
Abstract
Background:
Australia introduced the Better Access scheme in late 2006, which resulted in a large increase in the provision of mental health services by general practitioners (GPs), clinical psychologists, other psychologists and allied health professionals. It is unknown whether this increase in services has had an effect on the mental health of the population.
Methods:
The following data were examined: per capita use of mental health services provided by GPs, clinical psychologists, other psychologists, allied health professionals and psychiatrists from 2006 to 2015 according to the Australian Government Department of Human Services; prevalence of psychological distress in adults (as measured by the K10) from National Health Surveys in 2001, 2004–2005, 2007–2008, 2011–2012 and 2014–2015; and the annual suicide rate from 2001 to 2015 according to the Australian Bureau of Statistics.
Results:
The large increase in the use of mental health services after the introduction of the Better Access scheme had no detectable effect on the prevalence of very high psychological distress or the suicide rate.
Conclusion:
Better Access has not had a detectable effect on the mental health of the Australian population.
Introduction
It is concerning that, despite large increases in the provision of treatment to people with mental health problems in high-income countries over recent decades, there has been no detectable decline in the prevalence. This finding has been reported for Australia, Canada, England, the Netherlands, New Zealand and the United States (Jorm et al., 2017; Mulder et al., 2017; Ormel et al., 2004). However, one of the problems in evaluating the population impact of increases in treatment, such as the steady rise in use of antidepressants, is that they typically occur gradually over many years. It is possible that any effects of increases in treatment on reducing prevalence are counteracted by other social changes occurring at the same which are having the opposite effect. Such counteracting social changes could include increasing exposure to risk factors or greater acceptability of reporting symptoms of mental health problems (Jorm et al., 2017). A stronger test of the impact of increasing treatment on population mental health would be provided if there were a large increase in treatment over a short period of time, approximating an interrupted time series. Such a situation has occurred in Australia with the introduction of the Better Access scheme in November 2006.
The Better Access scheme was designed to greatly expand the availability of psychological treatment under Medicare (Australia’s national universal health insurance scheme). Originally, Medicare only covered services by medical practitioners, including private psychiatrists. Access to psychological treatment was not widely available, being provided by the public health services funded by the states and territories, by paying full fees to private practitioners or having costly private health insurance which covered these services. Under Better Access, patients could be referred to a clinical psychologist, other psychologist or allied health practitioner (occupational therapist or social worker) by a medical practitioner as part of a GP Mental Health Treatment Plan or referred by a psychiatrist or paediatrician. A range of new billing items were added to Medicare to cover mental health services by general practitioners (GPs), clinical psychologists, other psychologists, allied health practitioners and psychiatrists. The new items for clinical psychologists, other psychologists and allied health practitioners were intended to support a range of evidence-based treatments, including cognitive-behaviour therapy (CBT), psycho-education, relaxation strategies, skills training and interpersonal therapy. The introduction of this scheme led to a rapid increase in the uptake of services provided by GPs, clinical psychologists, other psychologists and allied health practitioners, with the cost of these services far exceeding what was budgeted by the Australian government. By 2011, it was reported that the scheme was costing ‘more than three times its initial 4 year estimate of $538 million, or more than $10 million each week’ (Rosenberg and Hickie, 2011). From the beginning, there was considerable controversy about the scheme. Apart from the cost, there were concerns about inequities in the distribution of services, the model of care, the quality of the treatment provided and the adequacy of the evaluation commissioned by the government (Allen and Jackson, 2011; Hickie et al., 2011; Jorm, 2011; Meadows et al., 2015; Pirkis et al., 2011b).
Because the Better Access scheme was rolled out nationally in advance of any evaluation, data on its effectiveness could only be collected in retrospect, making it impossible to carry out a controlled trial (Pirkis et al., 2011a, 2011b). Some uncontrolled data were collected showing substantial improvement in symptoms (Pirkis et al., 2011a), but this has been criticized because of potential biases in the data collection (Allen and Jackson, 2011; Hickie et al., 2011). Nevertheless, it has been recognized that the impact of Better Access could eventually be evaluated using population data. Littlefield and Giese (2008) anticipated that the introduction of Better Access would have ‘a substantial impact on the mental health of the community’. Jorm (2011) proposed that ‘The big remaining question is whether Better Access has improved population mental health’ and that ‘Population monitoring of mental health is needed to find out whether this investment in treatment has been justified’. Hickie et al. (2011) concurred with this view, stating that ‘the next level of questions relate not just to health service effectiveness but wider population-health impacts (e.g. reduction in suicide, self-harm, income support, non-participation in education and employment)’.
The purpose of this paper is to report data relevant to the population mental health impact of the introduction of Better Access. Time series data are presented showing the increase in mental health services that occurred following the introduction of the scheme. Data are also presented on the prevalence of psychological distress in adults and the national suicide rate before and after the introduction of Better Access. This paper examines available data sets up to 2015, which corresponded to the year of most recent national data on prevalence of psychological distress.
Methods
Data on Medicare-funded mental health services from 2006 to 2015 were obtained from a publicly accessible online database provided by the Australian Government Department of Human Services (2018). The Medicare Benefits Schedule item numbers that were included in the analysis were those listed by the Australian Institute of Health and Welfare (2018) as covering mental health services by psychiatrists, GPs, clinical psychologists, other psychologists and other allied health providers over any part of this period, whether or not these were newly introduced with Better Access. Dates for items were determined by the date the service was processed by Medicare Australia, not the date the service was provided. Services per 100,000 population were calculated by dividing the number of services by the number of people enrolled in Medicare.
Prevalence of psychological distress was based on the K10 questionnaire (Andrews and Slade, 2001) administered in the National Health Surveys carried out in 2001, 2004–2005, 2007–2008, 2011–2012 and 2014–2015 to people aged 18 years or over (Australian Bureau of Statistics, 2002, 2006, 2009, 2012b, 2015). According to the Australian Bureau of Statistics (2017b), the data from these five surveys are considered to be directly comparable. The K10 was scored from a minimum of 10 to a maximum of 50, with scores of 22–29 being defined by the Australian Bureau of Statistics as ‘high’ and scores of 30–50 as ‘very high’. According to Andrews and Slade (2001), the probability of an International Statistical Classification of Diseases and Related Health Problems, 10th revision (ICD-10) mental disorder rises with K10 scores as follows: 20–24 55%, 25–29 75%, 30–34 85%, 35–39 91% and 40–50 99%.
Annual suicide rates per 100,000 persons for the years 2001–2015 were taken from data published by the Australian Bureau of Statistics (2012a, 2017a).
Results
Figure 1 shows the number of Medicare mental health services per 100,000 persons from 2006 to 2015. The number of services provided by GPs, clinical psychologists, psychologists and allied health practitioners rose steeply from the inception of Better Access, with some levelling off in more recent years. The services provided by psychiatrists, who had been covered by Medicare prior to Better Access, remained fairly steady over the period.
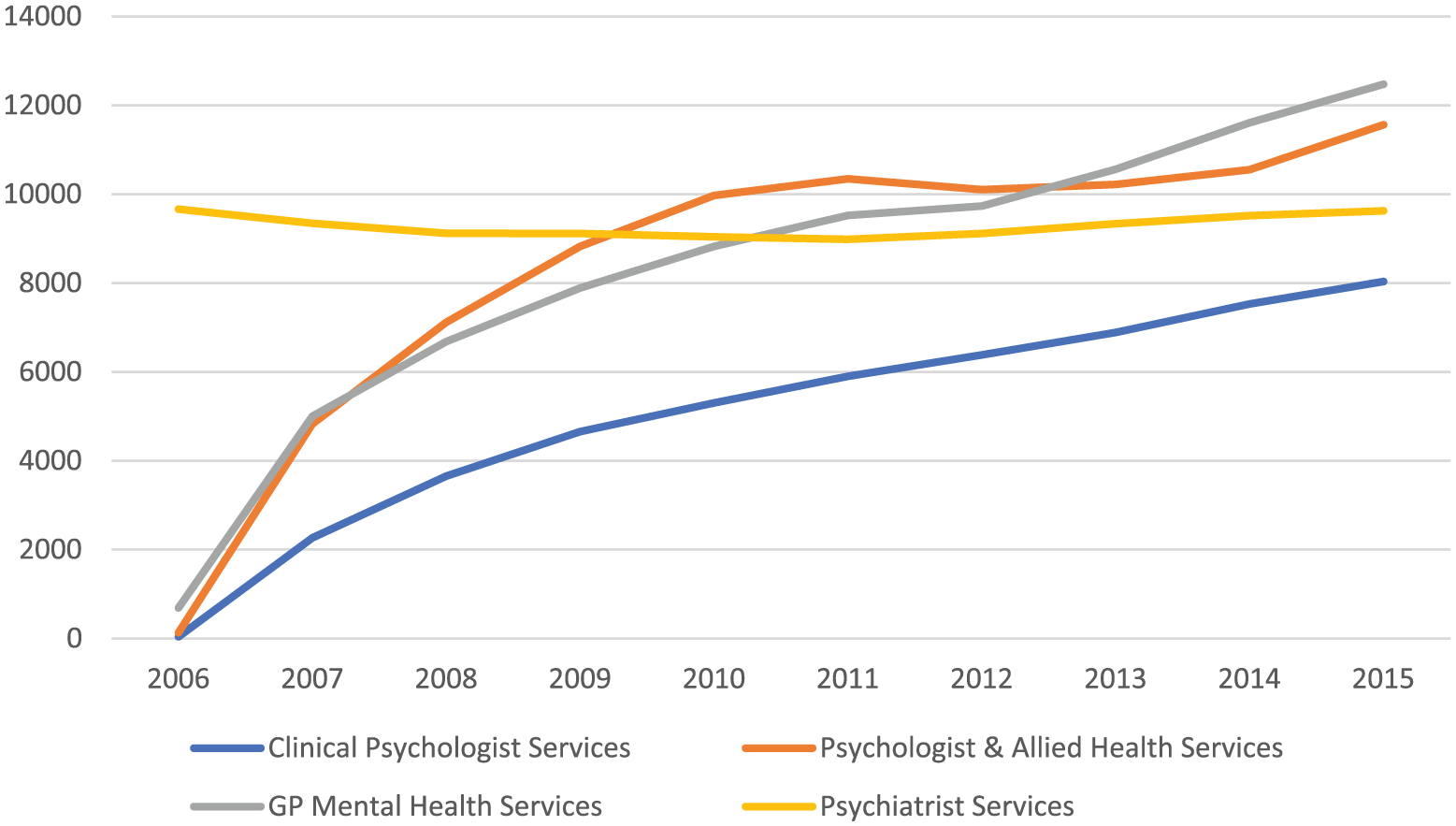
Medical Benefits Schedule mental health services (per 100,000 persons) by year since the Better Access scheme began in November 2006.
Figure 2 shows the prevalence of very high and high-plus-very-high psychological distress in adults aged 18 years or over at the five points where National Health Surveys were carried out. Two of these time-points (2001 and 2004–2005) preceded Better Access, one time-point (2007–2008) was during the phase of early implementation of Better Access and two points (2011–2012 and 2014–2015) were after Better Access was well established. The prevalence did not change over this period and was remarkably consistent for very high distress. Very high distress changed from 3.6% in 2001 to 3.7% in 2014–2015, while high-plus-very-high distress changed from 12.6% to 11.7% over the same period. According to the Australian Bureau of Statistics (2015), in 2014–2015 the 95% margin of error was ±0.4 for the prevalence of very high psychological distress and ±0.6 for high-plus-very-high psychological distress.
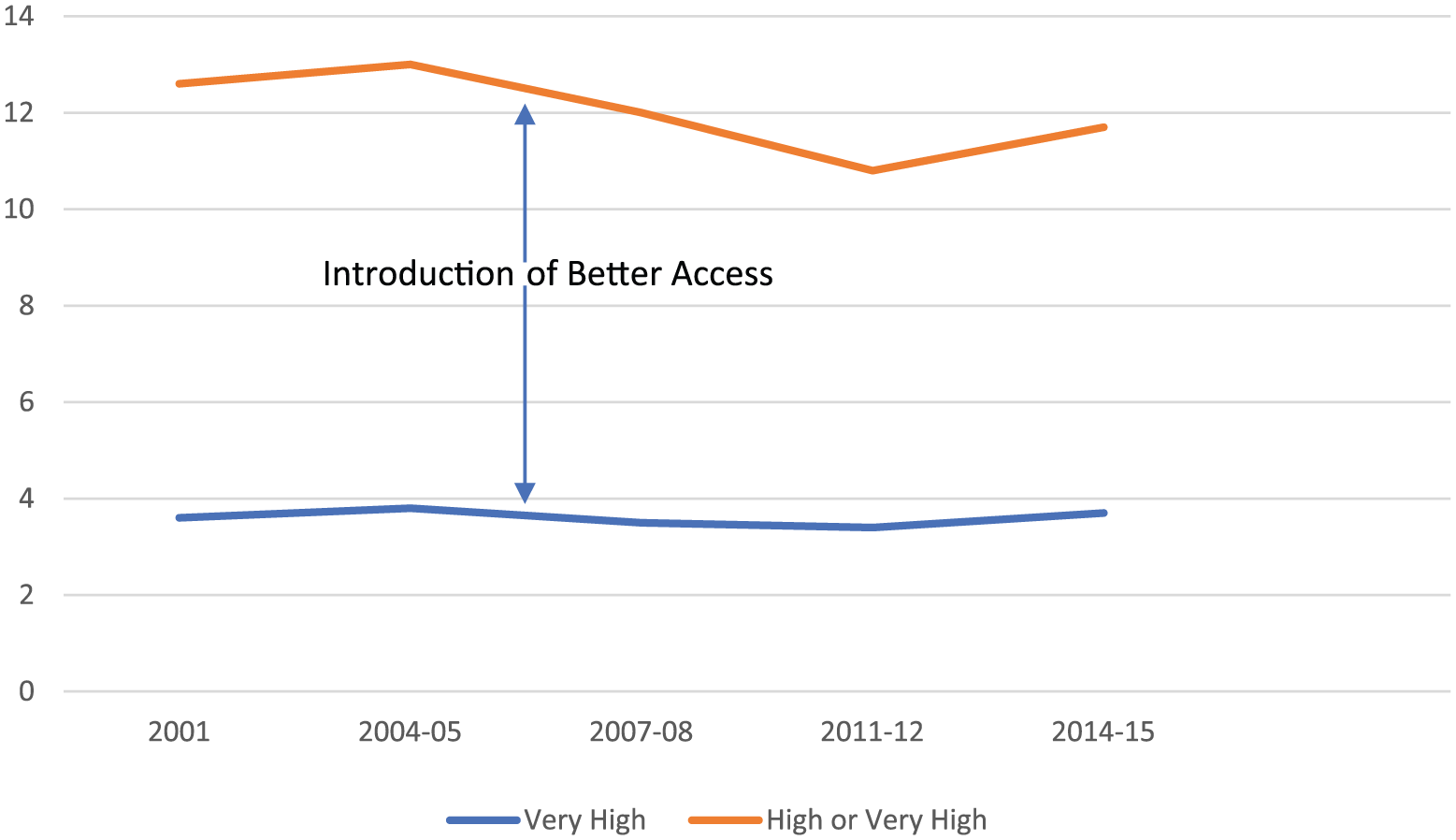
Prevalence (%) of psychological distress by year.
Figure 3 shows the annual suicide rate covering the same period as the National Health Surveys. Again, there is no indication that the suicide rate was affected by the introduction of Better Access.
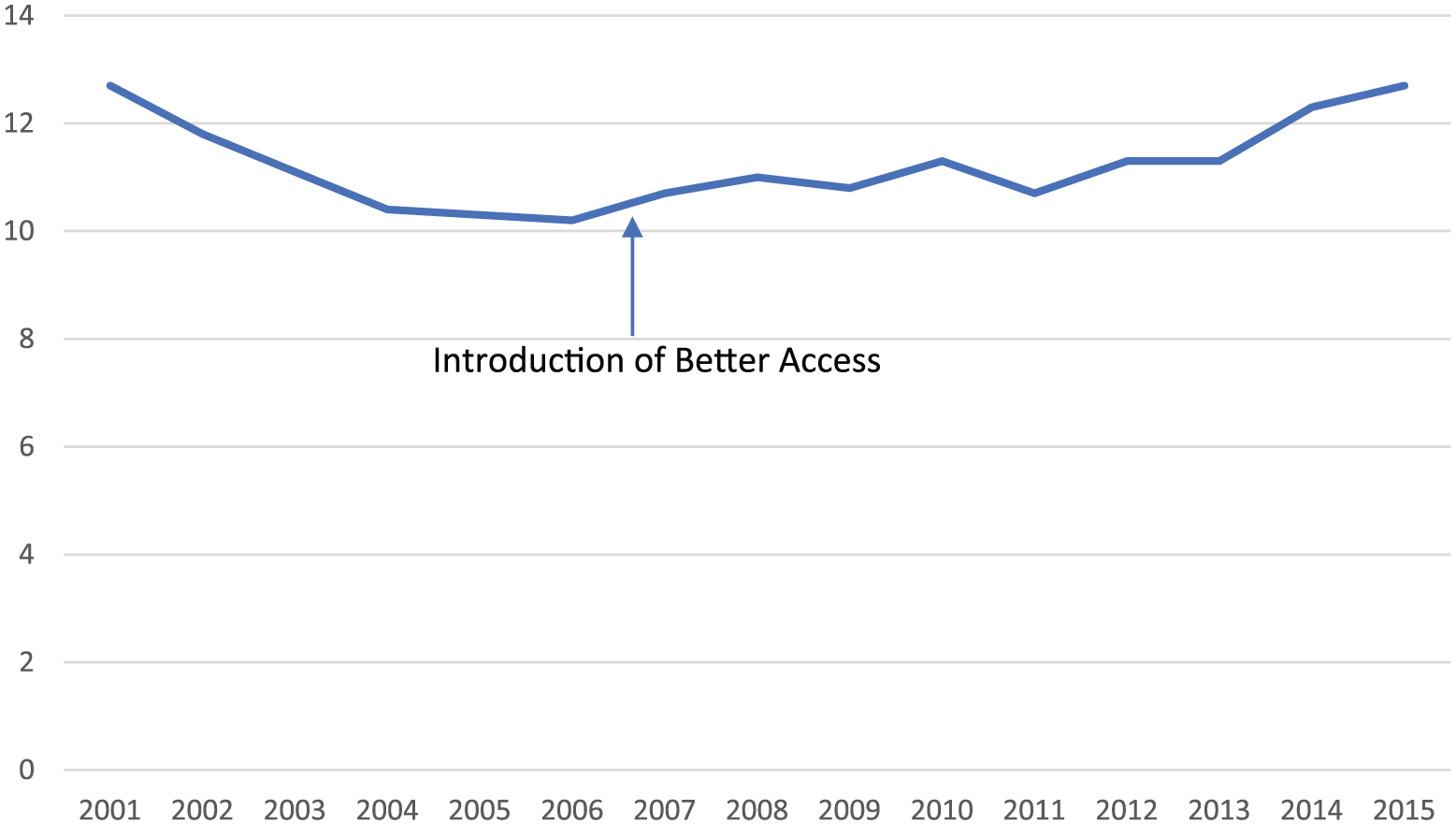
Suicide rate (per 100,000 persons) by year.
Discussion
Despite substantial increases in the provision of mental health services following the introduction of Better Access, there has been no discernable impact on the prevalence of psychological distress in adults or on the suicide rate in the total population. Because the increase in services under Better Access was so rapid, it is unlikely that other gradual changes in Australia, such as increased risk factor exposure or willingness to report symptoms, are masking any improvements in mental health. Given that Better Access funding is meant to cover evidence-based psychological treatments, the lack of impact of such a large increase in services is both surprising and concerning.
One possible explanation is that the dose of treatment has not been sufficient to produce population change. Harris et al. (2015) have defined ‘minimally adequate treatment’ as taking an antidepressant or mood stabiliser for 1 month or longer, plus four or more consultations with any medical practitioner for mental health; or receiving CBT or psychotherapy, plus six or more consultations of 30 minutes or longer average duration with any health professional (except a complementary or alternative medicine therapist) for mental health.
Because the three data sets analysed here are not linked, it is not possible to assess how many individuals at different levels of psychological distress received this level of treatment. However, it is possible to examine whether the total volume of treatment available in the population would be adequate if equally divided among those with greatest need. The group with greatest need is those with very high psychological distress, as they have a very high probability (over 85%) of having an ICD-10 mental disorder in the previous 12 months (Andrews and Slade, 2001). If we take the total number of Medicare mental health services for adults in the 2014–2015 financial year and divide it by the number of adults estimated to have very high psychological distress according to the 2014–2015 National Health Survey, we get a figure of more than 12 services per person, which well exceeds the threshold for minimally adequate treatment. However, if we take the larger high-plus-very-high group, we get a figure of 4 services per person, which would not meet the threshold.
Another possibility is that the services are not going to the people with the highest need. This cannot be determined from the data reported here. However, according to a non-representative sample of Better Access patients reported by Pirkis et al. (2011a) from 2009 to 2010, over half were in the very high distress group and over 80% in the high-plus-very-high distress group.
A third possible explanation is that the quality of the treatment provided is low – what has been termed the ‘quality gap’ (Jorm, 2015). Again, the current data cannot evaluate this possibility. While the item numbers added to the Medicare Benefits Schedule under Better Access are for interventions that have a strong evidence base, such as CBT, it is unknown whether practitioners provide treatments to the standards implemented in research trials. Indeed, Allen and Jackson (2011) have stated that ‘recent studies have found that many practitioners claiming to provide CBT either do not provide a treatment that conforms to the basic tenets of CBT, or do not deliver the treatment with adequate fidelity’ and ‘the assumption that these [Better Access] consumers have been receiving an evidence-based treatment akin to that evaluated in randomized efficacy trials is unwarranted’. Even where treatments are implemented with fidelity, their effectiveness may be limited. There is a continuing need to search for more effective treatments.
A final possibility is that increasing the provision of treatment does not address the major determinants of mental health problems in the community (Mulder et al., 2017). Numerous studies have been carried out on the factors associated with psychological distress as measured by the K10 questionnaire. Studies on Australian samples have shown that psychological distress is associated with unemployment (Reavley et al., 2011), low income (Enticott et al., 2018; Reavley et al., 2011), low social capital (Phongsavan et al., 2006), low social connectedness and social support (Atkins et al., 2013; Levula et al., 2018); workplace characteristics (Considene et al., 2017); poor quality diet (Hodge et al., 2013; Nguyen et al., 2017), limitations on physical functioning (Atkins et al., 2013; Byles et al., 2014) and physical diseases (Byles et al., 2014). There may be limits on how much change treatment can produce where such risk factors are present and persisting. Dealing with these risk factors may require a greater emphasis on prevention (Jorm, 2014) and on social factors that lie outside the domain of mental health services (Mulder et al., 2017).
The limitations of the data sets examined here must be acknowledged. While the Medicare data show a substantial rise in private practitioner services following the introduction of Better Access, they do not give the full picture on psychological services in Australia. In particular, they do not cover private psychological services prior to the introduction of Better Access or public mental health services funded by the states and territories. It is possible that the increase in services funded under Better Access was partly a shift in funding source for services that were already being provided. There are no data available to test this possibility. However, there are data showing that the growth in Better Access was not at the expense of an earlier smaller government-funded scheme, Access to Allied Psychological Services (ATAPS), which showed steady demand after the introduction of Better Access (Bassilios et al., 2010). Another limitation is that the three data sets are independent and cannot be cross-linked. To more fully examine the possibilities discussed above requires more detailed data on mental state and service use than currently available. Australia’s last National Survey of Mental Health and Wellbeing was in 2007, at a time when Better Access was just starting. To evaluate the current situation with Better Access would require a new national survey covering mental disorders, service use, risk factors, and with linkage to Medicare data. Longitudinal follow-up would also be necessary to investigate outcomes. Finally, the current evaluation only examined two population outcomes, prevalence of psychological distress and suicide rate, and did not cover other possible outcomes proposed by Hickie et al. (2011), including reduction in self-harm, income support, and non-participation in education and employment.
Conclusion
There is no detectable benefit to the mental health of Australians from the introduction of the Better Access scheme. The findings are consistent with previous reports from both Australia and other countries that large increases in treatment do not appear to reduce the prevalence of mental disorders. Such findings require considerable discussion by the mental health sector about future directions for service reform and caution against the practice rolling out service innovations nationally in advance of rigorous evaluation. The findings also indicate a need for the development of more effective treatments and for improved implementation of existing treatments in practice.
Footnotes
Acknowledgements
The author thanks Betty Kitchener and Amy Morgan for comments on the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an NHMRC Senior Principal Research Fellowship.