
Abstract
Objective:
To compare the symptoms and social function of patients with psychosis and current substance use to those with psychosis and no history of substance use.
Method:
The databases EMBASE, MEDLINE and PsycINFO were searched for peer-reviewed publications in English that reported the characteristics of patients with psychotic illness who were current substance users and those who had never used substances. The searches yielded 22 articles that met the inclusion criteria. Meta-analysis was used to compare four key outcome variables: positive symptoms, negative symptoms, depression and social function – and three secondary outcomes: violence, self-harm and hospital admissions.
Results:
Current substance-using patients were significantly younger than non-substance-using patients and were more likely to be male, but did not differ in age at onset of psychosis or in their level of education. Current substance users had higher ratings of positive symptoms and were more likely to have a history of violence. Older studies reported a stronger association between current substance use and positive symptoms than more recently published studies. Current substance users did not differ from non-users on measurements of negative symptoms, depressive symptoms, social function, self-harm, or the number of hospital admissions.
Conclusion:
Current substance users with psychosis may have more severe positive symptoms than patients who have never used substances, but this result should be interpreted with caution because of demographic differences between substance users and non-substance users.
Introduction
Substance use by patients with psychosis is a common problem faced by patients, their families and treating teams. There are numerous studies suggesting that patients with psychosis and substance use have worse outcomes than non-users (Barnes et al., 2006; Mauri et al., 2006; Sorbara et al., 2003; Wade et al., 2006). Establishing the differences between the pattern of symptoms of people with psychosis and substance use and those with no history of substance use might further our understanding of the role of substance use in the aetiology of psychoses and would assist clinicians treating patients with co-morbid substance use.
The association between substance use and positive, negative and depressive symptoms in psychosis has been reported on in primary research and in several previous meta-analyses. Earlier meta-analyses have suggested that patients with psychosis and substance use have more severe positive symptoms (Talamo et al., 2006) and more severe depressive symptoms (Potvin et al., 2007) than those with no history of substance use, but less severe negative symptoms than non-substance users (Potvin et al., 2006; Talamo et al., 2006). A weakness of the majority of primary studies, and consequently the previous meta-analyses, is that patients who have stopped using substances (former substance users) have been included in either the substance-using groups or in the non-using groups. It is now known that approximately half of all substance-using patients with psychosis stop using substances early in the course of their illness (Wisdom et al., 2011) and that patients who have given up substances have less severe symptoms than those who continue to use substances (Mullin et al., 2012). Hence, the earlier meta-analyses might not have reflected the true extent to which current substance use is associated with more severe symptoms. The inclusion of former substance users with more severe symptoms than non-substance users in the group of non-substance-using patients, or the inclusion of former substance users with less severe symptoms than substance users in the group of substance-using patients would result in an underestimation of the effect of substance use on the symptoms of psychosis.
A meta-analysis of studies that clearly distinguished current substance users with psychosis from those who have never used substances would provide a better estimate of the extent of the association between substance use and symptoms than previous meta-analyses. Moreover, there are at least six recent primary studies that were not included in earlier meta-analyses (Baeza et al., 2009; González-Pinto et al., 2011; Harris et al., 2010; Harrison et al., 2008; Hinton et al., 2007; Turkington et al., 2009).
We report a systematic review and meta-analysis that compares the characteristics of current substance users with psychosis (referred to as substance users) to those with psychosis who have never used substances (referred to as non-substance users). Former substance users were not included in the analysis. We hypothesised that the inclusion of former substance users in either the substance-using or non-substance-using groups would have lessened the estimated extent of the adverse effects of substances on symptoms in previous studies. Hence, we expected to find a stronger association between substance use and positive symptoms, negative symptoms and depressive symptoms than earlier meta-analyses. The specific null hypotheses were that groups of substance users and non-substance users with a psychotic illness would not differ in ratings of the key outcomes of positive symptoms, negative symptoms, depressive symptoms and social function.
Methods
The methods were based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Liberati et al., 2009).
Searches
Systematic searches of the electronic databases EMBASE, MEDLINE and PsycINFO were conducted for publications in English, comparing the characteristics of patients with a psychotic illness who reported current use of any psychoactive substance other than tobacco and caffeine with the characteristics of patients with a psychotic illness and no history of substance use (see Figure 1). All papers that appeared likely to include data were examined in full text because the abstracts proved to be an unreliable guide as to whether the papers met the inclusion criteria of separating current substance users and non-substance users. In order to ensure the completeness of our sample of studies, the electronic search results were supplemented with a hand searches of the reference lists of included studies, a recent systematic narrative review of substance use and outcome in first-episode psychosis (Wisdom et al., 2011), and previous meta-analyses of the relationship between substance use and positive, negative and depressive symptoms (Gupta et al., 2013; Mullin et al., 2012; Potvin et al., 2006, 2007; Talamo et al., 2006).
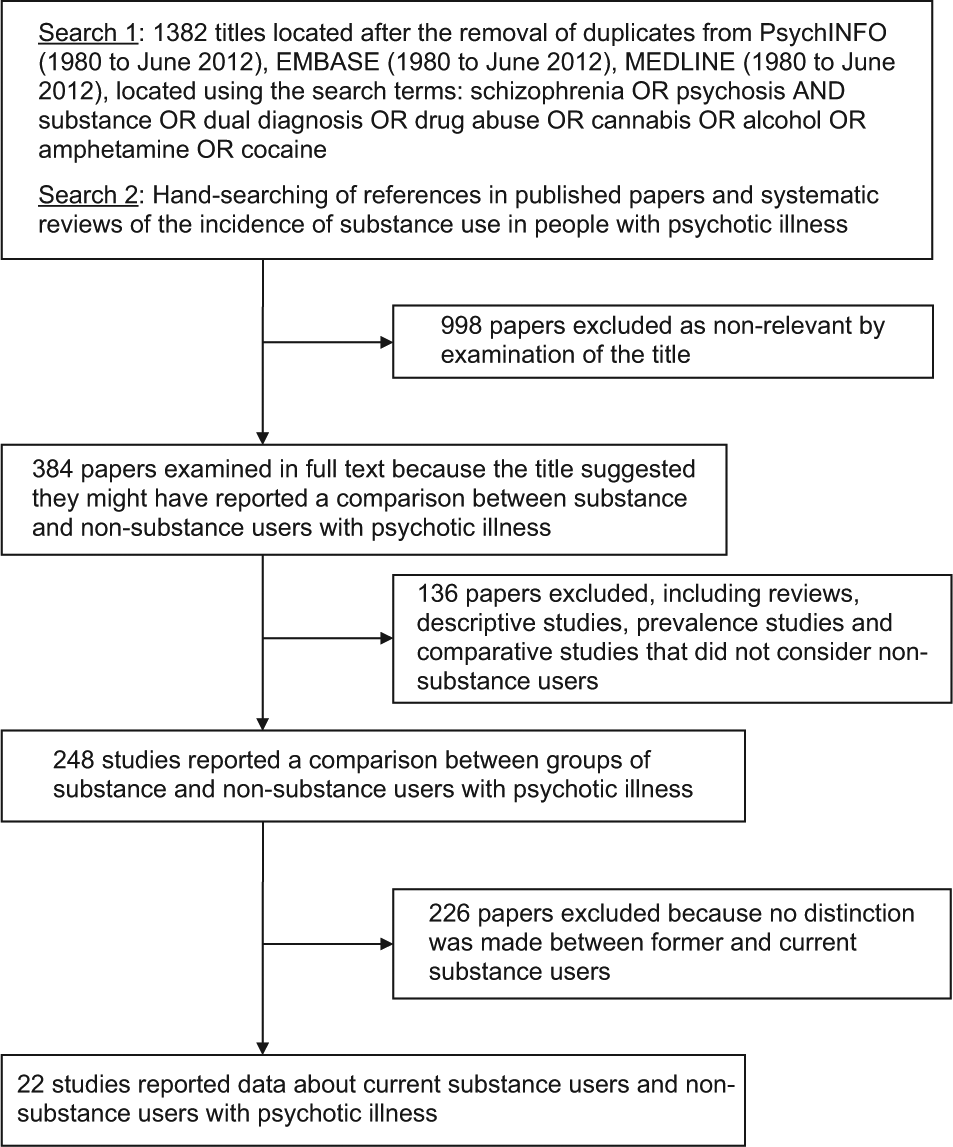
Search strategies and results.
Definitions and coding of substance use and symptoms
Psychosis was defined to include affective psychosis, first episode psychosis and schizophrenia-related psychosis (schizophrenia, schizoaffective disorder and delusional disorder). Studies of patients with bipolar disorder alone were not included because of the possibility that those studies included some patients with non-psychotic conditions. Studies of drug-induced psychosis were excluded.
The studies that met the inclusion criteria used a range of definitions of substance use (see Table 1). In all of the studies the level of substance use was considered to be clinically significant. We included studies that considered the use psychoactive substances, including alcohol, cannabis, stimulants and other drugs, as well as studies that specifically examined cannabis use (see Table 1). We did not consider studies that defined substance use as tobacco or caffeine use. We included cross-sectional studies reporting substance use histories and longitudinal studies reporting cohorts of substance-using and non-substance-using patients in whom symptoms were measured at baseline and at a later date (see Table 1).
Included studies reporting the characteristics of current substance users with psychosis and those with psychosis who have never used substances.
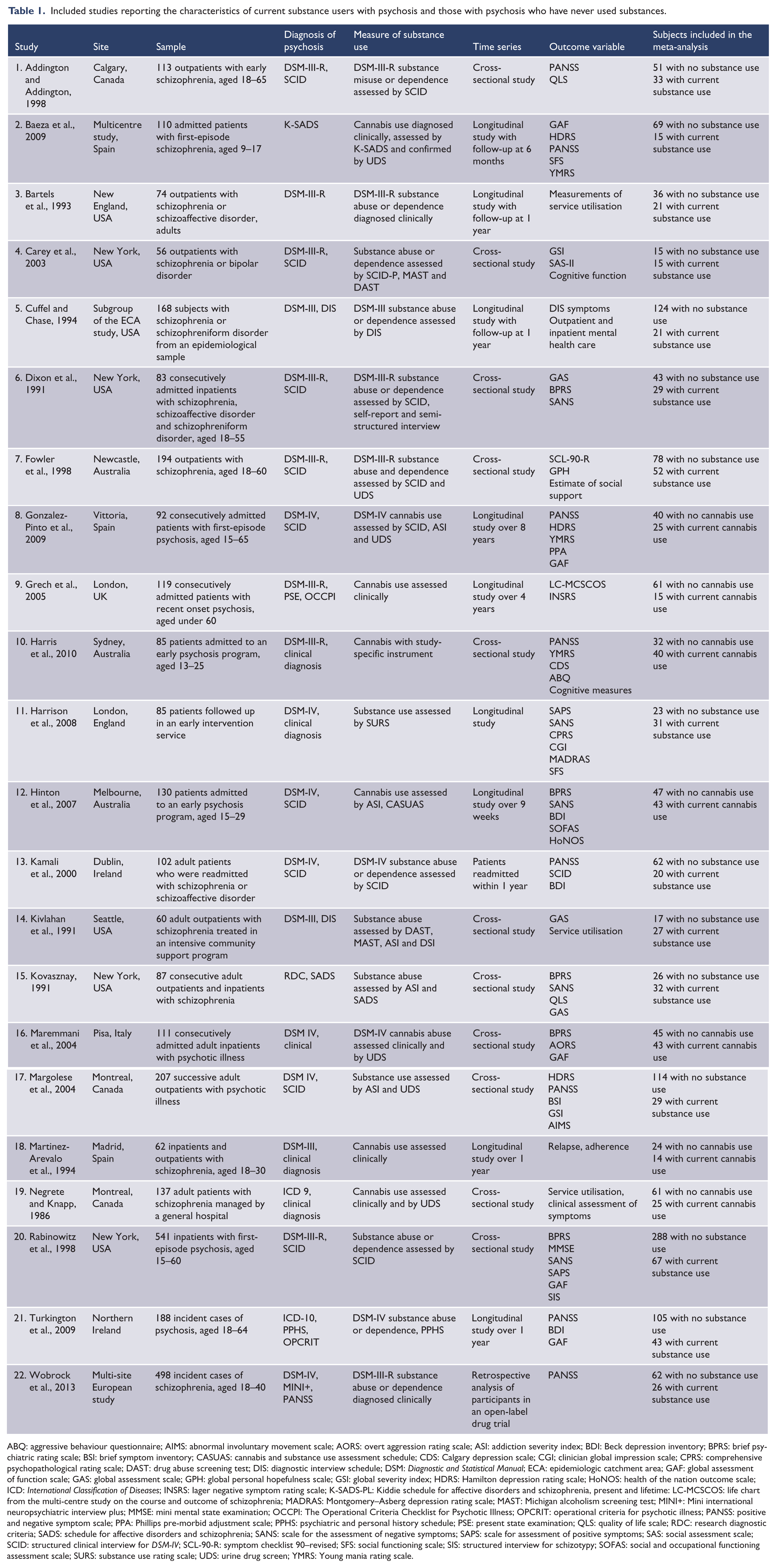
ABQ: aggressive behaviour questionnaire; AIMS: abnormal involuntary movement scale; AORS: overt aggression rating scale; ASI: addiction severity index; BDI: Beck depression inventory; BPRS: brief psychiatric rating scale; BSI: brief symptom inventory; CASUAS: cannabis and substance use assessment schedule; CDS: Calgary depression scale; CGI; clinician global impression scale; CPRS: comprehensive psychopathological rating scale; DAST: drug abuse screening test; DIS: diagnostic interview schedule; DSM: Diagnostic and Statistical Manual; ECA: epidemiologic catchment area; GAF: global assessment of function scale; GAS: global assessment scale; GPH: global personal hopefulness scale; GSI: global severity index; HDRS: Hamilton depression rating scale; HoNOS: health of the nation outcome scale; ICD: International Classification of Diseases; INSRS: Iager negative symptom rating scale; K-SADS-PL: Kiddie schedule for affective disorders and schizophrenia, present and lifetime: LC-MCSCOS: life chart from the multi-centre study on the course and outcome of schizophrenia; MADRAS: Montgomery–Asberg depression rating scale; MAST: Michigan alcoholism screening test; MINI+: Mini international neuropsychiatric interview plus; MMSE: mini mental state examination; OCCPI: The Operational Criteria Checklist for Psychotic Illness; OPCRIT: operational criteria for psychotic illness; PANSS: positive and negative symptom scale; PPA: Phillips pre-morbid adjustment scale; PPHS: psychiatric and personal history schedule; PSE: present state examination; QLS: quality of life scale; RDC: research diagnostic criteria; SADS: schedule for affective disorders and schizophrenia; SANS: scale for the assessment of negative symptoms; SAPS: scale for assessment of positive symptoms; SAS: social assessment scale; SCID: structured clinical interview for DSM-IV; SCL-90-R: symptom checklist 90–revised; SFS: social functioning scale; SIS: structured interview for schizotypy; SOFAS: social and occupational functioning assessment scale; SURS: substance use rating scale; UDS: urine drug screen; YMRS: Young mania rating scale.
Substance use and measurements of illness severity were coded so that a positive effect size indicated more severe positive, negative and depressive symptoms in current substance users. For measurements of social function, a positive effect size indicated better social function. We accepted any measure of social function including recognised scales such as the Social Functioning Scale (Birchwood et al., 1990) and the Social and Occupational Assessment Scale (Morosini et al., 2000), measures of employment and scales developed for particular studies.
Data extraction
Three raters independently extracted the following data:
diagnoses of included patients, the substances examined, and the number of current substance-using and non-substance-using patients,
demographic data for both groups: age, age at onset of psychosis, sex and the level of education,
measurements of the three key symptom outcomes: positive psychotic symptoms, negative symptoms and symptoms of depression,
measurements of social function (including employment) and,
secondary outcomes: numbers of hospital admissions, self-harm, episodes of violence and convictions for non-violent offences.
Assessment of strength of reporting in the primary research
The studies included in the meta-analysis were conducted over more than two decades, during which time the methods for measuring outcomes and reporting findings in observational studies have changed. We derived an eight-point ‘strength of reporting’ scale from the methods items of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement checklist (von Elm et al., 2007). Studies were accorded a score of 1 for each item and the sum of these scores was used as an overall strength of reporting score. We classified studies with a score of ≥6 as having stronger reporting. No study was found to be of poor quality and we acknowledge that the methods used in each individual study are likely to have reflected the best method that the primary researchers had at their disposal to address their study questions.
The items of the strength of reporting score were:
Use of patients with schizophrenia-related psychosis (because studies examining a mix of affective and non-affective psychoses might obscure the differing effects of substances use according to diagnosis).
Use of consecutive presentations (because those studies would be likely to have more representative samples).
Participation rate of over 50% (again because those studies would be likely to have more representative samples).
A sample of current substance of users ≥25 people (because of the lower probability of chance findings).
Re-measurement after a period of follow-up rather than a strictly cross-sectional design (because longer-term outcomes are more important than short-term outcomes).
Use of structured or semi-structured methods for establishing the history of substance use.
Use of structured or semi-structured methods for establishing the diagnosis of psychosis.
Use of structured or semi-structured methods for assessing key outcome variables.
Items 6–8 were used because structured and semi-structured methods could be expected to define variables more reliably.
Meta-analysis
Meta-analysis was performed using a random effects model because of differences in study design, including in diagnostic criteria, stage of psychotic illness studied, and in the measurement of key variables, such as positive and negative symptoms. A random effects model allows for differences in the populations and methods of measurement between the studies and only requires that definitions are consistently applied within each study. Variables reported in fewer than five studies were excluded from the meta-analysis because the random effects model lacks the statistical power to detect potentially significant effect sizes when the number of studies is small (Borenstein et al., 2009).
The statistical power of a random effects meta-analysis was considered on an a priori basis using assumptions based on our earlier meta-analysis of the symptoms of current and former substance users (Mullin et al., 2012) using the method described by Borenstein and associates (2009). We estimated that a random effects meta-analysis of 15 studies, each with a sample size of approximately 25 subjects in each group, where between-study heterogeneity was high, would have an 80% chance of detecting a small standardised mean difference (SMD) of 0.3 at a level of significance of 0.05. The power of the meta-analysis would be increased if there were more than 15 studies, if the included studies had larger mean sample sizes, if the heterogeneity was lower, or if the true difference between the groups was larger than a SMD of 0.3.
Comprehensive Meta-analysis (Version 2; Biostat, Englewood, NJ, USA) was used to convert all continuous data into a SMD, to calculate pooled effect sizes, to assess heterogeneity and to assess the possibility of publication bias. Categorical data were analysed using meta-analysis of odds ratios (ORs). All significance testing was conducted in a two-tailed form. Between-study heterogeneity was assessed with I-squared statistics. Between-study heterogeneity was classified as low if I-squared was below 25, moderate for between 25 and 50, and high above 50 (Higgins et al., 2003). Between-subgroup heterogeneity in effect size was examined using Q-value statistics and a significance level of 0.05. The possibility of publication bias was examined using funnel plots, Duval and Tweedie’s trim and fill test and a classic fail-safe N test.
Investigation of between-study heterogeneity
Three subgroup analyses were performed to explore between-study heterogeneity that may have arisen from: (a) whether the studies grouped patients according to the use of any substance or cannabis use; (b) whether the studies were conducted in cohorts of patients with first-episode psychosis or among patients with established illness; and (c) differences in the overall score on the strength of reporting scale.
Cannabis use was chosen for subgroup analysis because of the large body of evidence about the association between cannabis and psychosis (Andreasson et al., 1987; Large et al., 2011; Moore et al., 2007). Moreover, in the studies where cannabis use was the independent variable, some subjects who did not use cannabis but might have been using other substances could have been included in the non-substance-using group. Studies of first-episode psychosis were examined as a subgroup because of the increasing recognition that stage of illness is an important determinant of symptoms and response to treatment (McGorry et al., 2006) and because the effects of substance use in first-episode psychosis have not been the subject of a previous meta-analysis of this topic. Studies with higher strength of reporting scores were also examined as a subgroup because stronger studies had a reduced risk of reporting chance findings. The possible effect of the date of publication of the study on effect size was also explored with a mixed effect meta-regression using the year of publication as a moderator variable.
Results
Searches, data extraction and selection of variables for meta-analysis
The electronic searches and the hand searches of references identified 384 potentially relevant papers by title. Two raters examined all of the papers in full text (Figure 1) and 22 papers met the inclusion criteria (Table 1). Two raters extracted the data independently, with disagreements in 8 of 574 data points (1.4%). A third author performed an independent data extraction and the remaining discrepancies were resolved by a joint re-examination of the data.
The 22 studies reported a total of 2089 patients, of whom 1423 (68.1%) were non-substance users (mean sample size of 64.7 per study, standard deviation (SD) 58.2), and 666 (31.9%) were current substance users (mean of 30.3 per study, SD 35.8). Former substance users were not considered.
The studies that measured the key outcomes of positive symptoms, negative symptoms and depressive symptoms used well-established measurements of illness severity (see Table 1 for details). Of the 22 included studies:
eight used the Positive and Negative Syndrome Scale (Kay et al., 1987),
five used the Brief Psychiatric Rating Scale (Overall and Gorham, 1962),
two used the Scale for the Assessment of Positive Symptoms (Andreasen et al., 1995),
five used the Scale for the Assessment of Negative Symptoms (Andreasen et al., 1995),
three used the Beck Depression Inventory (Beck et al., 1988) and,
two used the Hamilton Depression Rating Scale (Hamilton, 1960).
There were eight papers that reported the course of subjects over a period of follow-up and 14 studies that were strictly cross-sectional in design (see Table 1). Of the studies that reported data measured at more than one point in time, the data after the longest period of follow-up were used. Hence, the meta-analysis can be considered to be of cross-sectional data.
A total of 12 variables were reported in five or more studies. These included five demographic and diagnostic variables (age, age at onset of psychosis, sex, years of education, proportion with a schizophrenia-related psychosis), four key outcome measurements (positive symptoms, negative symptoms, depressive symptoms, social function) and three secondary outcomes (a history of self-harm, episodes of violence or criminal convictions and, the number of hospital admissions). We did not include total symptom scores because they were not independent of the four key outcome variables.
Seven of the 22 studies reported on cannabis users and 15 used the broader definition of any substance use (Table 1). Nine studies were conducted among patients in first-episode psychosis (Table 1). Ten studies were rated as having stronger reporting methods, defined as a score of more than 6 out of 8 on our strength of reporting scale. Every study scored at least two on our strength of reporting scale and no study was excluded from the meta-analysis because of inadequate quality. There was no significant difference in the strength of reporting scores according to the year of publication. Twelve studies published after the year 2000 had an average strength of reporting score of 5.3 (SD 1.3) and 10 published before 2000 had an average score of 5.0 (SD 1.2). There were 17 studies reporting on positive symptoms but fewer studies reporting negative symptoms (n=11), depressive symptoms (n=10) or measurements of social function (n=10).
Main results
Current substance users had significantly more positive symptoms than non-substance users, with a small to medium effect size. Current substance users did not significantly differ from non-substance users in negative symptoms, depressive symptoms or in measurements of social function (Table 2).
Meta-analysis of the differences between current substance users and non-substance users.
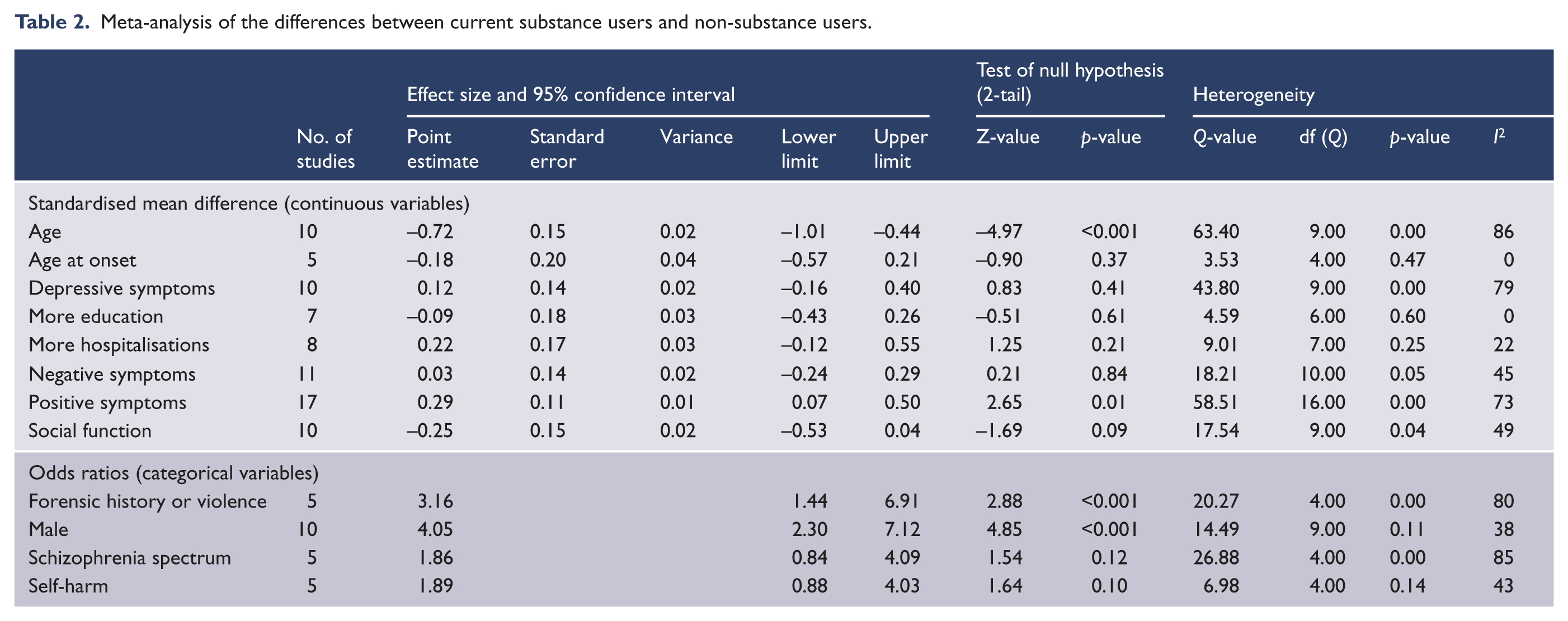
Current substance users were significantly younger, were more likely to be male and were more likely to have had a history of criminal convictions or a history of violence than non-substance users (Table 2). There were no significant differences between current substance users and non-substance users in the proportions of patients with a schizophrenia-related psychosis, age at onset of psychosis or years of education, nor were there significant differences between the groups in the number of hospital admissions or in the proportion of patients with a history of self-harm (Table 2, further details in data supplement: Supplemental Data 1).
Heterogeneity in effect sizes for key outcome variables
There was a high degree of between-study heterogeneity in the effect sizes for positive symptoms and depressive symptoms. Between-study heterogeneity in the effect size for negative symptoms and social function was rated as moderate.
Examination of the funnel plot for positive symptoms revealed five outlying studies: three on the left with less severe positive symptoms among current substance users, and two on the right with more severe positive symptoms among current substance users. When outlying studies were adjusted for using Duval and Tweedie’s trim and fill, the effect size for positive symptoms was reduced by 22% to SMD=0.23 (95% CI: 0.12 to 0.34). A classic fail-safe N test suggested that 83 missing studies with SMD=0 would be needed to return p to > 0.05.
Meta-regression suggested that studies with a later publication date reported a significantly smaller difference in positive symptom scores between current substance users and non-substance users (slope 0.034, 95% CI: 0.0013 to 0.67, Z-value=2.04, p=0.04). The year of publication was not significantly associated with effect size heterogeneity in negative symptoms (slope 0.04, 95% CI: –0.005 to 0.085, Z-value=1.74, p=0.08), depressive symptoms (slope 0.006, 95% CI: –0.05 to 0.06, Z-value=0.21, p=0.8) or social function (slope −0.005, 95% CI: –0.04 to 0.03, Z-value = −0.29, p=0.8).
Subgroup analysis of studies of cannabis users, first-episode patients and of studies with higher strength of reporting scores
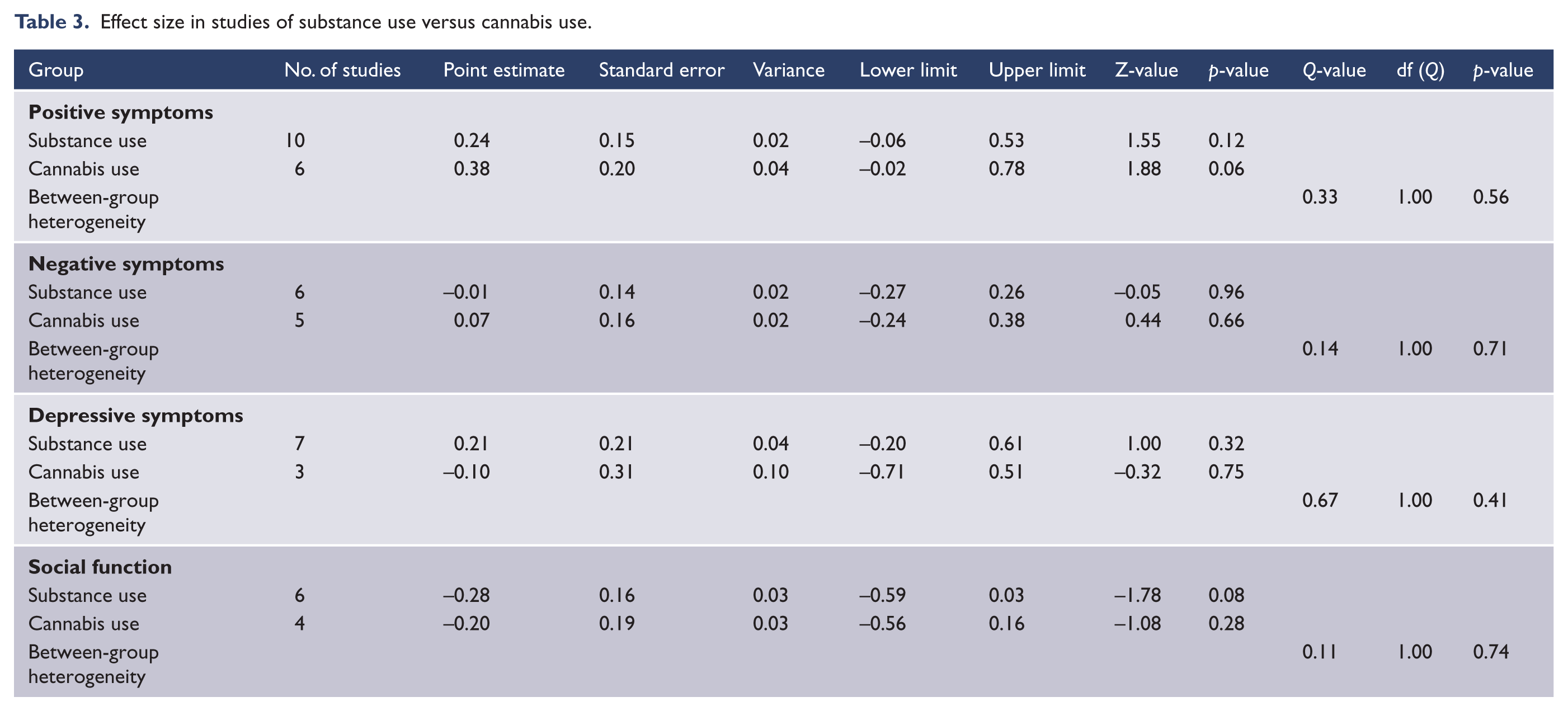
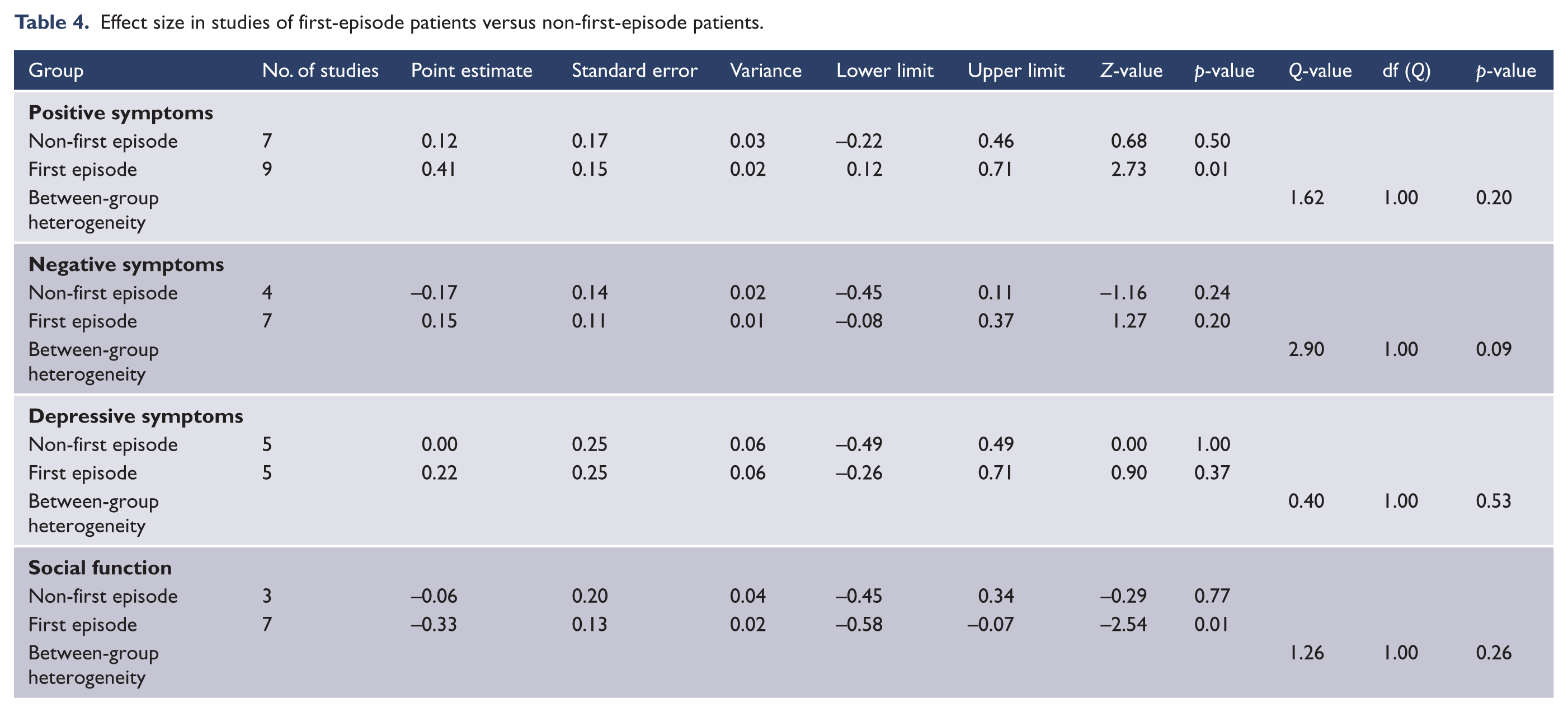
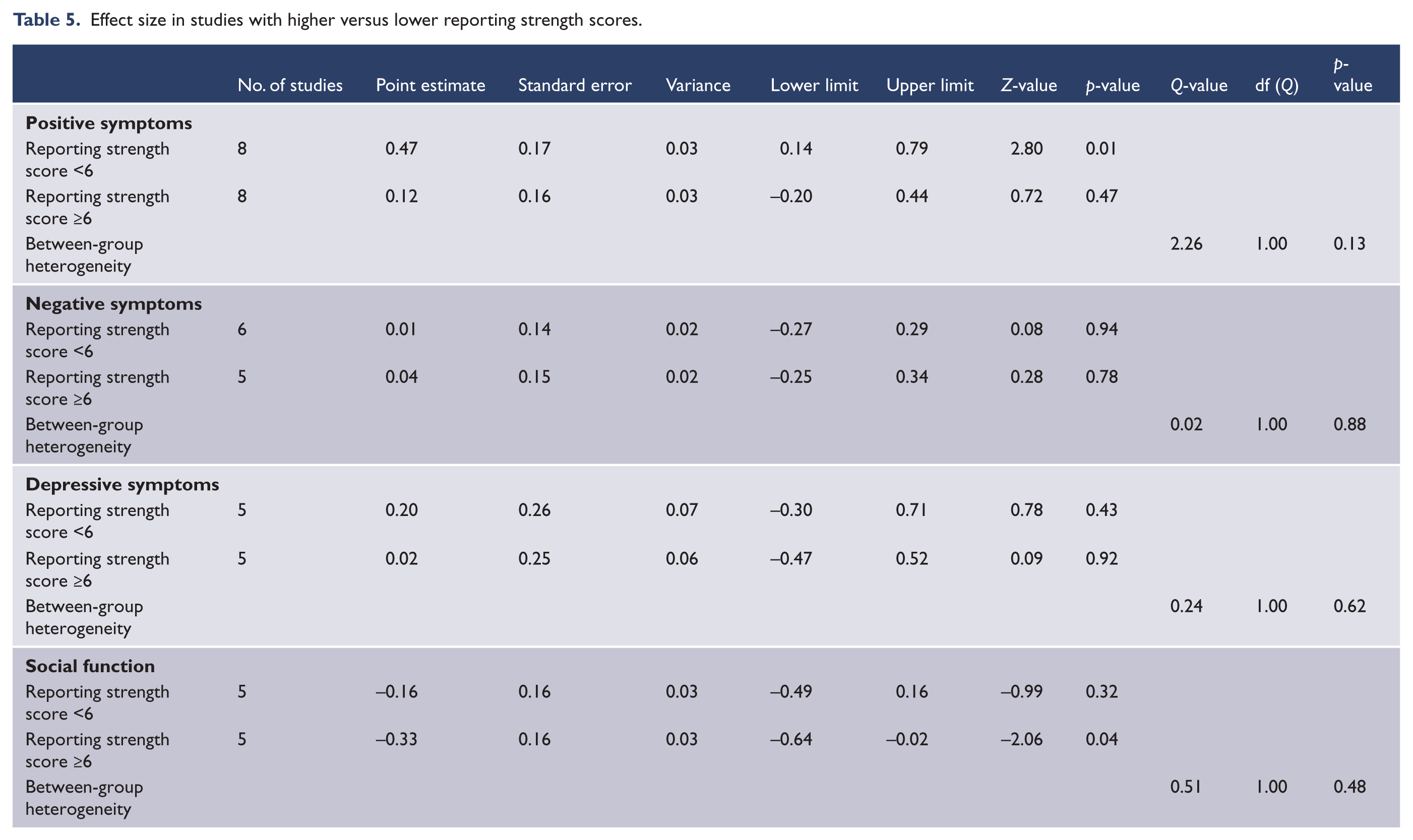
There were no significant between-group differences in the effect size for positive, negative and depressive symptoms, or for social function according to cannabis use versus other substance use (Table 3), studies of first-episode psychosis versus more established illness (Table 4) or studies with higher strength of rporting scores (Table 5).
Effect size in studies of substance use versus cannabis use.
Effect size in studies of first-episode patients versus non-first-episode patients.
Effect size in studies with higher versus lower reporting strength scores.
Discussion
Current findings compared to earlier meta-analyses
The results confirmed the association between current substance use and more severe positive symptoms found in an earlier meta-analysis (Talamo et al., 2006) which synthesized data from nine studies, including two of the 17 samples included in this meta-analysis. The methods of our meta-analysis differed from the Talamo study in two important respects. First, we excluded data relating to former substance users and second we were able to locate almost twice the number of studies reporting nearly three times the number of subjects. However, results of the previous meta-analysis are not directly comparable because the earlier study reported the change in the positive symptoms scale of the Positive and Negative Syndrome Scale (PANSS), whereas we reported the SMD, indicating a small to moderate effect of current substance use on positive symptoms (Rosenthal, 1996). Nevertheless, the finding of an association between substance use and positive symptoms by two meta-analyses that employed different analytical methods and samples of primary research in which there was only a small overlap suggests the existence of a robust association between substance use and more severe positive symptoms.
Contrary to our expectations, we did not find that patients with psychosis who used substances had significantly worse social function as measured by employment or scales of social function. This is a surprising result because substance misuse has a well-recognised potential to cause impairment in social function in the general population. However, the small number of studies available for our meta-analysis meant that our study lacked the statistical power to demonstrate small effect sizes. Further, we accepted a variety of methods for assessing social function that might have increased the degree of between-study heterogeneity and decreased the likelihood of a statistically significant result. Notably, social function was significantly impaired in substance-using patients when compared to non-substance-using patients in the subset of studies with stronger reporting methods and among first-episode samples. However, patients with cannabis use and psychosis might be less disabled because they have less severe cognitive impairment than non-cannabis-using patients (Yucel et al., 2012).
The results also suggest that current substance users have similar negative symptom scores to non-users, whereas two earlier meta-analyses that included nine studies (Talamo et al., 2006) and 11 studies (Potvin et al., 2006) (none of which were included in our meta-analysis because no study excluded former substance users) found that substance users had less severe negative symptoms than non-substance users. Our findings cast doubt on the earlier finding of less severe negative symptoms among substance-using patients with psychosis, which might possibly have been due to the inclusion of former substance users with mild negative symptoms in the substance-using group in earlier research.
The present study also failed to find a significant difference between current and non-substance users in their depressive symptoms, which also differs from the finding of the earlier meta-analysis (Potvin et al., 2007).
We had hypothesised that the inclusion of former substance users with either non-users or current users in earlier studies and the inclusion of those studies in earlier meta-analyses had minimised the extent of the differences between substance and non-substance-using patients. We found non-significant differences between current and non-substance users in measurements of depression and negative symptoms. Factors other than the way in which former substance users were classified might explain our failure to replicate earlier findings of fewer negative symptoms or more depressive symptoms among current substance users. There was a trend for studies with stronger reporting methods to find smaller differences in symptoms between the substance-using and non-substance-using groups. More recent studies also tended to report significantly smaller effect sizes for positive symptoms than older studies. Changes in the extent of the association between substance use and symptoms might be due to changes in patterns of substance use over time. For example, the previous meta-analyses included studies of alcohol and cocaine use (Potvin et al., 2006, 2007; Talamo et al., 2006) which were not the focus of the studies we included in our analysis, many of which were concerned with cannabis use.
Finally, the differences between the findings of our study and earlier research might be a result of differences in the diagnoses of patients included in the studies. The three earlier meta-analyses of positive symptoms (Talamo et al., 2006), negative symptoms (Potvin et al., 2006) and depressive symptoms (Potvin et al., 2007) compared substance-using patients to non-substance users with schizophrenia, whereas we included studies of patients with first-episode psychosis. However, differences in the type of study according to diagnostic inclusion criteria is an unlikely explanation for our non-significant results because the trend in our subgroup analysis of first-episode studies (that accepted a broader range of diagnosis in addition to schizophrenia) was for larger effect size differences between users and non-users in first-episode patients compared to those with more established illness.
Limitations of this study
The main limitation of our study was that the current substance users in the primary research were more likely to be younger and male than non-substance users. A lack of matching patients for age and sex in the primary research might have affected our results, and also the results of the previous meta-analyses. Younger age and male sex are associated with a poorer prognosis for psychotic disorders (Abel et al., 2010; Riecher-Rössler and Häfner, 2000), with poorer treatment adherence (Robinson et al., 1999) and more severe positive symptoms. The larger number of younger people and males in the current substance-using groups might have biased the study towards our main finding of significantly higher rates of positive symptoms among current substance users. Similarly, the finding of an association between continued substance use and criminal convictions and violence might simply be because younger males are the group of patients most at risk of substance use and committing acts of violence (Monahan et al., 2000).
The second limitation of our study relates to statistical power and sample size. While we had adequate power to detect moderate effect size differences in our four key outcome variables, our subgroup analyses comparing cannabis users with users of other drugs, first-episode and non-first-episode patients and studies with stronger and less strong reporting methods lacked the statistical power to reliably detect small effect size differences.
Conclusions
The relationship between substance use and psychosis is complex. Cannabis use is associated with an earlier onset of psychosis (Large et al., 2011) and a greater risk of developing schizophrenia (Moore et al., 2007). However, the role of other substances, such as stimulant drugs, in the genesis and course of psychosis, remains the subject of debate (Di Forti et al., 2007). Some forms of substance use might cause psychosis in susceptible individuals through a gene–environment interaction (Di Forti et al., 2012). However, it is possible that the observed association between substance use and positive symptoms might not be causal and could be partially explained by reverse causation and the self-medication hypothesis, whereby patients with more severe symptoms use substances in order to ameliorate distress (Hall and Degenhardt, 2000; Swendsen et al., 2011) or even by a spurious association resulting from coincidental demographic factors, such as young age and male sex (Sevy et al., 2010).
Some recent studies have added to the knowledge base about substance use and psychosis using a longitudinal examination of changes in substance use and symptoms over time (Barrowclough et al., 2013; Faber et al., 2012; van Dijk et al., 2012). Longitudinal studies do have some advantages over cross-sectional studies because they utilise an effective crossover design as patients reduce or increase their substance use. Longitudinal studies may be able to answer some clinically meaningful questions about the effect of stopping or reducing the use of various substances on patterns of symptoms. However, our review suggests there is a need for further cross-sectional studies that match for age, sex and stage of illness. Controlled cross-sectional studies could provide a better understanding of the effects of substance use on symptoms and social function in patients with psychotic illness.
Footnotes
Authors’ contributions
Dr Large has full access to all the data and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: Large; acquisition of data: Large, Gupta, Mullin; statistical analysis: Large; interpretation of data: Large, Gupta, Harris, Nielssen, Mullin; drafting of the manuscript: Large, Gupta, Nielssen, Harris, Mullin; administrative, technical, or material: Large; study supervision: Large.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper (see Authors’ contributions).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.