
Abstract
Objective:
To determine whether a population-delivered parenting programme assists in preventing internalising problems at school entry for preschool children at-risk with temperamental inhibition.
Methods:
Design: a randomised controlled trial was used. Setting: the setting was 307 preschool services across eight socioeconomically diverse government areas in Melbourne, Australia. Participants: a total of 545 parents of inhibited 4-year-old children: 498 retained at 1-year follow up. Early intervention: Cool Little Kids parenting group programme was implemented. Primary outcomes: the primary outcomes were child DSM-IV anxiety disorders (assessor blind) and internalising problems. Secondary outcomes: the secondary outcomes were parenting practices and parent mental health.
Results:
At 1-year follow up (mean (standard deviation) age = 5.8 (0.4) years), there was little difference in anxiety disorders between the intervention and control arms (44.2% vs 50.2%; adjusted odds ratio = 0.86, 95% confidence interval = [0.60, 1.25], p = 0.427). Internalising problems were reduced in the intervention arm (Strengths and Difficulties Questionnaire: abnormal – 24.2% vs 33.0%; adjusted odds ratio = 0.56, 95% confidence interval = [0.35, 0.89], p = 0.014; symptoms – mean (standard deviation) = 2.5 (2.0) vs 2.9 (2.2); adjusted mean difference = –0.47, 95% confidence interval = [–0.81, –0.13], p = 0.006). Parents’ participation in the intervention was modest (29.4% attended most groups, 20.5% used skills most of the time during the year). A priori interaction tests suggested that for children with anxious parents, the intervention reduced anxiety disorders and internalising symptoms after 1 year.
Conclusion:
Offering Cool Little Kids across the population for inhibited preschoolers does not impact population outcomes after 1 year. Effects may be emerging for inhibited children at highest risk with parent anxiety. Trial outcomes will continue into mid-childhood.
Keywords
Public health advocates point to internalising problems as a leading cause of global burden of disease (Mathers and Loncar, 2006; www.who.int/mediacentre/factsheets/fs369/en/). In childhood, internalising (anxious/depressive) problems are common affecting 10–20% at school age (Carter et al., 2010; Lawrence et al., 2015). Internalising problems can develop early in childhood (Bayer et al., 2008, 2010) and persist into adolescence and adulthood (Asendorpf et al., 2008; Bosquet and Egeland, 2006). Internalising problems impact children’s functioning, with effects on peer relationships, school engagement, adult employment and early mortality (Asendorpf et al., 2008; Duchesne et al., 2008; Jokela et al., 2009).
Temperamentally inhibited young children are at risk of developing internalising problems (Rapee et al., 2009). An inhibited temperamental style is manifested as a tendency to withdraw from unfamiliar people, objects or situations (Claus and Blackford, 2012; Muris et al., 2011). A child’s inhibited temperament has been shown to elicit overprotective and controlling parenting (Murray et al., 2009; Rubin et al., 1999), a pattern that can contribute to development of internalising problems (Bayer et al., 2006b; Coplan et al., 2008; Rapee et al., 2009). Such parenting is a potentially modifiable risk that could have most impact during early childhood development.
Preventing internalising problems from early childhood affords several potential advantages. The early years constitute a window to maximise parental involvement when there is brain neuroplasticity and coping skills can develop before anxiety interferes with children’s transition to school (Hirshfeld-Becker and Biederman, 2002). Broader evidence also supports the cost-effectiveness of early intervention (Heckman, 2001). Nevertheless, application of early childhood prevention for internalising problems is still in relative infancy (Bayer et al., 2009).
Bayer et al.’s (2009) systematic review of randomised trials of early interventions for child social, emotional and behavioural outcomes identified Cool Little Kids as the only preschool programme to successfully reduce anxiety disorders. In the first of two efficacy randomised trials, Rapee et al. (2005, 2010) recruited 146 temperamentally inhibited 4-year-old children measured by parent questionnaire and laboratory observation. Intervention parents received this six-session parenting group programme at a university clinic delivered by clinical psychologists. By follow up, significantly fewer anxiety diagnoses were detected among intervention than control children at age 5 years (50% vs 64%) and then 7 years (40% vs 69%). At 11-year follow up, adolescent girls in the intervention arm continued to have fewer internalising diagnoses, anxiety symptoms and life interference (Rapee, 2013). The indicated prevention was found to be cost-effective (Mihalopoulos et al., 2011). The second efficacy trial involved 71 inhibited preschoolers whose parents also had internalising problems (Kennedy et al., 2009). This also resulted in fewer anxiety disorders in intervention than control children by 6-month follow up (53% vs 93%).
Here, we report the first ‘translational’ trial with population implementation of Cool Little Kids for inhibited preschool children (Bayer et al., 2011). The translational design aspects were a brief parent-report screening tool for child inhibition offered universally across the population via preschool services in the year before school, followed by an invitation to attend the Cool Little Kids parenting group programme to parents of all inhibited children at venues in their local community setting. The prior efficacy trials precluded population conclusions by their sample bias (university location and self-selection by advertisement) and the labour-intensive laboratory observation methods used for selection. The challenge was to determine ‘real world’ effectiveness across a population. We aimed to determine whether systematically screening preschoolers for temperamental inhibition and offering this parenting programme in the community could reduce child internalising problems before school entry. We hypothesised that families who were offered the Cool Little Kids programme would report fewer child anxiety disorders and internalising problems (primary outcome), along with more positive parenting interactions and parent well-being 1-year later.
Methods
Setting and participants
The trial ran in metropolitan Melbourne (population = 4 million), Victoria, Australia (ISRCTN30996662; www.isrctn.com/ISRCTN30996662). Melbourne’s 31 local government areas were ranked by census-derived socioeconomic indexes of relative disadvantage (Australian Bureau of Statistics, 2006) and 8 areas were selected to provide broad social circumstance. All preschool services offering a government-funded programme for 4-year-old children in these districts were invited to participate. As described elsewhere (Beatson et al., 2014), 307 participating preschools (78% uptake) distributed a screening questionnaire to all parents of children enrolled in their year before school in 2011 and 2012 (17,661 enrolled). The research team received 6346 completed screening questionnaires from parents (36% response) and posted all a letter of their child’s inhibition status and trial eligibility. Parents with an inhibited child were also telephoned to explain the trial and mailed the baseline questionnaire with written informed consent (Ethics in Human Research Committee of the Royal Children’s Hospital Melbourne, 30105A; La Trobe University Human Ethics Committee, HEDC13-022). Parents with insufficient English to complete the questionnaire were excluded, along with children with major health or developmental problems who were considered unlikely to benefit from the intervention. Figure 1 presents the participants’ flowchart.
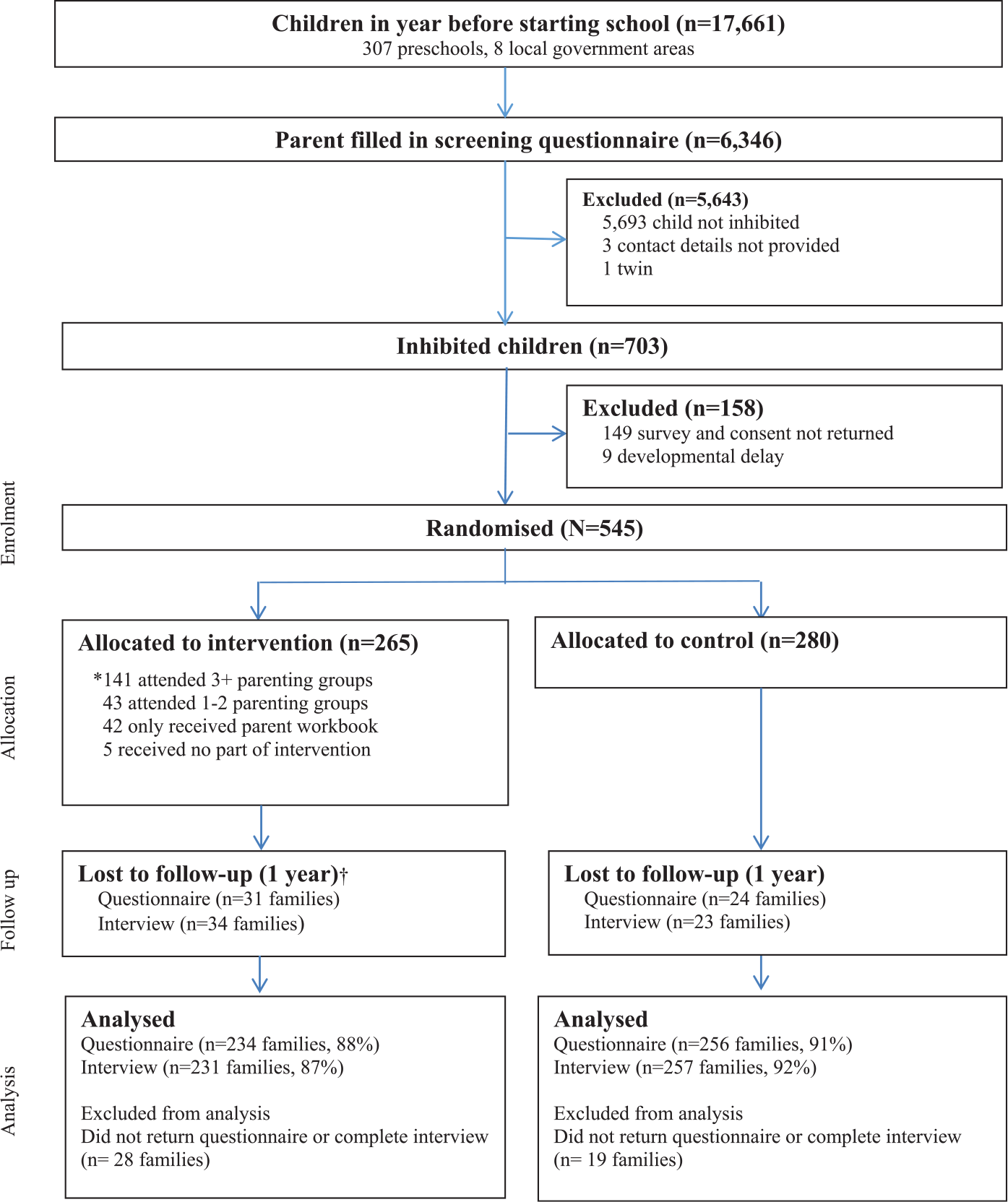
Flow chart of participants.
Targeted intervention
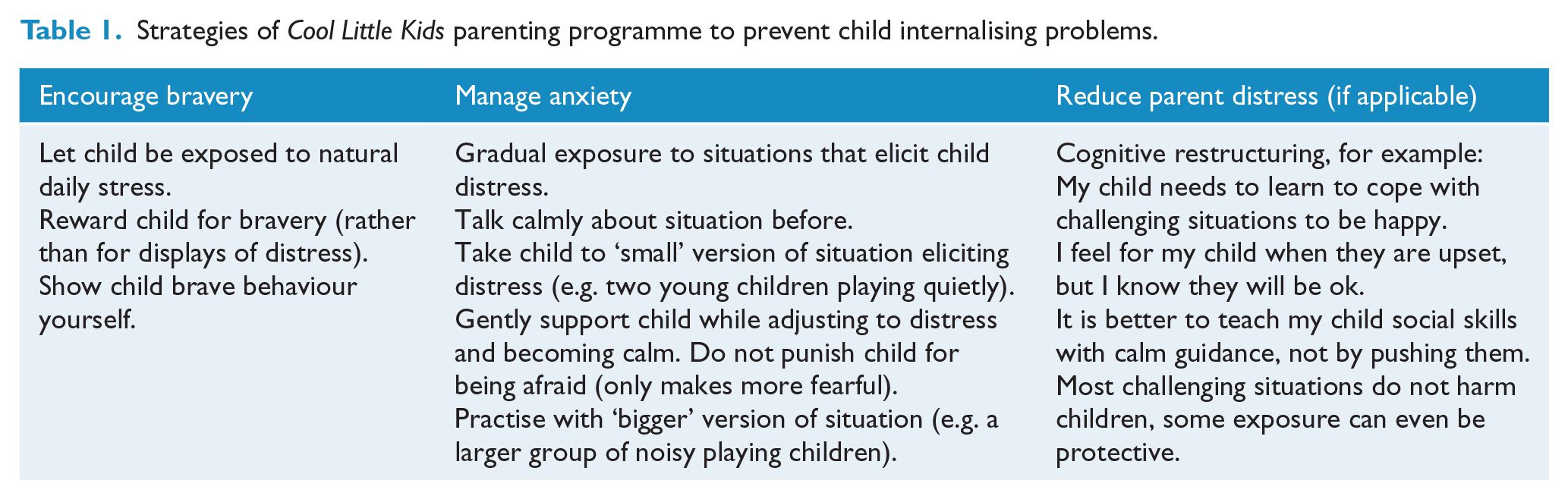
In the trial, Cool Little Kids intervention was six 90-minute manualised 1 parenting group sessions. As described previously (Bayer et al., 2011), the parenting groups provided information about the nature of child anxiety and principles of anxiety management, detailed instruction in exposing young children to specific triggers for emotional distress, and methods for parents to reduce overprotective responses and manage their own worries. Table 1 presents a summary of the strategies to prevent child internalising problems. The first two groups were delivered a week apart to ensure comprehension of materials, discuss motivation and commence implementing new skills. The following three sessions were delivered fortnightly to allow parents time to practise at home with their child (encountering challenges and implementing strategies). The final session was delivered a month after the fifth session, to review progress and plan ahead for likely future challenges as children grow. Groups were delivered at participating preschools in the local community by trained clinical psychologists and postgraduate clinical psychology interns. 2 After-hours timing facilitated attendance by working parents (7–9 pm). Group size ranged from 6 to 16 (median = 11) families. Primary and secondary caregivers were encouraged to attend, although mothers comprised 91% attending groups.
Strategies of Cool Little Kids parenting programme to prevent child internalising problems.
Usual care
Families in the control arm had ‘usual care’ access to available support services in the community. These services may provide advice on child behaviour but do not include the Cool Little Kids programme. The majority of young children with socio-emotional problems in Australia do not receive any help from professional services (Lawrence et al., 2015; Oh et al., 2015). A recent population-based study at child age 1.5–6 years found less than a quarter with externalising or internalising problems accessed general health services (10–21%; general practitioner, paediatrician and family nurse) and fewer received specialist care (0–16%; psychologist and psychiatrist) (Oh et al., 2015).
Measures
The child’s primary caregiving parent completed the trial questionnaire at points of enrolment (inhibition screening, baseline demographics, parenting and parent mental health), 6 months post-randomisation (intervention attendance and feedback) and 1 year post-randomisation (child internalising problems, parenting and parent mental health), together with structured telephone interviews (child anxiety diagnoses) 3 by assessors blind to allocation. 4
Child inhibition was measured at screening by the Australian Temperament Project’s approach/inhibition scale, a seven-item measure with sound psychometric properties (Sanson et al., 1994, 1996). Consistent with Rapee’s prior trials (Rapee et al., 2005, 2010), children scoring above 30 on this measure were inhibited and eligible for the trial. This parent-report screen mimicked what may be possible if early intervention were to be rolled out in the population. 5
Demographics at baseline included child sex and birth order, household composition, caregiver age, marital status, education, main home language, family finance and hardship (welfare card). Each family was assigned an Australian neighbourhood disadvantage score for home postcode (Australian mean (standard deviation (SD)) = 1000 (100)) (Australian Bureau of Statistics, 2011).
Parenting was measured at baseline and follow up with the Parent Behaviour Checklist (PBC; Brenner and Fox, 1998) for nurturing and harsh discipline supplemented by Bayer et al.’s (2006b, 2010) over-involved/protective subscale. The PBC yields T-scores (mean (SD) 50 (10)) derived from developmental norms with 6-month age bands. Parent mental health was measured at baseline and follow up by the Depression Anxiety Stress Scales (DASS-21; Lovibond and Lovibond, 1995).
The primary outcome (for power analysis) was child anxiety diagnoses measured by the Anxiety Disorders Interview Schedule for DSM-IV, Child Version, Parent Interview Schedule (ADIS-CP-IV; Silverman and Albano, 1996). Assessments for separation anxiety disorder, specific phobia, social phobia and generalised anxiety disorder were covered. Child internalising (anxious/depressive) measures included the Strengths and Difficulties Questionnaire’s (SDQ) emotional symptoms subscale (Goodman, 2001) that is widely used internationally, as well as the newer Children’s Moods, Fears and Worries Questionnaire (CMFWQ; Bayer et al., 2006a). The SDQ-emotional comprises five items and has demonstrated acceptable convergent validity with diagnostic interviews and other child behaviour questionnaires (Hawes and Dadds, 2004). The SDQ subscale cut-points identify the highest 10% of the population as ‘abnormal’ (http://www.sdqinfo.com/py/sdqinfo/c0.py). The CMFWQ comprises 34 parent-report items and has demonstrated convergent validity with internalising scales of the Child Behaviour Checklist (CBCL; Achenbach and Rescorla, 2000) and Behaviour Assessment System for Children – 2nd Edition (BASC-2; Reynolds and Kamphaus, 2004) (Andrijic et al., 2013).
Randomisation
After recruitment and trial consent, a concealed web-based computer-generated randomisation process was implemented to determine trial arm status for each child. Block randomisation was used with randomly permuted block sizes in a non-systematic sequence. Allocation was stratified by preschool. Researchers in the Clinical Epidemiology and Biostatistics Unit at the Murdoch Childrens Research Institute (otherwise unconnected to the study) conducted randomisation and allocation. Diagnostic outcome assessors were blind to allocation status via password-protected access to randomisation sections of the study database. 6
Sample size
To detect a 14% reduction in anxiety disorders between the intervention and the control arms (as per Rapee et al. [2005] efficacy trial), with 80% power at two-sided significance of 0.05 and allowing for 15% drop-out, the population study required a sample size of 500 inhibited children.
Analyses
Trial arms were analysed as randomised, using the intention to treat principle with participants analysed in the arm to which they were randomised. One-year post-baseline is the first randomised trial outcome point (post-intervention collected only parent attendance and acceptability). Continuous, count and binary outcomes were analysed using unadjusted and adjusted Generalised Estimating Equations (GEEs) assuming Gaussian, Poisson and binomial distributed outcomes, respectively, and with sandwich estimates of standard error. The GEEs allowed for correlation within preschool which was chosen as the cluster variable. As per protocol (Bayer et al., 2011), potential baseline confounders were adjusted for including child sex, mother’s mental health, education and socioeconomic disadvantage. 7 Means and SDs or percentages are presented for each trial arm, along with the mean difference between arms or odds ratio, 95% confidence interval (CI) and p-value. We explored a priori interactions for baseline parent mental health and child comorbid externalising problems with the intervention on the child internalising outcomes. We also tested for intervention dose effect. R version 3.0.2 (R Core Team, 2013) and package geepack (Højsgaard et al., 2006) were used for the analysis. Missing data were not an issue. When looking at participants retained at 1-year follow up, less than 2% of data were missing across outcome and baseline variables used in the adjusted analyses.
Results
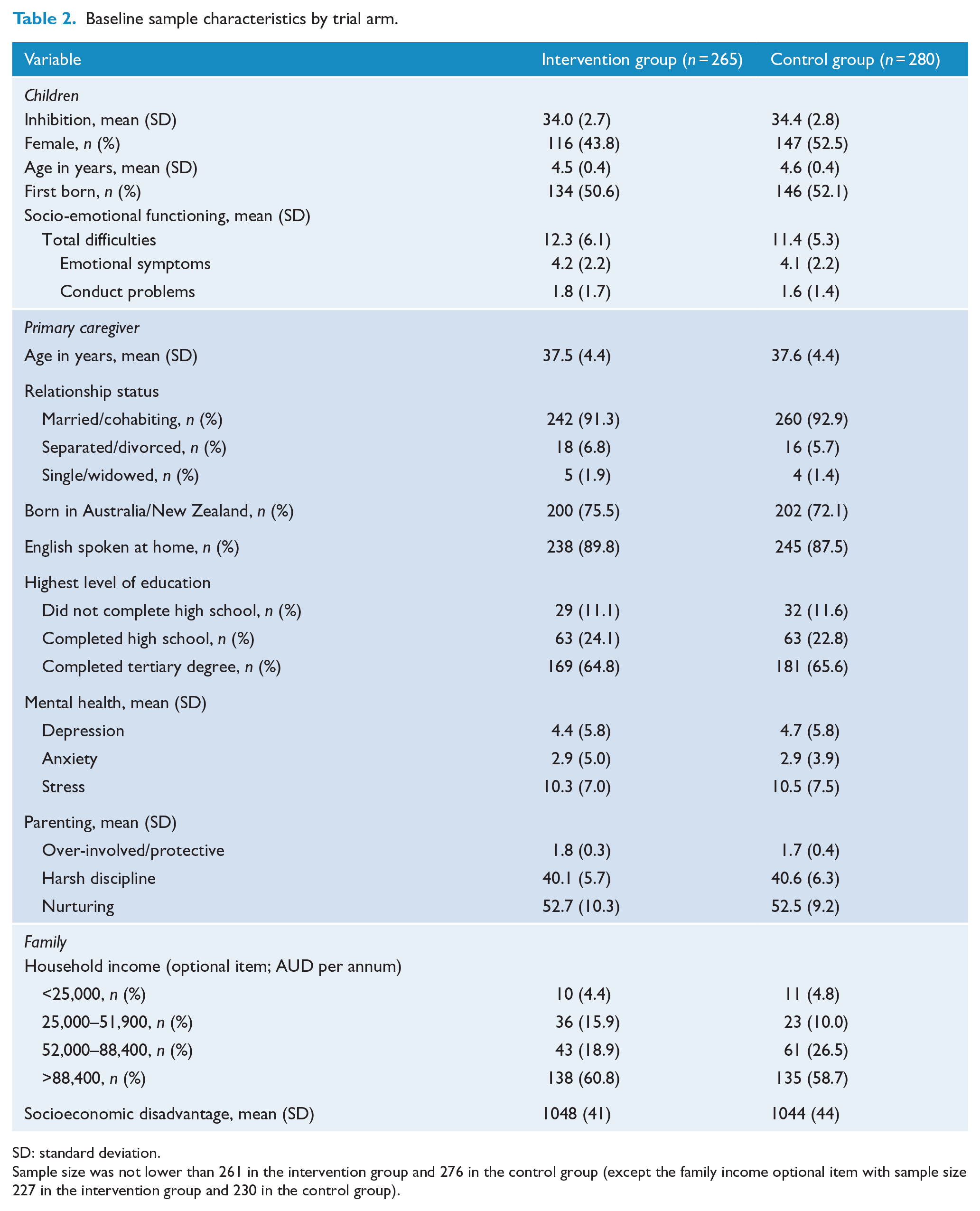
Of 703 children who were inhibited on the preschool screening questionnaire, parents of 545 (78%) completed the baseline questionnaire and were recruited to the trial (Figure 1): 265 in the intervention and 280 in the control arms. Table 2 describes the sample characteristics, which were well balanced between trial arms. At 1-year follow up (child mean (SD) age 5.8 (0.4) years), 234 (88%) intervention and 256 (91%) control families returned questionnaires, while 231 (87%) intervention and 257 (92%) control families completed their telephone interview. There was no association between loss to follow up and baseline child internalising symptoms.
Baseline sample characteristics by trial arm.
SD: standard deviation.
Sample size was not lower than 261 in the intervention group and 276 in the control group (except the family income optional item with sample size 227 in the intervention group and 230 in the control group).
Child anxiety diagnoses and internalising problems
At 1-year follow up (Table 3), there was little difference in anxiety disorders in the intervention versus control arms across the population (44.2% vs 50.2%; adjusted odd ratio = 0.9; 95% CI = [0.6, 1.2], p = 0.427). There was an indication that child internalising problems on the SDQ showed improvement in the intervention versus control arm. Proportionally less children scored in the abnormal range (24.2% vs 33.0%; adjusted odds ratio = 0.6; 95% CI = [0.4, 0.9], p = 0.014), along with a lower mean (SD) score (2.5 (2.0) vs 2.9 (2.2), adjusted mean difference = –0.5; 95% CI = [–0.8, –0.1], p = 0.006). A linear mixed-effects (LME) analysis of SDQ internalising symptoms revealed a significantly greater reduction in the intervention arm after 1 year (0.6 greater reduction, 95% CI = [0.2, 0.6], p = 0.004). A priori interaction tests suggested that for inhibited children with parents higher in anxiety (at baseline), the intervention, compared to the control group, reduced child internalising symptoms and anxiety disorders (Table 4; Figure 2A and B – note that due to the discrete nature of both variables, a small value has been added to each point to avoid overlapping in B). These interactions were due to parents with severe anxiety. The three parents with severe anxiety in the control group all had children with separation anxiety after 1 year. Conversely, the six parents with severe anxiety in the intervention group all had children without separation anxiety after 1 year, representing a significant difference (Fisher’s exact test: p = 0.012). The small number of parents with severe anxiety warrants further investigation into this association. Child externalising problems (comorbidity) did not moderate intervention outcomes.
One-year follow-up outcomes by prevention trial arm status.
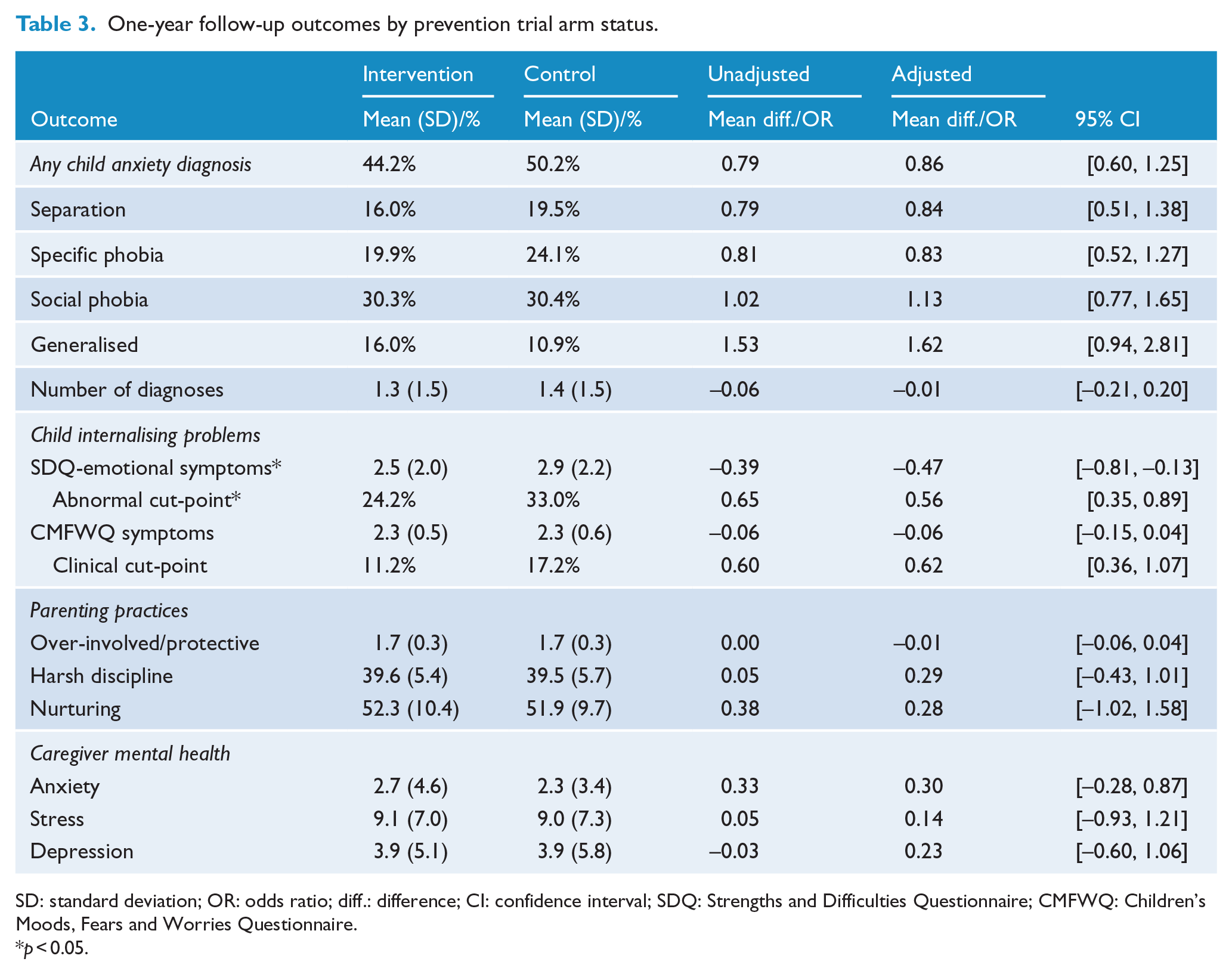
SD: standard deviation; OR: odds ratio; diff.: difference; CI: confidence interval; SDQ: Strengths and Difficulties Questionnaire; CMFWQ: Children’s Moods, Fears and Worries Questionnaire.
p < 0.05.
Higher parent anxiety (baseline) moderates prevention effect on child internalising outcome: GEE regression coefficients, by group, for parent anxiety predicting child outcomes.
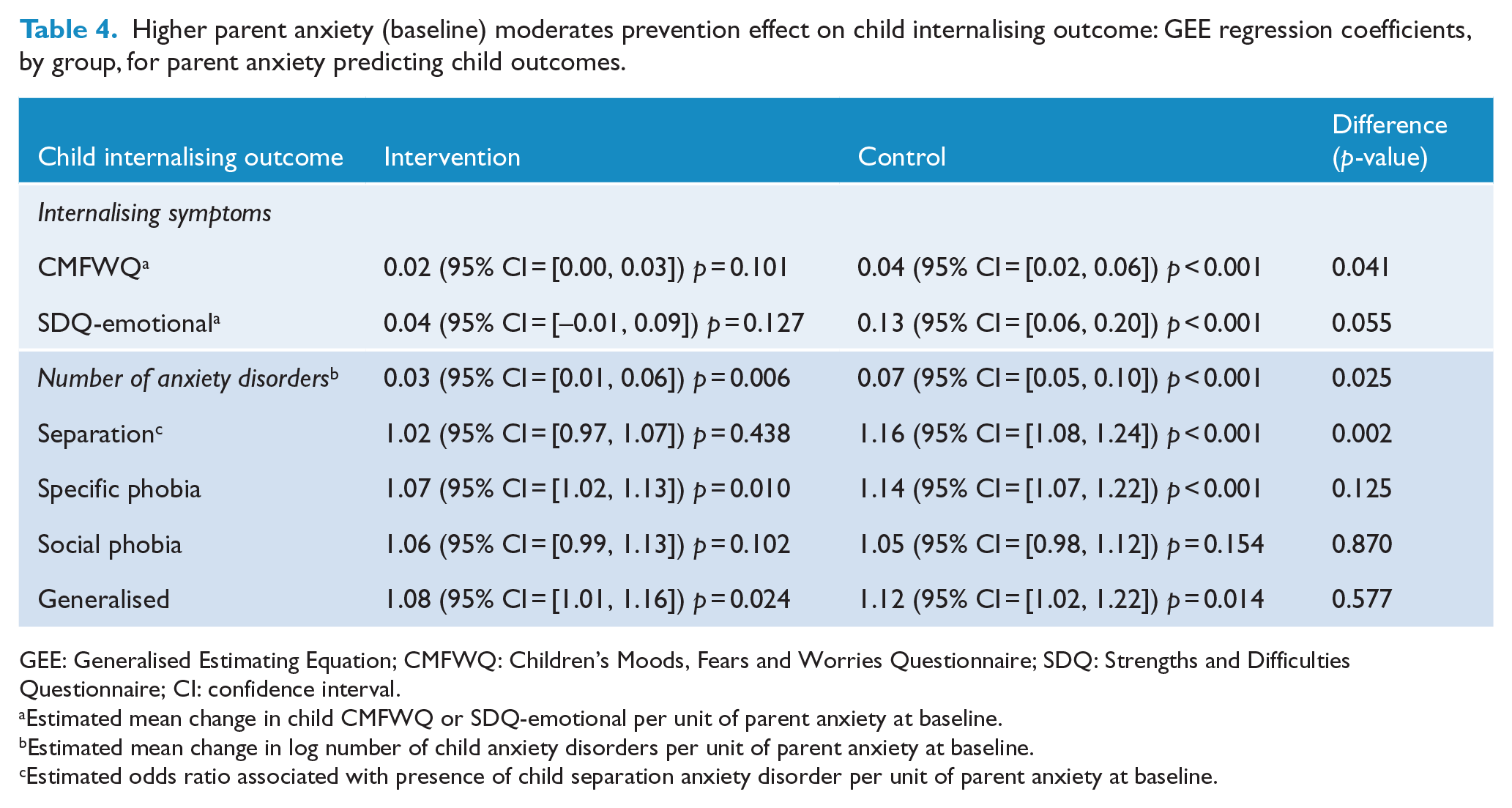
GEE: Generalised Estimating Equation; CMFWQ: Children’s Moods, Fears and Worries Questionnaire; SDQ: Strengths and Difficulties Questionnaire; CI: confidence interval.
Estimated mean change in child CMFWQ or SDQ-emotional per unit of parent anxiety at baseline.
Estimated mean change in log number of child anxiety disorders per unit of parent anxiety at baseline.
Estimated odds ratio associated with presence of child separation anxiety disorder per unit of parent anxiety at baseline.
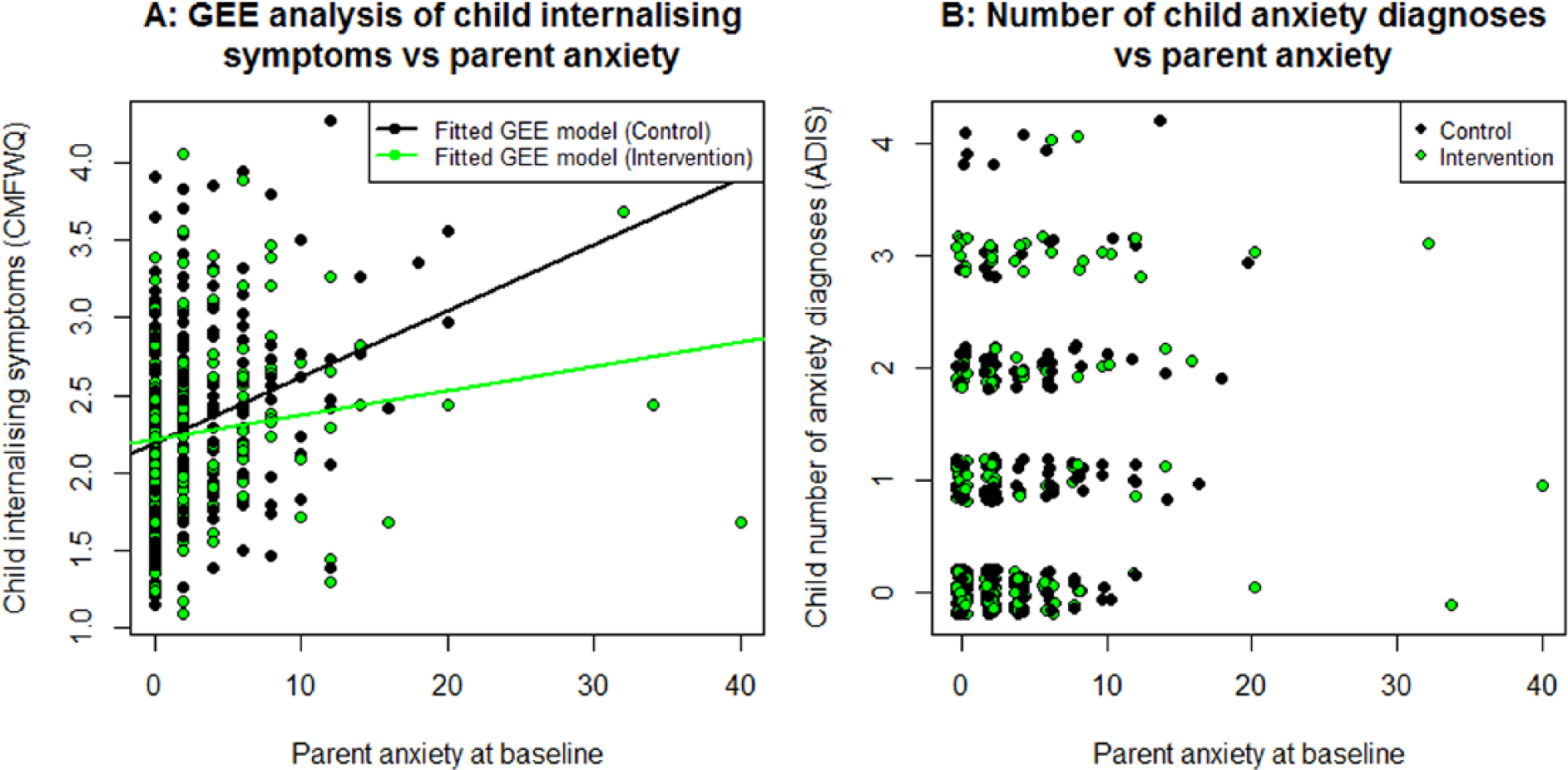
Parent anxiety at baseline moderating child internalising outcomes. For (B), due to the discrete nature of both variables, a small value has been added to each point to avoid overlapping.
Parenting and parent mental health
At 1-year follow up, over-involved/protective, harsh discipline and nurturing parenting were similar across the population in the intervention and control arms. Likewise, across the population maternal depression, anxiety and stress were similar at follow up in the intervention and control arms (Table 3).
Intervention implementation
Content checklists showed that the clinicians delivered all six group sessions of this programme in the community. The research team posted the Cool Little Kids parent workbooks to any intervention families who missed their first group session. In the intervention arm, 85% of parents reported receiving some intervention materials (Table 5). However, intervention parents’ level of attendance varied greatly across the population: only 34% attended most of the programme (5–6 groups) and 27% attended about half the programme (3–4 groups), whereas 19% attended only the introduction (1–2 groups) and 18% received only the parenting workbook (no group sessions). The main reasons offered by parents for missing pre-scheduled group sessions included illness (51 families), lack of childcare (33 families) and too busy (25 families). Parent anxiety did not predict the number of parenting groups attended (dose, p = 0.900). Child internalising outcomes were not predicted by dose (all p > 0.38) or by couple/individual attendance (all p > 0.46). In the year that followed the intervention, relatively few parents continued regular practise of their new Cool Little Kids skills with their inhibited child (Table 5). Only 20% of parents reported implementing their new skills the majority of the time, in contrast to 53% who rarely implemented the new skills.
Parent uptake of preventive intervention across the population.
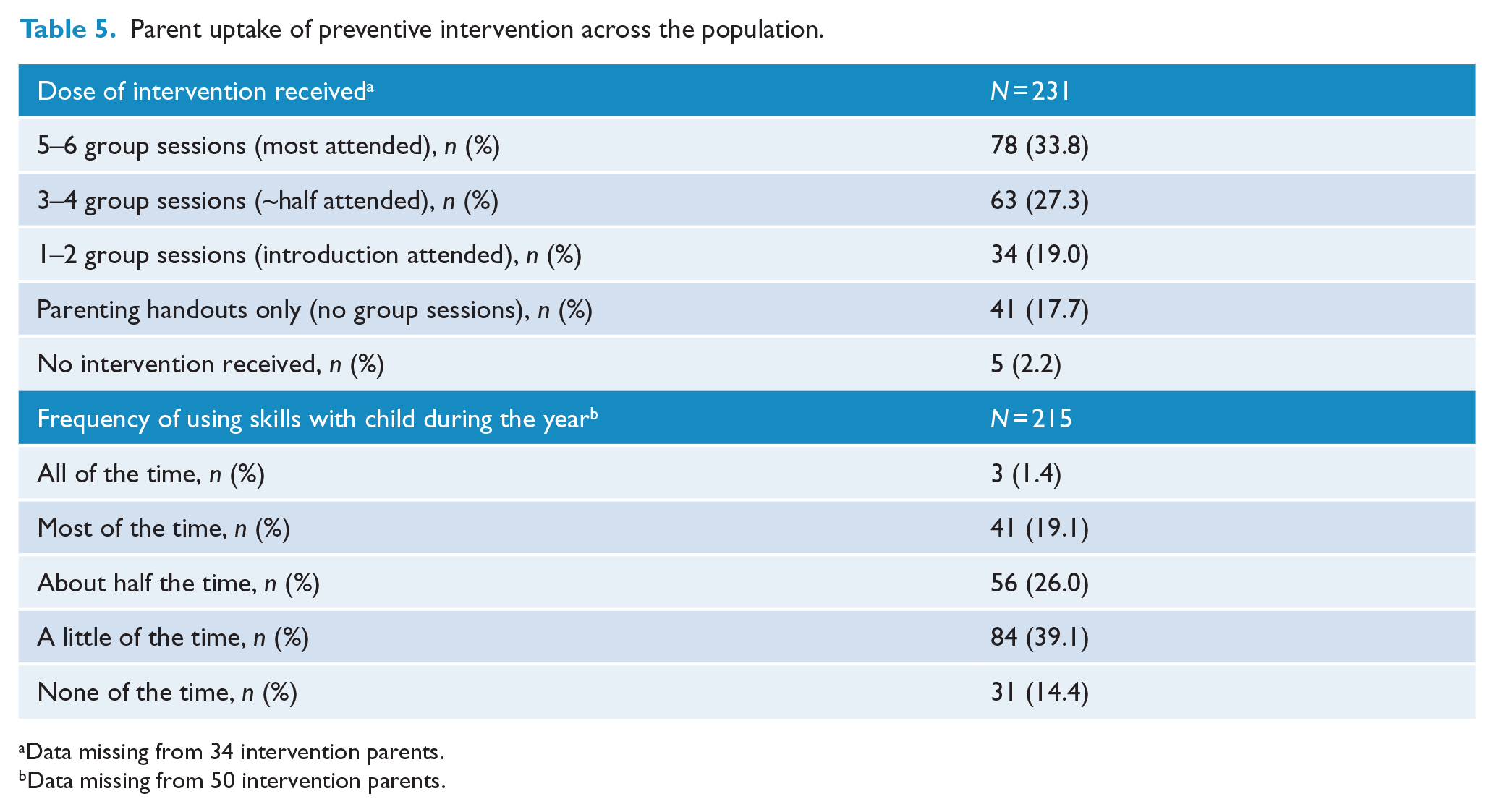
Data missing from 34 intervention parents.
Data missing from 50 intervention parents.
Discussion
This translational trial of the Cool Little Kids parenting programme for shy/inhibited preschool children found no widespread impact on child anxiety disorders, parenting practices or parent mental health when assessed across the population after 1 year. There was an indication of fewer internalising problems across the population on the SDQ. There was also an indication of fewer anxiety disorders for children at highest risk (with inhibition and parent anxiety).
Parents have provided feedback that they find Cool Little Kids helpful in understanding and managing their inhibited child’s anxiety and emotional distress (Beatson et al., 2014). Nevertheless, most engaged in a small amount of the preventive intervention when offered at no direct cost in the local community (only 34% attended 5–6 groups) and few practised the skills with their child regularly after the programme. In contrast, in the efficacy research, most parents attended most of the programme (73% attended 5–6 groups) (Rapee et al., 2010).
Strengths
The translational trial had the following strengths. First, 78% of eligible parents consenting to participate represent good uptake for population trials (Hiscock et al., 2008; Rapee et al., 2005). Non-participants’ social disadvantage scores were only marginally lower than participants’ (on parent education and welfare card recipient), indicating that findings can be generalised to a wide socioeconomic spectrum (although perhaps not the lowest end). Second, psychometric and developmentally sensitive child mental health outcome measures were included with both symptom-scales and assessor-blind diagnoses. Third, 90% of recruited families were retained at 1-year follow up, supporting validity of the findings and acceptability of a population approach.
Limitations
This translational trial had single source (primary caregivers) rather than multisource assessment. Primary caregivers are widely recognised to be the most informed source on young children’s socio-emotional functioning (Glascoe, 2005). The results could nevertheless be open to some bias as parents cannot be blinded to trial arm in parenting programmes. Multisource measures could possibly tap some more child functioning and family environment aspects (i.e. clinician observation and teacher report). Direct observation, however, is impractical in population studies. A second potential limitation is that disadvantaged families may preferentially not participate in studies. The screening questionnaires were universally distributed by preschools to all children in their year before school, but only 36% were returned by parents to the study team. The response rate was similar to that typically achieved by postal surveys in research (McLean et al., 2014; Rapee et al., 2005), and socioeconomically disadvantaged families were included in the trial’s sample. Nevertheless, two-thirds of parents had tertiary education and this limited the potential to examine intervention impact among the more socially disadvantaged. Third, a lack of diagnostic assessment at baseline means that some included children may have met criteria for anxiety disorders, reducing the extent to which the trial reflects pure prevention. However, inclusion of children based on inhibition questionnaires reflects the most likely method for use in community delivery.
Implications
This is the first trial with shy/inhibited preschoolers identified via a population screen to assess impacts of offering prevention on child internalising problems at school entry. After 1 year, only a few effects on child internalising problems were detected, perhaps primarily for inhibited children at highest risk due to parent anxiety. The earlier efficacy research with Cool Little Kids included highly motivated parents by research design. Parents in prior university-based trials committed to intensive direct observation playroom assessments (pre- and post-intervention). Motivated parents attending most of the parenting group programme achieved significant reduction in child anxiety and internalising disorders over time (Rapee, 2013; Rapee et al., 2010). In the present translational trial, child inhibition screening and the parenting groups were widely offered at no direct cost to parents and their level of engagement was much lower (36% screening uptake, 34% full parenting programme attendance and 20% implementing skills in the following year). The translational trial aimed to make it easy for all parents to participate with relatively little effort via a brief child shyness screen and nearby free parenting groups. This may result in less child need and parent motivation.
The weaker outcomes in the translational trial make sense in this context. Mian (2014) recently highlighted that ‘the greatest challenges to dissemination and establishing effectiveness of early childhood anxiety interventions for high-risk children will likely be related to parents’ interest, willingness, or ability to engage in these programs’ (p. 90). This parallels difficulties in engaging parents in programmes to prevent or manage child disruptive behaviour disorders in the real-world setting (Baker et al., 2011). This seems to be universal truth whether the child’s problems are externalising or internalising. A way forward could be to facilitate accessibility of Cool Little Kids in the community for those parents who demonstrate commitment to involvement. A financial payment may be an option to secure commitment (Heinrichs et al., 2005). Parents with a lifetime of anxiety might be particularly motivated to prevent their children from suffering in the same way. There could be a shift to indicated prevention by adding child anxiety diagnostic interviews for eligibility plus motivational interviewing in the first intervention session. Motivational interviewing that emphasises knowledge about longer term risk of inhibited temperament may increase parental motivation to seek change. After an introduction, those parents with high motivation could then commit to the full programme. A shift to indicated prevention is consistent with current practice later in childhood (Gladstone and Beardslee, 2009).
Conclusion
Parents appreciate offering Cool Little Kids across the population without direct cost to families, but on balance, this does not impact child and family outcomes at the population level after 1 year. Some effects may be emerging for children at highest risk with inhibition and parent anxiety. Prevention effects may continue to develop in the longer term and we are following trial outcomes through school entry into mid-childhood. Future dissemination work on Cool Little Kids could consider techniques to ensure that parents enrolling in the programme are highly motivated and will continue practising with their young child as they grow.
Footnotes
Acknowledgements
The authors thank the preschool services and families in the Victorian cities of Banyule, Boroondara, Frankston, Kingston, Knox, Maroondah, Whitehorse and Wyndham who took part in this research. They thank Joyce Cleary (Victorian Department of Education and Early Child Development) for her support in contacting preschool services. We also acknowledge and thank Alexandra Perry, Megan Mathers, Kate Beasley, Cassima Beechey, Timothy Grant-Taylor and Chelsea Cornell who were research assistants during the trial. Trial registration: ISRCTN30996662; ![]() .
.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article. Dr Rapee is an author of the Cool Little Kids treatment manual, but receives no royalties.
Funding
This research was supported by the Australian National Health and Medical Research Council (NHMRC) Project Grant 607302 and by the Victorian Government’s Operational Infrastructure Support Program. J.K.B. and H.H. were supported by NHMRC Population Health Capacity Building Grant 436914 and C.M. by NHMRC Capacity Building Grant 456002 and NHMRC Early Career Fellowship 1035887. J.K.B. was also part supported by the Australian Rotary Health. M.W. was supported by NHMRC Senior Research Fellowship 1046518 and Cure Kids New Zealand.