
Abstract
Aim:
To compare the characteristics of clinic attenders in inner city homeless hostels with and without a diagnosed psychotic illness.
Method:
A cross-sectional study of homeless people attending psychiatric clinics in three inner city homeless hostels over a period of 8 years. The demographic characteristics, comorbid conditions, pathway to homelessness and pattern of homelessness of clinic attenders with a diagnosis of psychosis were compared with those who were not known to have psychotic illness.
Results:
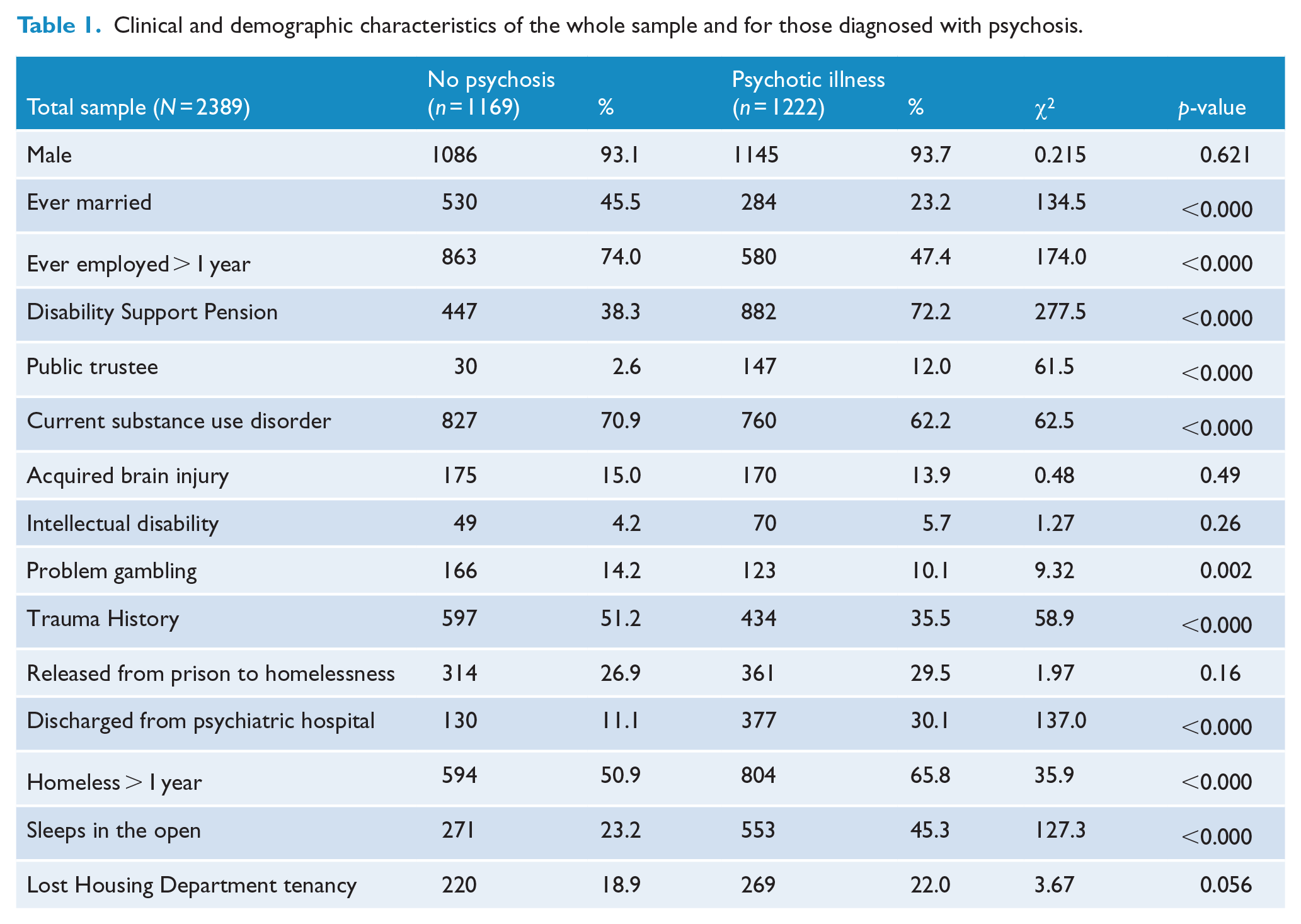
2389 homeless people attended one or more of the clinics in the 8 years of the study, of whom 1222 (51.2%) had a diagnosed psychotic illness, mostly schizophrenia. Those with psychosis were less likely to have been married (23.2% vs 45.5%), were less likely to have worked for more than a year (47.4% vs 74%) and were more likely to have been discharged from hospital to homelessness, to receive the Disability Support Pension (72.2% vs 38.3%), or be under financial management orders (12.0% vs 2.6%). Homeless people with psychosis were also more likely to have been homeless for more than a year, sleep in the open, and were less likely to have a current substance use disorder, problem gambling or a history of early life or recent trauma. A high proportion of those with psychosis (29.5%) had been released from prison to homelessness and a surprising number (22%) reported the loss of public housing tenancy.
Conclusion:
The results demonstrate the homeless with psychotic illness are particularly disabled and disadvantaged, often have multiple comorbid conditions, and many have been unable to maintain public housing tenancy. The inability of many of the homeless mentally ill to maintain public housing tenancy suggests the need for more supported housing to help the chronically homeless with psychotic illness maintain tenancy.
Introduction
Severe mental illnesses such as schizophrenia are common among homeless people in Sydney (Doutney et al., 1985; Teesson et al., 2004), other cities in Australia (Harvey et al., 2012; Lee et al., 2010), and in other high-income countries (Fazel et al., 2008). Estimates of the prevalence of psychotic illness among homeless populations range from 2.8% to 42.3%, with a meta-analysis finding a pooled prevalence of schizophrenia of 12.7% (Fazel et al., 2008). Earlier studies have estimated the proportion of homeless people with schizophrenia in Sydney to be between 11% and 36% (Doutney et al., 1985) consistent with a 2010 study suggesting a prevalence of schizophrenia of 25% (Teesson et al., 2004).
The reasons people become homeless in high-income countries are complex and varied, and include both individual vulnerabilities and personal circumstances, as well as the availability of affordable housing. However, people with psychotic illness seem to be particularly vulnerable to homelessness. Co-morbid substance use appears to be one of the main contributing factors, with one study finding that 70% of a homeless sample with a diagnosis of schizophrenia also had a substance use disorder (Teesson et al., 2000). Other studies emphasise the effect of combinations of psychiatric disorder, substance use and social circumstances (Fowler et al., 2009; Sullivan et al., 2000). Low rates of employment by people with psychosis probably contribute directly to the likelihood of becoming homeless (Hanlon et al., 2017), a situation worsened by the reduced availability of affordable housing in the inner city areas where the services to the homeless are concentrated. The financial stress due to expenditure on tobacco products is also a likely contributor because as many as 85% of the homeless smoke (Power et al., 2015). Moreover, people with psychosis often lack the cognitive ability and social skills required to find and keep a tenancy (Stergiopoulos et al., 2011), consistent with an observed association between the duration of psychotic illness and homelessness (Hanlon et al., 2017). Living outdoors has also been reported to be a choice for patients who may be uncomfortable in group accommodation because of the effect of symptoms or because of an inability to tolerate the behaviour of other residents of low-cost housing (Owen et al., 1996).
Even in inner city areas with generally accessible health care, the lack of a fixed place of abode can make it more difficult for those services to provide continuous care, contributing to increased hospital admissions and days spent in hospital by the homeless mentally ill (Russolillo et al., 2016). Studies have shown that homeless mentally ill people generate health care and other costs to the community that exceed the cost of providing appropriate housing (Evans et al., 2016; Larimer et al., 2009). The homeless mentally ill also face excess mortality, as an earlier conducted study in Sydney found that homeless people with schizophrenia had an almost fourfold standardised mortality ratio (Babidge et al., 2001).
The aims of this study were (1) to describe the characteristics of a large cohort of patients with psychotic illness seen at the mental health clinics of three inner city homeless hostels and (2) to examine the differences between homeless clinic attenders with psychotic illness and people with other disorders.
Methods
The sample comprised consecutive presentations to the mental health clinics at the three large homeless hostels in inner city Sydney, the Matthew Talbot Hostel run by the Society of St Vincent de Paul, Edward Eagar Lodge run by the Wesley Mission and Foster House run by the Salvation Army (Nielssen et al., 2018) between 21 July 2008 and 31 December 2016. The main purpose of each of the hostels was to provide care to people who were currently homeless, had been homeless or were at risk of becoming homeless.
Matthew Talbot Hostel provides overnight accommodation for 98 men in both single-room and eight-bed dormitories, as well as providing meals, clothing and health care facilities for as many as 250 men every day, many of whom live in the open. The hostel clinic dispenses medication, most commonly psychotropic medication, to approximately 100 men per day. Edward Eagar Lodge provides accommodation for 63 men and 13 women, and at the time of the study hosted a mental health clinic that served hostel residents and people referred by other agencies. Foster House has 97 male beds and a general practice, and at the time of the study also had a clinic provided by a psychiatrist and mental health nurse. Clinic attenders were either self-referred, referred by reception staff on presentation to the hostels if a history of psychiatric disorder or treatment was disclosed or suspected, or by welfare services within the hostels or other agencies. All patients attended the clinic voluntarily, and any treatment was provided on a voluntary basis, although some attenders were on bail or parole with the condition that they seek treatment. The population was quite transient, in part because each hostel had a nominal maximum length of stay of 3 months. However, many of the clinic attenders received long-term care, and other returned for treatment, often after losing accommodation found for them. The sample included a number of very disabled and difficult-to-manage mentally ill patients, and from time to time, acutely unwell patients were sent to hospital under the Mental Health Act, and returned to the clinic for continued treatment after discharge. Some residents of the hostels were treated as a condition of Community Treatment Orders administered by the St Vincent’s Mental Health Service. The clinics themselves were nurse-run clinics, with visiting psychiatrists and nurse practitioners funded by Commonwealth government schemes.
Sociodemographic and clinical information extracted from patients’ medical records included age, sex, employment history, marital status, social security benefit, whether under a financial management order, forensic history, history of sleeping in the open, duration of homelessness, whether they had previously lost a public housing tenancy, Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) psychiatric diagnoses, current psychotropic medication, adherence to medication, the pattern of symptoms, past psychiatric hospital admissions, the presence of documented cognitive impairment arising from intellectual disability (ID) or acquired brain injury (ABI), the presence and nature of substance use disorder, and whether there was a history of childhood or adult trauma. The assessment that a patient was treatment-resistant was made on clinical grounds from the information that was available, as many of the patients were transient. The psychiatric diagnoses were taken from the diagnoses recorded by visiting psychiatrists in the clinical records, or in some cases, by mental health nurse practitioners, rather than using any diagnostic instrument or tool.
For the purposes of this study, a diagnosis of psychotic illness included schizophrenia, schizo-affective disorder, bipolar disorder, delusional disorder, drug-induced psychosis, other organic psychosis and psychosis not otherwise specified.
Statistical analysis
Data were analysed by compiling a table of frequencies, comparing the characteristics of patients with and without a diagnosis of psychosis using chi-square statistic and F-values. Multiple logistic regression was then performed, using independent variables that differed to a p-value of >0.05, with psychosis as the independent variable.
Approval to conduct this study was obtained from the St Vincent’s Hospital Human Research Ethics Committee.
Results
Sample characteristics
Data were available for 2389 individuals (2232 men and 157 women), with a mean age of 42.3 (SD = 12.8) years. Over half of the attenders were diagnosed with a psychotic illness, mainly schizophrenia (n = 1222, 51.2%) and almost two-thirds (n = 1587, 66.1%) had a current diagnosis of substance use disorder. Other common psychiatric diagnoses were ABI (14.4%) and ID (5.0%). More than half (58.8%) had been homeless for more than a year, and about a third (34.5%) reported sleeping in the open. There was a large overlap between the diagnoses of psychosis and substance use disorder, and chronic homelessness. The demographic and clinical characteristics of the homeless clinic attenders with and without psychosis are summarised in Table 1.
Clinical and demographic characteristics of the whole sample and for those diagnosed with psychosis.
Characteristics of homeless patients diagnosed with psychotic illness
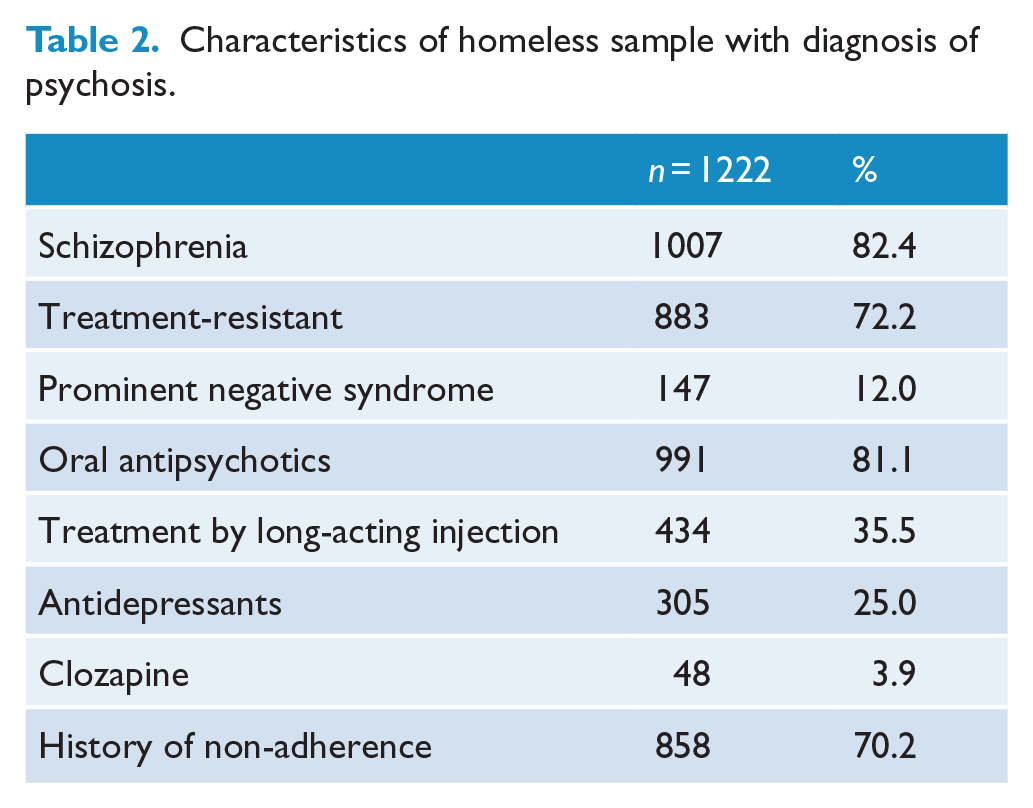
There were 1222 homeless clinic attenders diagnosed with psychotic illness, of whom 82.4% were diagnosed with schizophrenia. There was a significant inverse correlation between psychosis and the likelihood of an additional diagnosis of depression or anxiety, although a quarter (25.0%) were also prescribed antidepressant medication. Nearly three-quarters (72.2%) were described as treatment-resistant in the sense that they continued to experience symptoms of schizophrenia or express delusional beliefs despite adequate treatment. However, only 12.0% were described as having a prominent negative syndrome, which was probably an underestimate arising from the clinicians failing to make note of the presence of those symptoms.
More than two-thirds (70.2%) were reported to have a history of non-adherence to treatment, although most of the patients agreed to treatment at the time of the consultations and a third (35.5%) were receiving treatment with antipsychotic medication by long-acting injection (Table 2).
Characteristics of homeless sample with diagnosis of psychosis.
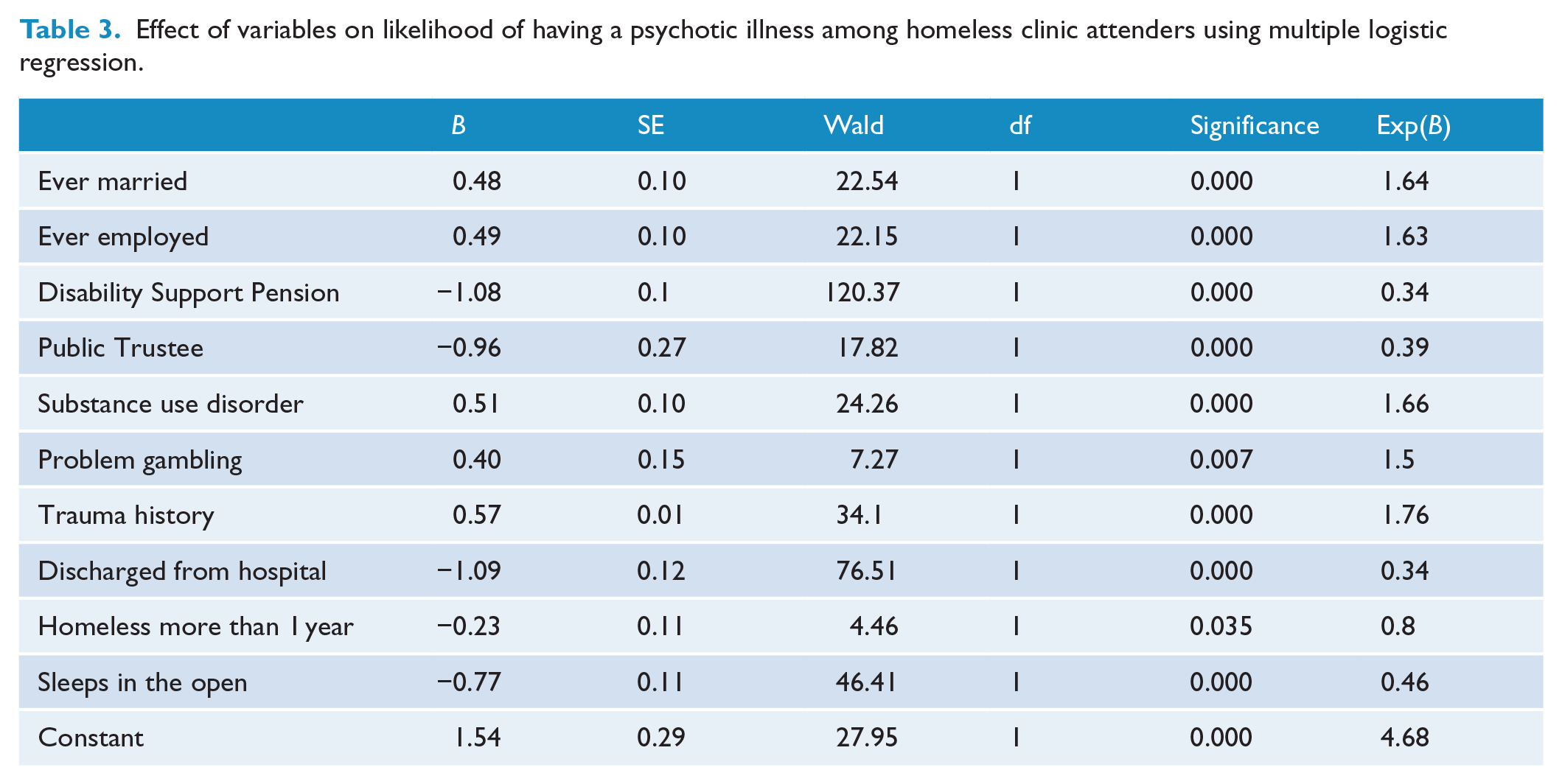
The multiple logistic regression model using independent variables significant to p > 0.05 found, not surprisingly, that the factors most strongly predictive of a diagnosis of psychosis were receiving the Disability Support Pension and having been discharged from a psychiatric hospital. However, a diagnosis of psychosis was also strongly associated with the likelihood of sleeping in the open and having been homeless for more than a year (Table 3).
Effect of variables on likelihood of having a psychotic illness among homeless clinic attenders using multiple logistic regression.
Discussion
We found that about half of the sample had a diagnosed psychotic illness, mainly schizophrenia, which is a higher proportion than found in other studies conducted in Sydney (Doutney et al., 1985; Teesson et al., 2004), and elsewhere (Fazel et al., 2008), and which is probably because our sample was of clinic attenders, rather than a representative sample of homeless hostel residents, or of a sample taken from those attending for free meals or using other services provided by the homeless hostels. However, it is possible that the proportion of people with schizophrenia who are homeless has increased over time, and the sample was representative in other ways, as many of the clinic attenders came from nearby public or supported housing, or reported attending the clinic while sleeping in the open.
We found statistically significant and clinically important differences between homeless people with psychotic illness and those without psychosis. Patients with psychotic illness were less likely to have been married, to have worked for a year, or to disclose a history of early life or recent trauma or report problem gambling. Despite high rates of substance use, attenders with psychosis were less likely to have a current substance use disorder (excluding tobacco use) than attenders without psychosis. They were more likely to receive the Disability Support Pension, to have their financial affairs managed by the Public Trustee, to have been homeless for more than a year, to sleep in the open and a high proportion had been released from prison to homelessness, all of which indicate significant disability and social disadvantage.
The high rate of psychotic illness in this sample confirms the results of other studies that have shown that many people with severe mental illness will become homeless if they are not provided with the necessary psychosocial support (Pearson and Linz, 2011). The finding that 22% of the sample had lost public housing tenancy suggests that the social disability associated with severe forms of psychotic illness prevents many patients from maintaining tenancy without support. Moreover, the lack of secure and affordable housing continues to be a barrier to participation in both treatment and community life for people with severe mental illness, resulting in continued reliance on homeless services (Gilmer et al., 2010) and supporting the view that stable housing is a pre-requisite for adequate treatment of severe mental illness (Holmes et al., 2017; Whittaker et al., 2015).
Thirty percent of our sample had been discharged from psychiatric hospitals to the homeless sector, often from wards in other parts of the state and even interstate. While it is hardly surprising that those with psychotic illness were more likely to have been discharged from a psychiatric hospital, the high proportion discharged from hospital without stable accommodation is troubling, because being homeless is associated with more frequent hospital admissions of longer duration and hence the high cost of health care generated by the homeless mentally ill (Russolillo et al., 2016). A similar pattern is observed among those discharged from prison to homelessness. In both groups, the reduced likelihood of continuing recommended treatment as a result of not having a fixed place of abode may contribute to relapse of illness and the return to institutional care. Moreover, the suboptimal treatment received by the homeless mentally ill, including low rates of treatment with clozapine, and the persistence of substance use may have added to the high proportion of patients deemed to be treatment-resistant.
The rate of comorbid substance use disorder among those with psychosis was comparable to the rates reported in previous studies (Teesson et al., 2000, 2003), but significantly less than the rate of current substance use disorder among the clinic attenders who were not diagnosed with psychosis. Hence, comorbid substance use is a major contributing factor, but not the only reason for people with psychosis becoming homeless, as more than 40% of the homeless mentally ill did not have a substance use disorder, whereas in our sample, substance use was the most common reason for homelessness among people who do not have psychosis. Substance use among people with psychotic illness may be a consequence of homelessness among people with psychosis as much as a cause, from living in an environment where substances are freely available and peer pressure to participate is common (Teesson et al., 2000) and as a way of coping with the stress of not having a safe place to live. Complications of substance use among the homeless with psychotic illness include poor physical health (Brown et al., 2018; Nielssen et al., 2017) and increased mortality (Babidge et al., 2001). Continued substance use also acts as barrier to returning to stable accommodation for many patients, both due to the priority given to substance use over paying rent and because of the effect of daily intoxication on organisational skills and other aspects of social performance. However, results from Housing First studies in the United States and Canada show that having supported accommodation is associated with a significant decline in substance use by people who were previously homeless (Cherner et al., 2017).
More than a quarter (29.5%) of those with psychosis reported recent release from prison, confirming the lack of suitable preparation for the social support of released prisoners. Between 5% and 7% of prisoners in NSW have schizophrenia (Nielssen and Misrachi, 2005), which translates to between 700 and 1000 people with schizophrenia in prison at any one time, many of whom are serving short sentences or are remanded in custody because they have no fixed place of abode or have failed to attend court. Ex-prisoners are more vulnerable to homelessness than the general population, because their status as former prisoners can result in discrimination when attempting to secure accommodation (Baldry et al., 2006) and also because Housing Department tenancies are usually cancelled after 3 months in custody. Former prisoners with psychotic illness are particularly vulnerable to homelessness after release because of impairment in social skills and negative symptoms associated with more severe forms of schizophrenia.
The frequent transfer between prison and psychiatric hospital care raises the possibility that the homeless mentally ill are part of a subpopulation that is subject to a phenomena first described by Lionel Penrose (1939), in which the reduced availability of psychiatric hospital beds or other suitable therapeutic accommodation increases the likelihood that people with mental illness will be detained in prisons. Penrose’s study took place before the introduction of antipsychotic medication which allowed large-scale discharge from psychiatric hospitals to community care, and before modern patterns of substance use and the reduced tolerance of deviant behaviour led to an increase in the prison population (Large and Nielssen, 2009). Nevertheless, there are now nearly as many people with schizophrenia in prison as there are psychiatric hospital beds in New South Wales (Nielssen and Misrachi, 2005), many of whom could be safely managed in lower cost supported accommodation (Hayes et al., 2014).
A limitation of this study is that it is a sample of clinic attenders, rather than of all the residents of the hostels, or a sample of people sleeping in the open. At the Matthew Talbot Hostel, for example, only about a third of the 99 residents of the hostel were known to the clinic at any one time, and among the 250 or so served lunch at the hostel every day were some obviously mentally ill rough sleepers who refused an invitation to attend the clinic for review. However, the sample is drawn from three hostels with quite different cultures, and includes many people who were not staying in the hostels, either because they were sleeping in the open, or were living in public housing or other accommodation, and is probably a representative sample of homeless people seeking or willing to have mental health care. Another limitation is the underrepresentation of women, because two of the hostels only took men. However, women comprise a relatively small proportion of the homeless in inner city Sydney (Virgona et al., 1993) for a range of reasons, including better social skills, fewer problem behaviours and lower rates of substance use. A further limitation is that the data are mostly taken from self-report by a population in which it was often difficult to elicit a reliable history, and a better understanding of the relationship with, for example, public housing tenancy, imprisonment, hospital admission and homelessness would require a study that linked the data from those sources. The rate of trauma in the sample is also likely to be underreported.
This study identified that homeless people with psychotic illness are more likely to have severe and disabling forms of psychotic illness, to be chronically homeless and to sleep in the open. The high prevalence of substance use disorder confirms that any attempt to address homelessness in this population would have to include treatment for substance use. The high proportion of patients who have lost what should be secure Housing Department tenancy reveals the need for supported accommodation for people who do not have the living skills required to maintain a public housing tenancy. The proportion of people with psychotic illness released from prisons and psychiatric hospitals to homelessness suggests a need for better discharge planning and more supported accommodation to prevent the rapid return to institutional care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.