
Abstract
Objective:
Most studies have investigated either the singular or relative contributions of premorbid adjustment, verbal memory and symptom remission to functional outcomes in first-episode psychosis. Fewer studies have examined the pathways of these factors in impacting functioning. Our study addresses this gap. The objective was to determine whether the relationship between premorbid adjustment and functional outcomes was mediated by verbal memory and symptom remission.
Method:
A total of 334 first-episode psychosis participants (aged 14–35 years) were assessed on premorbid adjustment, verbal memory upon entry, and positive and negative symptom remission and functioning at multiple time points over a 2-year follow-up.
Results:
Mediation analyses showed that over the first year, the relationship between premorbid adjustment and functioning was mediated by verbal memory and positive symptom remission (β = –0.18; 95% confidence interval = [–0.51, –0.04]), as well as by verbal memory and negative symptom remission (β = –0.41; 95% confidence interval = [–1.11, –1.03]). Over 2 years, the relationship between premorbid adjustment and functioning was mediated by verbal memory and only negative symptom remission (β = –0.38; 95% confidence interval = [–1.46, –0.02]).
Conclusion:
Comparatively less malleable factors (premorbid adjustment and verbal memory) may contribute to functional outcomes through more malleable factors (symptoms). Promoting remission may be an important parsimonious means to achieving better functional outcomes.
Introduction
Resuming functional roles following a first episode of psychosis (FEP) is a very significant marker of recovery (Windell et al., 2012). One established predictor of the resumption of functioning is premorbid adjustment (Ayesa-Arriola et al., 2013; Jordan et al., 2014; Larsen et al., 2000).
Premorbid adjustment has been independently linked to verbal memory at illness onset (Addington and Addington, 2005) and to symptom remission (Diaz et al., 2013; Lambert et al., 2010). Verbal memory has also been shown to predict symptom remission (Benoit et al., 2014; Bodnar et al., 2008), and both verbal memory and symptom remission have been reported as predicting the level of functioning among persons with psychosis (Green, 1996; Green et al., 2000; Jordan et al., 2014; Lutgens et al., 2014). Furthermore, verbal memory has been shown to mediate the relationship between symptoms and functioning (Lin et al., 2013; Ventura et al., 2009). While no study has examined if premorbid adjustment’s influence on symptom remission is mediated by verbal memory, these findings taken together suggest that the influence of premorbid adjustment on functional outcomes in psychosis may be mediated by verbal memory and symptom remission.
While several studies have examined the singular roles of premorbid adjustment, verbal memory and symptoms in predicting functioning or their roles relative to one another, most have analyzed their importance using correlational or regression approaches (Ayesa-Arriola et al., 2013; Chang et al., 2013; Macbeth et al., 2014; Malla et al., 2002). Although valuable, such approaches have made it difficult to examine how such factors interact to impact functioning while acknowledging that they may emerge at different junctures temporally over the course of the illness. Specifically, research thus far on predictors of functioning in FEP has not yielded many insights on the pathways by which premorbid adjustment impacts functional outcomes.
Our objective was to address the knowledge gap on how the impact of premorbid adjustment on later functioning may be mediated by additional factors. Specifically, we hypothesized that the relationship between premorbid adjustment and functioning after 1 and 2 years of treatment will be mediated by verbal memory at illness onset and positive and negative symptom remission over the course of 1 and 2 years.
Methods
Participants
Participants were individuals treated for FEP at the Prevention and Early Intervention Program for Psychosis (PEPP) between 2003 and 2011. PEPP is the only specialized early intervention service treating all potential FEP cases in a specific Montreal catchment. PEPP serves individuals aged 14–35 years with a Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) diagnosis of non-affective or affective psychosis not caused by organic brain disease, an IQ above 70 and no history of antipsychotic medication for more than 30 days. Treatment is provided for 2 years and comprises intensive case management and psychosocial (e.g. family psychoeducation) and medical management (Iyer et al., 2015). The relevant ethics board approved the study and all participants granted informed consent.
Materials
Premorbid adjustment
Educational and social functioning prior to illness onset were measured using the Premorbid Adjustment Scale (PAS) (Cannon-Spoor et al., 1982). We considered scores only for childhood (up to age 11) and early adolescence (12–16 years), and not for the period above 16 years. This was done to avoid overlap with the period when prodromal/psychotic symptoms usually manifest. Scores of 0 on the PAS imply good premorbid functioning, while scores of 1 imply poorer premorbid functioning.
Verbal memory
A neurocognitive battery was administered when participants were clinically stable, usually by month 3. We focused on verbal memory because it is a well-established predictor of functional outcomes (Jordan et al., 2014; Lutgens et al., 2014). Furthermore, verbal memory has been associated with both premorbid adjustment (Addington and Addington, 2005) and symptom remission (Benoit et al., 2014; Bodnar et al., 2008). Verbal memory was assessed using the Logical Memory subtest of the Wechsler Memory Scale-II (Wechsler, 1997). A z-score representing overall verbal memory performance was calculated using the mean and standard deviation of age and gender-matched community healthy controls (n = 73).
Symptom remission
Symptoms were assessed using the Scale for the Assessment of Positive Symptoms (SAPS) (Andreasen, 1984) and the Scale for the Assessment of Negative Symptoms (SANS) (Andreasen, 1983) by trained evaluators with good inter-rater reliability (κ = 0.74 for SAPS; κ = 0.71 for SANS). Assessments were conducted at entry and Months 1, 2, 3, 6, 9, 12, 18 and 24.
Remission was defined according to the Remission in Schizophrenia Working Group’s consensus criteria (Andreasen et al., 2005) as a simultaneous rating of mild or less (⩽2) on specified positive and negative symptoms. Remission from positive and negative symptoms was examined separately for each month from baseline to month 24. We considered the maximum number of months a participant was in remission instead because we felt a continuous remission variable would more accurately reflect each participant’s remission trajectory.
During months where no symptom assessments were conducted, positive symptom remission was established through the last observation carried forward technique and confirmed through clinical notes. For negative symptom remission, we used the last observation carried forward technique, but did not use clinical notes, due to concerns about the reliability of rating negative symptoms from notes. The maximum number of months carried over was 6. Participants missing more than 6 months of symptom data were excluded. Sensitivity analysis conducted in a prior study revealed that up to 82.9% of last observation carried forward technique estimates may be accurate (Jordan et al., 2014).
We included the maximum number of consecutive months in remission in our analyses. Such a continuous variable may be a more ecologically valid and statistically accurate measure of remission (MacCallum et al., 2002).
Covariates
Medication adherence (Miller, 2008), duration of untreated psychosis (DUP) (Norman et al., 2001), age of onset of psychosis (Amminger et al., 2011), sex (Segarra et al., 2012) and substance abuse/dependence (Mazzoncini et al., 2010) were included as covariates due to their known associations with functioning. Using a validated method that surveys participants, families, case managers and clinical notes (Cassidy et al., 2010b), we classified participants as medication-adherent (75–100%) or non-adherent (0–74%) every month. Mode values for medication adherence were analyzed. DUP, defined as number of weeks between the onset of psychosis and the start of adequate antipsychotic treatment, was estimated using a well-established method, the Circumstances of Onset and Relapse Schedule (Norman et al., 2004). Substance abuse/dependence diagnoses at baseline were established using the Structured Clinical Interview for DSM Disorders-IV (American Psychiatric Association, 2000).
Functional outcome
Functioning during the past year was measured at months 12 and 24, using the Strauss Carpenter Scale (Strauss and Carpenter, 1974, 1977). We considered only the subscales for employment (i.e. amount of time employed or in school) and social functioning (i.e. number of times friends were seen).
Results
Data analyses
Analyses were conducted using PROCESS, a widely used SPSS macro for testing mediation which allows the estimation of direct, indirect and total or overall effects. A direct effect is the effect of an independent variable (in our case, premorbid adjustment) on a dependent variable (in our case, functioning). An indirect effect is the effect of a mediator (in our case, verbal memory and positive or negative symptom remission) on the relationship between an independent and a dependent variable. The sum of all indirect effects represents the total indirect effect and the sum of indirect and direct effects represents the overall effect (Hayes, 2013).
Controlling for pertinent covariates, four main analyses were conducted with negative and positive symptom remission tested separately across 1 and 2 years of treatment, yielding four mediation models. Separate models were conducted because positive and negative symptom remission can impact functioning differently (Cassidy et al., 2010a; Jordan et al., 2014).
We tested whether the impact of premorbid adjustment on functioning over 1 and 2 years was mediated by verbal memory, positive symptom remission and negative symptom remission.
Since 0 implies good premorbid functioning and 1 implies poorer premorbid functioning, a negative predictive value for the effect of premorbid adjustment on another variable (e.g. verbal memory) indicates that better premorbid adjustment predicts the second variable (e.g. better premorbid adjustment predicts higher verbal memory).
Initial analyses
Sample
A total of 334 individuals entered PEPP and consented to participate from 2003 to 2011. We excluded those who had incomplete data (i.e. missing baseline, final or 6 or more months of symptom assessments). Of those considered for analyses incorporating positive symptom remission, 81 had incomplete assessments in Year 1, leaving a sample of 253. In Year 2, 134 had incomplete symptom assessments, leaving a sample of 200. Of those considered for analyses incorporating negative symptom remission, 98 had incomplete assessments in Year 1, leaving a sample of 236. In Year 2, 154 had incomplete assessments, leaving a sample of 180. Excluded participants were likelier to have schizophrenia-spectrum (as opposed to affective) psychosis and to be medication-non-adherent (Table 1) but were similar on other relevant demographic and clinical characteristics compared to included participants.
Differences among participants included and excluded from evaluations.
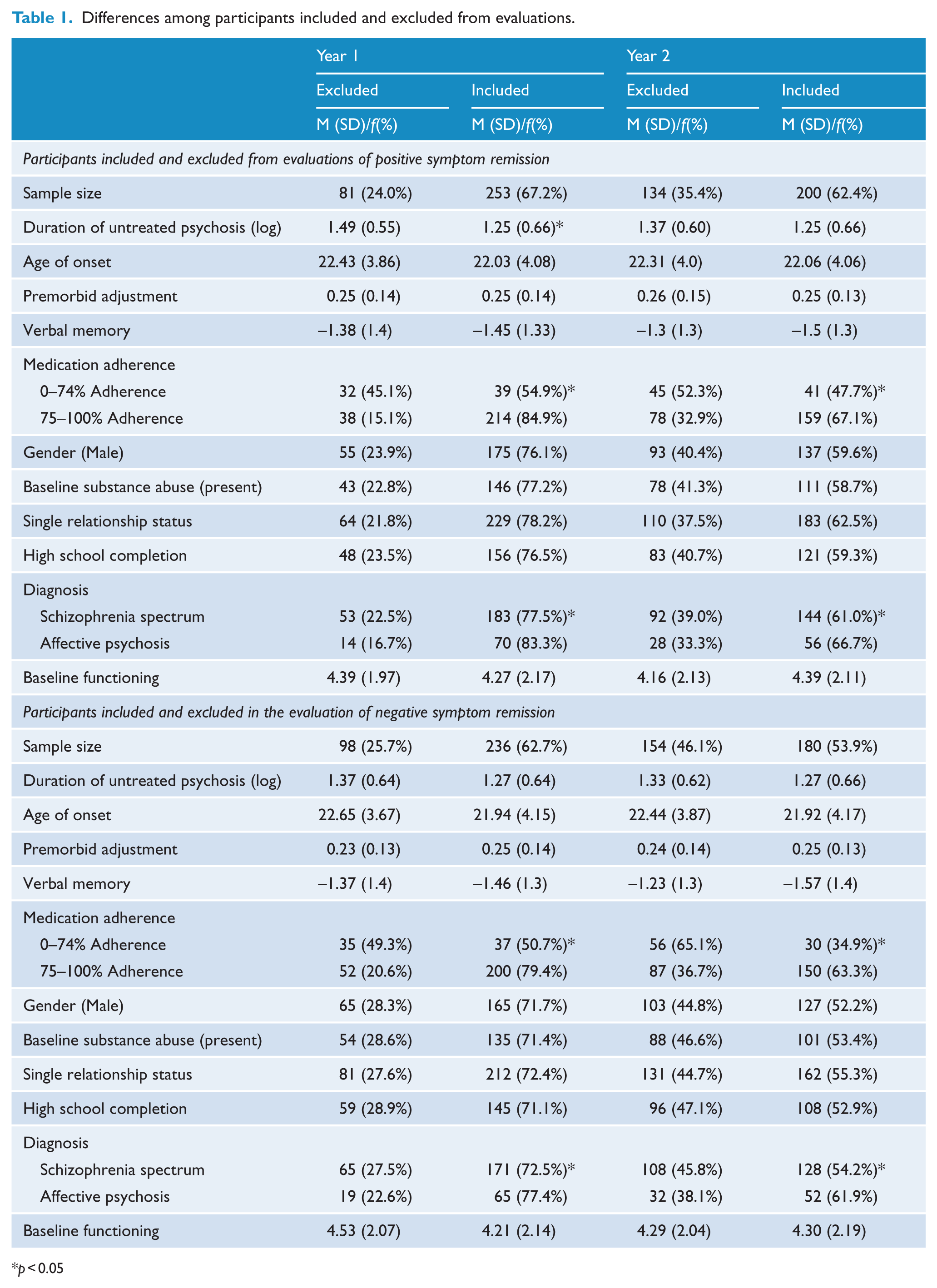
p < 0.05
Data screening
Skewed variables (i.e. DUP, negative symptom remission over Year 2) were corrected with logarithmic transformations. Multicollinearity (r ⩽ 0.4) and non-independence among predictors and covariates was not detected.
Descriptive statistics and correlations
Supplementary Table 1 includes information regarding the maximum number of consecutive months in positive and negative symptom remission over Years 1 and 2 after entry.
Preliminary analyses were performed to determine whether, in addition to a theoretical rationale for including verbal memory as a predictor in our model, there was also a statistical justification for the inclusion of verbal memory. Correlational analyses showed that relative to other cognitive domains (i.e. processing speed, executive functioning, visual memory, problem solving and attention), verbal memory was significantly correlated with PAS, symptom remission and functioning over 1 and 2 years (Table 2). On average, participants scored 1.37 standard deviations lower than healthy controls on verbal memory; F (1,196) = 60.53, p < 0.001. Table 3 presents correlations between PAS, symptom remission and functioning over 1 and 2 years.
Correlations among cognitive domains, premorbid adjustment, symptom remission and functioning.
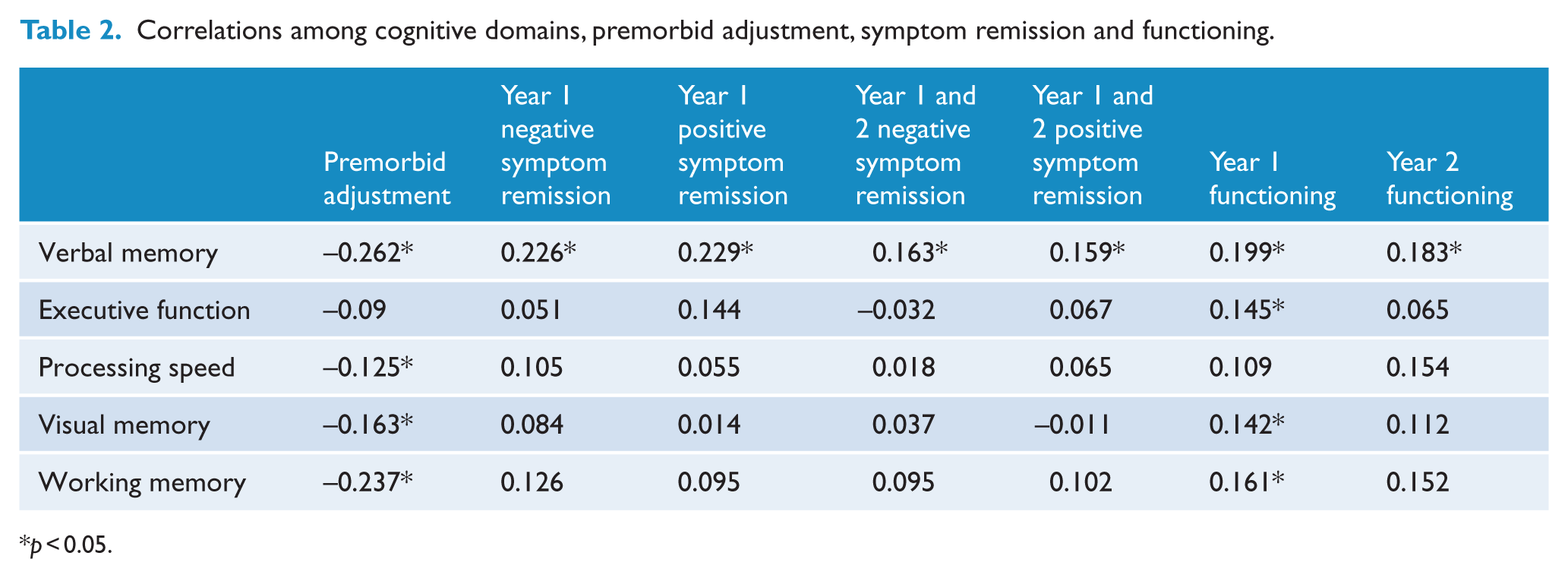
p < 0.05.
Correlations among premorbid adjustment, symptom remission and functioning.
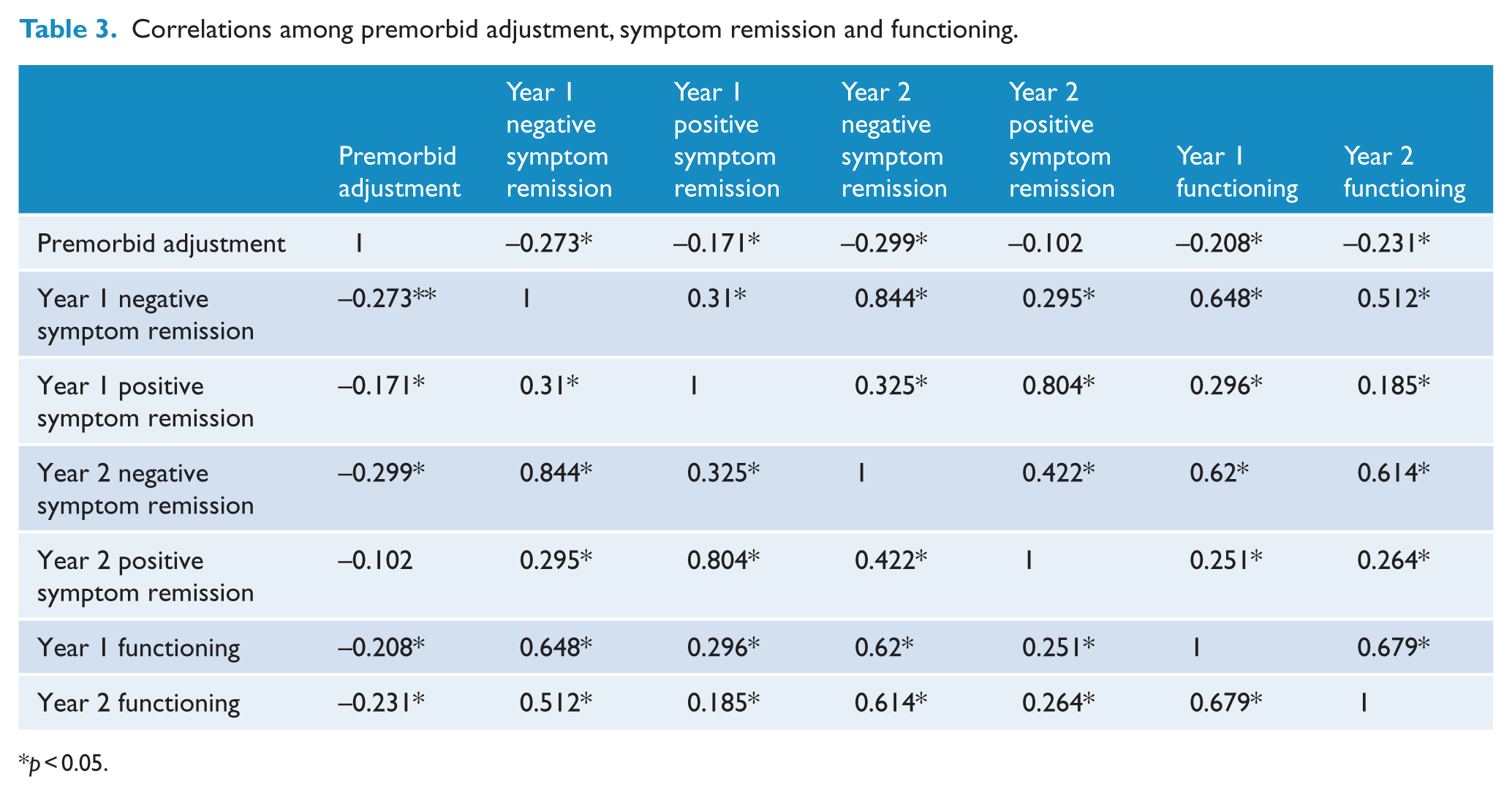
p < 0.05.
Main analyses
Do verbal memory and negative symptom remission mediate the relationship between premorbid adjustment and functioning over the first year?
Better premorbid adjustment predicted higher verbal memory (a = –1.97) and more months in continuous negative symptom remission (a1 = –0.51). Better verbal memory predicted more consecutive months in negative symptom remission (b = 0.07), which, in turn, predicted better functioning (c = 3.04) (Figure 1, Table 4, Supplementary Table 2).
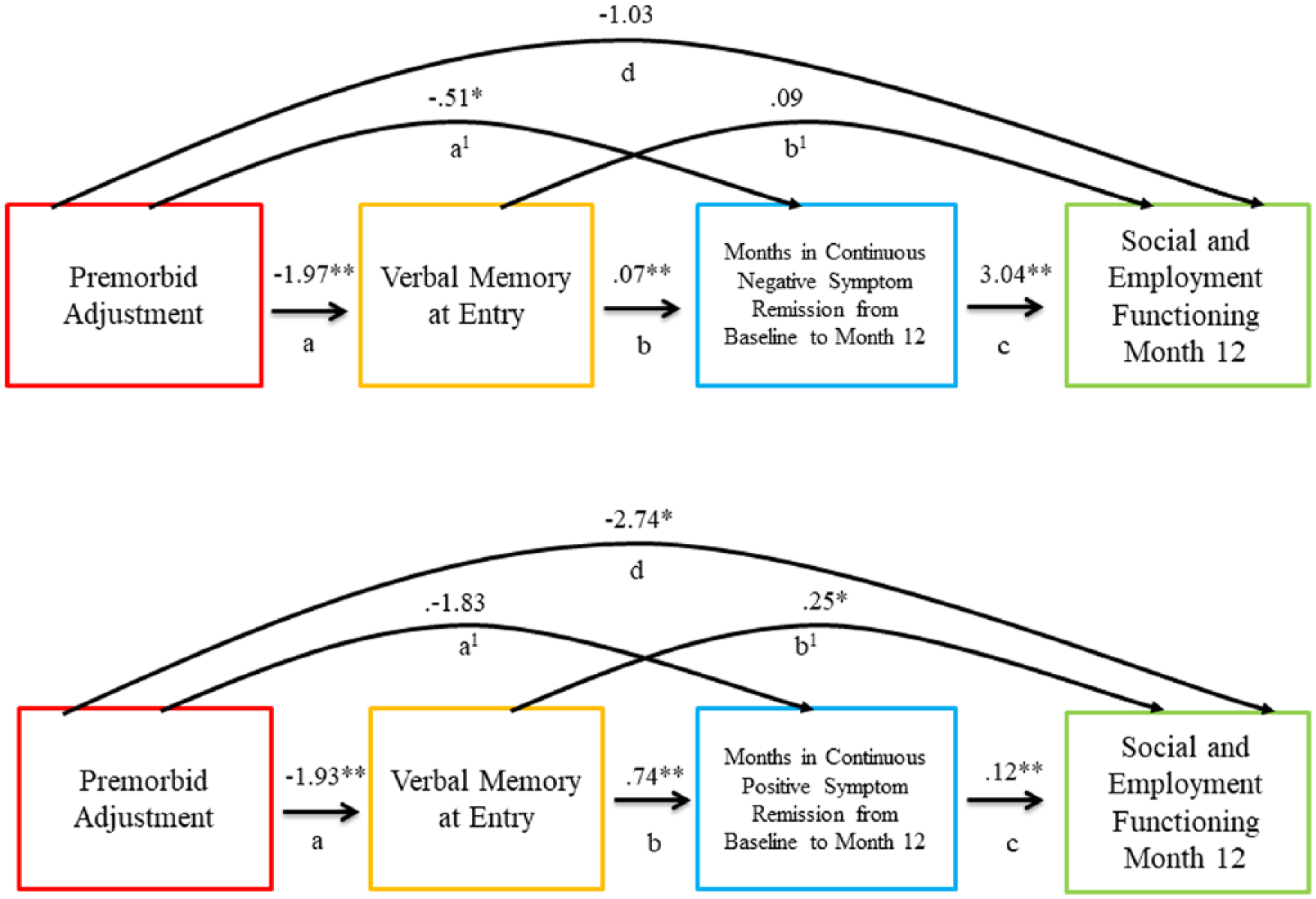
Mediation model depicting Year 1 analysis.
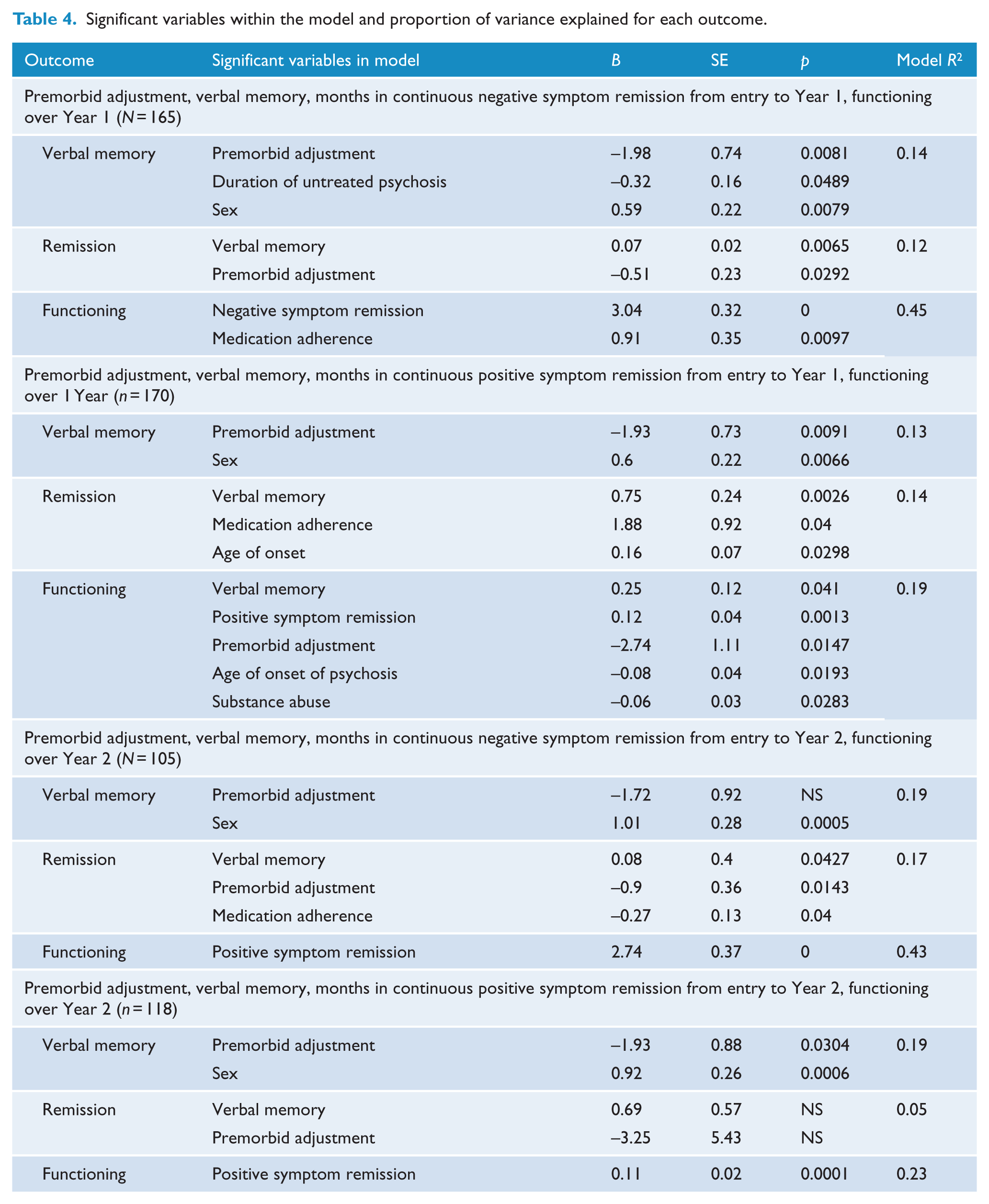
Significant variables within the model and proportion of variance explained for each outcome.
Analyses of bias-corrected bootstrap intervals showed a significant overall effect of the entire model (β = –3.17, SE = 1.16, 95% confidence interval [CI] = [–5.47, –0.88]) and total indirect effect of verbal memory and negative symptom remission (β = –2.15, SE = 0.68, 95% CI = [–3.69, –0.97]). However, no significant direct effect of premorbid adjustment on functioning was observed.
Examining the three specific indirect effects showed that the influence of premorbid adjustment on functioning was fully mediated by verbal memory and months in continuous negative symptom remission (β = –0.41, SE = 0.22, 95% CI = [–1.10, –0.10]).The second specific indirect effect indicated that maximum months in continuous negative symptom remission over the first year significantly mediated the relationship between premorbid adjustment and functioning (β = –1.56, SE = 0.67, 95% CI = [–2.94, –2.93]). The specific indirect effect of verbal memory as a mediator of the relationship between premorbid adjustment and functioning was not significant.
Examining the impact of covariates in this model revealed that DUP (β = –0.32 SE = 0.16, 95% CI = [–0.63, –0.0015]) and a female sex (β = 0.59, SE = 0.22, 95% CI = [0.16, 1.02]) predicted verbal memory, while high medication adherence (β = 0.91, SE = 0.3, 95% CI = [0.22, 1.60]) predicted functioning.
Do verbal memory and positive symptom remission mediate the relationship between premorbid adjustment and functioning over the first year?
Better premorbid adjustment predicted higher verbal memory (a = –1.93), which in turn predicted more consecutive months in positive symptom remission (b = 0.74) and better functioning (b1 = 0.25). The maximum number of consecutive months in positive symptom remission also predicted better functioning (c = 0.12) (Figure 1, Table 4, Supplementary Table 2).
The overall effect of the entire model (β = –3.61, SE = 1.14, 95% CI = [–5.87, –1.36]), the direct effect of premorbid adjustment on functioning (d = –2.74, SE = 1.11, 95% CI = [–4.93, –0.55]) and the total indirect effect of verbal memory and positive symptom remission (β = –0.88, SE = 0.45, 95% CI = [–1.94, –0.16]) were significant.
Examining specific indirect effects showed that the effect of premorbid adjustment on functioning was fully mediated by verbal memory and maximum consecutive months in positive symptom remission over Year 1 (β = –0.18, SE = 0.11, 95% CI = [–0.52, –0.03]). The second specific indirect effect, that of positive symptom remission as a mediator of the relationship between premorbid adjustment and functioning at Year 1, was not significant. The third specific indirect effect, that of verbal memory as a mediator of the relationship between premorbid adjustment and functioning, was significant (β = –0.47, SE = 0.30, 95% CI = [–1.33, –0.05]).
Examining the covariates of this model revealed that female sex predicted verbal memory (β = 0.59, SE = 0.22, 95% CI = [0.17, 1.03]), high medication adherence (β = 1.88, SE = 0.92, 95% CI = [0.06, 3.70]) and an older age of onset of psychosis (β = 0.16, SE = 0.07, 95% CI = [0.02, 0.31]) predicted positive symptom remission, and a younger age of onset of psychosis (β = –0.08, SE = 0.04, 95% CI = [–0.16, –0.01]) and an absence of a substance abuse/dependence diagnosis (β = –0.06, SE = 0.03, 95% CI = [–0.10, –0.006]) predicted functioning.
Do verbal memory and negative symptom remission mediate the relationship between premorbid adjustment and functioning at Year 2?
Better premorbid adjustment predicted more months in continuous negative symptom remission over 2 years (a1 = –0.89) but did not predict verbal memory. Verbal memory predicted months in negative symptom remission over the 2-year course (b = 0.08), which in turn predicted functional outcomes (c = 2.74) (Figure 2, Table 4, Supplementary Table 2).
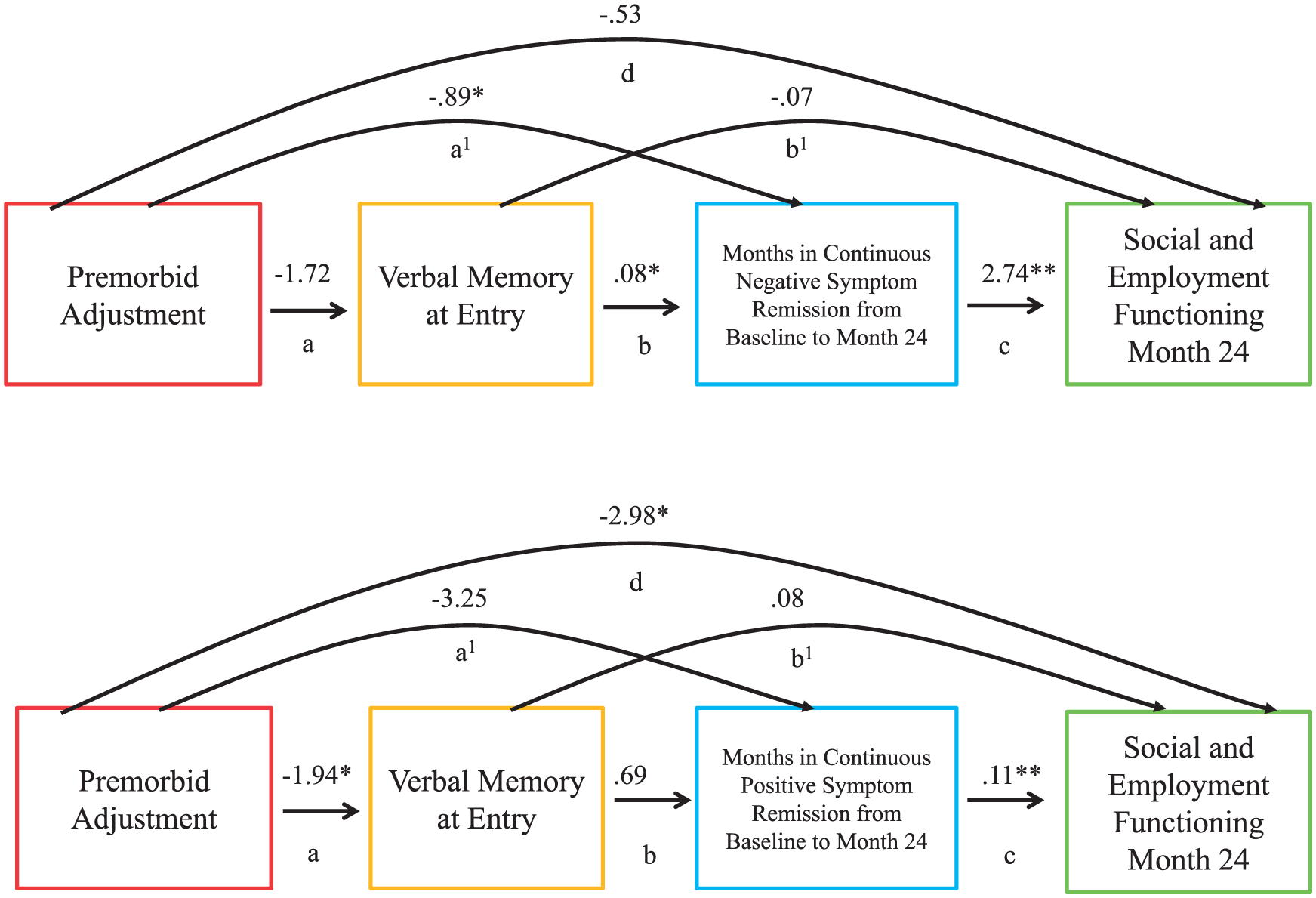
Mediation model depicting Year 2 analyses.
The overall effect of the entire model (β = –3.25, SE = 1.59, 95% CI = [–6.41, –0.08]) and total indirect effect of verbal memory and negative symptom remission (β = –2.72, SE = 1.00, 95% CI = [–4.84, –0.88]) were significant, but the direct effect of premorbid adjustment on functioning was not.
Examining specific indirect effects showed that the effect of premorbid adjustment on functional outcomes was fully mediated by verbal memory and negative symptom remission over 2 years (β = –0.38, SE = 0.28, 95% CI = [–1.46, –0.02]). A specific indirect effect showed that the relationship between premorbid adjustment and functioning was fully mediated by negative symptom remission (β = –2.46, SE = 1.02, 95% CI = [–4.69, –0.50]). The specific indirect effect of verbal memory as a mediator of the relationship between premorbid adjustment and functioning was not significant.
Examining covariates of this model revealed that female sex (β = 1.01, SE = 0.28, 95% CI = [0.45, 1.57]) predicted verbal memory, and lower medication adherence (β = –0.03, SE = 0.13, 95% CI = [–0.53, –0.01]) predicted negative symptom remission.
Do verbal memory and positive symptom remission mediate the relationship between premorbid adjustment and functioning at Year 2?
Better premorbid adjustment predicted better verbal memory (a = –1.94) but not positive symptom remission over 2 years. Verbal memory did not predict symptom remission or functioning. Furthermore, maximum months in continuous positive symptom remission over the 2-year course predicted functioning (c = 0.11) (Figure 2, Table 4, Supplementary Table 2).
The overall effect of the entire model (β = –3.62, SE = 1.52, 95% CI = [–6.62, –0.61]) and direct effects of premorbid adjustment on functioning at 2 years (d = –2.98, SE = 1.44, 95% CI = [–5.84, –0.11]) were significant, but the total indirect effect of verbal memory and positive symptom remission was not.
Examining specific indirect effects showed that the effect of premorbid adjustment on functioning was not mediated by verbal memory and positive symptom remission. Specific indirect effects of either verbal memory or positive symptom remission alone as mediators of the relationship between premorbid adjustment and functioning were not significant.
Examining covariates in this model revealed that female sex predicted verbal memory (β = 0.92, SE = 0.26, 95% CI = [0.40, 1.44]).
Post hoc test
Given that the effect of premorbid adjustment on functioning at Year 2 was not mediated by verbal memory and positive symptom remission (unlike at Year 1), we hypothesized that earlier symptom remission may be more important for functional outcomes than later symptom remission, which is consistent with other findings (Norman et al., 2014).
Verbal memory and early positive symptom remission (i.e. over Year 1) mediated the effect of premorbid adjustment on functioning at Year 2 (β = –0.14, SE = 0.12, 95% CI = [–0.64, –0.01]). Later positive symptom remission (i.e. over Year 2) yielded a non-significant model. Similarly, the effect of premorbid adjustment on functioning at Year 2 was mediated by verbal memory and early negative symptom remission (β = –0.58, SE = 0.38, 95% CI = [–1.61, –0.05]). Including only later negative symptom remission again yielded a non-significant model.
Discussion
To our knowledge, no study has specifically examined how the impact of premorbid adjustment on functional outcomes is mediated by verbal memory and symptom remission. More broadly, our objective was to examine how each factor was related to the others and predicted functioning on its own and within a mediation model.
Mediational influences
The effect of premorbid adjustment on functional outcomes was influenced by baseline verbal memory and the maximum number of months in continuous negative symptom remission over 1 and 2 years. This is consistent with previous research showing a relationship between premorbid adjustment and verbal memory (Addington and Addington, 2005), and between premorbid adjustment and symptom remission (Diaz et al., 2013; Lambert et al., 2010), especially negative symptom remission (Addington and Addington, 2005; Chang et al., 2013; Norman et al., 2014). The impact of premorbid adjustment on functional outcomes through baseline verbal memory and positive symptom remission was significant over the first year, but not the second. Unlike months in consecutive positive symptom remission, the number of months in consecutive negative symptom remission was strongly related to functional outcomes at over 2 years. This is consistent with studies showing that sustained improvement in negative symptoms is more likely to enhance functioning than sustained improvement in positive symptoms (Cassidy et al., 2010a; Jordan et al., 2014; Rabinowitz et al., 2012).
Premorbid adjustment impacted functional outcomes through its influence on negative symptom remission over the first and second year, independent of the impact of verbal memory on functioning. This furthers our prior finding that negative symptom remission was a stronger predictor of functioning than verbal memory (Jordan et al., 2014).
The impact of premorbid adjustment on functional outcomes was mediated by verbal memory, independent of months in positive symptom remission, but only over Year 1. This implies that the influence that verbal memory has on functional outcomes may reduce over the course of treatment, as other factors like symptom remission become stronger mediators of the effect of premorbid adjustment on functioning.
Premorbid adjustment impacted functioning over 2 years, more through its influence on remission over the first year than over the second year. This supports the idea that early course may be a strong prognostic predictor of later outcomes in psychosis (Brewer et al., 2005; Steger et al., 2012; Verdoux et al., 2002).
Independent influences
Verbal memory was most influenced by premorbid adjustment. Persons with FEP with better premorbid adjustment may have stronger verbal memory skills at entry into treatment. Alternatively, it could be argued that individuals with better verbal learning early in life may have more easily achieved better premorbid milestones. Longitudinal studies of verbal memory and social and educational adjustment before the onset of psychosis are needed to better tease out their inter-relations.
Female sex was an additional consistent predictor of verbal memory in each model, in line with trends showing that females have recently surpassed males with respect to educational achievement in Canada (Turcotte, 2011). DUP may have been important in predicting verbal memory because a longer DUP may negatively impact brain structures important for cognition (Malla et al., 2011).
Verbal memory most consistently contributed to longer periods of remission, especially from positive symptoms, as in other studies (Bodnar et al., 2008). Verbal memory may be a marker of clinical outcomes (Benoit et al., 2014; Bodnar et al., 2008). Verbal memory skills may also help individuals interpret positive symptoms more accurately, contributing to earlier remission from such symptoms.
In keeping with prior findings (Lambert et al., 2010), better premorbid adjustment independently positively impacted symptom remission, except over Year 1. Better medication adherence was associated with positive symptom remission over Year 1. In contrast, poor medication adherence was associated with longer periods of negative symptom remission over the 2-year course. Having fewer negative symptoms over a sustained period may enable participants to exercise the will to not take medications. This extends to 2 years an effect that we have found over 6 months in our previous work (Steger et al., 2012).
An older age of onset of psychosis was also found to predict months in positive symptom remission over the first year, but not the second. Furthermore, age of onset was not related to negative symptom remission over 1 or 2 years. This finding is consistent with results from our previous research that those with an onset in adulthood (compared to onset in adolescence) were more likely to attain early positive symptom remission (Veru et al., 2016).
Finally, remission was the most consistent predictor of functional outcomes, and premorbid adjustment primarily contributed to functioning through negative symptom remission. Previous research highlights the stronger contribution that negative symptoms make to functioning than cognition does (Jordan et al., 2014; Milev et al., 2005; Norman et al., 1999).
Indeed, individuals may still function despite positive symptoms through good coping skills but the same may not hold for negative symptoms. Furthermore, verbal memory impacted functioning 1 and 2 years after treatment, through its influence on remission, especially from negative symptoms. This indicates a synergistic association between negative symptoms and verbal memory, owing perhaps to common neural substrates (Harvey et al., 2006).
It may be often more difficult to find or resume work than it is to resume or continue school after the onset of psychosis. Therefore, younger participants being likelier to be in school, had better functional outcomes than older participants whose employment trajectories the onset of psychosis may have disrupted. By the second year, however, the older participants seemed to have been able to initiate or resume employment at similar rates as the ones at which younger participants resume school. This may explain why the effect of age of onset on functioning did not persist over the second year. Those who had a substance abuse and/or dependence diagnosis at baseline had poorer functional outcomes at the end of the first year, suggesting that abusing substances had a negative impact on one’s ability to engage in social or educational/occupational roles (Menezes et al., 2009).
Limitations
Although premorbid adjustment difficulties and verbal memory deficits begin much earlier, we only measured them upon the commencement of treatment. This is noteworthy because our choice of analytic models emphasizes the sequencing of predictors. Given this, caution must be exercised before assuming causality from the mediation models presented in our paper. In addition, some of our models may have suffered from reduced statistical power, especially the analysis of functional outcomes at 2 years owing to sample attrition. We did not simultaneously determine the relative contributions of negative and positive symptom remission within one model. Including both paths in one model could not be accomplished with the statistical software used in this paper. Future studies should explore more such complex mediation models with larger sample sizes.
A further limitation was that there may be an overlap between measures of negative symptoms and functioning. Finally, we relied on the last observation carried forward technique to carry forward up to 6 months of missing negative symptom remission data in the 2-year analysis, which may have compromised our results pertaining to the role of negative symptom remission.
Strengths
A well-characterized, catchment area-based sample and nearly monthly assessments make our results more reliable and generalizable. We also ordered the analyzed variables to accurately reflect the time when they were measured. In conclusion, our paper makes a useful contribution to the literature by using novel statistical methods to yield better insights into possible pathways by which premorbid adjustment impacts functional outcomes over 1 and 2 years in individuals with first-episode psychosis.
Footnotes
Acknowledgements
We thank Megan Pope and Kayleigh Munn for help with editing this manuscript.
Declaration of Conflicting Interests
G.J. has received funds to support his graduate studies from the Department of Psychiatry at McGill University, Fonds de recherche du Québec-Santé and the Canadian Institutes of Health Research. F.V. has received funding from Fonds de recherche du Québec-Santé. M.L. has received funding from the Sackler Foundation, The James McGill Professorship and Fonds de recherche du Québec-Santé. R.J. has received funds from Fonds de recherche du Québec-Santé and the Canadian Institutes of Health Research. He sits on the advisory boards and speakers’ bureaus of Pfizer Canada and Janssen Ortho Canada; he has received grant funding from them and from AstraZeneca. He has received honoraria from Janssen Ortho Canada for CME presentations and royalties for Henry Stewart talks. A.M. has received funds from Fonds de recherche du Québec-Santé, National Institutes of Health Research and the Canadian Institutes of Health Research. He is also funded through the Canada Research Chair Program and has received research funding, unrelated to this study, from BMS, Pfizer, Otsuka and Lundbeck as well as honoraria related to CME lectures and advisory board participation from BMS, Otsuka, Sunnovian, Lundbeck and Pfizer. S.N.I. is funded by Fonds de recherche du Québec-Santé and the Canadian Institutes of Health Research.
Funding
The work was funded by operating grants from the Canadian Institutes of Health Research under Grant #68961.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.