
Abstract
Psychosis is a clinical problem that although rare in the community is a cause of considerable long-term morbidity and mortality [1], [2]. The management of first episode psychosis has altered over the past decade with the development of early intervention teams with their brief of rapid response, engagement, continuity of care and a balanced biopsychosocial approach. Research has emphasized that caution is needed in determining diagnosis early in the course of illness with the recognition that the boundaries between syndromes are often tenuously based upon duration of symptoms arbitrarily determined [3], or upon a predominant pattern of psychopathology when the admixture of symptoms is increasingly being recognized as the rule [2], [4]. The problems of comorbidity with substance abuse [3], [4] and cognitive impairment [5], [6] are recognized as essential issues to be addressed in the management plan. Pharmacological treatments for the various syndromes that make up psychosis are often pragmatic with antipsychotic and antidepressant medication being used together in a symptom rather than disorder based approach.
Research into first episode psychosis has most often focused upon first episode schizophrenia to the exclusion of a broader perspective. This reflects the understandable wish to obtain as homogenous a sample of subjects as possible, but creates a number of difficulties. Diagnosis is made on the basis of a cross-sectional interview. This may be subject to change as the clinical picture develops over the initial six to 12 months after presentation, e.g. the diagnosis of schizophrenia is based partially upon duration of symptoms and may change according to the time period over which the study is carried out. Importantly, the effort to restrict subjects to as homogenous a sample of subjects as possible distances the study from clinical practice where people present with a range of co-morbid conditions. To exclude all such patients radically undermines the utility of any findings.
The Western Sydney First Episode Psychosis Project (WSFEPP) was initiated by clinicians to explore and integrate clinical, neurocognitive and neurobiological descriptors across the spectrum of psychotic disorders, in a clinically representative population of individuals drawn from local early intervention services. The project planned to follow a baseline group of 100 subjects for a minimum of 2 years. This period was chosen because of evidence suggesting that long-term psychosocial function can be accurately predicted from the level of recovery attained at this stage [7].
A number of different aims were subsumed within the project. Specifically, the project sought to investigate key areas of clinical concern, such as symptomatology, substance abuse, aggression and mood disturbance, and examine how these factors were distributed across the whole range of psychotic disorders. In addition, the relationship of these clinical variables to measures of cognitive and psychophysiological function as well as structural neuroimaging will be examined. The emphasis is to determine if the existing categorical nosology was useful across this range of investigations as well as to provide a detailed examination of young people with diagnoses that are frequently excluded from research. This paper serves to introduce the study, describing the sample and the way the existing categories differ in demographics, symptoms, treatment and functioning.
Method
Referrals to Western Sydney and Wentworth Area Mental Health Services (combined population base of approximately 950 000 people [8]) were screened for individuals presenting with a first episode of psychosis. Both areas operate early intervention programs targeted to young people with their first episode of a significant mental illness. In addition to community based early intervention services, subjects were referred from an inpatient unit for adolescents with a significant mental illness at Westmead Hospital. Local private psychiatric practitioners and a private psychiatric hospital were also contacted though only two referrals were received from private practitioners.
Subjects
Inclusion criteria for entry into the project were: (i) aged from 13 to 25 years inclusive; (ii) first contact with mental health services with psychotic symptoms (prior contact for non-psychotic problems was acceptable); and (iii) presence of psychotic symptoms as defined by hallucinations, delusions, formal thought disorder or prominent negative symptoms present for a minimum of 3 days. Exclusion criteria included: (i) treatment with electroconvulsive therapy in the 6 months prior to referral; (ii) gross neurological disease; (iii) developmental delay (IQ < 75); (iv) a history of head injury causing unconsciousness for at least one hour; and (v) though disorder ≥5 on the Positive and Negative Symptom Scale (PANSS) Conceptual Disorganization item.
Diagnosis was made by means of a consensus conference of three qualified psychiatrists that drew upon all available information including project assessment, information from family and case manager and case notes some 6–9 months after initial contact with the subject. Diagnoses were made according to DSM-IV [9] and ICD-10 [10].
Consent was gained with reference to subject's clinical state and personal and family wishes. As subjects were all within the first 3 months of attending a mental health service for the treatment of psychosis they frequently remained symptomatic though they were not markedly thought disordered (see exclusion criteria above). If subjects were judged incapable of providing consent by their treating clinician they were not approached. Once the clinician thought that the subject was capable they were given a brochure about the project and the possibility of involvement was broached by the clinician (either their medical officer or case manager). Subsequently an approach was made by a member of the research team and written informed consent was obtained. As subjects were aged 13–25 years inclusive, family members were almost always involved in the consent process. Further to this process, the project included multiple investigations and agreement to participate was required for each investigation, resulting in some subjects declining to take part in one or other arms of the project.
Baseline investigation
Using a semi-structured interview, subjects were assessed by a psychiatrist who had reached an acceptable level of interrater reliability with the PANSS [11]. Evaluation covered the following areas:
1. Clinical state. Psychiatrists rated the psychotic symptomatology of the subjects using PANSS [11], depression using the Calgary Depression Rating Scale [12], and any manic component using the Young Mania Rating Scale [13]. This allowed for detailed measurement across a range of symptomatic presentations. The duration of undiagnosed psychosis was defined as the period from the first onset of clear positive psychotic phenomena to the time of first mental health assessment for a psychosis. This was established via interview with both patient and parent/next of kin.
2. Premorbid social adjustment – This was assessed using the Premorbid Social Adjustment Scale [14]. The Premorbid Social Adjustment Scale asks parents to rate their children, using a 7-point Likert scale, over five different areas of achievement – sociability, peer relations, scholastic performance, adaptation to school and interests. The parents are asked to assess both childhood (5–11 years) and adolescent (12–16 years) adjustment. If the subject had been referred to the project before turning 17 years only the childhood scale was used.
3. Current psychosocial functioning was assessed using the Role Functioning Scale [15], [16]. This scale assesses four areas of functioning – working productivity, self care, relationship with family and relationship with wider community – using a 7-point scale with broadly based anchor points over the 3 months prior to the assessment.
4. Substance use and aggression. Detailed clinical assessment of frequency and type of recent and long-term substance abuse was made. Assessment of levels of aggression was sought from the primary carer. Both these measures were administered using a semi-structured interview format.
The neuropsychological and psychophysiological assessments that also formed part of the project are described in the accompanying article to this or elsewhere [17], [18].
Data analysis
As the range of diagnoses made split the subjects in the study into a large number of diagnostic categories, subjects were combined into 3 groups to assist further analyses. All subjects with diagnoses of schizophrenia, schizophreniform disorder and schizoaffective disorder were combined into the ‘Schizophrenia’ group. All subjects with bipolar disorder and major depression with psychotic features were combined into a ‘Mood Disorders’ group. The third group was made up primarily of subjects with a diagnosis of Substance induced Psychotic Disorders or Psychosis Not Otherwise Specified and was named the ‘Mixed Psychosis’ group. Descriptive statistical analysis was completed using SPSS V.11.0. ANOVA or Pearson's χ2 was used to examine the relationship between the three groups of subjects as was appropriate.
Results
Over a two-year period 224 referrals were made to the project from which 104 subjects initially consented and met all the inclusion criteria. Subjects did not take part for a variety of reasons which included refusal to take part in research (n = 48), refusing all services (n = 11), uncontactable (n = 16), moved out of area (n = 8), working full-time (n = 7) and did not make criteria for study (n = 30). Those who declined to take part were significantly older (χ2 = 6.703, df = 1, p = 0.01), but did not differ on gender (χ2 = 1.263, df = 1; p = 0.168). A further 10 subjects dropped out because of illness related factors and were unable to complete more than one arm of the study. They were excluded from further analysis. No subject was excluded because of the unavailability of a parent or guardian.
Of those who did complete more than one arm, 44% were diagnosed with schizophrenia (n = 41), 14% bipolar disorder (n = 13), 14% with a substance induced psychotic disorder (n = 13), 12% with a schizophreniform disorder (n = 11), 5% with major depression with psychosis (n = 5), 5% with psychosis not otherwise specified (n = 5), 4% with a brief psychotic disorder (n = 4) and 1% with schizoaffective disorder (n = 1). Two subjects were diagnosed with a non-psychotic disorder at this stage and removed from subsequent analyses.
The three groups differed significantly in their basic demographic profile (Table 1). The most outstanding area of differentiation was the overwhelming gender imbalance in the groups with 70% and 78% of the ‘Schizophrenia’ and ‘Mixed Psychosis’ groups, respectively, being male as against only 33% of the ‘Mood Disorders’ group being male (χ2 = 10.2; df = 2; p = 0.006). This, and the younger age of the subjects with a mood disorder, no doubt contributed to the significant difference that was found in the occupational status of the subjects. A far higher proportion of the ‘Mood Disorders’ group remained students, while a higher proportion of the ‘Mixed Psychosis’ group was employed. A high proportion of the ‘Schizophrenia’ group was either unemployed or receiving a pension (χ2 = 26.7; d.f. = 14; p = 0.021).
Demographic descriptions of study subjects by diagnostic group
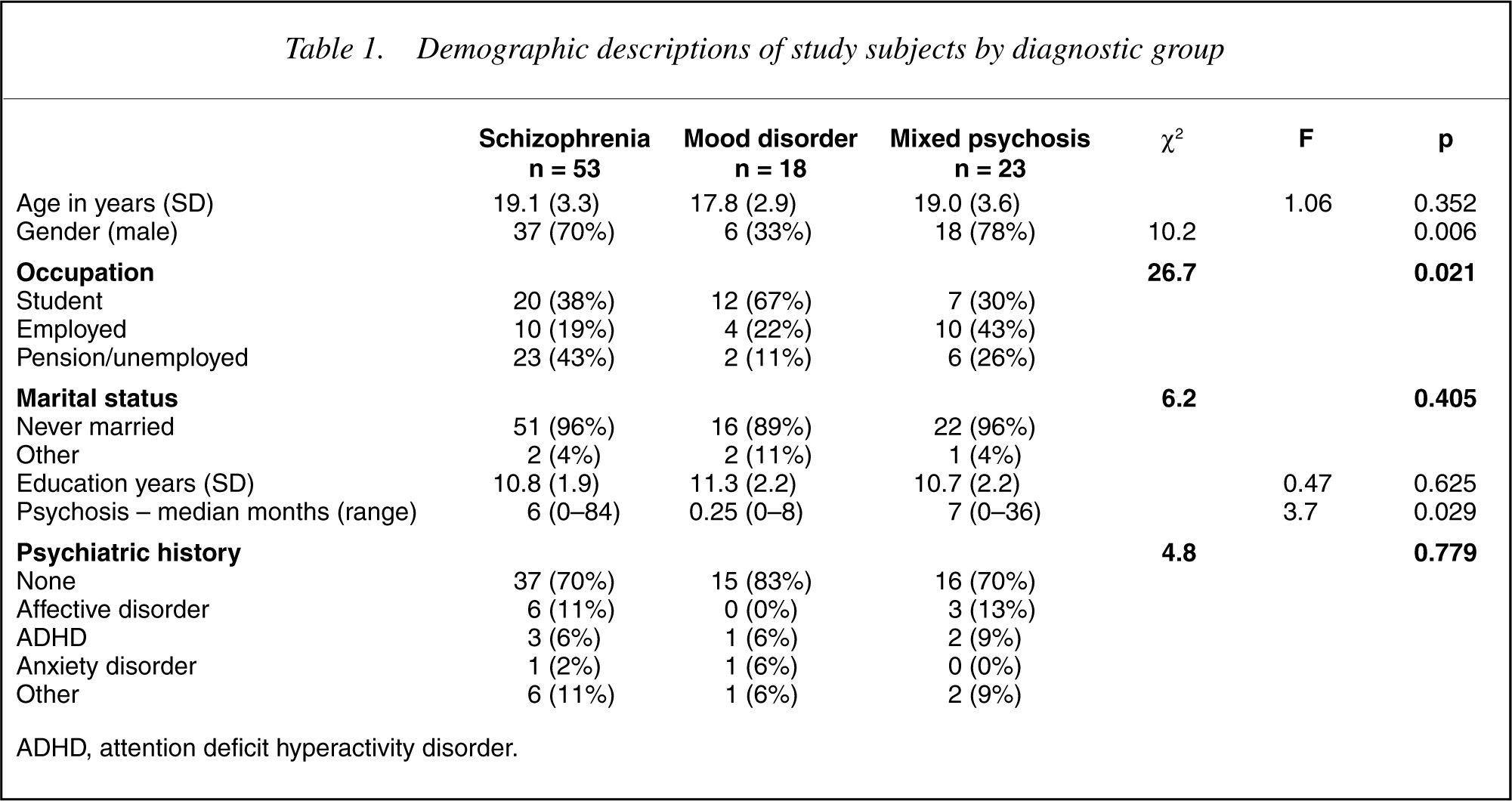
ADHD, attention deficit hyperactivity disorder.
The duration of undiagnosed psychosis was assessed using the median value in light of its skewed distribution. It differed significantly between groups being less in the group with ‘Mood Disorders’ (F = 3.70; d.f. = 2, 75; p = 0.029). There was no evidence to suggest that any group had an increased incidence of prestudy treated psychiatric illness.
The subjects were unwell, displaying levels of symptomatology in the mild to severe range (Table 2). Although there were no significant differences between the three groups for the positive symptom subscale of the PANSS, significant differences were observed for the negative symptom subscale (F = 10.1; df = 2, 91; p = 0.000), the general psychopathology subscale (F = 3.2, d.f. = 2,91; p = 0.044) and the total PANSS score (F = 7.1; df = 2,67; p = 0.002). These differences related to increased psychopathology in the ‘Schizophrenia’ group. The difference was most marked in the negative subscale scores, where the group with ‘Schizophrenia’, even at this early stage of their first presentation clearly displayed higher levels of negative symptoms than the other diagnostic groups. There was a trend for the ‘Mood Disorders’ group to have a higher burden of depressive symptoms. There was no evidence of any differences in manic symptoms between groups.
Symptomatology of study subjects by diagnostic group
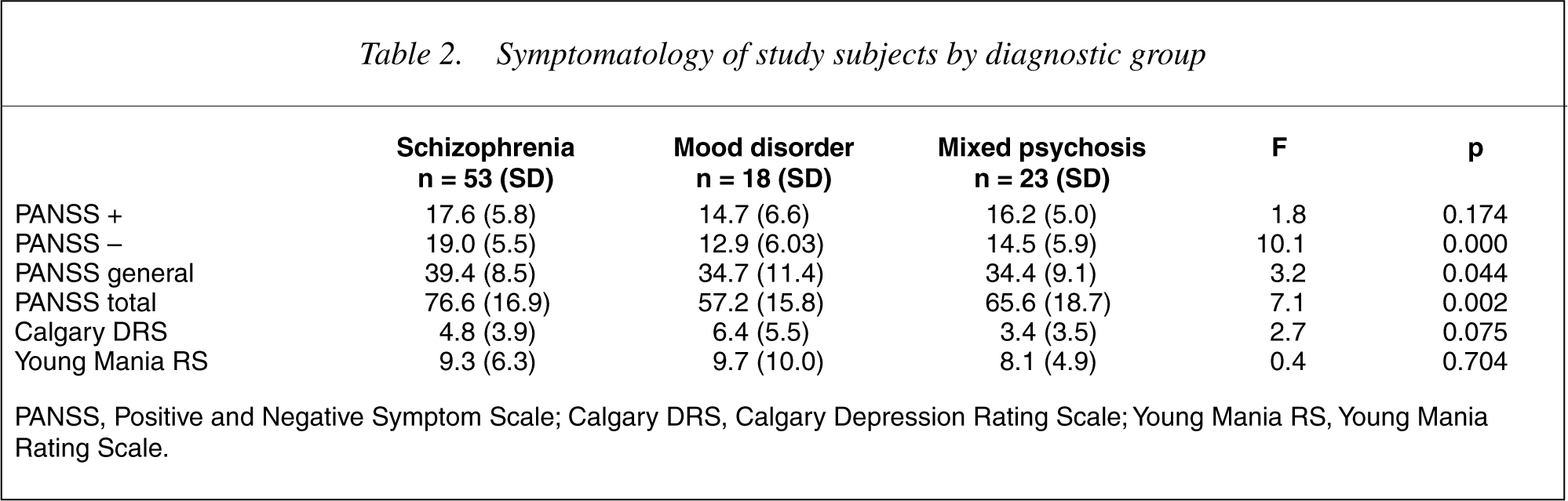
PANSS, Positive and Negative Symptom Scale; Calgary DRS, Calgary Depression Rating Scale; Young Mania RS, Young Mania Rating Scale.
Most subjects were treated with an antipsychotic medication, which in almost all cases was an atypical antipsychotic (19]. Prescription of mood stabilisers differed significantly across groups and this appeared to be because of an increased use in the group with ‘Mood Disorders’ (χ2 = 20.9; df = 4; p = 0.000). Antidepressant use was spread across all groups, underlining the high incidence of depression across the spectrum of psychotic disorders [20].
Medication prescribed to subjects by diagnostic group
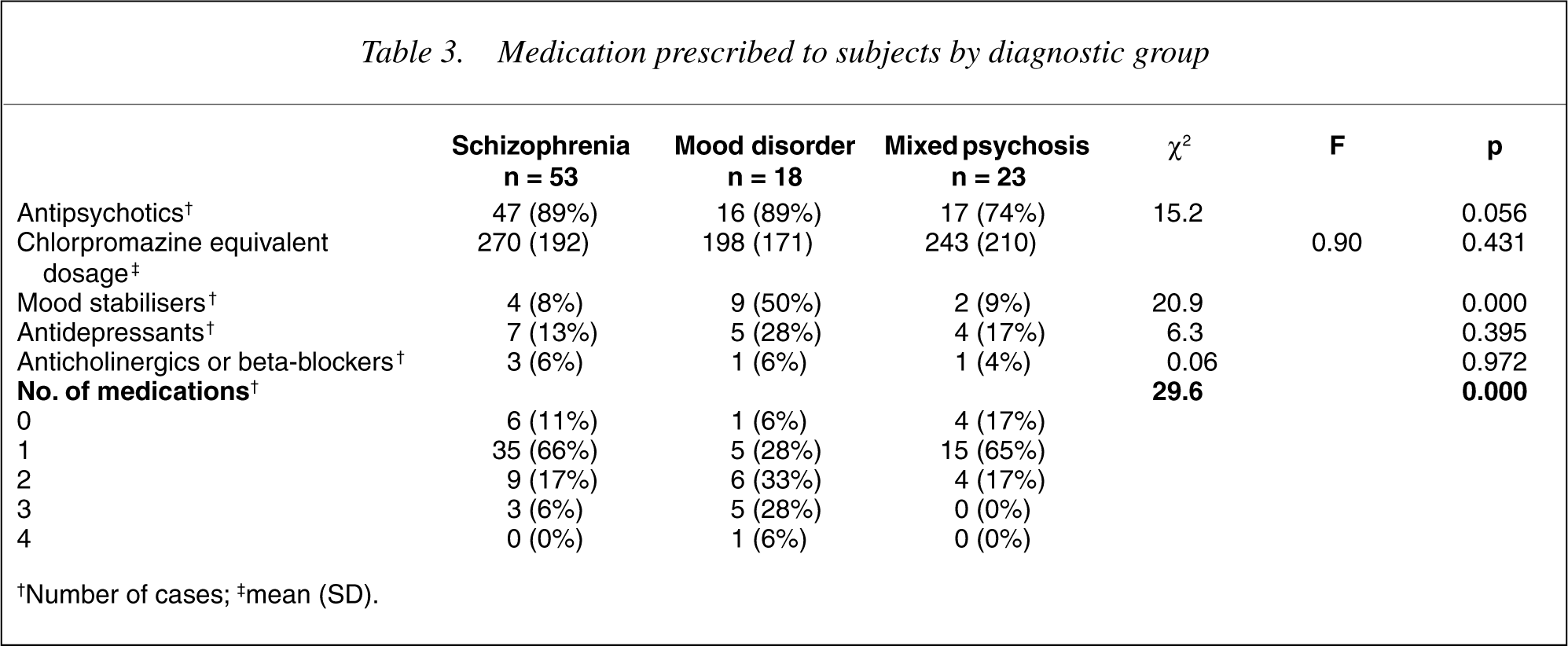
†Number of cases; ‡mean (SD).
The incidence of polypharmacy was also examined. While young people from either the ‘Schizophrenia’ or ‘Mixed Psychosis’ group were more likely to be treated with a single antipsychotic, those from the Mood Disorder group were frequently more likely to be on either two or three medications reflecting combinations of antipsychotic + mood stabiliser +/– another medication (χ2 = 29.6, df = 2; p = 0.000).
14]. In a number of cases, a parent was not available for interview and the subjects were then not included in the analysis. When the age of the subject placed them within the range of the adolescent subscale (12–16 years old), this score was excluded, due to concerns that ratings would reflect performance directly affected by active psychosis. There was a trend evident for decreased schooling during childhood. This reached significance during adolescence when significant difference in school functioning was found between the groups (F = 4.4; df = 2,75; p = 0.016). This appeared to be linked to deterioration in the level of school functioning in the ‘Schizophrenia’ and ‘Mixed Psychosis’ groups.
Premorbid and present day functioning of subjects by diagnostic group
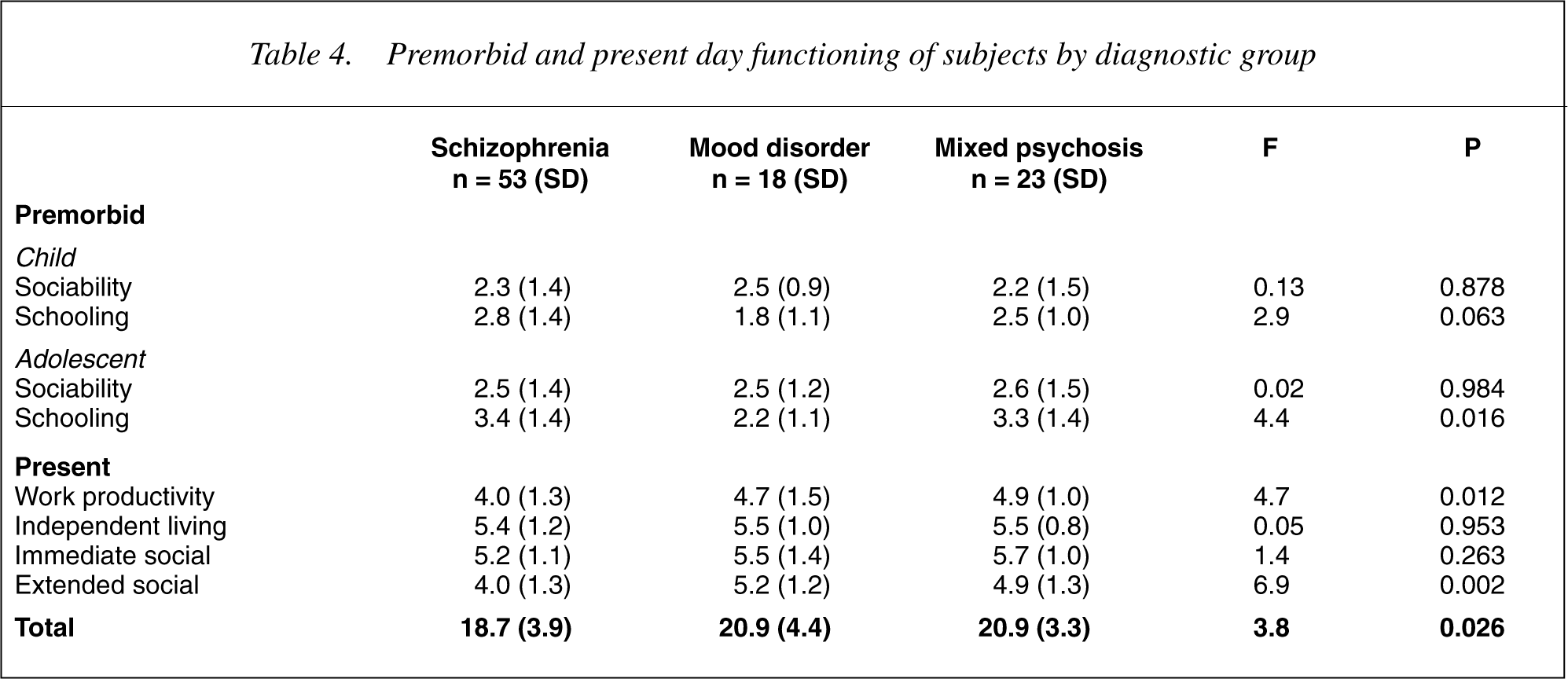
When current social functioning was evaluated using the Role Functioning Scale, there was strong evidence to suggest that the ‘Schizophrenia’ group was more impaired than the other two groups. Work productivity, as measured either in school or in employment, was significantly decreased (F = 4.7; df = 2, 87; p = 0.012), as was the ability to engage a wider social network (F = 6.9; df = 2, 87; p = 0.002). Overall, subjects from the ‘Schizophrenia’ Group had significantly worse social functioning (F = 3.8; df = 2,87; p = 0.026).
Discussion
This paper portrays the characteristics of a group of young people presenting to mental health services with their first episode of psychosis. It remains a crosssectional examination and as such is limited. Further longitudinal examination will help confirm the diagnoses, check for change in diagnosis and provide far more detailed information about the variation of psychopathology and outcome. A more significant limitation is that the final group of subjects only represents slightly under half of the total number referred to the project. Leaving aside the 25% who were found not to meet inclusion criteria, this reflects the difficulty that services can have in engaging with this population. It is concerning that 22% of those who refused to take part in the study were either not contactable or refusing all services. Thus, as far as could be ascertained, as many as 10% of young people who had presented to mental health services with a serious psychiatric condition were not being treated. This was despite the existence of early intervention teams in the catchment area of the project, all with a practice of assertive follow-up and care. We can only hope that the majority of these young people found their way to care via other routes.
Although all efforts were made to enlist all possible subjects including those from the private sector, it is likely that some potential subjects for the trial were either not referred by their private practitioner or were referred to psychiatrists working outside the catchment area. As this potential group was not detained compulsorily, and did not come to the notice of a public mental health service, they probably represent a group with a milder form of psychotic illness than those referred to the project.
The study sample did differ significantly from the referred sample which was slightly older. Despite this, the study underlines that in the 13–25 years age group schizophrenia is predominantly a diagnosis of young men, who have already withdrawn from education after a relatively unsuccessful engagement with school. They are unskilled, unemployed and socially isolated. This is accompanied by higher levels of total psychopathology but especially negative symptoms. High levels of depression are already evident, but this has not yet translated through to pharmacological treatment, which is usually limited to an atypical antipsychotic medication alone.
On the other hand the ‘Mixed Psychosis’ group, although of a similar age and gender mix as the group with ‘Schizophrenia’ were less symptomatic, particularly less troubled by negative or depressive symptoms. They were more likely to be employed despite leaving school at comparable periods as those subjects with ‘Schizophrenia’ and had better social contacts both with family and with the broader community. This might be surprising in a group that had high levels of polysubstance abuse which is usually linked with poor outcome.
The differences in occupational outcomes may in part be due to the gender imbalance between groups. Whilst two-thirds of the ‘Mood Disorders’ group remained engaged with education, in the male-dominated ‘Schizophrenia’ and ‘Mixed Psychosis’ groups, over half had left school, were working, unemployed or receiving government benefits. The ‘Mixed Psychosis’ group was more likely to be employed and less likely to be receiving social security benefits when compared to the ‘Schizophrenia’ group. The gender imbalance in the ‘Schizophrenia’ group is not observed in population based surveys of schizophrenia [21]. This may be a product of the age inclusion criteria, placing a ceiling upon the age of the study population of 25 years excluding later onset schizophrenia which tends to have a greater preponderance of women. In turn, this would bias the study as early onset and male gender both predispose towards a poorer outcome [21].
The measurement of the duration of undiagnosed psychosis, as well as its significance, is a vexed issue in this field [22]. However it did mark an area of clear differentiation between ‘Mood Disorders’ and the other diagnostic groups. The ‘Mood Disorders’ group had only brief periods of undiagnosed psychosis as against widely varying periods for both the ‘Schizophrenia’ group and the ‘Mixed Psychosis’ group. The data was skewed markedly with a small number of subjects with very long histories of psychosis in the ‘Schizophrenia’ and ‘Mixed Psychosis’ groups. For both of these groups, the first experience of psychotic symptoms was frequently in the context of substance use.
Past psychiatric history did not differentiate between groups, nor did the presence or type of diagnosis of family psychiatric illness. Proportionally fewer of the subjects in this study had been diagnosed prior to the onset of their psychosis with a psychiatric disorder than observed in other studies [23], but this may relate to the age limitation on entry, especially in regards to the diagnosis of mood disorders which frequently has an onset at an older age.
Although negative symptoms were identified in all clinical groups, they were a defining characteristic of the ‘Schizophrenia’ group. In other diagnostic groups they have been observed to be less pervasive [2],[24–26] and in follow-up less persistent [27] than in schizophrenia. They were more specific than mood symptoms, which were identified in all clinical groups. Depressed mood and depression is widely experienced in psychosis and has been observed to form an independent symptom domain in both cross sectional [24], [28], [29] and longitudinal studies [30], [31]. There is some evidence to suggest that it may be a particular problem during and after the first episode of psychosis [20].
Antipsychotic medication was the most frequently prescribed medication (32].
Although past reports had indicated that subjects with schizophrenia [14],[33–35] have poorer levels of premorbid social functioning, debate remained about premorbid psychosocial dysfunction in mood disorders [33], [34]. Remarkably little difference was observed between groups for this measure until adolescence when the level of academic attainment dropped for both the ‘Mixed Psychosis’ and ‘Schizophrenia’ groups. For many of the young subjects with schizophrenia, it can be argued that what is being measured here is the deterioration expected during the prodrome of the illness, and for those with a substance induced psychosis, the social disruption experience by those with high levels of substance misuse. In addition, as this information was gathered from family members usually within a few months of the first contact with mental health services, difficulties with recall and attribution bias would be expected. The assessment of premorbid functioning remains difficult.
Measures of present day social and vocational functioning suggested that the ‘Schizophrenia’ group was the most impaired group of the three, with significantly lower productivity at work or at school and a less developed extended social network. Both the ‘Mood Disorders’ and the ‘Mixed Psychosis’ groups had similar levels of social functioning. Besides diagnostic criteria that ensconce deterioration in psychosocial functioning as part of the definition of schizophrenia in DSM-IV, factors that may have contributed to poorer social functioning in the ‘Schizophrenia’ group include the level of negative symptoms [36], [37] and cognitive functioning [37], [38]. This divergence in the level of social competence of young people with schizophrenia from young people with mood disorders has been observed from early adolescence [39] and can be linked to the higher rates of isolation and lower rates of marriage in men with schizophrenia and a poorer quality of life [40], [41].
A confounding factor of the association of psychosocial decline and schizophrenia is the circularity of the diagnosis of schizophrenia that requires psychosocial decline as one of its criteria. Compounding this are negative symptoms, in themselves an important part of the diagnosis of schizophrenia, but defined in part by social withdrawal and a loss of the social persona, both indicators of psychosocial function. So it is hardly surprising to find high levels of psychosocial dysfunction in young people with schizophrenia. Although this is merely tautological if viewed alone, when placed in the context of other diagnostic groups of young people with psychosis it is more informative. Young people diagnosed with a psychotic illness have diminished psychosocial function along many dimensions of measurement. Individuals may bounce back rapidly, but on average, even those with psychotic mood disorders are significantly impaired. Further, negative symptoms are found in other diagnostic groups, albeit at lower levels, even at this early stage of illness. However, over and above this, those diagnosed with schizophrenia clearly have the most severe degree of impairment and thus should be the target of particular therapeutic effort.
This paper serves as an introduction to a complex longitudinal project. Unlike other such projects, the subjects for it are drawn from a representative community sample, have been diagnosed with a spectrum of psychotic disorders and have been treated almost universally with atypical antipsychotic medication. As is evident from the results presented, the subjects have significant levels of symptomatology and disability established at the time of their first presentation to mental health services. These deficits are most severe for people diagnosed with schizophrenia or schizophreniform disorder but are by no means negligible for those with either mood or other psychotic illnesses. This exploration of the consequences of being psychotic as against suffering from schizophrenia will be a continued focus of the project.
Footnotes
Acknowledgements
Thanks to Mark Kneebone, Wayne Reid and Sue Meares for their help in the project. This research was funded in part by the Centre for Mental Health, NSW Health and the Neuroscience Institute for Schizophrenia and Allied Disorders (NISAD).