
Abstract
Objective:
Functional remission represents an intermediate functional milestone toward recovery. Differential relationships of negative symptom sub-domains with functional remission in first-episode psychosis are understudied. We aimed to examine rate and predictors of functional remission in people with first-episode psychosis in the context of a 3-year follow-up of a randomized controlled trial comparing 1-year extension of early intervention (i.e. 3-year early intervention) with step-down psychiatric care (i.e. 2-year early intervention).
Method:
A total of 160 participants were recruited upon completion of a 2-year specialized early intervention program for first-episode psychosis in Hong Kong and underwent a 1-year randomized controlled trial comparing 1-year extended early intervention with step-down care. Participants were followed up and reassessed 3 years after inclusion to the trial (i.e. 3-year follow-up). Functional remission was operationalized as simultaneous fulfillment of attaining adequate functioning (measured by Social and Occupational Functioning Scale and Role Functioning Scale) at 3-year follow-up and sustained employment in the last 6 months of 3-year study period. Negative symptom measure was delineated into amotivation (i.e. motivational impairment) and diminished expression (i.e. reduced affect and speech output). Data analysis was based on 143 participants who completed follow-up functional assessments.
Results:
A total of 31 (21.7%) participants achieved functional remission status at 3-year follow-up. Multivariate regression analysis showed that lower levels of amotivation (p = 0.010) and better functioning at study intake (p = 0.004) independently predicted functional remission (Final model: Nagelkerke R2 = 0.40, χ2 = 42.9, p < 0.001). Extended early intervention, duration of untreated psychosis and diminished expression did not predict functional remission.
Conclusion:
Only approximately one-fifths of early psychosis patients were found to achieve functional remission. Functional impairment remains an unmet treatment need in the early stage of psychotic illness. Our results further suggest that amotivation may represent a critical therapeutic target for functional remission attainment in early psychosis.
Keywords
Introduction
Psychotic disorders are associated with pronounced functional impairment and incur huge societal costs (Jin and Mosweu, 2017). Although evidence has shown that specialized early intervention (EI) service is superior to standard care in improving outcome in first-episode psychosis (FEP; Nordentoft et al., 2014), literature has consistently found that a significant proportion of people with FEP experience persistent functional disability even in the presence of symptom remission (Chang et al., 2012; Verma et al., 2012; Wunderink et al., 2009). Thus, functional impairment represents an unmet therapeutic need in the early stage of psychotic illness.
There is substantial evidence indicating negative symptoms as a major determinant of functional outcome in psychotic disorders (Milev et al., 2005). It is also acknowledged that negative symptom construct is multi-dimensional in nature and comprises two distinct sub-domains, namely, motivational impairment (amotivation) and diminished expression (DE, that is, reduced affect and speech output; Messinger et al., 2011). Recent studies have further demonstrated that, among these two symptom sub-domains, amotivation is more prevalent and persistent over time (Fervaha et al., 2015; Norman et al., 2015), and a much stronger predictor of functioning than DE (Chang et al., 2016a, 2017a; Fervaha et al., 2015; Strauss et al., 2013). Of note, most previous research studying functional outcome prediction examined negative symptoms as a single composite measure without delineation into two symptom sub-domains. Among those few studies which investigated the differential relationships of amotivation and DE with functional impairment, the majority focused on patients with chronic schizophrenia. Few studies have been conducted in early psychosis in this respect, and most, if not all (Evensen et al., 2012a), either adopted cross-sectional design (Chang et al., 2017a; Faerden et al., 2009; Fervaha et al., 2013a) or had follow-up duration of 1 year or less (Chang et al., 2016a; Faerden et al., 2010, 2013; Fervaha et al., 2015a).
Recently, there has been a growing interest in studying rate and predictors of functional remission (FR) and recovery in FEP. Until now, although consensus definition for FR and recovery has yet to be established, it is recognized that functional outcome represents a multifaceted construct consisting of various relatively separable domains that are necessary for adequate everyday functioning in the community (Harvey and Bellack, 2009). Compared to recovery, which generally incorporates both symptom and functional dimensions measured over a sustained period of time (mostly 2 years) in its operational criteria (Jaaskelainen et al., 2013), FR focuses on attainment of short-term adequate functional levels. In this regard, FR can be conceptualized as an intermediate functional milestone toward recovery. In fact, recent studies have revealed that achievement of FR status in the early illness course was associated with better functioning at long-term follow-up (Alvarez-Jimenez et al., 2012). This thus underscores a potential critical role of early FR attainment in reducing the risk of developing enduring functional disability in FEP. Nonetheless, despite its significant clinical implication, FR has been understudied in the early phase of psychotic illness, with discrepant findings being observed on the prevalence and predictors of FR in FEP populations (Alvarez-Jimenez et al., 2012; Chang et al., 2012, 2016b; Flyckt et al., 2006; Henry et al., 2010; Lambert et al., 2008; Ventura et al., 2011; Verma et al., 2012). Thus far, there is no published report examining prospectively the differential relationships of negative symptom sub-domains with FR achievement in FEP samples.
Hong Kong (HK) is among the few cities in Asia to implement a territory-wide EI service for psychosis. The program, namely, Early Assessment Service for Young People with Psychosis (EASY), provided 2-year specialized EI for young people presenting with FEP in HK (Chung and Chen, 2013). We have conducted a 3-year follow-up of a randomized controlled trial (RCT; i.e. 1-year RCT + 2-year post-RCT follow-up) which compared a 1-year extension of EI (Extended EI; i.e. 3-year EI) with step-down psychiatric care (SC; i.e. 2-year EI) in a representative cohort of Chinese patients who had just completed 2-year treatment in EASY program for FEP (Figure 1; Chang et al., 2015, 2017b). (Please refer to section ‘Methods’ for detailed description of two treatment conditions.) This is the first RCT follow-up study examining sustainability of therapeutic benefits of EI service for FEP on clinical and functional outcomes with its treatment period extended beyond 2 years. Results of this study, however, showed that superior effects achieved by Extended EI could not be maintained after termination of the specialized service (Chang et al., 2017b) and are thus congruent with two previous post-RCT follow-up studies (namely, the OPUS trial with 2-year EI and the Lambeth Early Onset [LEO] study with 18-month EI) which demonstrated that positive effects of EI over standard care were not sustainable after service withdrawal (Bertelsen et al., 2008; Gafoor et al., 2010).
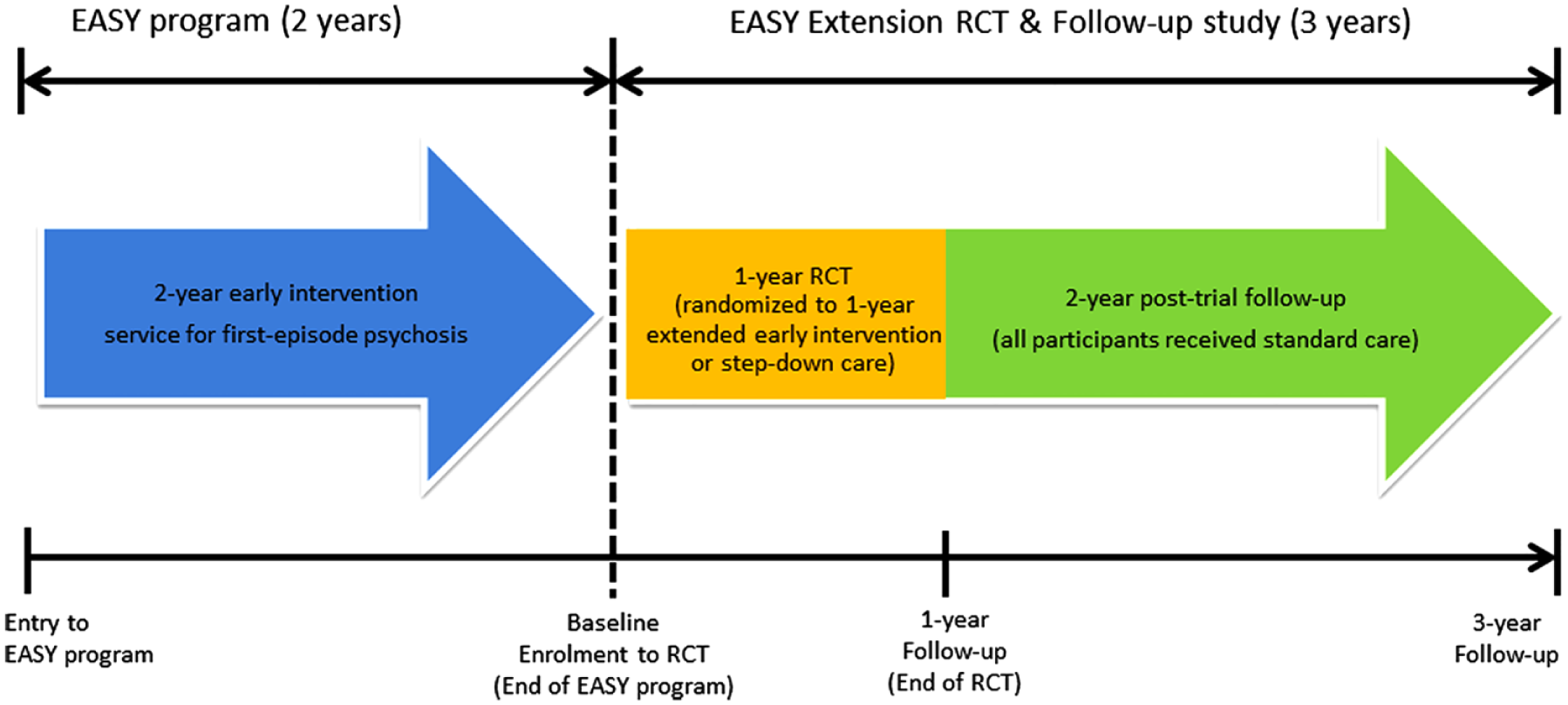
Flow diagram of EASY Extension trial and follow-up study.
In the current report, we sought to examine the rate and predictors of FR in people with FEP in the context of this 3-year RCT follow-up study. To comprehensively capture the multifaceted nature of functioning, FR was operationalized on the basis of standardized functional assessments encompassing independent living, social relationships and instrumental role activity. Negative symptom measure was subdivided into amotivation and DE components to enable clarification of potential unique contributions of these negative symptom sub-domains to prospective FR status.
Methods
Participants and setting
Details of the study methodology have been reported elsewhere (Chang et al., 2015, 2017b). Briefly, this was a 3-year follow-up of a single-blind RCT comparing a 1-year extension of specialized EI (a 3-year EI service) with a step-down care (a 2-year EI service) in patients who were recruited upon completion of 2-year EASY program for FEP (Figure 1). Since 2001, this publicly funded specialized program has been providing early assessment and phase-specific intervention for all individuals aged 15–25 years experiencing their FEP in HK (Chung and Chen, 2013). The service consisted of five clinical teams, each covering a geographically defined catchment area and comprising two psychiatrists, three case managers and one social worker. The service adopts phase-specific case-management approach in which each individual with FEP is assigned with a case manager who provides protocol-based psychosocial interventions. People with FEP were assertively followed up for a period of 2 years, after which they were managed by step-down clinic in the third year of treatment without provision of case-management (Chung and Chen, 2013). They were then transferred to generic psychiatric service for continuous care.
A total of 160 participants with a Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) diagnosis of psychotic disorder were recruited from EASY program, randomly allocated to Extended EI (n = 82) or SC (n = 78), and underwent 1-year clinical trial (Chang et al., 2015). Exclusion criteria were intellectual disability, substance-induced psychosis or psychotic disorder due to general medical condition. Participants in both treatment conditions were managed by psychiatrists from their respective EASY clinical teams. In Extended EI condition, specialized EI was continued in the form of an additional year of case-management. A trained case manager took over cases (a case-load of 82 participants, comparable to the EASY program) from EASY program and was responsible for providing care and coordinating treatment with clinicians, allied health professionals and community centers. Case-management provided closely aligned with treatment protocols (So, 2013) adopted by EASY program, focusing specifically on functional enhancement by assisting participants to re-establish supportive social networks, to resume leisure pursuits and to return to work. Continuous supportive care, psychoeducation and stress management were also delivered to participants’ caregivers by case manager. Participants allocated to SC received outpatient medical follow-up with limited community support which focused mainly on crisis intervention, and no case-management was provided. Two treatment groups did not differ from each other regarding the intensity of medical follow-up by psychiatrists, prescription of antipsychotic medications, and availability of various psychosocial interventions and community-based services (Chang et al., 2015). Participants were followed up and re-interviewed 2 and 3 years after inclusion in the trial (Chang et al., 2017b).
In this report, we focused on investigating predictors of FR in 143 participants of the initial cohort who had completed assessments at 3-year follow-up. The study was approved by the local institutional review boards. All participants provided written informed consent. For those aged under 18 years, consent was also obtained from a parent or guardian.
Assessments
Diagnosis was ascertained using all available information encompassing the entire follow-up period including Chinese-bilingual Structured Clinical Interview for DSM-IV (CB-SCID; So et al., 2003) (conducted at study intake [baseline], 1- and 3-year follow-up), informant histories and medical records. Premorbid personality and adjustment were evaluated, on the basis of information obtained via interviews with participants and their relatives, using an assessment of Premorbid Schizoid-Schizotypal Traits (PSST; Foerster et al., 1991) and Premorbid Adjustment Scale (PAS; Cannon-Spoor et al., 1982), respectively. Interview for the Retrospective Assessment of the Onset of Schizophrenia (IRAOS; Hafner et al., 1992) was employed to determine duration of untreated psychosis (DUP) and age at onset of psychosis. Psychopathology was assessed at baseline, 1-, 2- and 3-year follow-up using Positive and Negative Syndrome Scale (PANSS; Kay et al., 1987) and Calgary Depression Scale (CDS; Addington et al., 1990). Following the method applied in previous research (Fervaha et al., 2014), measurement of negative symptoms was divided into two distinct sub-domains, that is, amotivation and DE using PANSS ratings: amotivation score was derived by summing the PANSS items N2 (emotional withdrawal), N4 (passive social withdrawal) and G16 (active social avoidance), while DE score was the sum of items N1 (blunted affect), N3 (poor rapport), N6 (lack of spontaneity) and G7 (motor retardation). Medication Adherence Rating Scale (MARS; Thompson et al., 2000) was applied to assess treatment adherence. Psychosocial functioning was measured by Social and Occupational Functioning Assessment Scale (SOFAS; Goldman et al., 1992) and Role Functioning Scale (RFS; Goodman et al., 1993). SOFAS provided global functioning estimate of an individual participant, while RFS, which comprised four subscales, was used to assess functional levels of various domains including independent living and self-care, work productivity, immediate and extended social networks. Occupational status was also assessed. Functional evaluation was conducted at baseline, at 6 months, and 1, 2 and 3 years after study entry.
Operational definition of FR
Operational definition of FR at 3-year follow-up was adapted from a previous report based on ratings on SOFAS and RFS, and employment status (Chang et al., 2016b). Participants were categorized as functionally remitted if they simultaneously fulfilled the following criteria: (1) attained SOFAS score >60 (achieving functional level of ‘generally functioning well though with some difficulty in social or occupational functioning’ or above), RFS independent living and immediate social network subscale scores >5 (achieving ‘adequate’ functional level or above), and RFS work productivity (at least ‘moderately functional’ in independent employment, at home or in school) and extended social network (at least ‘moderately effective and independent’ in community interactions) subscale scores >4 at 3-year follow-up; and (2) was engaged in sustained competitive employment (full-time or part-time work or full-time study) in the last 6 months of 3-year follow-up.
Statistical analysis
The primary analysis focused on identifying baseline predictors of FR status at 3-year follow-up. A series of univariate logistic regression analyses were conducted with functional status (i.e. remitted vs non-remitted) as dependent variable, and demographics, premorbid functioning, clinical variables at intake encompassing onset characteristics, diagnosis and symptom severity, baseline functional levels, allocated treatment condition (i.e. Extended EI vs SC) and other treatment-related variables including the use of second-generation antipsychotics (SGAs) and medication adherence as candidate predictors. Then, those variables that showed a p-value <0.10 in preceding analyses were entered into a multivariate regression model to determine which factors independently predicted FR based on Wald statistics. The level of statistical significance other than correlation analyses was set at p < 0.05. All statistical analyses were carried out using the IBM Statistical Package for the Social Sciences (SPSS) version 24.
Results
Characteristics of the sample
Of the initial cohort (n = 160), 143 participants (Extended EI: n = 76; SC: n = 67) completed 3-year follow-up assessment and were included in the current investigation. Among the 17 dropouts (10.6%), 2 committed suicide (Extended EI: n = 1, SC: n = 1), 2 died by natural cause (SC: n = 2), 1 withdrew consent (Extended EI: n = 1) and 8 defaulted follow-up (Extended EI: n = 2; SC: n = 6). Attrition analysis revealed no significant difference between completers and non-completers in sociodemographic characteristics, allocated treatment condition or baseline clinical, functional and treatment variables, with the exception of RFS immediate social network score (completers had higher scores than non-completers, p = 0.03). Of 143 participants, 52.4% were male. The mean age of the sample at study intake was 22.9 years (SD = 3.2) and the median DUP was 13 weeks (mean = 36.0, SD = 52.5). At 3-year follow-up, 31 patients (21.7%) achieved FR.
Inter-rater reliability
Intra-class correlation coefficients (ICCs) for PANSS general psychopathology, positive and negative symptom subscales, and CDS total score were 0.92, 0.95, 0.79 and 0.96, respectively, indicating good inter-rater reliability. Satisfactory level of concordance was also observed in functional measures, with ICCs for SOFAS and RFS total scores being 0.91 and 0.86, respectively.
Predictors of FR
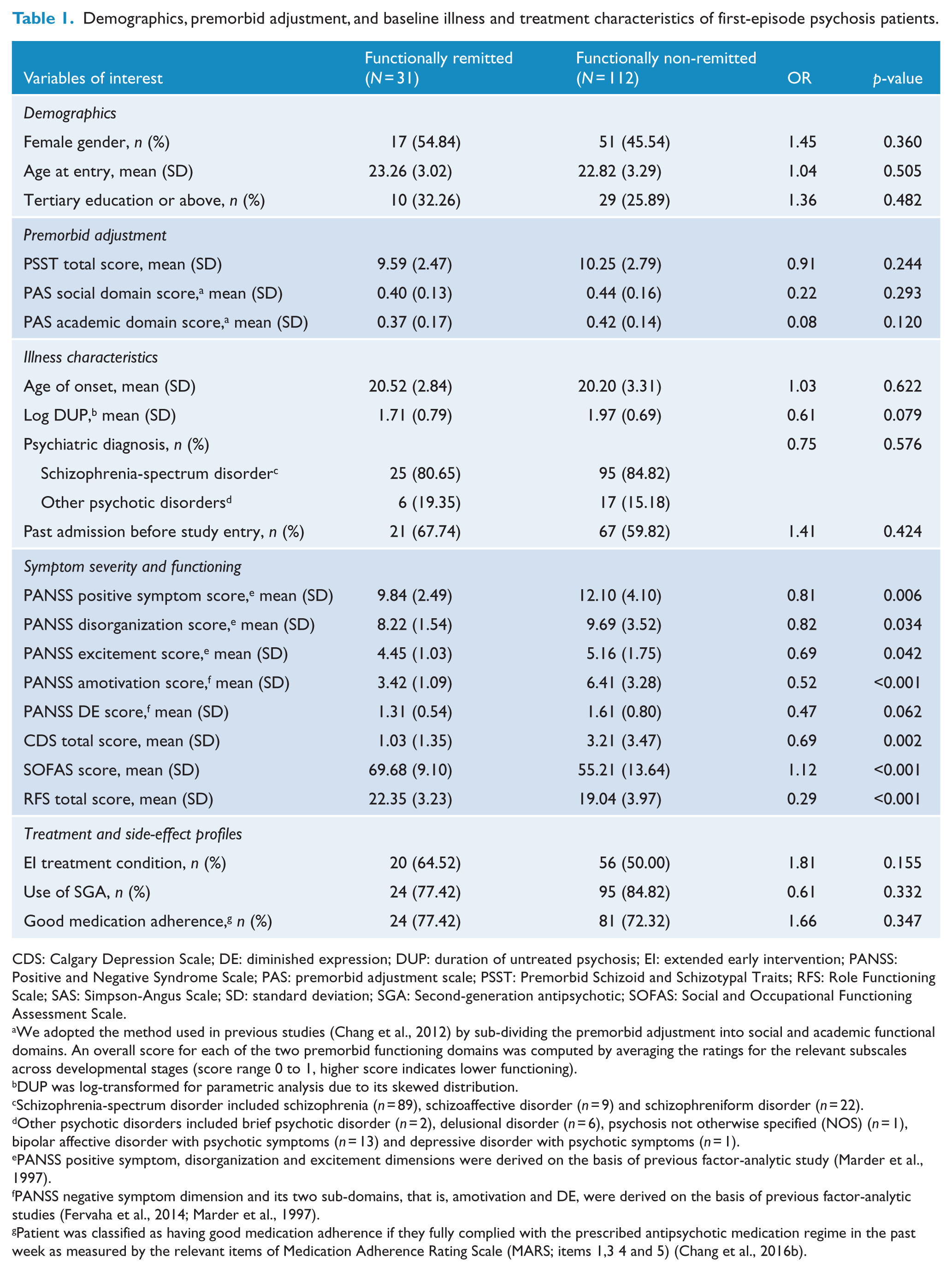
As shown in Table 1, FR was significantly associated with DUP, baseline positive symptom, disorganization, amotivation, DE and depressive symptom scores, and functional levels at intake. Multivariate regression analysis revealed that lower levels of motivational impairment at intake, odds ratio (OR) = 0.61, 95% confidence interval (CI) = [0.42, 0.89], p = 0.010, and better baseline functioning (OR = 1.08, 95% CI = [1.02, 1.13], p = 0.004) independently predicted FR at 3-year follow-up (Table 2).
Demographics, premorbid adjustment, and baseline illness and treatment characteristics of first-episode psychosis patients.
CDS: Calgary Depression Scale; DE: diminished expression; DUP: duration of untreated psychosis; EI: extended early intervention; PANSS: Positive and Negative Syndrome Scale; PAS: premorbid adjustment scale; PSST: Premorbid Schizoid and Schizotypal Traits; RFS: Role Functioning Scale; SAS: Simpson-Angus Scale; SD: standard deviation; SGA: Second-generation antipsychotic; SOFAS: Social and Occupational Functioning Assessment Scale.
We adopted the method used in previous studies (Chang et al., 2012) by sub-dividing the premorbid adjustment into social and academic functional domains. An overall score for each of the two premorbid functioning domains was computed by averaging the ratings for the relevant subscales across developmental stages (score range 0 to 1, higher score indicates lower functioning).
DUP was log-transformed for parametric analysis due to its skewed distribution.
Schizophrenia-spectrum disorder included schizophrenia (n = 89), schizoaffective disorder (n = 9) and schizophreniform disorder (n = 22).
Other psychotic disorders included brief psychotic disorder (n = 2), delusional disorder (n = 6), psychosis not otherwise specified (NOS) (n = 1), bipolar affective disorder with psychotic symptoms (n = 13) and depressive disorder with psychotic symptoms (n = 1).
PANSS positive symptom, disorganization and excitement dimensions were derived on the basis of previous factor-analytic study (Marder et al., 1997).
PANSS negative symptom dimension and its two sub-domains, that is, amotivation and DE, were derived on the basis of previous factor-analytic studies (Fervaha et al., 2014; Marder et al., 1997).
Patient was classified as having good medication adherence if they fully complied with the prescribed antipsychotic medication regime in the past week as measured by the relevant items of Medication Adherence Rating Scale (MARS; items 1,3 4 and 5) (Chang et al., 2016b).
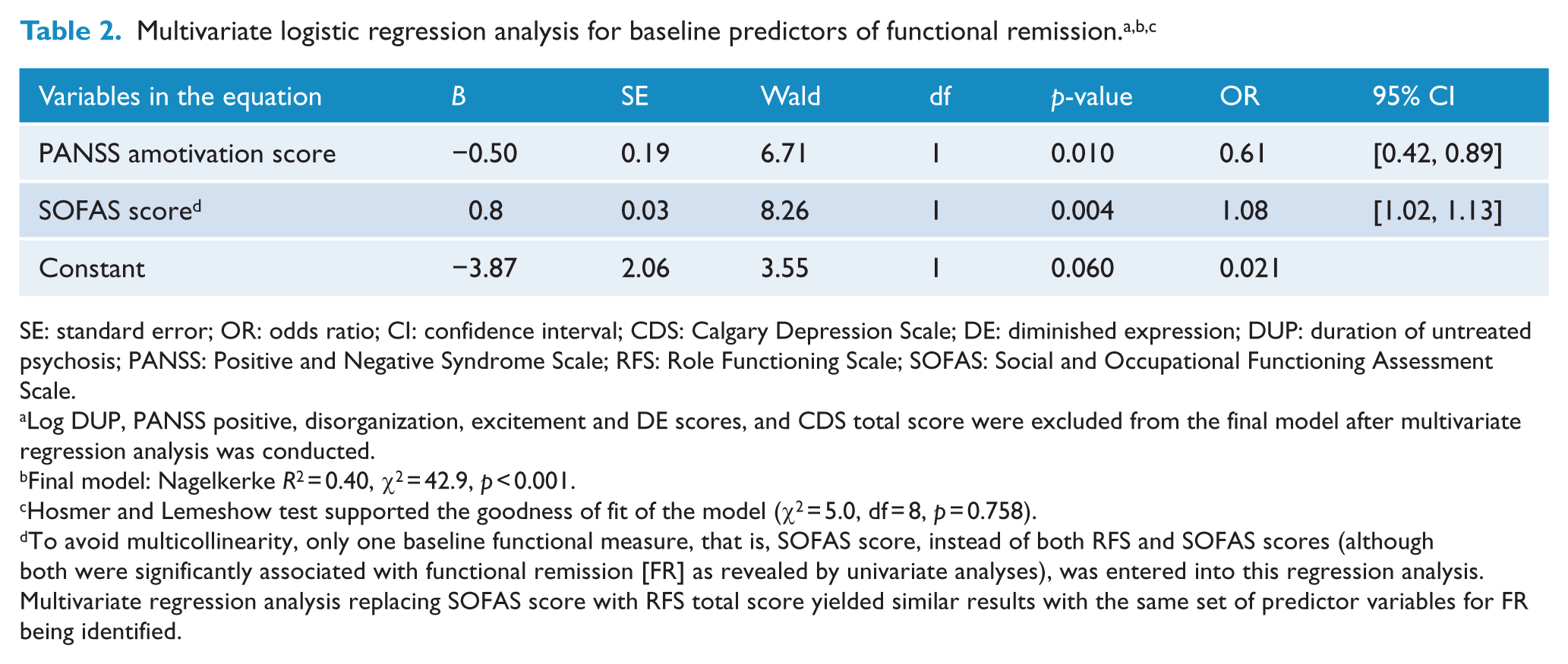
SE: standard error; OR: odds ratio; CI: confidence interval; CDS: Calgary Depression Scale; DE: diminished expression; DUP: duration of untreated psychosis; PANSS: Positive and Negative Syndrome Scale; RFS: Role Functioning Scale; SOFAS: Social and Occupational Functioning Assessment Scale.
Log DUP, PANSS positive, disorganization, excitement and DE scores, and CDS total score were excluded from the final model after multivariate regression analysis was conducted.
Final model: Nagelkerke R2 = 0.40, χ2 = 42.9, p < 0.001.
Hosmer and Lemeshow test supported the goodness of fit of the model (χ2 = 5.0, df = 8, p = 0.758).
To avoid multicollinearity, only one baseline functional measure, that is, SOFAS score, instead of both RFS and SOFAS scores (although both were significantly associated with functional remission [FR] as revealed by univariate analyses), was entered into this regression analysis. Multivariate regression analysis replacing SOFAS score with RFS total score yielded similar results with the same set of predictor variables for FR being identified.
Discussion
In the current analysis, we found that 21.7% of participants achieved FR at the end of 3-year follow-up. This is similar to our earlier finding observed in the same RCT cohort with FR rate of 19.9% at 1-year follow-up (Chang et al., 2016b) and is in the lower range of that reported (17.7–58.4%) in the first-episode literature. It should, however, be noted that substantial methodological heterogeneity across studies may preclude direct comparison of our results with those of previous research. In particular, there might be an overestimation of FR rates in some FEP samples whose FR status was defined cross-sectionally (Alvarez-Jimenez et al., 2012; Verma et al., 2012) without taking into consideration the duration criterion.
In line with previous studies (Chang et al., 2012, 2016b; Flyckt et al., 2006; Lambert et al., 2008b), we found that baseline functioning was independently associated with FR status. Our finding that motivational impairment at study intake predicted FR attainment at 3-year follow-up is well aligned with the literature which found that amotivation was significantly related to concurrent (Chang et al., 2017a; Faerden et al., 2009; Fervaha et al., 2013a) and longitudinal (up to 1 year; Chang et al., 2016a; Faerden et al., 2010, 2013; Fervaha et al., 2015a) functional outcome in early psychosis. In contrast with some prior investigations showing that impaired emotional expressivity was linked to poor functional outcome (Evensen et al., 2012b), our results revealed a lack of significant relationship between DE and FR status in the final multivariate regression model. This is, however, consistent with increasing evidence demonstrating that DE does not contribute independently to functional outcome prediction (Chang et al., 2017a; Fervaha et al., 2014; Green et al., 2012a). Our results thus confirm the differential relationships of negative symptom sub-domains with FR attainment in FEP and indicate that the predictive capacity of negative symptoms on functional levels is mainly contributed by deficits in motivation rather than emotional expressivity. Alternatively, we found that positive symptoms, disorganization and depression failed to predict FR at follow-up (despite significant associations observed in univariate analyses) and hence replicate the results of most previous research (Chang et al., 2016a; Faerden et al., 2013, 2015; Milev et al., 2005a) which showed that negative symptoms, in particular motivational impairment, is predictive of functional outcome above and beyond the contributions of other symptom dimensions.
Contrary to our previous findings on prediction of FR at 1-year follow-up (Chang et al., 2016b), we failed to find any significant association of FR status at 3-year follow-up with female gender or premorbid personality. More importantly, we found an absence of positive effect of Extended EI on enhancing the likelihood of FR attainment at the end of 3-year study period. This negative finding reflects the non-sustainability of superior effect of Extended EI over SC on functional improvement after specialized service was ended (Chang et al., 2017b). This, nonetheless, concurs with two previous post-RCT follow-up studies (Bertelsen et al., 2008; Gafoor et al., 2010) which also failed to demonstrate sustained beneficial effects of specialized EI over standard care on functional outcome after transition to generic psychiatric service. Of particular note, an apparent loss of superiority and hence lack of predictive value of Extended EI on subsequent FR attainment might be attributable to an array of factors including inadequacy of our local existing EI service (e.g. insufficient treatment intensity with high patient to case manager ratio), disruptive effect resulting from an abrupt transfer of care from EI to generic service (Chang et al., 2017b) and dilution of the long-term impact of Extended EI on functional outcome by an improvement in overall quality of local generic care with recently enhanced community psychiatric service received by patients during the 2-year post-trial period. Owing to the paucity of existing data, further research is needed to clarify the optimal duration and active treatment elements of EI to facilitate sustained functional improvement, FR attainment and hence early recovery of people with FEP.
Consistent with most (Alvarez-Jimenez et al., 2012; Chang et al., 2016b; Flyckt et al., 2006; Lambert et al., 2008; Ventura et al., 2011), though not all (Verma et al., 2012), previous studies examining FR in FEP, our finding revealed a lack of independent contribution of DUP to FR attainment at 3-year follow-up. This seems to be at odds with some recent data showing that shorter DUP was associated with recovery in FEP (Petersen et al., 2008; Wunderink et al., 2009). It might be possible that the comparatively briefer DUP (median DUP: 13 weeks) of our cohort might also obscure the potential impeding effect of prolonged untreated psychosis on FR attainment. Another possible explanation is that inclusion of symptom criteria in operationalizing recovery, which is a more broadly defined construct comprising both symptom and functional dimensions, might blur the differential contributions of DUP to symptom and functional outcomes.
The study results have to be interpreted considering the following methodological limitations. First, amotivation was measured by selected items from PANSS instead of employing an instrument that is designed to specifically assess the degree of amotivation (e.g. Apathy Evaluation Scale, Marin et al., 1991). Adoption of the latter would provide a more refined assessment of amotivation and may therefore improve the accuracy in deriving the prospective prediction model for FR. Second, the comparatively lower degree of inter-rater reliability for PANSS negative symptom subscale (ICC = 0.79) than that of other symptom and functional measures (ICCs of 0.86 or above) might introduce measurement bias which may compromise an accurate estimation of predictors for FR status. Third, cognitive dysfunction, which is one of the major predictors of functional outcome in psychotic disorders (Allot et al., 2011), was not assessed in our study.
In conclusion, our results indicate that lower levels of motivational impairment and better functioning at study intake independently predict FR at 3-year follow-up. Our findings thus underscore amotivation as a critical therapeutic target for promoting FR attainment in the early course of psychotic illness. Further clinical trials evaluating the efficacy of interventions that specifically address motivational deficits such as cognitive therapy targeting at modifying maladaptive attitudinal beliefs (Grant et al., 2012) in people with FEP are warranted. In addition, more research is required to unravel the neurobiological underpinnings of motivational impairment in psychotic disorders so as to facilitate development of effective treatments to ameliorate diminished motivation and its adverse impacts on functional outcome.
Footnotes
Acknowledgements
We thank all the coordinating clinicians and staff from the psychiatric inpatient and outpatient units, as well as the medical records departments for their kind assistance. We are also grateful to the individuals who participated in the study.
Declaration of Conflicting Interests
E.Y.H.C. has participated in the paid advisory board for Otsuka, has received educational grant support from Janssen-Cilag and has received research funding from Astra-Zeneca, Janssen-Cilag, Eli Lilly, Sanofi-Aventis and Otsuka. The other authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This study was supported by grants from the Commissioned Research on Mental Health Policy and Services (SMH-29) and Health and Medical Research Fund (HMRF no. 11121881) of the Food and Health Bureau, the Government of Hong Kong Special Administrative Region. The funding body had no involvement in any aspect of the study or manuscript preparation.