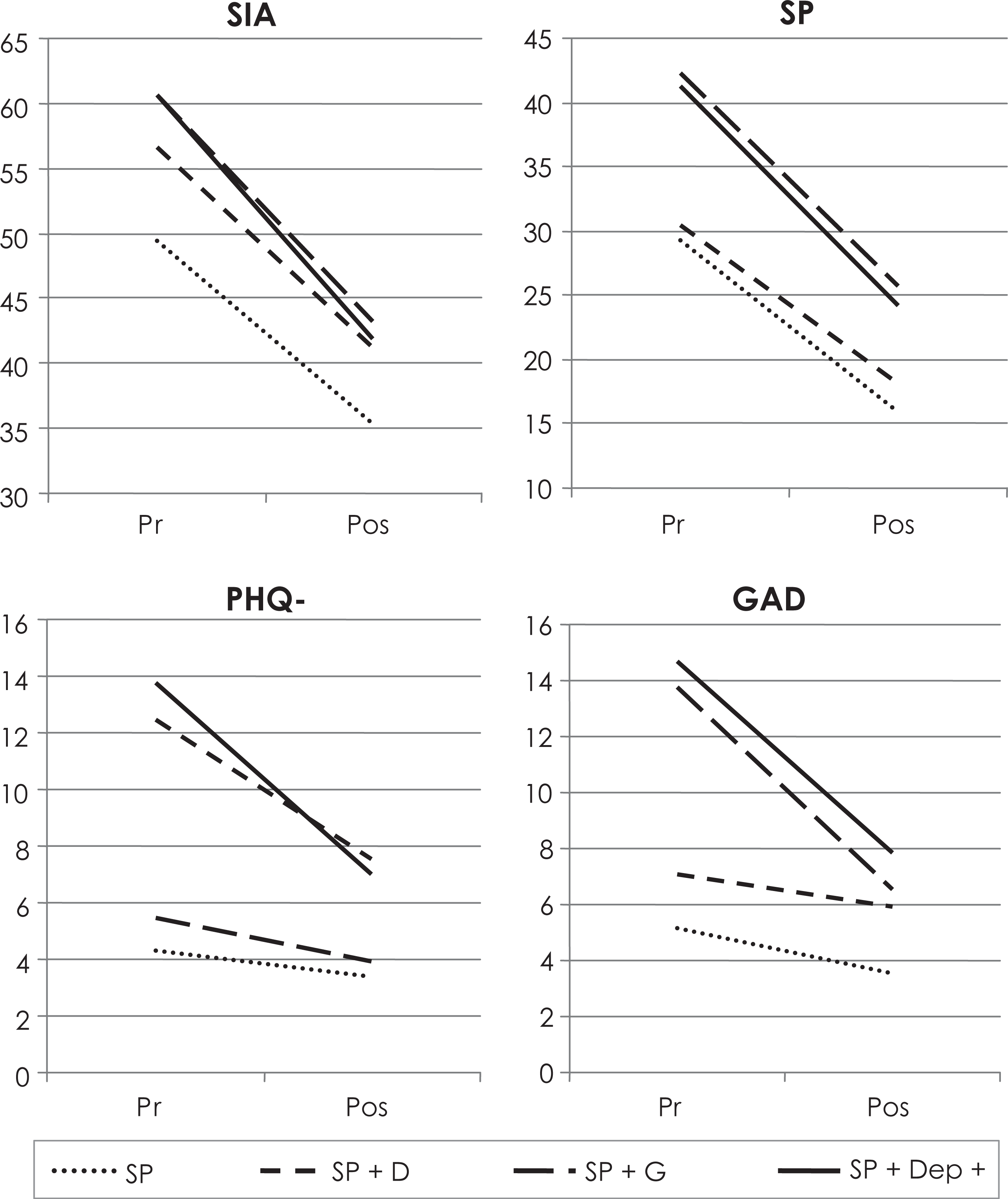
Pre-treatment and change scores (before minus after)
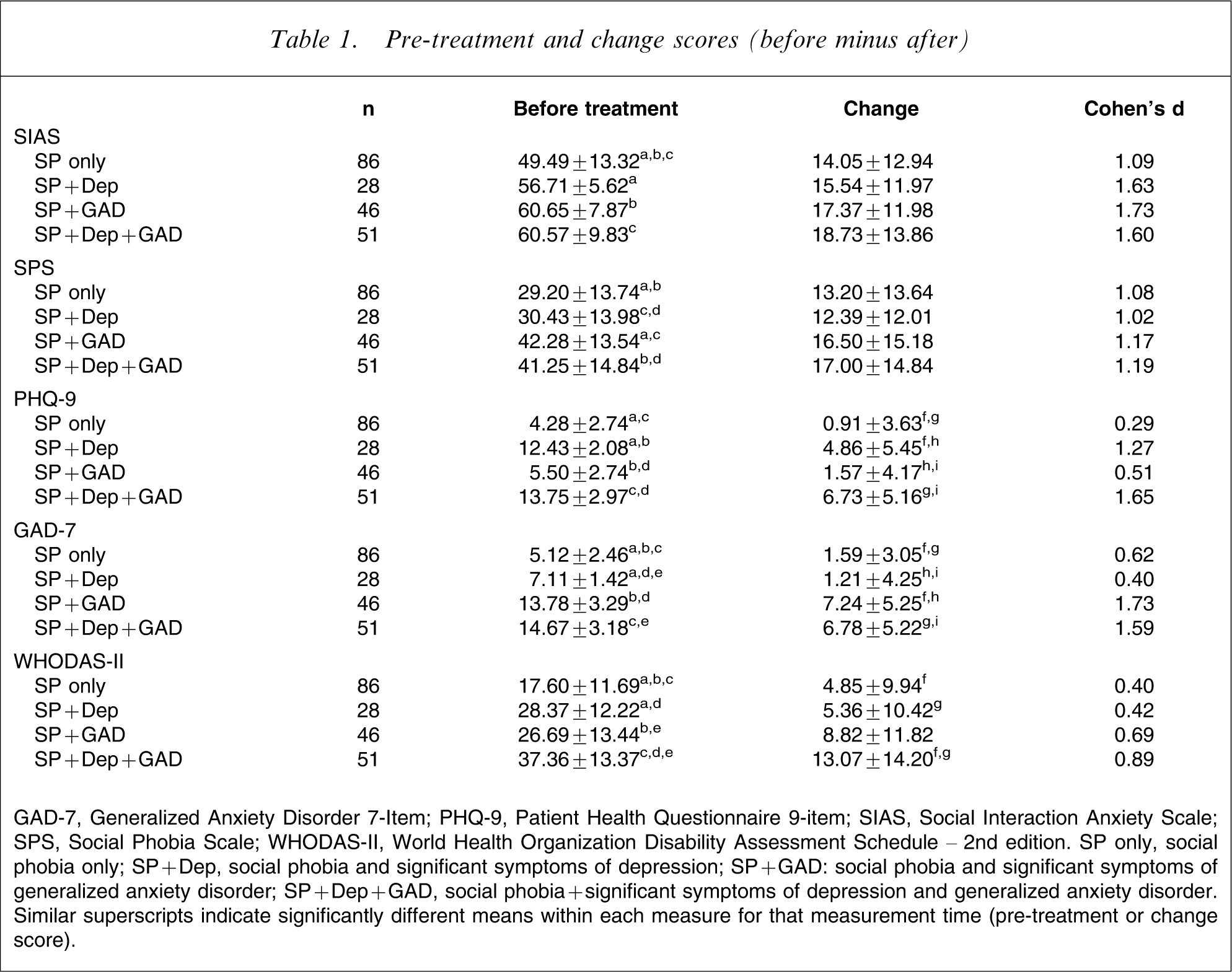
GAD-7, Generalized Anxiety Disorder 7-Item; PHQ-9, Patient Health Questionnaire 9-item; SIAS, Social Interaction Anxiety Scale; SPS, Social Phobia Scale; WHODAS-II, World Health Organization Disability Assessment Schedule – 2nd edition. SP only, social phobia only; SP + Dep, social phobia and significant symptoms of depression; SP + GAD: social phobia and significant symptoms of generalized anxiety disorder; SP + Dep + GAD, social phobia + significant symptoms of depression and generalized anxiety disorder. Similar superscripts indicate significantly different means within each measure for that measurement time (pre-treatment or change score).
Before–after treatment
Paired-sample t-tests confirmed that participants improved significantly from pre- to post-treatment assessment on the SIAS (t(210) = 18.13, p < 0.001), SPS (t(210) = 15.16, p < 0.001), PHQ-9 (t(210) = 8.61, p < 0.001), GAD-7 (t(210) = 11.46, p < 0.001, and WHODAS-II (t(210) = 9.43, p < 0.001).
Magnitude of change scores
Univariate ANOVAs failed to show significant between-group differences on the magnitude of change scores for the SIAS (F(3,207) = 1.61, p = 0.19) or SPS (F(3,207) = 1.28, p = 0.28) change scores. Statistically significant difference in changes scores between groups were observed on the PHQ-9 (F(3,207) = 21.82, p = 0.001), GAD-7 (F(3,207) = 28.32, p = 0.001), and WHODAS-II (F(3,207) = 5.94, p = 0.001), with the specific between-group differences found on post-hoc Bonferroni corrected t-tests included in Table 1.
Effect sizes
All four groups, whether or not comorbid, showed improvement in the main outcome measures of SPS and SIAS with all effect sizes exceeding 1.0, and no between-groups differences on these measures. Large pre–post-treatment effect sizes (>0.8) were observed on the PHQ-9 for groups with pre-treatment PHQ-9 scores in the pathological range, while large effect sizes were observed on the GAD-7 for the two groups with pre-treatment GAD-7 scores in the pathological range. The two groups with PHQ-9 scores in the pathological range improved significantly (mean effect size = 1.52), and the two groups with GAD-7 scores in the pathological range improved significantly (mean effect size = 1.66).
Discussion
The present paper examined the effect of Internet-based treatment for social phobia on comorbid symptoms of depression and GAD. Consistent with previous reports, this reanalysis, which also included the treatment results of the waitlist control group participants from the RCTs, indicated that the Shyness treatment programme resulted in significant improvement in measures of social phobia 5–7. Consistent with the second hypothesis, the present reanalysis showed that concurrent symptoms of anxiety or depression did not reduce rates of improvement. The groups with high depression scores had significant reductions in depression and the groups with high GAD scores also had significant reductions in GAD scores, even though the treatment programme was directed at the core issue of social phobia. All subjects met DSM-IV diagnostic criteria for social phobia. The median age of onset of this disorder is in adolescence and because the mean age of the subjects was 38 years, the disorder was, in all probability, chronic. The mean pre-treatment score on the WHODAS-II was 26, an indication that the average disorder was disabling. The number of subjects in each group was adequate, and the measures used are reliable and valid. The average duration of therapist input via email and via advice on the forum was brief (mean = 150 min clinician time per person). Participants in the first two trials have now been followed for 6 months and benefits in that group are stable [10].
The improvements in symptoms of depression and GAD are surprising. The content of treatment was focused on social phobia, with what we would consider as relatively minor references to managing mood. We are unaware of reports of the efficacy of computerized clinician-assisted CBT in people with social phobia comorbid with other disorders. We can only conjecture that the pre-determined and focused Internet therapy was helpful generally and was not distracted, as a face-to-face clinician could be, by the problems posed by significant comorbid disorders, thus providing more opportunity for the participant to learn coping skills that they could generalize to symptoms of other internalizing disorders.
The generalized benefits observed in the present study are broadly consistent with a growing body of research exploring the efficacy of unified or transdiagnostic treatment programmes for disorders of anxiety and depression [21]. While at least one study has reported that face-to-face CBT that remained focused on the core disorder was more effective than CBT that deliberately sought to accommodate the comorbid disorders [31], other evidence suggests that unified treatment approaches compare well to diagnosis-specific treatments, while also reducing the severity of comorbid disorders and symptoms [21]. Transdiagnostic treatment programmes that address the underlying vulnerability associated with internalizing disorders while also increasing resilience appear to be a promising area of research with considerable potential benefits.
Limitations
Internet therapy may be ideally suited to people with social phobia and the results, at least in terms of efficacy of treatment in the presence of comorbid disorders, may be confined to that disorder. We will examine the reliability of this finding with future participants from the Shyness programme using at least equivalent numbers. We have data on the benefits of Internet treatment for major depression and for panic disorder and agoraphobia 32–34 but the numbers, as yet, do not allow us to explore the effect of comorbidity.
Conclusions
Internet CBT for social phobia is effective, whether or not participants report scores consistent with concurrent comorbid major depression or GAD.
Footnotes
Acknowledgements
The authors gratefully acknowledge the participants for their involvement and helpful comments. We also wish to gratefully acknowledge the contributions to the development of the Climate Clinic programme by Mr Jason Hando, and Mr Daniel Winter.