
Abstract
Objective:
The Zero Suicide Framework, a systems approach to suicide prevention within a health service, is being implemented across a number of states in Australia, and internationally, although there is limited published evidence for its effectiveness. This paper aims to provide a description of the implementation process within a large health service in Australia and describes some of the outcomes to date and learnings from this process.
Method:
Gold Coast Mental Health and Specialist Services has undertaken an implementation of the Zero Suicide Framework commencing in late 2015, aiming for high fidelity to the seven key elements. This paper describes the practical steps undertaken by the service, the new practices embedded, emphasis on supporting staff following the principles of restorative just culture and the development of an evaluation framework to support a continuous quality improvement approach.
Results:
Improvements have been demonstrated in terms of processes implementation, enhanced staff skills and confidence, positive cultural change and innovations in areas such as the use of machine learning for identification of suicide presentations. A change to ‘business as usual’ has benefited thousands of consumers since the implementation of a Suicide Prevention Pathway in late 2016 and achieved reductions in rates of repeated suicide attempts and deaths by suicide in Gold Coast Mental Health and Specialist Services consumers.
Conclusion:
An all-of-service, systems approach to suicide prevention with a strong focus on cultural shifts and aspirational goals can be successfully implemented within a mental health service with only modest additional resources when supported by engaged leadership across the organisation. A continuous quality improvement approach is vital in the relentless pursuit of zero suicides in healthcare.
Introduction
In 2015, the Gold Coast Mental Health and Specialist Services (GCMHSS), based in Queensland, Australia, commenced a large clinical reform initiative targeted at improving suicide prevention in the service. Suicide prevention has been an important focus for the GCMHSS for a number of years prior to this; however, as with other services, traditional approaches to safety and suicide prevention were yielding little change in outcomes. The reform was precipitated in part by a review of a death by suicide in the service, but also in response to a number of concerns with the status quo, including (1) challenges of a mental health service responding to consumers in crisis who do not necessarily have a psychiatric diagnosis, (2) ongoing use of risk assessment to stratify and predict risk despite evidence of ineffectiveness of such assessment (Large et al., 2011), (3) lack of focus on meaningful interventions, (4) fragmented training and (5) concerns about the impacts and outcomes of incident review processes which appeared to contribute to blame rather than learning from incidents. These issues were thought to be contributing to a sense of nihilism about the ability to prevent suicides.
A review of state, national and international frameworks for suicide prevention identified several evidence-based practices that could be adopted within mental health services and ultimately a Zero Suicide Framework (ZSF) was adopted. While not an evidence-based intervention per se, the ZSF approach provides an overarching framework for leadership, cultural change, change management, evaluation and innovation, while allowing for the implementation of clinical interventions most suited for individual services.
The ZSF adopts a systems approach to suicide prevention within health services that arose from recommendations by the National Action Alliance for Suicide Prevention (Covington et al., 2011). This report identified three critical success factors underpinning improvements in suicide prevention (Mokkenstorm et al., 2017): (1) suicide-specific, evidence-based practices; (2) reliably delivered by well-managed whole systems of care that are continuously improving service access, quality and safety; and that are (3) firmly rooted in core values reflecting a service culture that no longer accepts suicide as an outcome.
A shift in values and culture is facilitated by the relentless pursuit of the aspiration of zero suicides within a healthcare setting, through the delivery of high reliability healthcare (May, 2013). The framework addresses therapeutic nihilism by treating suicidality directly rather than using diagnosis as a gateway to treatment, and by emphasising individualised care planning and interventions as part of a clinical pathway of care, rather than a preoccupation with risk assessment as an end in itself. It also includes a strong focus on staff training and provision of a dedicated staff support service. Finally, the ZSF emphasises the importance of the involvement of people with lived experience, family and carers, clinicians, broader community groups and researchers in the development, implementation and evaluation of the initiatives.
The ZSF identifies seven essential elements: Leadership, Training, Identification, Engagement, Treatment and Transition of consumers, and Improvement. Table 1 describes the goals of each of those elements and summarises the steps undertaken by GCMHSS in their implementation. A toolkit of resources, developed by the Suicide Prevention Resource Centre (zerosuicide.sprc.org), was utilised in the implementation of the ZSF at GCMHSS, alongside many other evidence-based frameworks and practices identified during the preparation phase.
Elements of Zero Suicide Framework, associated goals and steps taken by GCMHSS in achieving those goals.
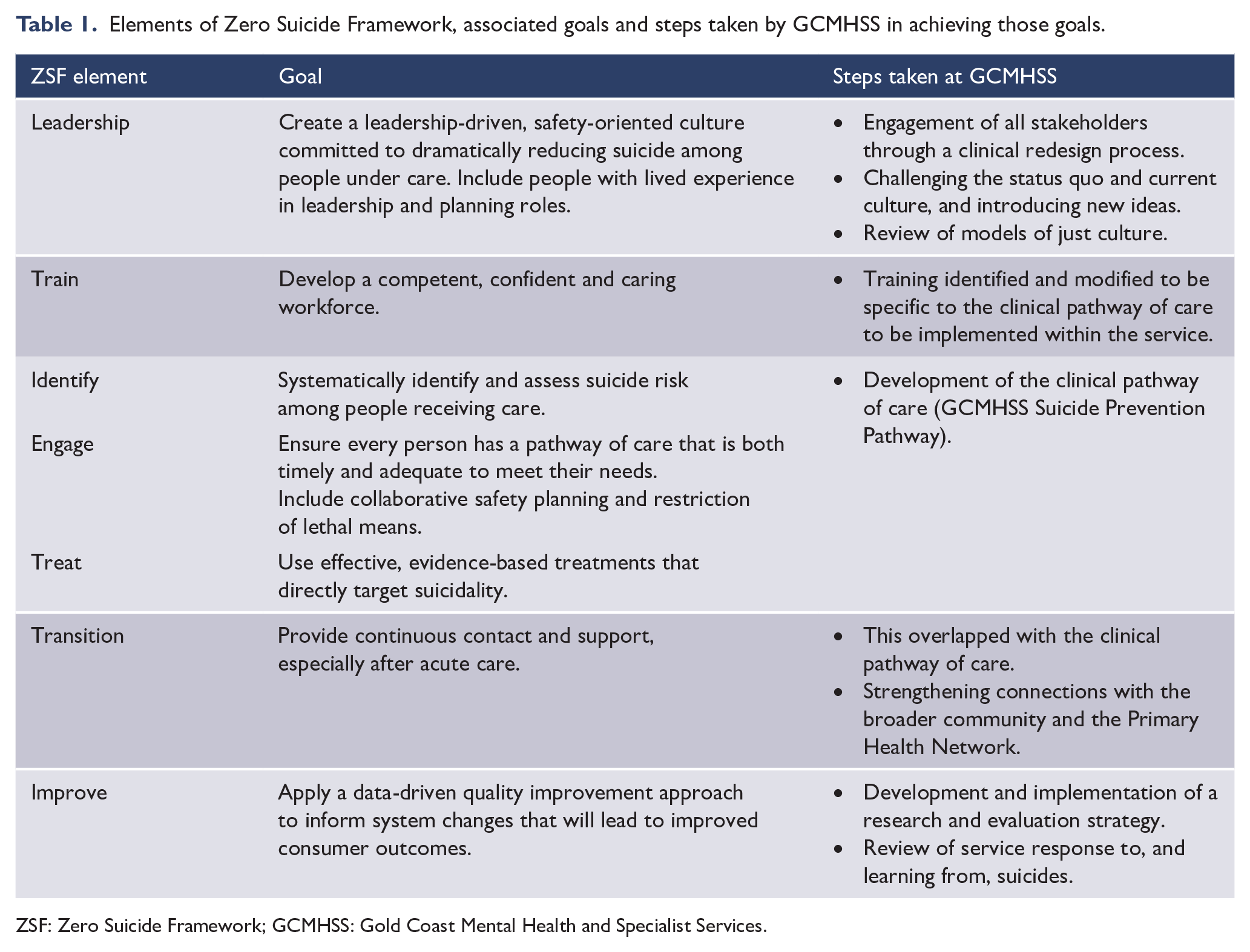
ZSF: Zero Suicide Framework; GCMHSS: Gold Coast Mental Health and Specialist Services.
The ZSF has seen a rapid adoption internationally, with considerable resources also invested in its roll out across Queensland and other parts of Australia (Queensland Health, 2017). At the same time, the framework has been subjected to some criticism over the lack of robust evidence of its effectiveness (Coyne, 2016; Mokkenstorm et al., 2017). Similarly, available (scholarly and grey) literature lacks a clearly documented example of a health service that has implemented this framework with a high fidelity to all its components, which represents a substantial gap in the literature. This paper has two aims: (1) to describe the process of the implementation of each of the seven key elements of ZSF at GCMHSS, and (2) to report on the key outputs and outcomes of the implementation.
Implementation of ZSF at GCMHSS
GCMHSS is a directorate within the Gold Coast Hospital and Health Service (GCHHS) which provides integrated mental health services across all ages to an estimated population of 600,000 people. Specialised crisis assessment and intervention is provided by a mental health Acute Care Team (ACT) for adults and the Access Team for people under 18 years presenting to Emergency Departments (EDs) of the Gold Coast University Hospital and Robina Hospital campuses, Gold Coast, Australia.
Leadership
‘Zero’ terminology
In addition to the potential benefits of the ZSF, the GCMHSS leadership group also recognised potential risks associated with the terminology of ‘zero suicide’, and whether it may exacerbate a blame culture and staff anxiety about suicide (Coyne, 2016; Smith et al., 2015). However, it was felt that a framework that explicitly and directly addresses what was felt to be a pre-existing blame culture was seen as particularly beneficial. Ultimately, it was decided that the Zero Suicide terminology would be used for several reasons, including the facilitation of a culture change through a bold and aspirational goal, while explicitly allowing for open discussion about issues of blame; a focus on a ‘zero defect environment’ and ‘high reliability healthcare’ when introducing a standardised care pathway; and ethical and moral concepts of ‘What other goal is there? What else is acceptable?’. These concepts were supported by our leadership, including our consumer and carer representatives.
An implementation and evaluation strategy was progressed, with the title Suicide Prevention Strategy 2016-2018: Journey to Zero through Leadership, Support and Continuous Improvement, clearly referencing the ZSF within written material. The strategy included a range of specific and measurable actions under each of the seven key elements.
Stakeholder consultation
An important first step by MHSS leadership was to undertake multiple consultation conversations with the Board and Executive of the Health Service and all levels of clinicians across GCMHSS. The aim was (1) to promote a nuanced message of aspiration towards zero; (2) to promote the goal of preventing, rather than predicting, suicides; and (3) to mitigate against the devastating impacts of suicide on consumers, carers and staff. The response from the Board and Executive was supportive. Clinicians were given an opportunity to express their fears and concerns, and there was a predominantly positive response, including comments that the proposal gave staff hope for the future.
Working groups
A Steering Committee and several working groups were established to address individual elements of the ZSF. The project manager role was undertaken by the existing Suicide Risk and Management Clinical Nurse Consultant (SRAM CNC). The working groups were led by senior staff from each service line and were made up of GCMHSS clinicians, consumers and carers, representatives from Patient Safety, the Emergency Department, Primary Health Network, and community members. One of the challenges for the leaders of working groups was their capacity to commit to the role given their full-time responsibilities. This was addressed by utilising a stepwise facilitated clinical redesign approach. Each lead was provided with a toolkit and steps to take towards rapidly developing an implementation plan over two workshops, supported by the project manager. Each working group presented to an ‘Expo’ which celebrated the achievements of the groups.
Just culture
As with other services that have implemented Zero Suicide internationally (Coffey, 2007; Coffey and Coffey, 2016), an emphasis on just culture was seen as crucial to its successful implementation. A review of literature on Just Culture was undertaken, and although initially more traditional approaches to Just Culture (Marx, 2001; Reason, 2016; Wachter and Pronovost, 2009) were considered, a decision was made that Restorative Just Culture (RJC) provided a more compelling way forward. A separate publication outlines learnings about the importance of RJC in the context of ZSF implementation (Turner et al., 2020).
Training
Staff training is a core aspect of the ZSF. An expectation is that all staff are first assessed for their beliefs, training and skills needed, which is followed by the provision of the training appropriate to their role (Mokkenstorm et al., 2017). At GCMHSS, a staff survey ‘Voice of Staff’ (VOS) was developed, based on the ZSF Workforce Survey from the website toolkit. In early 2016, before the official roll-out of the Suicide Prevention Strategy, the survey was completed by 256 persons, which accounted for around 40% of all MHSS staff. The results indicated that despite suicidal assessment and management being a central part of the clinicians’ responsibilities, almost 40% felt they hadn’t received the necessary training, and between 20% and 30% did not believe they had the necessary skills or confidence (GCMHSS, 2020a). This deficit was more pronounced in interventions than assessment. These results are not dissimilar to results found in other organisations (Silva et al., 2016).
A training course (online and 1 day face to face) was developed, which saw a partial adaptation of the state-wide training Suicide Risk Assessment and Management for Emergency Department Settings (SRAM-ED) provided by the Queensland Centre for Mental Health Learning (QCMHL). The course includes a reflection on the clinicians’ attitudes and beliefs in relation to suicide, building a therapeutic alliance, risk factors and warning signs, the Chronological Assessment of Suicide Events (Shea, 2009a, 2009b) approach and safety planning. The adaptation of the training package which supported the GCMHSS-specific pathway of care saw the replacement of the categorical risk statement which was in line with the state-wide documentation at the time with the Prevention Oriented Risk Formulation (Pisani et al., 2016), and the inclusion of specific reference to Aboriginal and Torres Strait Islander people, older persons, child and youth, LGBTIQAP+ and culturally and linguistically diverse (CALD) communities. This adaptation was enabled by a supportive partnership approach with QCMHL.
Training was supported through the addition of a 0.6FTE clinical psychologist to provide in-service education to teams, modelling and constructive feedback on clinical practice and documentation. Orientation for new staff now includes this content as core training. In subsequent years, a small additional resource of lead clinician time has been added to assist with embedding processes within the service, initially in the adult service line and then the Child and Youth Service line. This was in part due to support from the Queensland Mental Health Alcohol and Other Drugs Branch Multisite Collaborative which supported the implementation of Zero Suicide across multiple Queensland services (Queensland Health, 2017). GCMHSS also provided support and resources to multiple sites across Queensland in our role within the Multisite collaborative.
Identify / Engage / Treat – the Suicide Prevention Pathway
The process of developing the GCMHSS Suicide Prevention Pathway (SPP) (Figure 1) began by reviewing relevant literature and mapping the service’s current procedures. The overarching structure of the SPP was shaped by the following principles:
The SPP would guide all staff across the service and would be considered a change to ‘business as usual’;
The SPP would need to be implemented within existing clinical teams with no additional resources (apart from modest additional resources for training and data collection);
Avoidance, where possible, of any increase in mandatory clinical documentation;
Support for engagement and standardisation through a clinical pathway, but avoidance of a ‘tick box’ approach to care;
Enhancement and refinement of processes to build on existing skills rather than replacing already embedded approaches.
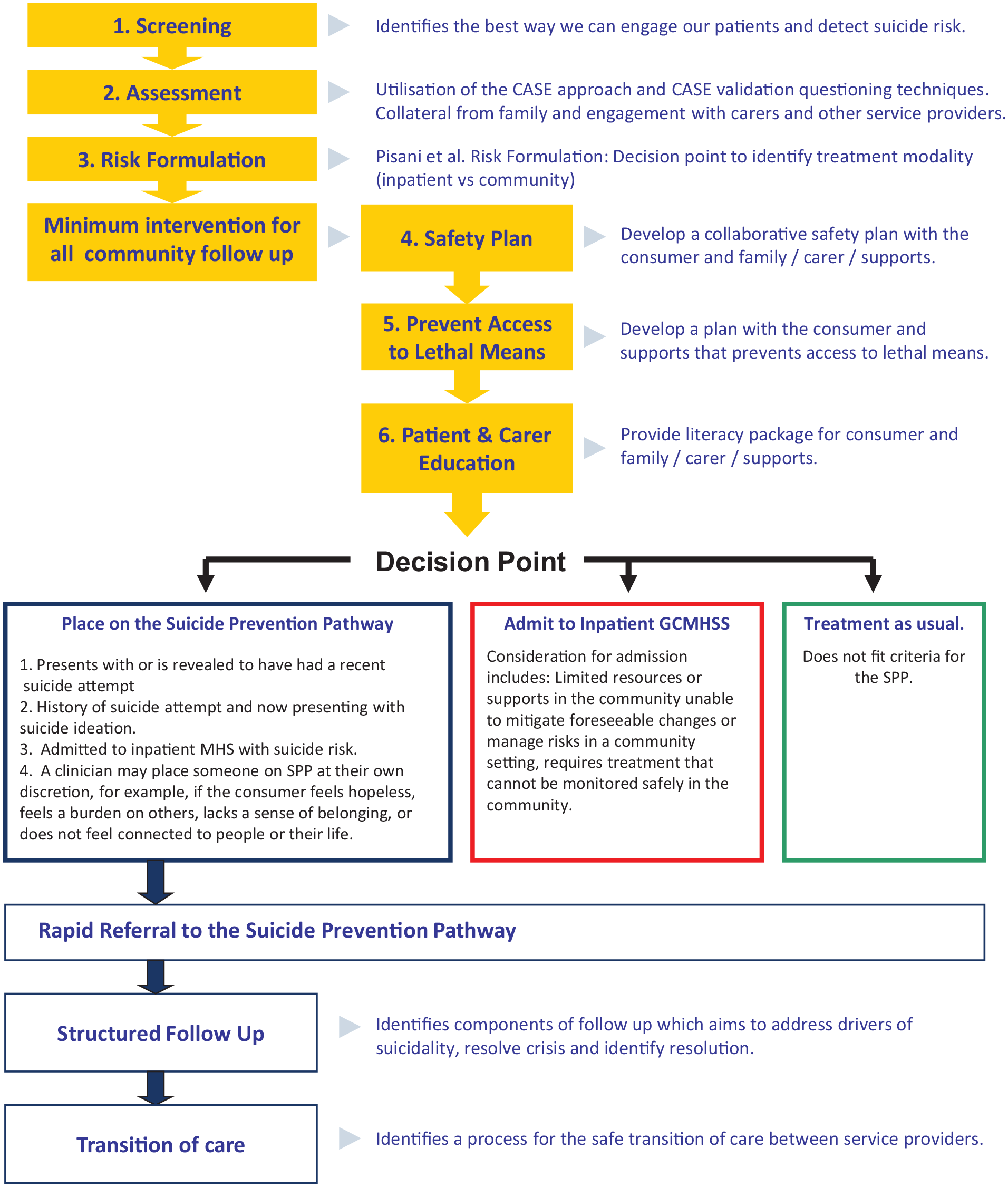
GCMHSS Suicide Prevention Pathway.
Screening
Screening to identify consumers at risk of suicide is an important component of the ZSF; however, it was also recognised that a screening tool should not be used to determine access to interventions or to predict risk. For the purposes of the SPP, the UK Mental Health Triage Scale (Sands et al., 2016) was selected and endorsed at a state level and embedded in the Electronic Medical Record.
Assessment
Clinicians’ existing skills in assessment were enhanced by introducing the Chronological Assessment of Suicide Events (CASE) approach which assists the clinician to explore suicidal ideation, planning, behaviours and intent, while maximising engagement with the consumer (Shea, 2016). A strong therapeutic alliance and collaborative, non-judgmental stance is key to the CASE approach, which complements the broader comprehensive psychiatric assessment that includes risk and protective factors, and warning signs (Shea, 2016).
Formulation of risk
Despite warnings that categorical stratification of suicide risk (high, medium, low) is not helpful in predicting future risk of suicide (Chan et al., 2016; Large et al., 2011; Mulder et al., 2016) or in determining who should receive what services, moving away from risk categorisation was seen as a challenge, with limited available alternatives. Authors advocating for abandoning risk categorisation argue for the importance of the engagement with the consumer, building a strong therapeutic relationship, understanding the act of self-harm and developing a management plan in collaboration with the consumer (Chan et al., 2016; Mulder et al., 2016; Ryan et al., 2015). Pisani et al. (2016) addressed these concerns by developing the Prevention Oriented Risk Formulation which provides an algorithm to integrate information gathered in a comprehensive assessment. It provides a synthesis based on relative, contextually anchored risk relative to specified subgroups (risk status) and relative to the consumer’s own baseline (risk state). The formulation then assesses available internal and external resources, and foreseeable changes that, if they occur, might lead to a rapid change in risk (Pisani et al., 2016). Importantly, the risk formulation is not used for predictive purposes or to determine acceptability for treatment, but rather enables broader understanding of the issues for the person in crisis, so that an individualised, forward-looking collaborative plan can be developed (see Figure 2).
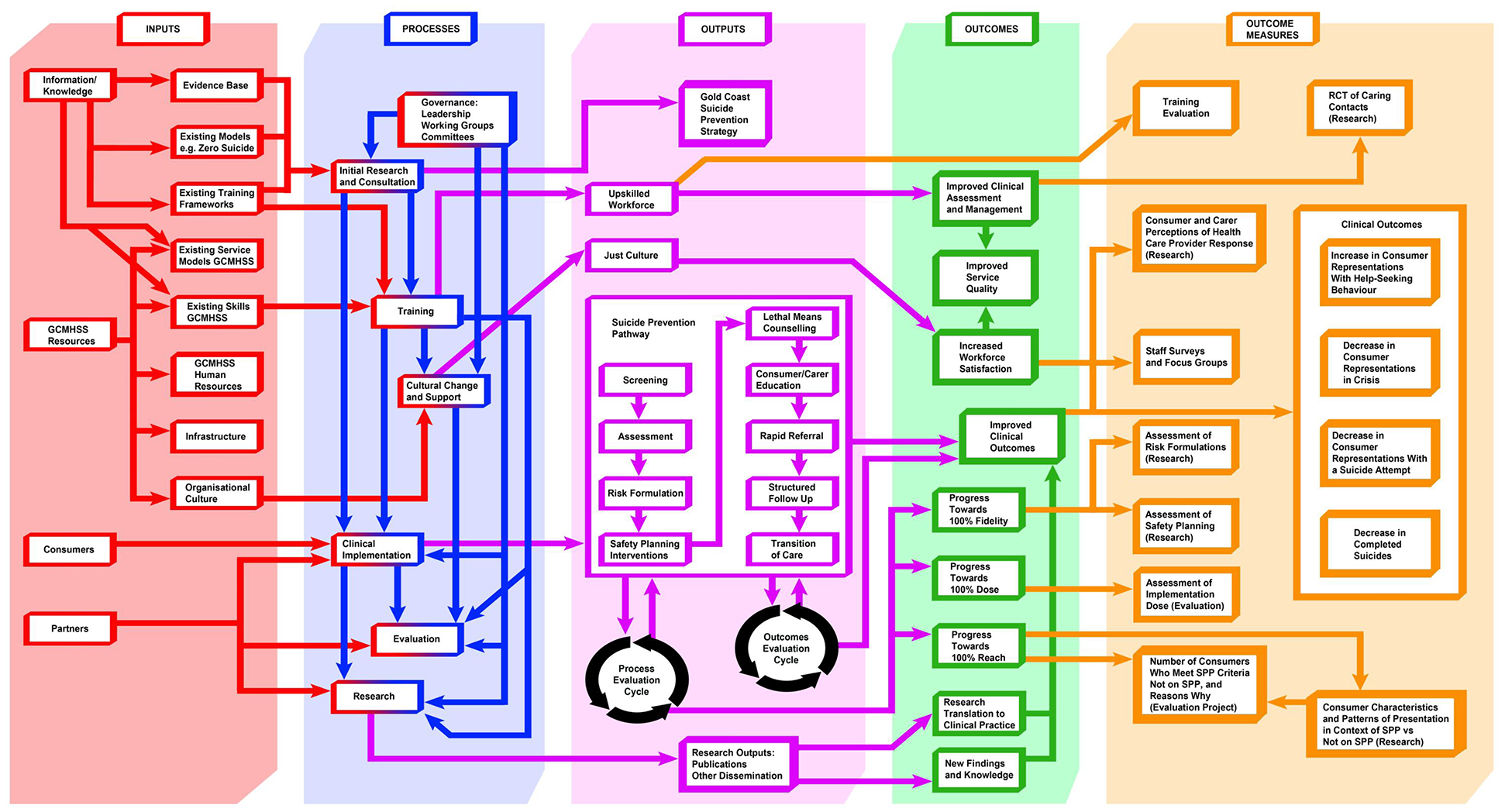
Logic model for the GCMHSS Suicide Prevention Strategy.
Additional reasons for implementation of this risk formulation were that it would allow clinicians to feel more comfortable in documenting risk factors when developing management plans and alleviate pressures to describe a consumer as ‘low risk’ prior to discharge.
Brief interventions
Key in the development of the SPP was an exploration of ‘universal interventions’ that would help enhance the safety of consumers as part of an individualised care plan. The ED setting was a focus, as it offers an opportunity for brief interventions with a high-risk group who can be challenging to engage in follow-up care (Stanley et al., 2016).
In 2015, the Suicide Prevention Resources Centre published ‘Caring for Adult Patients with Suicide Risk: A Consensus Guide for Emergency Departments’ which outlined several evidence-based brief interventions that could be implemented in a busy ED prior to discharge. In consideration of the capacity of our service at the time, five of those interventions were implemented as part of the GCMHSS SPP:
Safety Planning Intervention (SPI);
Counselling on Restricting Access to Lethal Means (contained within the SPI);
Crisis Numbers (contained within the SPI);
Brief Patient and Carer Information;
Rapid Follow-Up.
SPI, counselling on access to lethal means, crisis numbers
Suicidal thoughts often fluctuate over time (Sveticic and De Leo, 2012). Thus, consumers who are given skills and strategies for future use may be able to resist and delay acting on those thoughts until the thoughts subside or they are able to access care. The SPI is a prioritised set of coping skills and supports, developed in collaboration with the consumer, and, ideally, a family member or other support person (Stanley and Brown, 2012). The SPI includes individualised warning signs, internal coping strategies, social contacts to distract from suicidal thoughts, social and professional supports to assist with resolving suicidal crises, and strategies to restrict access to lethal means of suicide. There is growing evidence that a SPI improves engagement with consumers, helps in resolving their suicidal crisis (Stanley et al., 2016) and may reduce repeated self-harm and overall suicide risk (Chang et al., 2016).
A Safety Plan, based on the SPI by Stanley and Brown (2012), was developed for inclusion in the GCMHSS SPP. GCMHSS added two questions at the beginning about the drivers of suicide and the measures they felt would assist in resolving these issues. The form also captures the consumer’s current address and information on how to contact them and who to contact if we were not able to reach them (which also pre-emptively allowed for a discussion around contacting family or friends if the person was uncontactable). Information on the 24-hour crisis numbers was also included.
Brief patient and carer information
A Patient Brochure and a Family/Carer Brochure, developed in consultation with GCMHSS representatives of people with lived experience, are given to consumers on the SPP.
Rapid follow-up
Effective transitions of care are of central importance in the ZSF, considering the elevated risk of suicide in the post-discharge period (Bickley et al., 2013); however, engaging with consumers following a suicide attempt can be very challenging. Between 50% and 70% of people do not engage with their first follow-up appointment after presenting with suicide attempts, however, scheduling the first appointment within 2 to 3 days, and an intensive outreach in the post discharge period has been shown to improve the chances of follow-up engagement (Knesper, 2010). Although challenging from a resource perspective, in the majority of cases, we found that patients can be given an appointment date and time for their follow-up within 48 hours, prior to leaving the ED.
Structured follow-up
Staff were provided a framework to support follow-up care in the community, spanning these steps:
Mood check and assessment of current suicidality;
Review and revision of the safety plan;
Creation or updating of a care plan;
Ensuring communication with carers, family and other health professionals;
Identification of other agencies required, and referral;
Agreement on a plan and next appointment as well as identification of any barriers to treatment.
The principle of ‘warm handovers’ was emphasised, where the consumer would ideally have their first appointment with the next health provider prior to closure from GCMHSS.
Implementation of the SPP
Who would go on the SPP?
The SPP was implemented for all age groups and across the GCMHSS without any increase in clinical workforce, therefore requiring a pragmatic approach to identifying consumers to be placed on the SPP. The following criteria were implemented for referral to the SPP:
Anyone presenting following a suicide attempt, or with a recent suicide attempt;
Anyone with a history of a suicide attempt, and presenting with suicidal ideation;
Anyone admitted to the inpatient unit due to suicide risk;
At the treating clinician’s discretion.
Commencement of the SPP
The SPP was implemented in December 2016, following training of all medical and community staff. Inpatient staff were trained several months later due to the competing priority of implementation of the new Mental Health Act in early 2017. Supports provided included the following:
Training manual and posters;
A 2-week roster of senior clinical staff to attend ED and ACT Community teams on each shift, to provide hands-on support for staff as they gained a working knowledge of the SPP;
Regular meetings with senior management of GCMHSS and the ACT leaders to troubleshoot any issues;
A senior psychologist provided one-on-one consultations and presentations to teams to support the implementation of the SPP and building of new skills;
Regular newsletters showing data on the fidelity to the SPP, tips for improvement and links to training materials to refresh knowledge and skills;
Introduction of an alert in the electronic medical record so that consumers on the SPP could be readily identified, allowing for data-driven continual quality improvement and provision of feedback to clinicians.
Responding to an increased workload
Shortly after the commencement of the SPP, ACT was overwhelmed by an increased workload. Leadership meetings were held daily to explore and respond to this challenge. It was thought that some of the increased load was temporary, as clinicians gained familiarity with the processes. A temporary diversion of clinicians from other parts of the service to ACT occurred over a 2-week period, which was sufficient to address the backlog and allowed for the development of streamlined processes. The ability of ACT team to absorb the additional workload highlighted the importance of an agile, collaborative and all-of-service approach to this work, and a culture that supported resilience and flexibility of the system in addressing challenges when they arose.
Transition
In addition to transitions from the ED, the safe transitions from GCMHSS to ongoing community care were also considered. The local Primary Healthcare Network worked in collaboration with GCMHSS at the initiation of the SPP to fund an initiative called Lotus, which is run by a non-government organisation and co-located in ACT. This has now transitioned to the Way Back Service (Beyond Blue, 2020), which provides non-clinical support for up to 3 months after discharge and is available to anyone on the SPP.
Improve
Research and evaluation
The implementation of SPP had a strong focus on data-driven evaluation to enable timely feedback to clinical teams and to progress a continuous quality improvement approach. It was deemed important that evaluation implementation occurred in parallel with clinical implementation. Simultaneously, it was identified that research questions were likely to arise and would be developed into research projects pursuant to obtaining grant funding or other resources.
The Research and Evaluation working group developed a logic model (Figure 2) for the evaluation of the SPP which included process and outcomes evaluation. Process evaluation is concerned with monitoring whether individual components of the SPP are implemented as intended (fidelity), the proportion of the interventions that are implemented (dose), and finally, what percentage of the targeted population has engaged with the SPP (reach) (Moore et al., 2015; Wilson et al., 2009). Outcome evaluation monitors short- and long-term outcomes for consumers engaging with SPP, specifically changes in help-seeking behaviours, representations with suicide attempts and deaths by suicide.
Sourcing the data to inform outcome evaluation of a ZSF is challenging, and our team noted substantial under-enumeration of suicidal presentations in ED administrative data (Sveticic et al., 2020). To overcome this challenge, a machine learning approach was used to develop software for the identification of suicidal presentations, titled Searching EDIS for Records of Suicidal Presentations (SERoSP). SERoSP has proven to be a time- and cost-effective solution to obtaining data on suicidal presentations required for the evaluation of the SPP (Stapelberg et al., 2020).
Responding to and learning from deaths by suicide
Implementation of the new Suicide Prevention Strategy required the creation of a substantial cultural change and supportive environment not only for consumers presenting in suicidal crises but also for our staff. To that end, we performed a review of the literature on just culture and examined current experiences of staff through focus groups and surveys. Consequently, two large pieces of work were undertaken.
Staff support programme ‘Always There’
In 2017, the VOS identified the need to strengthen organisational support offered to staff members involved in critical incidents. Staff identified the need for a timely, reliable response following a traumatic event or as a result of a cumulative or vicarious stress. In response, a staff support programme ‘Always There’ was developed based on Scott’s Model of Peer Support Intervention (Scott et al., 2010), the GRACE model of compassion (Halifax, 2014), the Social Resilience Framework (Paton and Johnston, 2001) and Denham’s five rights of the second victim (Denham, 2007). The ‘Always There’ staff support programme provides a confidential, rapid response to staff involved in a critical incident (suicide-related or otherwise), and all staff who may be experiencing cumulative and vicarious stress reactions. The responder team includes volunteer peer supporters who undergo an 8-hour training on providing emotional and practical support using the principles of psychological first aid. Between December 2018 and May 2020, the programme has delivered 189 interventions.
Responding to, and learning from, critical incidents
A new approach to learning from clinical incidents, Gold Coast Clinical Incident Response Framework (GC-CIRF), was developed, which was structured around principles of RJC (including the strong engagement of all stakeholders), human factors, complexity and safety II (GCMHSS 2020a; Turner et al., 2020). The new process also supports enhanced quality and strength of recommendations arising from these reviews.
Achievements so far
A range of evaluation strategies were put in place from the outset, which aimed to capture cultural changes, uptake and fidelity of the SPP, and the effectiveness of the SPP, by monitoring the rates of suicide re-attempts and deaths by suicide.
Cultural change
Organisational cultural change is underpinned by changes in patterns of behaviour, values and meanings (Meyerson and Martin, 1987). The VOS survey conducted periodically with mental health clinicians has shown encouraging trends in the shifting of staff beliefs, attitudes and values, as well as changes in behaviour such as acquiring and implementing new skills. In 2019, 315 staff members, accounting for 50.0% of the MHSS workforce, participated in the survey (GCMHSS, 2020a). Of those, 76.8% felt they had received the training needed to help consumers at risk of suicide (compared to 61.5% in 2016), and 83.2% were confident in their ability to manage consumers’ suicidal thoughts and behaviours (compared to 68.9% in 2016) (GCMHSS, 2020a). Significant changes were also observed in the staff rating of the commitment GCMHSS has made towards improving approaches to suicide prevention.
In addition, several domains of just culture and second victim experiences have shown significant improvements since initiatives improving incident reporting processes and staff support programme were introduced in 2018 (Turner et al., 2020). In 2019, over 60% agreed that the organisation understands that staff may need help in processing and resolving potential effects of their involvement in incidents and offers a variety of resources in overcoming these. Furthermore, in comparison to 2017, in 2019, less staff reported that involvement in a critical incident caused feelings of professional inadequacy (26.7%) or being risk-averse (21.1%). Finally, 60% of staff in 2019 reported feeling emotionally supported at the time incident occurs and during the review process, and nearly 75% stated that involvement in an incident did not damage the trust and relationship within their team (GCMHSS, 2020a). While the results show significant improvement from 2017, they reinforce the importance of ongoing work to address these issues.
Operational implementation of the SPP
Data on the consumers placed on the SPP and information about the completion of SPP components are recorded as part of routine care and document keeping by the treating clinical team and communicated to a GCMHSS research officer. In the 3 years since the implementation of SPP to December 2019, GCMHSS has successfully placed 4744 consumers on the SPP; on average, 129.0 (SD = 31.6) per month. This number has been increasing steadily (see Figure 3), reflecting both an increase in demand and an increase in appropriate identification of consumers who meet criteria for the SPP.
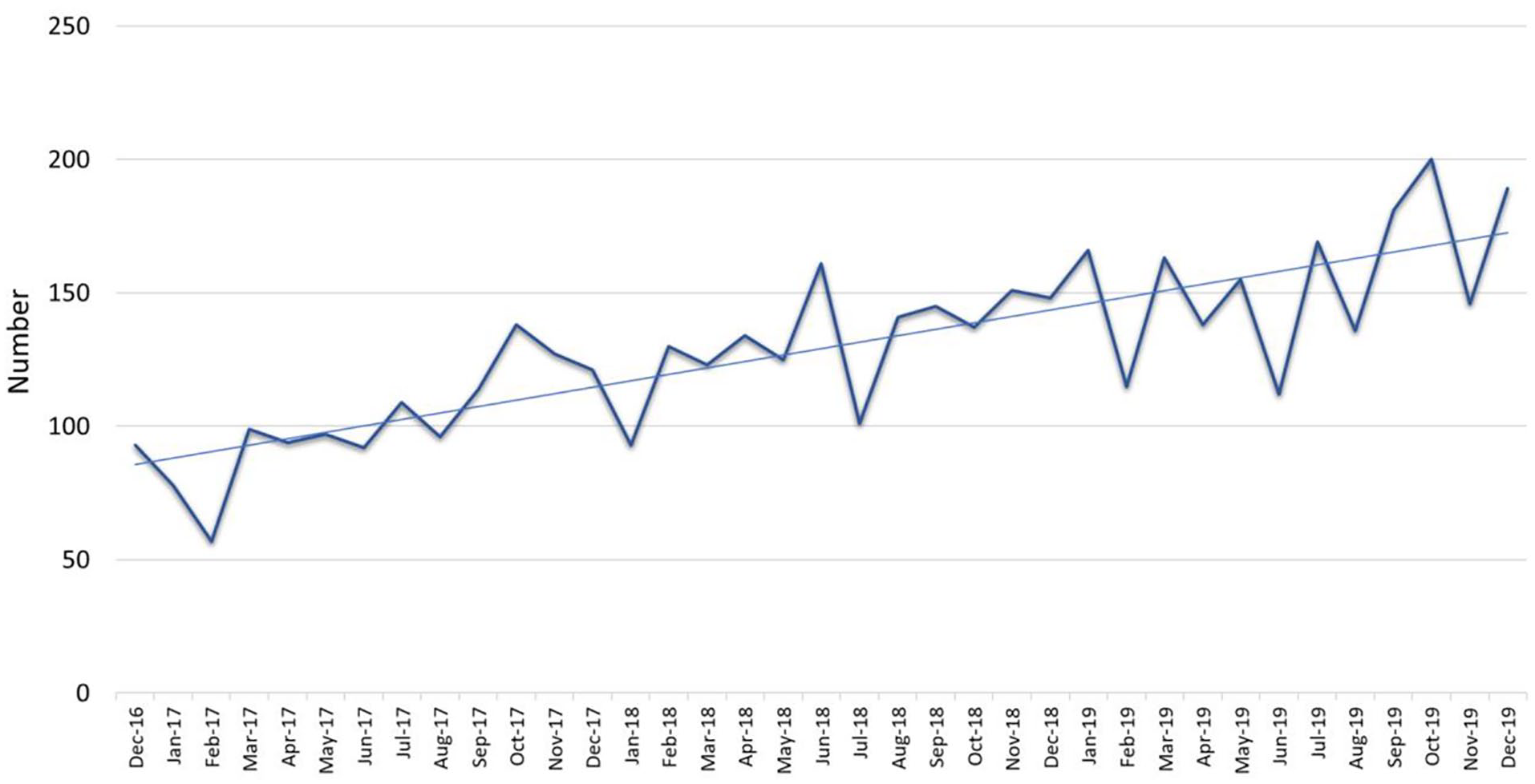
Number of consumers placed on Suicide Prevention Pathway.
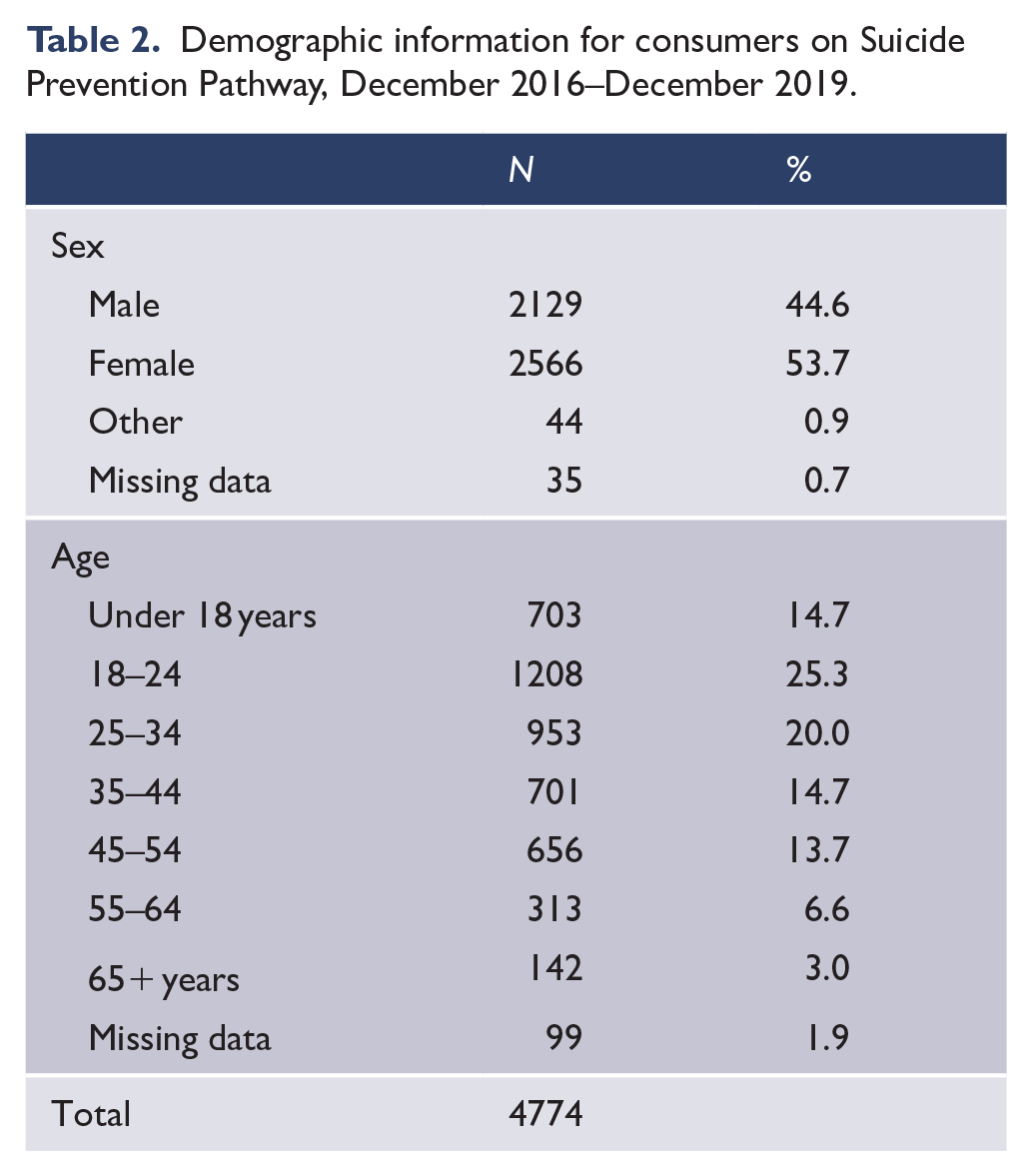
Table 2 presents basic demographic information of the consumers placed on SPP between December 2016 and December 2019. Just over half of consumers on SPP were females (53.2%), 45.1% were males and around 1% identified as intersex, non-binary or transgender. The average age of consumers placed on SPP was 32.5 years (SD = 15.2, min = 6, max = 91). Around 15% of consumers on SPP were under the age of 18, and the largest proportion were between the ages of 18 and 34 (combined, they accounted for 45.6% of all SPP consumers).
Demographic information for consumers on Suicide Prevention Pathway, December 2016–December 2019.
Implementation dose (completeness) of the SPP components
Implementation dose (completeness) of individual components of SPP is presented in Table 3 for the selected months of March and April prior to the implementation of SPP (2015) and in the three subsequent years after implementation (2017–2019). The 2015 data pertain to suicide attempts recorded in March and April 2015, while the 2017–2019 data include all consumers placed on SPP (including suicide attempts and suicidal ideation).
Implementation dose (completeness) of Suicide Prevention Pathway components, before and after implementation.
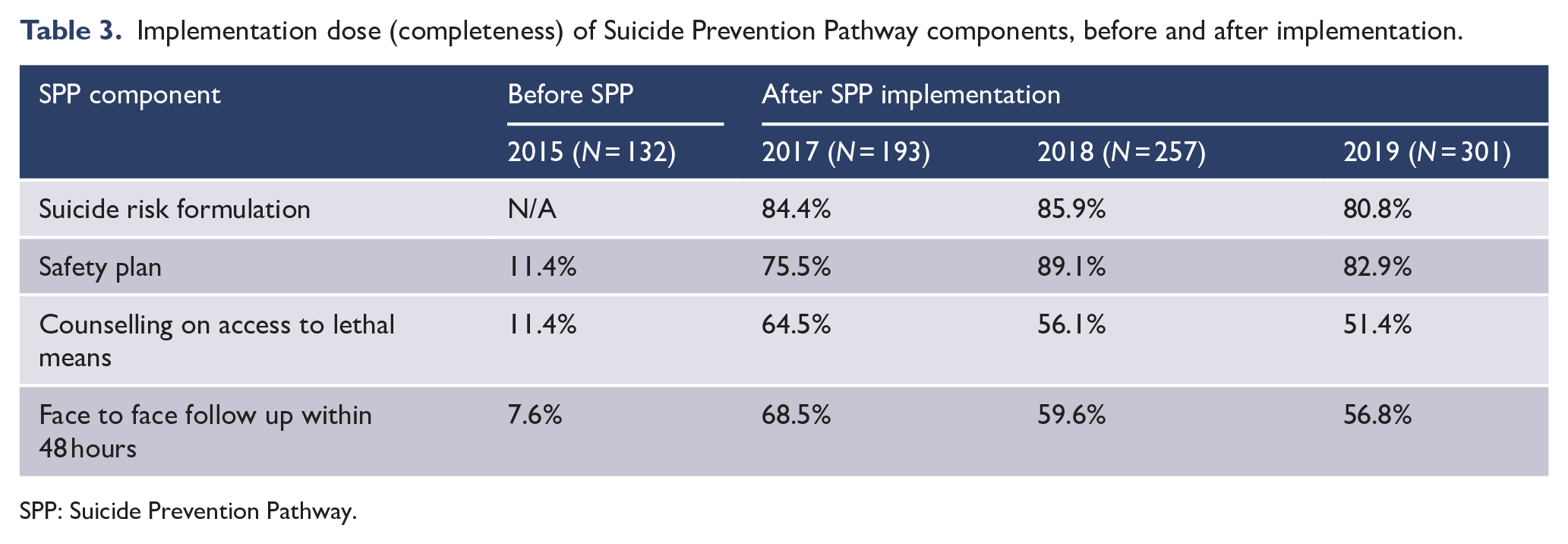
SPP: Suicide Prevention Pathway.
Before implementation of the SPP, most risk assessments categorised a consumer’s risk of suicide as low, medium or high. Within a few months of the introduction of SPP, these were almost completely replaced with the prevention-oriented risk formulation. In 2015, only 11% of cases contained any elements of safety planning (the SPI, as is currently in place as part of SPP, had not been introduced yet, therefore any elements of safety planning noted in consumers’ risk management plans were considered for this analysis).
Table 3 shows a marked improvement in the dose of all SPP components post-implementation, with slight fluctuation in the subsequent years. It is hypothesised that with the rapidly increasing numbers of consumers placed on SPP, it is becoming increasingly challenging for clinicians to complete all components of the pathway. A more detailed evaluation of the fidelity to SPP as well as its links to the long-term outcomes for consumers, is currently being progressed.
Effectiveness of the SPP
Effectiveness of the SPP was evaluated by analysing rates of re-presentations with suicide attempts for consumers who presented to GCMHSS after a suicide attempt between July and December 2017, comparing those placed on SPP and those who were not. The methodology used for this analysis is described in more detail elsewhere (Stapelberg et al., in press). Time-to-event analysis demonstrated a significant reduction in repeated suicide attempts, and a prolonged time to a repeated attempt, for consumers on SPP, reducing their risk of a repeated attempt by approximately 35% (Stapelberg et al., in press).
The evaluation of SPP through analysis of deaths by suicide is more challenging given the relatively small numbers compared to the population who touch the mental health service. To overcome the potential for significant variability across short time frames, we compared the cumulative rates of suicides in the 4 years prior to implementation of SPP (2013–2016) and subsequent 3 years (2017–2019). Suicide cases represent suspected suicide deaths of consumers who were open to the service at the time of death or closed within 30 days prior to death and classified as Severity Assessment Code 1 (SAC1); these data are routinely collected by the Patient Safety Officers, confirmed by the GCHHS Commissioning Authority independently of GCMHSS, and analysed through processes described in a report by GCMHSS (2020b). The rate shown is calculated as a percentage of service episodes (either an open case or referral in which a consumer has been seen face to face on at least one occasion) across that period of time.
Results in Figure 4 demonstrate a reduction of 23.3% in the rate of mental health consumers who died by suicide since the implementation of SPP.
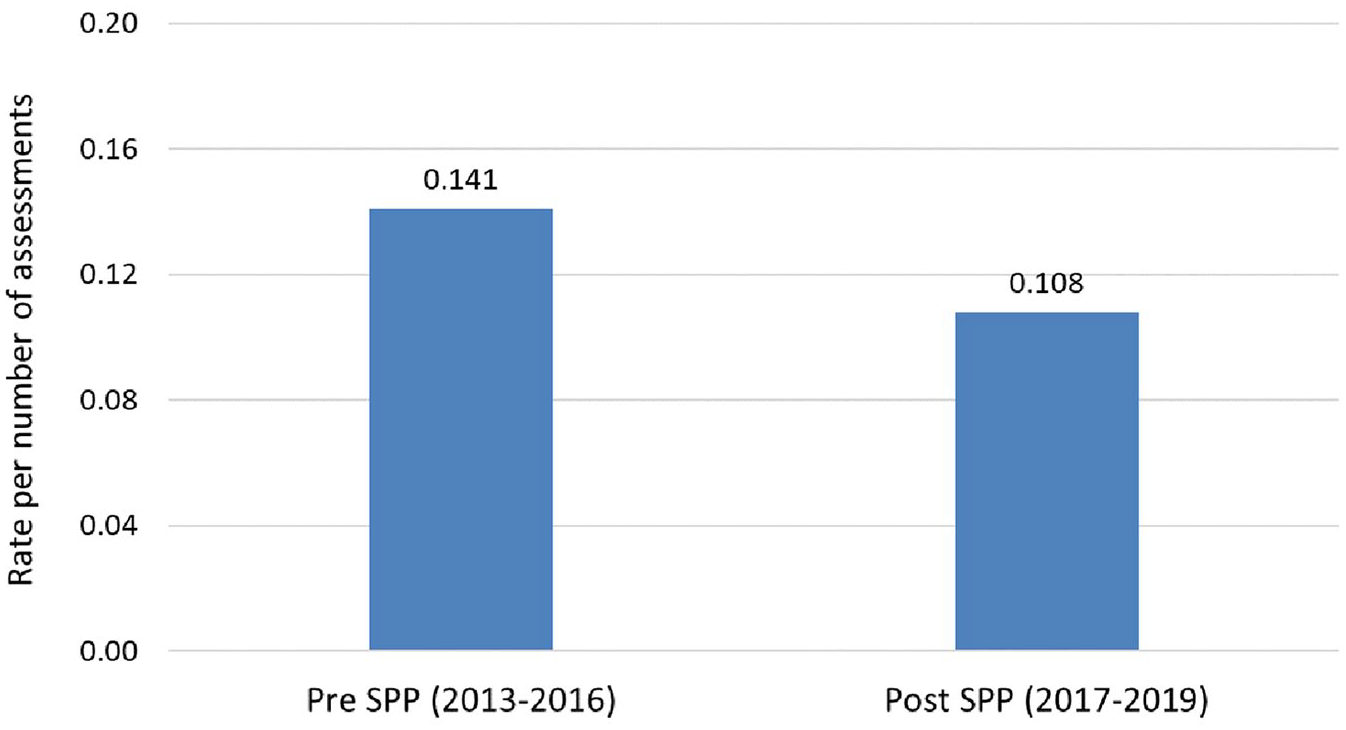
Suicide rates of mental health consumers, pre- and post-implementation of Suicide Prevention Pathway.
Discussion
Sustained change in large health systems is challenging to bring about, and change initiatives have high failure rates (By, 2005). Moran and Brightman (2000) argue that managing change is about managing the impact on the main drivers of work performance, including purpose, identity and mastery, and highlight the need for both a focus on cultural change and robust educational approach to achieve desired change in processes.
The ZSF provides a tool for change management which can enable health services to take on an ambitious goal in suicide prevention, although it is acknowledged that this approach must be implemented alongside broader strategies targeting social determinants of suicide in a community, and an all-of-community approach such as Lifespan (Baker et al., 2018).
Change management occurs through three main elements. First, leadership at every level of the organisation is required to set a clear vision, but also maintain the commitment and focus every day to achieve fidelity to the clinical pathways. Second, staff need to be supported through training to support attitude and skills development, including evidence-based practices, and enable high fidelity to the clinical pathways. Third, a robust continuous quality improvement approach needs to be implemented early and be driven by quality data.
In this paper, we have outlined the steps taken to bring about a significant change in the clinical approach to suicide prevention across a large mental health service. Implementing such a change in the absence of a significant increase in clinical resources has not been without challenges. Below we share a synthesis of key learnings from this experience:
It is imperative to engage in conversations with staff, people with lived experience, the health service Executive and Board prior to embarking on implementation.
Listen to everyone, including those opposed to this approach, reflect on the concerns, and ensure that risks are addressed. Courage is also required to maintain focus as there is always resistance to any change.
The importance of all components of a ‘Systems Approach’ (Leadership, Training and Improvement) is as important as a clinical pathway and should not be viewed as ‘optional extras’. The development of a strategy with specific and measurable actions under each key element was felt to be an important contributor to success.
Adapting to increases in workloads is not possible without an agile and collaborative response from the whole service.
A strong commitment to RJC is central to enabling staff’s trust and commitment to these changes, to allow for effective learning following a loss of consumers to suicide, and facilitate healing for all.
In line with ‘high reliability healthcare’, maintain an awareness of the possibility of failure. This often arises where focus on one aspect will lead to reduction in performance in other areas. For example, a focus on suicide specific interventions and not using diagnosis as a gateway to care should not detract from the need for a robust approach to diagnosis- and evidence-based biological treatments, where appropriate.
Maintain fidelity to developed pathways but encourage innovation across all areas of the service.
Avoid short-term goals for suicide-related outcomes given the relatively rarity of these events and their significant fluctuations from year to year (which could result in either inappropriate optimism or pessimism about early outcomes). Even in a large service such as GCMHSS, we felt a 3-year time frame was required to see any stable trends over time. Similarly, a 3-year rolling average could be used to track progress in the future.
Share learnings and resources with other organisations, and find opportunities to celebrate successes.
Conclusion
The experience of GCMHSS demonstrates that the ZSF, when combined with some limited but well-placed resources for staff training and data collection, can assist in changing organisational culture and embedding of evidence-based practices across the service. This has benefited thousands of consumers across the 3 years of implementation, with results demonstrating improved clinical outcomes through reductions in rates of repeated suicide attempts and deaths by suicide following the implementation of the new pathway of care. Importantly, the feared risk of a worsening blame culture as a result of using the ‘zero terminology’ has not been realised; in fact, there is evidence of improvements in measures of just culture and support for staff following the loss of consumers to suicide, which occurred in the context of active work to implement RJC within the service.
GCMHSS is continuing to evaluate outcomes of the Suicide Prevention Strategy, which, in addition to further stakeholder engagement, is currently informing the development of the next iteration of the strategy. A great deal has been achieved and we continue to be driven by the relentless pursuit of zero suicides through a continuous improvement approach.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.