
Abstract
Objective:
Successive suicide prevention frameworks and action plans in Australia and internationally have called for improvements to mental health services and enhancement of workforce capacity. However, there is debate regarding the priorities for resource allocation and the optimal combination of mental health services to best prevent suicidal behaviour. This study investigates the potential impacts of service capacity improvements on the incidence of suicidal behaviour in the Australian context.
Methods:
A system dynamics model was developed to investigate the optimal combination of (1) secondary (acute) mental health service capacity, (2) non-secondary (non-acute) mental health service capacity and (3) resources to re-engage those lost to services on the incidence of suicidal behaviour over the period 2018–2028 for the Greater Western Sydney (Australia) population catchment. The model captured population and behavioural dynamics and mental health service referral pathways and was validated using population survey and administrative data, evidence syntheses and an expert stakeholder group.
Results:
Findings suggest that 28% of attempted suicide and 29% of suicides could be averted over the forecast period based on a combination of increases in (1) hospital staffing (with training in trauma-informed care), (2) non-secondary health service capacity, (3) expansion of mental health assessment capacity and (4) re-engagement of at least 45% of individuals lost to services. Reduction in the number of available psychiatric beds by 15% had no substantial impact on the incidence of attempted suicide and suicide over the forecast period.
Conclusion:
This study suggests that more than one-quarter of suicides and attempted suicides in the Greater Western Sydney population catchment could potentially be averted with a combination of increases to hospital staffing and non-secondary (non-acute) mental health care. Reductions in tertiary care services (e.g. psychiatric hospital beds) in combination with these increases would not adversely affect subsequent incidence of suicidal behaviour.
Introduction
Suicide remains a significant public health concern in Australia, with preliminary 2016 estimates showing an average of 7.9 deaths each day and a standardised death rate of 11.7 per 100,000 population (Australian Bureau of Statistics [ABS], 2016). Trends in incidence rates have remained largely consistent over the past 10 years with a rate of 10.6 suicide deaths per 100,000 in 2007 (ABS, 2016). Decades of investment and action in suicide prevention in Australia appear to have had limited impact on reductions in suicidal behaviour (Atkinson et al., 2015a; Spittal et al., 2012). Lack of impact from existing initiatives has led to substantial reform in the governance, arrangement and delivery of mental health and suicide prevention services in Australia with an emphasis on person-centred care and regionally led commissioning of primary and specialist services (Hickie, 2017).
Higher rates of suicide in rural compared to urban areas (Qi et al., 2014), despite protective factors such as higher social supports (Tirupati et al., 2010; Yoshimasu et al., 2008), in addition to differential rates of suicide by migrant, indigenous and socioeconomic status (Law et al., 2016; Page et al., 2006; Qi et al., 2012; Too et al., 2018), suggests the potential role of mental health service availability and access as an important modifiable factor in preventing suicide (Korosec Jagodic et al., 2013). Successive suicide prevention frameworks and action plans have called for improvements to the availability, quality and integration of mental health services and enhancement of workforce capacity, which continues under current mental health reforms (Department of Health, 2009, 2012, 2017).
Studies exploring the relationship between the availability of mental health services and suicide show inconsistent results. A number of ecological studies from Europe and the United States suggest that lower suicide rates are associated with increased physicians (Rihmer et al., 1993; Tondo et al., 2006), psychiatrists (Korosec Jagodic et al., 2013; Tondo et al., 2006), staffing levels and training (Kapur et al., 2016) and the availability of outpatient mental health care and multifaceted community-based services (Pirkola et al., 2009). However, several ecological studies from Norway, the United Kingdom and elsewhere have found no association between improved provision of mental health services and standardised suicide mortality ratios (Johannessen et al., 2011; Lewis et al., 1994; Shah et al., 2010), including small-area analyses in Austria of access to general practitioners (GPs) and psychiatrists (Kapusta et al., 2010).
There are different perspectives on the extent to which evidence from international studies are applicable to the Australian context, with uncertainties regarding how local population and behavioural dynamics and regional variation in the determinants of suicide, mental health needs and local resources, capacity, appropriateness and quality of services might affect outcomes. There is also ongoing consideration regarding the allocation of resources between tertiary treatment services and community-based preventive services (Allison and Bastiampillai, 2015). The Australian Government commissioned the National Mental Health Commission to conduct a review of Government-funded programmes and make recommendations for mental health services and suicide prevention reform and to do so assuming there would be no increase in total funding for mental health programmes (Hickie, 2017). One prominent recommendation was the proposal to ‘Reallocate a minimum of $1 billion in Commonwealth acute hospital funding in the forward estimates over the 5 years from 2017–18 into more community-based psychosocial, primary and community health services’ (National Mental Health Commission [NMHC], 2014: 10), a recommendation that has not been implemented to date.
One approach to better understanding the implications over time of the strategic re-allocation of resources on suicidal behaviour in a given population is to employ dynamic simulation models, co-designed and developed by key stakeholders (Atkinson et al., 2015b, 2017; Loyo et al., 2013; Rouwette et al., 2002). Dynamic simulation modelling provides a method for bringing together a variety of sources of evidence such as research, expert and local knowledge, practice experience and existing data to map, quantify and simulate complex problems, including mental health service pathways and suicide prevention activity (Atkinson et al., 2015a; Page et al., 2017, 2018). The resulting model is an interactive ‘what-if’ tool that allows decision makers to test the likely population-level impacts on suicide of alternative intervention and service planning strategies before they are implemented in the real world.
The extent to which investments in improving, or re-distributing, mental health service capacity will contribute to reductions in suicidal behaviour is unknown, as is the relative contribution of investing in tertiary versus non-tertiary mental health services. Accordingly, a dynamic simulation model of the Greater Western Sydney (Australia) population catchment (Page et al., 2018) was used to investigate the optimal combination of service capacity improvements that would potentially deliver the largest reductions in suicide and attempted suicide of the period 2018–2030.
Methods
Model context, design and structure
A system dynamics model was co-developed with Western Sydney Primary Health Network (PHN) in collaboration with local stakeholders. Western Sydney is one of the fastest growing urban populations in Australia (N ~971,000 in 2016) with a range of ethnic and non-Australian-born backgrounds and varying geography (Western Sydney Primary Health Network, 2016). It has been estimated that 20% of the population have experienced a mental health issue in the last 12 months, of whom almost 15% were classified as severe (Western Sydney Primary Health Network, 2016). There is also an increasing trend in hospitalisations for mental disorder placing pressure on tertiary services in the population catchment (Western Sydney Primary Health Network, 2016).
The model structure, parameterisation and the participatory approaches used are detailed elsewhere (Page et al., 2018). Briefly, for the Western Sydney PHN population catchment, the model captures (a) the pathway from vulnerability to psychological distress and to mental disorder; (b) mental health service pathways, including assessment of care needs and delivery of low intensity services, moderate intensity services (also known as non-secondary services) and high intensity services (also known as secondary or hospital services) based on changing individual needs (a ‘stepped care’ approach; Cross and Hickie, 2017); (c) pathways to suicidal behaviour (attempted suicide and suicide) either with or without contact with mental health services and (d) mental health recovery pathways with and without contact with mental health services. The model has an open population, with births and migration contributing to the population and deaths (from causes other than suicide) subtracting from the population. The computational model was developed using Stella Architect® software (www.iseesystems.com/).
Model inputs and outcome indicators
The structure and parameterisation of the model drew on a range of data sources including population survey data, systematic reviews (and meta-analyses), administrative data and expert knowledge of the multidisciplinary stakeholders. Demographic data, psychological distress data, mental health hospitalisations, suicide attempts (for which there was a hospital admission) and completed suicides for Western Sydney were sourced from NSW Health administrative datasets (Centre for Epidemiology and Evidence, 2017). Prevalence of mental disorder and service capacity and use data were sourced from a WentWest – Western Sydney PHN needs assessment conducted in 2016 (Western Sydney Primary Health Network, 2016) and data from the Medicare Benefits Schedule (MBS) relating to mental health services in the WentWest – Western Sydney PHN population catchment. These data were used for model initialisation, calibration and validation purposes. In instances where data were not available, estimates were reached by consensus and the ability to test the impact of alternative values for those parameters provided in the model interface. Key assumptions of the model are provided in Supplementary File (Box 1), and all model parameters are published in Page et al. (2018).
Estimates of the effects of selected interventions, and the specific mechanism of action in the model, were based on evidence from the literature and informed by stakeholder feedback for local application. The model forecasts the primary outcome indicators (suicide and hospitalised suicide attempts) to 2030. The final model provides a ‘what-if’ tool to test the likely impacts of different combinations of service planning options to maximise reductions in attempted suicide and suicide in Western Sydney over a 10-year period (Page et al., 2018).
Simulation experiments
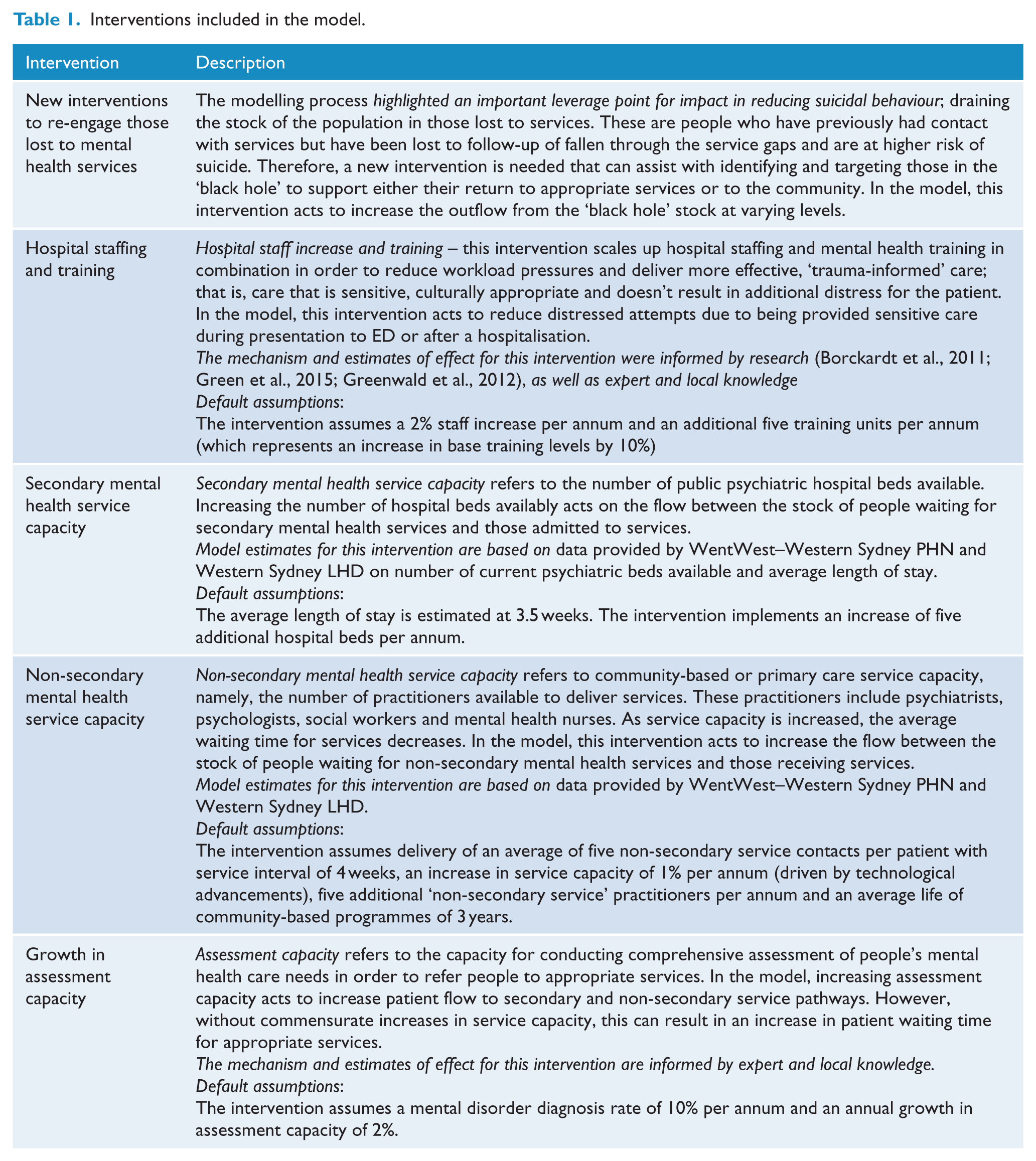
The baseline (‘business as usual’) scenario forecasts suicide and attempted suicide across a 10-year period from mid-2018 to mid-2028 and assumed no changes to existing mental health service capacity across Greater Western Sydney. A series of scenarios were specified to investigate a number of potential changes (or re-distribution) of mental health services on suicidal behaviour. These included scenarios that (a) increased existing resources and staffing capacity for secondary mental health services; (b) increased existing resources, staffing and assessment for non-secondary mental health services; (c) retained existing secondary and non-secondary mental health services, but increased resources to re-engage those lost to services and (d) relocated resources from secondary to non-secondary mental health services to determine the scenario that would deliver the greatest impact on suicidal behaviour. Specifically, the following scenarios were considered: (Table 1 provides intervention definitions and their default parameter values):
Scenario 1. Increases in hospital staffing and training.
Scenario 2. Increases in hospital staffing and training, plus increases in psychiatric hospital beds.
Scenario 3. Increases in non-secondary service capacity through the provision of five additional practitioners for the population catchment per annum.
Scenario 4. Increases in hospital staffing and training, plus increases in non-secondary service capacity through the provision of five additional practitioners for the population catchment per annum.
Scenario 5. Increases in mental health assessment capacity.
Scenario 6. Increases in hospital staffing and training, plus increasing non-secondary service capacity through the provision of five additional practitioners for the population catchment per annum, plus increases in mental health assessment capacity.
Scenario 7. Increased re-engagement of those lost to services (during the simulated period) by 15%.
Scenario 8. Increased re-engagement of those lost to services (during the simulated period) by 45%.
Scenario 9. Increases in hospital staffing and training, plus increases in non-secondary service capacity through the provision of five additional practitioners for the population catchment per annum, plus increases in mental health assessment capacity, plus increased re-engagement of those lost to services by 45%.
Scenario 10. Decreases in hospital beds by 15%, plus increases in non-secondary service capacity through the provision of 10 additional practitioners for the population catchment per annum.
Interventions included in the model.
Sensitivity analyses
Due to the large number of parameters in the model, exhaustive sensitivity analysis for each combination of variables is not feasible due to combinatorial explosion. It is standard practice in system dynamics modelling to prioritise parameters that are most uncertain and likely to have the greatest impact on key outcomes of interest. Therefore, in the current model, sensitivity analysis was conducted by introducing variation in the values of two key parameters (simultaneously): the proportion of the population that become vulnerable each year (default value 2%; variation between 1% and 5%; step of 0.5%) and the initial value of non-secondary mental health service staff (default value 100 practitioners; variation between 90 and 110 practitioners; step of two practitioners). Baseline and scenarios were each run 100 times. Comparison of simulation results between baseline and intervention scenarios was expressed as the mean number of cases averted and as the absolute percent difference in the mean of two independent samples for the same population and presented with the associated margin of error. Description of the output data processing method is presented in Figure 1 in Supplementary File.
Results
The combination of increases in hospital staffing and training, non-secondary service capacity, mental health assessment capacity and the re-engagement of 45% of those previously lost to services was forecast to avert the largest number of attempted suicides (28.2% ± 0.05%) and suicide cases (28.7% ± 0.1%) compared to the baseline scenario (Table 2, Figure 1). This equates to 3927 suicide attempts and 489 suicide cases averted over the 10-year forecast period. Increases to hospital staffing and training to deliver trauma-informed care was forecast to contribute to a 7.2% ± 0.2% reduction in attempted suicides (1004 attempts averted) and a 7.3% ± 0.6% reduction in suicide cases (124 cases averted), with no additional benefit observed with increases in the number of psychiatric hospital beds. Increases in mental health assessment capacity alone had no significant impact on the forecast number of attempted suicides and suicide. However, combining increases in assessment capacity with increases in hospital staffing and training and non-secondary service capacity forecast a 12.2% ± 0.1% reduction in attempted suicides and 12.5% ± 0.4% reduction in suicide cases; enhancing the effect of these interventions alone (which are forecast to deliver a 10.7% ± 0.1% reduction in attempted suicides and a 10.9% ± 0.4% reduction in suicide cases).
Summary of estimated reductions in suicide and attempted suicide in Western Sydney for selected scenarios (10-year forecast period: 2018–2028).
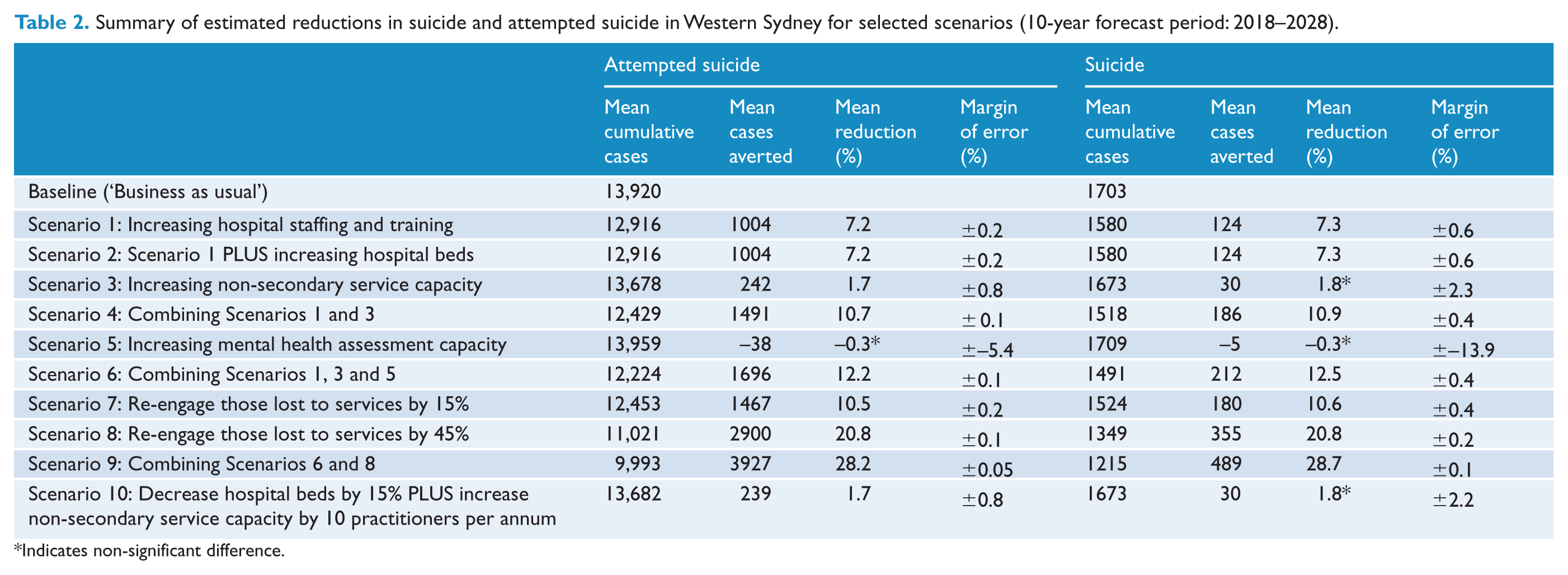
Indicates non-significant difference.
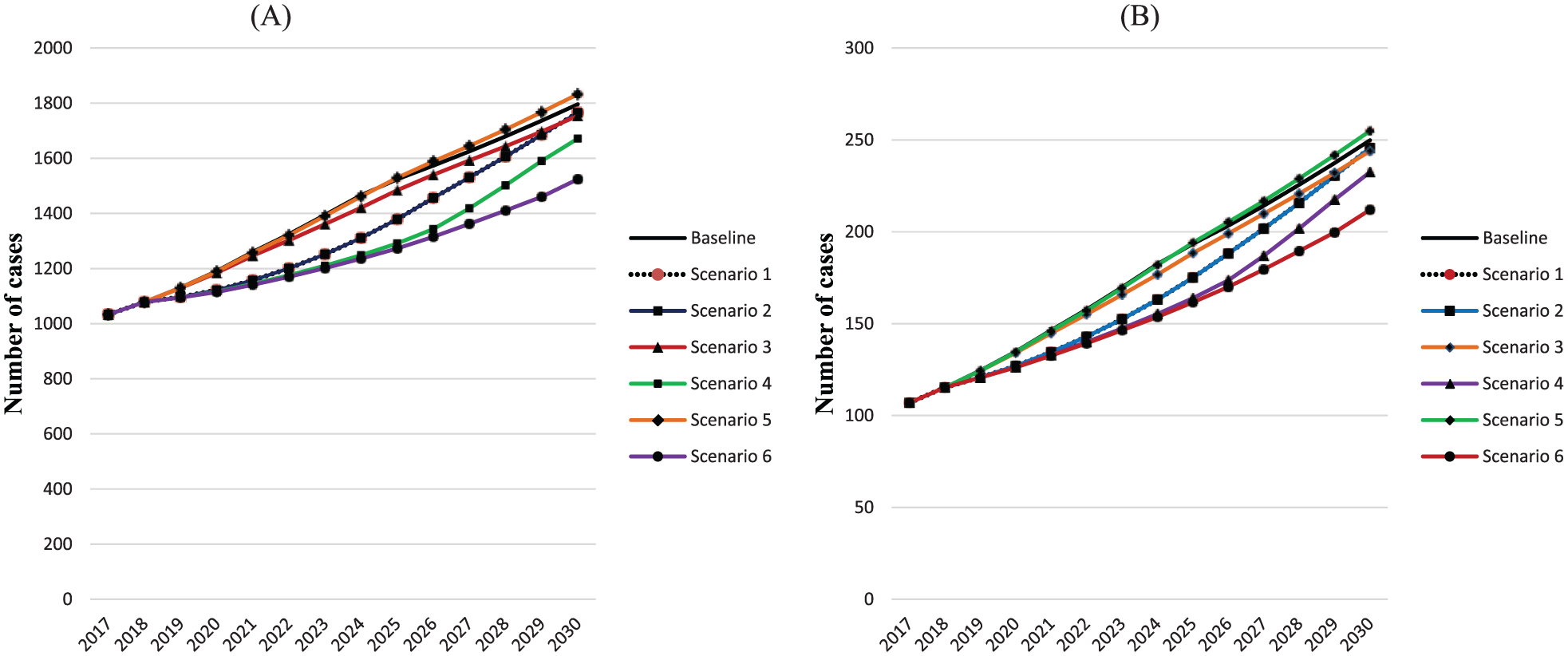
Effect over time of modelled service capacity scenarios 1 to 6 on (A) attempted suicide and (B) suicide cases.
Re-engagement of those lost to mental health services was forecast to deliver substantial reductions in suicidal behaviour over the 10-year period. Re-engagement of 15% and 45% of those lost to services suggested that ~10.5% of suicides (180 cases) and 20.8% attempted suicides (355 cases) could be averted over the follow-up period. However, as shown in Figure 2, the initial effect compared to the baseline is reduced over time unless there were contemporaneous increases in mental health service capacity. Finally, a 15% reduction in the number of available psychiatric beds had no significant impact on forecast reductions in suicide or attempted suicide, if supported by increases in non-secondary mental health service capacity (i.e. 10 additional practitioners per annum) over the 10-year period (Table 1).
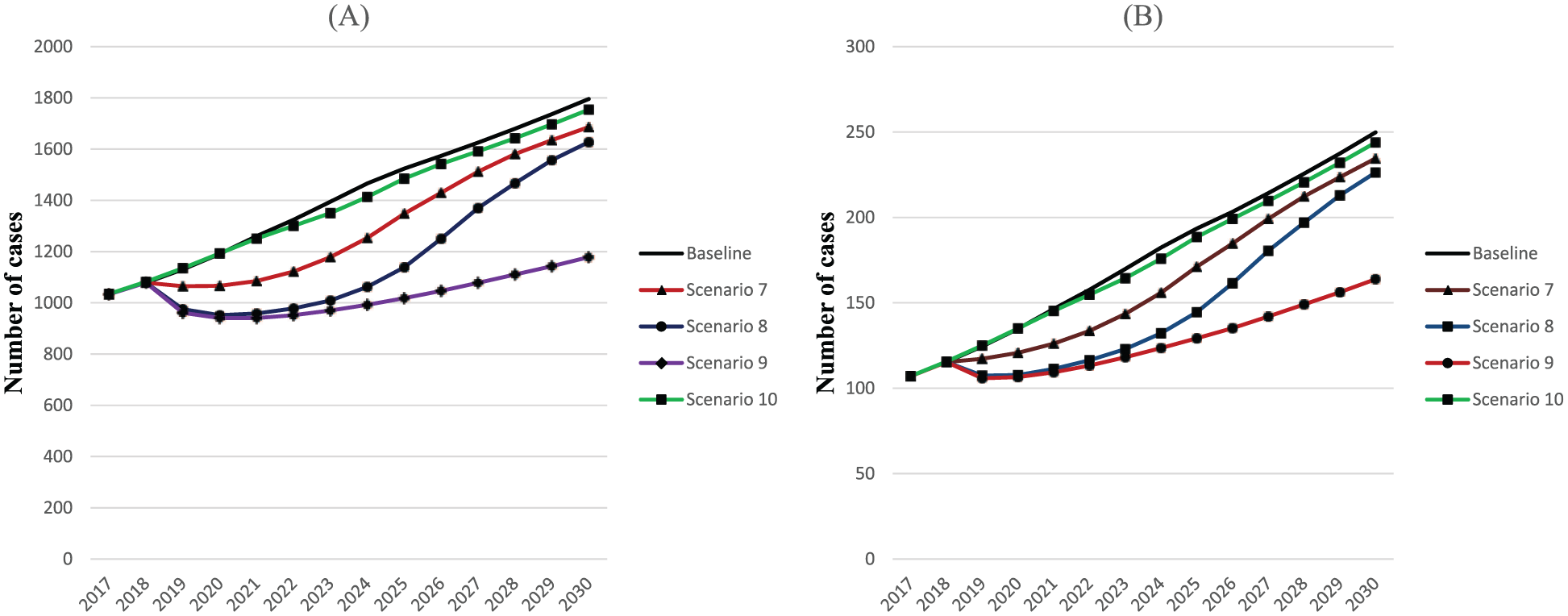
Effect over time of modelled service capacity scenarios 7–10 on (A) attempted suicide and (B) suicide cases.
Discussion
Current national and international plans for reducing suicide and attempted suicide recommend significant enhancement of health services (Department of Health, 2009, 2012, 2017; World Health Organization (WHO, 2014). However, it remains contentious as to which aspects of those services are most likely to deliver benefit in real-world settings and the extent to which such enhancements can be implemented effectively, given workforce, financial and infrastructure constraints. Findings from this study suggest that the number of suicides and attempted suicide could be reduced by focussing on a combination of increases in hospital staffing and training and non-secondary health service capacity, expansion of mental health assessment capacity and strategies to re-engage those lost to mental health services.
The use of dynamic modelling techniques such as system dynamics can address the challenges associated with using traditional analytic methodologies to evaluate impacts of multiple service changes implemented simultaneously (Kapur et al., 2016). It also permits more contentious scenarios to be compared in silico to advance debate, promote learning and identify priority interventions, before implementing solutions in the real world. For example, while there is frequent public commentary (Allison and Bastiampillai, 2015; Bastiampillai et al., 2016) advocating for more hospital-based and specialist mental health beds, the findings in this study suggest there is no clear benefit for these resource-intensive initiatives in the Greater Western Sydney context, compared to the potential gains obtained from increases in trauma-informed care trained staff and other more targeted community-based strategies.
Service developments that engage directly with those at risk, and do so in non-hospital-based settings, are more likely to deliver substantive benefits. In addition, such initiatives are highly feasible as they rely largely on existing workforce development and deployment rather than building or servicing of new physical infrastructure. No adverse impacts on suicidal behaviour were apparent following a reduction of hospital beds by 15% if also accompanied by increases in investment in community-based mental health service capacity. These findings provide support for the recommendations of the 2014 National Mental Health Commission Review of Services, which emphasised the need for financial support for community-based primary and secondary care–based service initiatives. However, it is important to note that given the interacting population, behavioural and service dynamics of a region, there may be a threshold below which a reduction in psychiatric beds would result in increases in suicide (Bastiampillai et al., 2016). This is the subject of further analysis using dynamic modelling for the Greater Western Sydney population catchment.
With adequate service capacity in place, re-engaging those lost to services was shown to be an effective strategy for reducing suicides over the forecast period. While no specific interventions were considered by PHN stakeholders for this intervention point in the model, there are a range of potential strategies that could be considered, including the use of new digital technologies, to ensure that services remain more effectively connected with individuals who have previously made contact with mental health services (Iorfino et al., 2017). Further development of enhanced primary care models (e.g. health-care homes, headspace-style services, GP-liaison care) may be additional interventions of relevance to deliver more effective care for those at high risk but who do not require ongoing care from more specialised services.
There are a number of limitations for consideration when interpreting the findings from this study. First, the model presented is a system dynamics model—an approach that models populations in aggregate. The model accounts for behavioural and population dynamics that impact mental health service capacity, suicidal behaviour and suicide outcomes. Aggregate systems models cannot consider the complex mechanisms and trajectories that affect the behaviours and outcomes for individuals. However, system dynamics models offer significant value for strategic planning in timeframes that are more congruent with the timelines and priorities of service providers and policy makers. In addition, they are suited to analysis and improved understanding of the dynamics of complex problems, the non-additive effects of intervention combinations, the identification of leverage points where interventions can deliver greater than anticipated returns and strategic directions for achieving population-level reductions in suicidal behaviour.
Second, there is potential measurement bias in the range of secondary data used to parameterise the model. Where possible, routinely collected local health service information was obtained to estimate population-based estimates of psychological distress, mental health service contacts (via MBS data), workforce information (in terms of numbers of GPs, psychologists, psychiatrists and allied health professionals) and primary, secondary and tertiary service capacity (in terms of numbers of beds, available appointments and waiting times) from PHN and Local Health District (LHD) datasets, hospital-based suicide attempts (from LHD data) and suicide data (from the ABS). In addition, hospital admissions for suicide attempts capture only those cases serious enough to warrant medical intervention and will under-enumerate the total population burden of attempted suicide in the Western Sydney PHN population catchment. The model acknowledges these potential sources of measurement bias, and a number of commonly used strategies were employed to address them, including the triangulation of multiple data sources; calibration to refine parameter estimates and the engagement of stakeholders with detailed knowledge of the limitations and likely direction and size of potential measurement biases in key data sources (Page et al., 2018).
Conclusion
Findings from this study suggest that over a quarter of suicides and attempted suicides in the Greater Western Sydney population catchment could potentially be averted with a combination of increases to hospital staffing and non-secondary (non-acute) mental health care and that reductions in tertiary care services (e.g. psychiatric hospital beds) in combination with these increases would not adversely affect subsequent incidence of suicidal behaviour. This study also demonstrates the utility of dynamic simulation models in quantifying the impact of improvements to non-hospital based mental health service capacity on suicide prevention, in identifying synergistic effects in intervention combinations and in identifying leverage points in the mental health service system. This information can be used by the PHN to guide decisions on commissioning (and co-commissioning arrangements) of suicide prevention activity, as well as informing ongoing systematic evaluation of regionally based service suicide prevention initiatives. Useful next steps could include integration of costs into the model to facilitate health economic analyses and an exploration of barriers to implementation of selected interventions.
Supplemental Material
Supplementary_files – Supplemental material for The impact of strengthening mental health services to prevent suicidal behaviour
Supplemental material, Supplementary_files for The impact of strengthening mental health services to prevent suicidal behaviour by Jo-An Atkinson, Andrew Page, Mark Heffernan, Geoff McDonnell, Ante Prodan, Bill Campos, Graham Meadows and Ian B Hickie in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
This model was developed by Decision Analytics (Sax Institute) and the Translational Health Research Institute (Western Sydney University) in partnership with WentWest – Western Sydney Primary Health Network and the Brain and Mind Centre, University of Sydney. Importantly, this work was made possible by the generous contributions of local expert knowledge and data by representatives of the following stakeholder agencies: Western Sydney Local Health District; Hills Shire, Parramatta, Blacktown and Cumberland City councils; the Western Sydney Regional Organisation of Councils; NSW Police Force; Headspace; WESTIR Ltd. and consumer representatives.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a Western Sydney University Partnership Grant and in-kind contributions from WentWest – Western Sydney (in part with the Commonwealth Department of Health) and Western Sydney Local Health District.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.