
Abstract
Objective:
Mental health problems are an international public health issue affecting a substantial proportion of youth. This study aimed to identify groups of young children exhibiting distinct internalising and externalising symptom trajectories across early childhood compared to existing norms. Linear regression then identified child, parenting and family predictors from infancy in the development of internalising and externalising behaviours at age 5 years.
Method:
This consisted of a follow-up of 5-year-old children from a longitudinal, population-based study with earlier surveys having been completed by primary caregivers when the children were aged 7, 12, 18, 24 and 36 months. Five hundred 5-year-olds (68% retention) were included from 733 children recruited at age 6–7 months from routine well-child appointments across six socio-economically diverse government areas in Victoria, Australia. Mothers then completed a further questionnaire when their children reached 5 years of age, repeating the instruments included in previous waves. The primary outcomes were the Child Behavior Checklist (CBCL), 1.5–5 internalising and externalising symptoms (T-scores in relation to norms) and behaviours (raw scores).
Results:
Across early childhood, three distinct profiles for each of the internalising and externalising symptoms (T-scores) were identified and compared to CBCL norms. Around 20% of this Australian child population exhibited consistently elevated symptoms for each problem. Regarding aetiology, longitudinally the strongest predictors of internalising behaviours at 5 years of age were harsh discipline, maternal stress, having no older siblings, single parenthood and maternal substance misuse. The strongest predictors of externalising behaviours at 5 years of age were male sex, harsh discipline and maternal stress. The predictors explained 22% of the variation in internalising behaviours and 24% of the variation in externalising behaviours at 5 years.
Conclusions:
Starting as early as the toddler period, effective population approaches to preventing mental health problems are needed. Randomised trials of preventive interventions focused on improving parenting practices and reducing maternal stress are under way.
Introduction
In childhood, mental health problems consist primarily of internalising (anxiety, depression) and externalising (aggression, oppositional defiance) problems. They pose a public health issue affecting up to a quarter of youth in Australian and international populations (Anderson, 1994; Egger and Angold, 2006; Sawyer et al., 2000) and can continue into adolescence and adulthood (Bosquet and Egeland, 2006; Kessler et al., 2005; Morgan et al., 2009; Pihlakoskia et al., 2006; Prior et al., 2001).
Epidemiological data show that half of all lifetime mental health disorders start by age 14, and even earlier for anxiety and impulse control problems which have a median age of onset of 11 years for clinical level diagnoses (Kessler et al., 2005). Negative sequelae of children’s mental health problems include peer and learning difficulties, school dropout, substance abuse, poor vocational prospects, family violence and suicide, with significant service costs to society (Bor et al., 2004; Stewart-Brown, 1998).
A detailed understanding through the early childhood years of internalising and externalising symptom trajectories compared to available norms, as well as the relative impact of specific family contextual influences, could inform prevention initiatives for mental health. Yet, to date, few population-based longitudinal studies have focused in depth on the development of child internalising and externalising symptoms, together with the impact of family context from infancy throughout early childhood (Essex et al., 2006; Gilliom and Shaw, 2004; McCarty et al., 2005; Mathiesen et al., 2009; Robinson et al., 2008). A large body of literature refers to child behavioural problems, but it is somewhat fragmented in that separate studies examine either internalising or externalising outcomes, focus on either parenting practices or broader family context as predictors, and conduct cross-sectional rather than longitudinal analyses (Ashford et al., 2008; Bayer et al., 2006; Brenner and Fox, 1998; Miner and Clarke-Stewart, 2008; Pike et al., 2006; Rapee et al., 2010).
We first published longitudinal data in 2008 on socioemotional outcomes from infancy to early preschool age (3 years) (Bayer et al., 2008) from a wider population-based prevention trial that is published elsewhere (Hiscock et al. 2008). The trial evaluated the effect of a very brief parent education program (two group sessions) on reducing toddler externalising behaviours and had no significant impact on child outcomes (Hiscock et al., 2008). At recruitment, mothers of infants attending universal well-child visits were eligible in socio-economically diverse government areas of metropolitan Melbourne, Australia (Department of Human Services, 2003). Consenting mothers were posted a questionnaire when the child was aged 7 months, and then again at 1, 1.5, 2 and 3 years of age. By the age of 3, key predictors of externalising behaviours were harsh discipline parenting and maternal stress, while predictors of internalising behaviours included small family size, parental stress and harsh discipline (Bayer et al., 2008).
We now report the outcomes through to age 5 for this population-based sample of Australian children. We first aimed to identify groups of children exhibiting distinct internalising and externalising symptom trajectories across early childhood. We hypothesised that the internalising and externalising difficulties of young Australian children [t-score symptoms of problems in relation to the norms outlined in the Child Behaviour Checklist (CBCL)] would be persistent over time. We then aimed to identify child, parenting and family predictors from infancy in the development of the internalising and externalising behaviours of 5-year-olds. We hypothesised that the internalising and externalising behaviours of 5-year-old Australian children would be predicted by family environmental experiences during their formative early childhood development years.
Methods
More detailed and extensive prevention trial methods were published previously (Hiscock et al., 2008) and are briefly included here.
Setting and participants
Eighty-five per cent of all Victorian parents attend the free universal maternal and child health (MCH) well-child visit at age 6–7 months (Department of Human Services, 2003). MCH nurses in six socio-economically diverse local government areas (LGAs) consecutively invited, over a two-month period, all mothers of infants attending this visit to take part in the study, excluding mothers with insufficient English to complete the questionnaires. Recruited participants included 733 families, representing 69% of eligible births attending the 6–7 month well-child visit in the six LGAs included in the trial (Figure 1).
Measures
Mothers completed a further questionnaire when their children reached 5 years of age, repeating the instruments included in previous waves. The primary outcomes were the Child Behavior Checklist (CBCL), 1.5–5 internalising and externalising symptoms (T-scores in relation to norms) and behaviours (raw scores) (Achenbach and Rescorla, 2000).
The following socio-demographic factors were measured once in infancy (7 months): infant gender, birth order, childcare hours per week, parents’ age, education, marital status, cultural identity, language mainly spoken at home and family income. Each family was assigned a local neighbourhood socio-economic indexes for areas (SEIFA) of relative disadvantage score by home postal code [population mean (SD) = 1000 (100)], higher scores being indicative of better socio-economic status] (Australian Bureau of Statistics, Commonwealth of Australia, 2001). Also in infancy, temperamental difficulty was measured using the Australian Temperament Project’s global rating scale (Sanson et al., 1991), while home violence, substance misuse and social isolation were measured using the Kemper and Kelleher’s (1996) health service screening questions. At 1 year of age, partner relationship satisfaction was measured using the abbreviated Dyadic Adjustment Scale (Sharpley and Rogers, 1984), while parenting conflicts were measured using the Parent Problem Checklist (Dadds and Powell, 1991). Repeated measures across time (1, 1.5, 2, 3 and 5 years) of parenting interactions were taken using the Parent Behaviour Checklist (PBC subscales: harsh discipline, nurturing, developmental expectations) (Brenner and Fox, 1998). Maternal mental health was measured repeatedly (at 7 months, then at 1.5, 2, 3 and 5 years) using the Depression Anxiety Stress Scales (DASS) (Lovibond and Lovibond, 1995).
Statistical analyses
Latent class analysis (McCutcheon, 1987; Muthén and Muthén, 2000) was applied to the children’s CBCL T-scores across waves (1.5, 2, 3 and 5 years) to identify the salient trajectories of development for each of the internalising and externalising symptoms (Aim 1). For each modality, five latent class models were fitted with increasing numbers of classes from 1 to 5 using the Mplus software, version 5.1. The likelihood ratio test was used to compare the goodness of fit between models that differ by only one class to quantify the evidence that the model with an extra class is a significantly better fit (Nylund et al., 2007). We retained the most complex model that provided interpretable class profiles, accounted for a non-trivial percentage of the population, and for which there was evidence that it provided an improvement on the simpler model with one less class. The analysis used pairwise deletion, which meant all participants who provided CBCL data for at least two waves were included in the analysis.
Consistent with our previously published aetiological analysis (Bayer et al., 2008; De Stavola et al., 2006) we fitted linear regression models to the CBCL 5-year internalising and externalising behaviours (raw scores), predicting from all potential risk variables from infancy available for each time point (Aim 2). For predictors measured at more than one time point, change scores between adjacent waves were used in the regression models in addition to the score at the first time point at which it was measured. The regression coefficients thereby quantify the cumulative associations of risk factors across waves.
To illustrate, the maternal depression regression coefficient for the score at 7 months is the expected change in the 5-year CBCL behaviour corresponding to a one unit increase at all four waves at which maternal depression is measured, and so on, until the coefficient for change between 3 and 5 years is the expected change in CBCL corresponding to a one unit increase in the risk factor at 5 years only. The risk factors for which most or all of the regression coefficients for the first score and subsequent changes show strong evidence of association are said to have consistent associations (i.e. the risk factor is predictive throughout). Participants were included in the regression analyses if they were non-missing on all predictor variables as well as outcomes. Analyses were carried out using Stata 11.2 (Stata Corporation, College Station, Texas, USA). Project approval (EHRC 28098 B) was obtained from the Ethics in Human Research Committee of the Royal Children’s Hospital, Melbourne, Australia.
Results
Population characteristics
Figure 1 shows a flow chart of eligible and consenting participants to age 5 years. Follow-up questionnaires at child age 5 years were returned by 68% (500/733) of the parents of children originally recruited in infancy. Table 1 summarises the characteristics of the complete original sample and the characteristics of the subsets of those who provided full risk factors and CBCL outcome data at each of the 1.5, 2, 3 and 5 years time points. Families across all social strata were represented (SEIFA range: 825–1140) and parents reported a broad range of education and cultures. Participants included in the analyses at child age 5 were broadly representative of the original recruited sample.
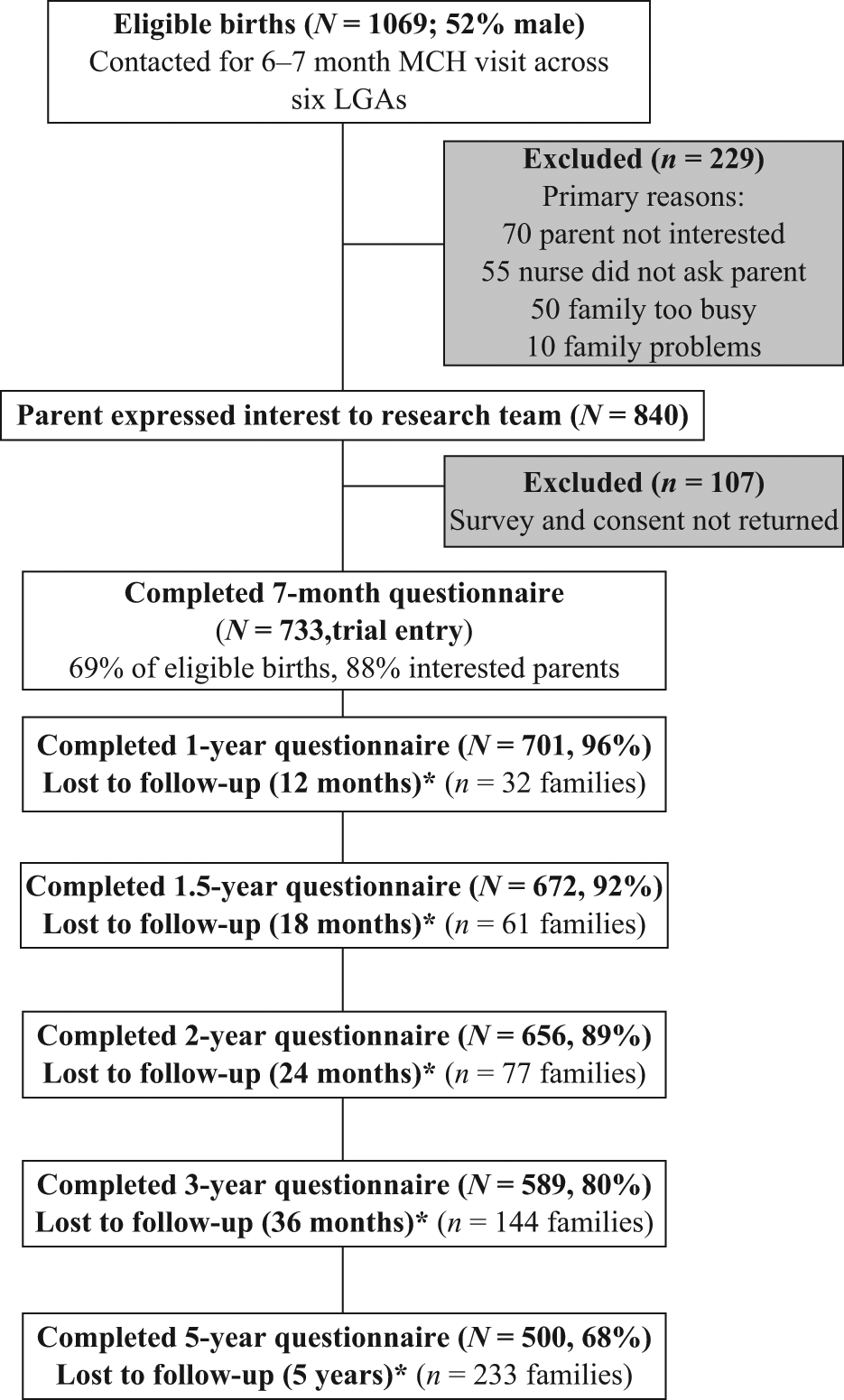
Flow chart of study participants. LGA: local government area; MCH: maternal and child health.
Sample characteristics in infancy (at approximately 7 months)
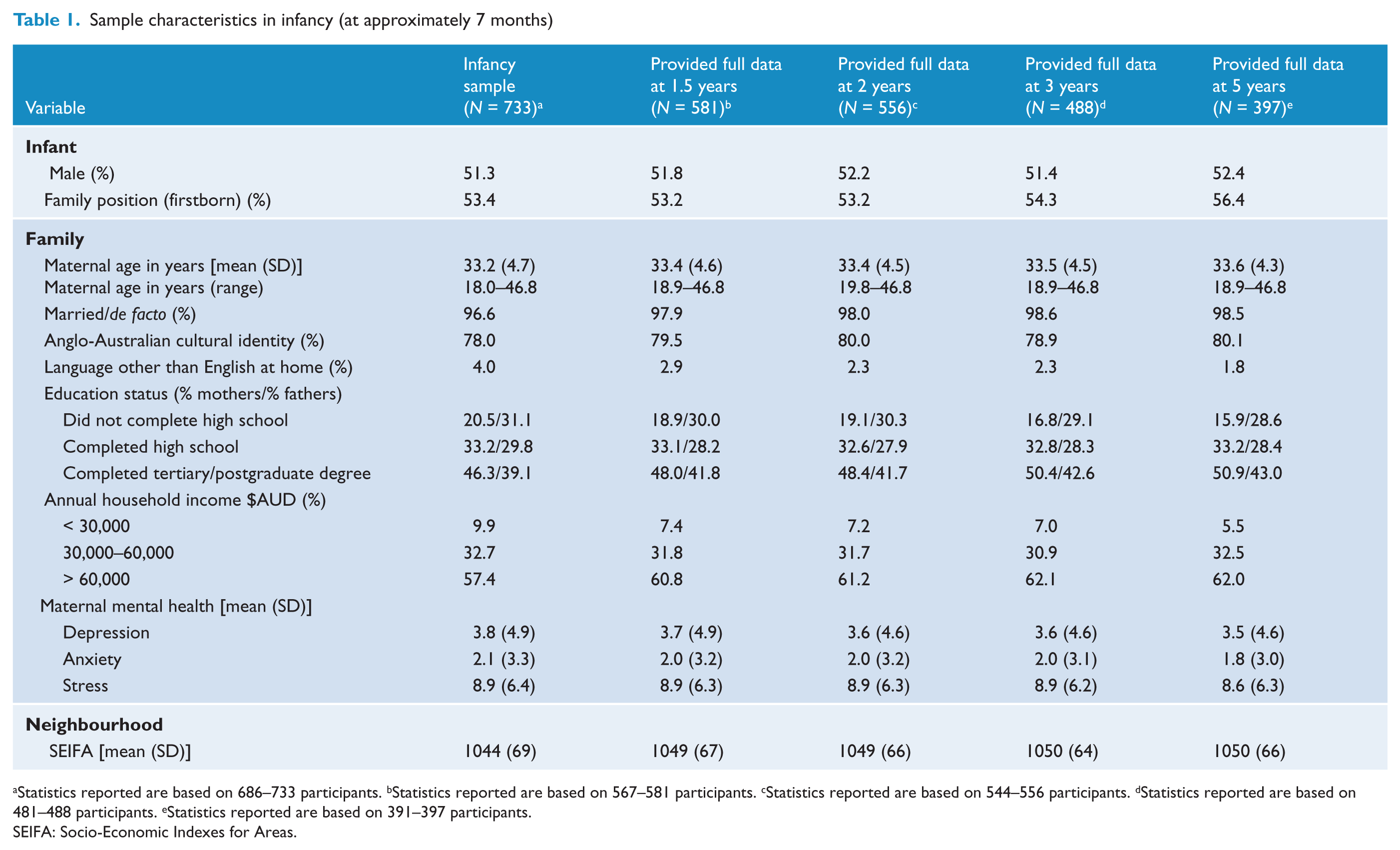
Statistics reported are based on 686–733 participants. bStatistics reported are based on 567–581 participants. cStatistics reported are based on 544–556 participants. dStatistics reported are based on 481–488 participants. eStatistics reported are based on 391–397 participants.
SEIFA: Socio-Economic Indexes for Areas.
Summary of child internalising and externalising distributions
Table 2 summarises the CBCL distributions for this sample by age and gender. The T-score distributions indicated that, in this Australian sample, children aged 5 years had fewer internalising and externalising symptoms compared to the United States norms (mean = 50, standard deviation = 10). In the Australian sample, 11.5% of males and 8.0% of females had internalising problems, while 7.3% of males and 5.5% of females had externalising problems (borderline clinical cut-off points).
Child mental health distributions at age 5 years
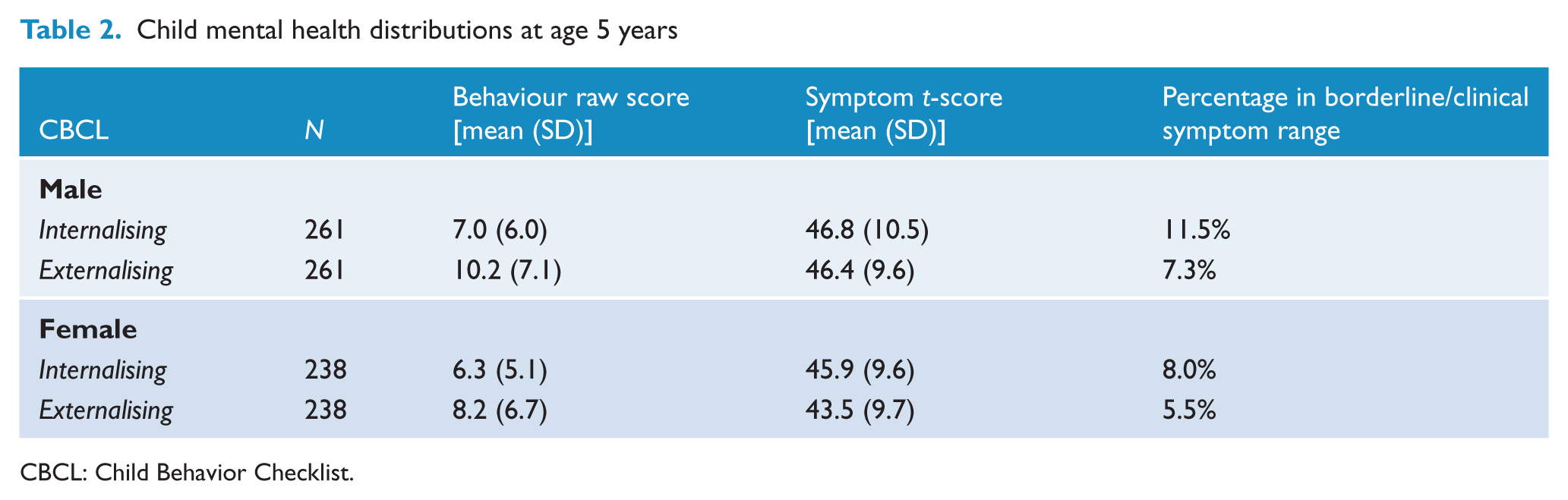
CBCL: Child Behavior Checklist.
Latent profile trajectories
The latent class analysis results include the 696 participants (95%) who provided at least two waves of data from infancy (pairwise deletion analysis). While results from the likelihood ratio test indicated a four-class model for internalising symptoms, the three-class model was retained because the fourth class accounted for a trivial estimated proportion (0.6%) of the population. Results from the likelihood ratio tests indicated that the three-class model was optimal for externalising symptoms. For each of the internalising and externalising analyses, one class (group of children) displayed higher than average mean symptom scores throughout development (21.4% for internalising and 20.0% for externalising), one class had average mean symptom scores throughout (48.4% and 52.2%, respectively), while another class had lower than average mean symptom scores throughout (30.2 and 27.8%, respectively). Figure 2 (internalising symptoms) and Figure 3 (externalising symptoms) show that the estimated mean symptom levels for each group of young children broadly follow flat and parallel (non-crossing) trajectories, consistent with a view that early childhood problems tend to persist rather than being merely transient over time.
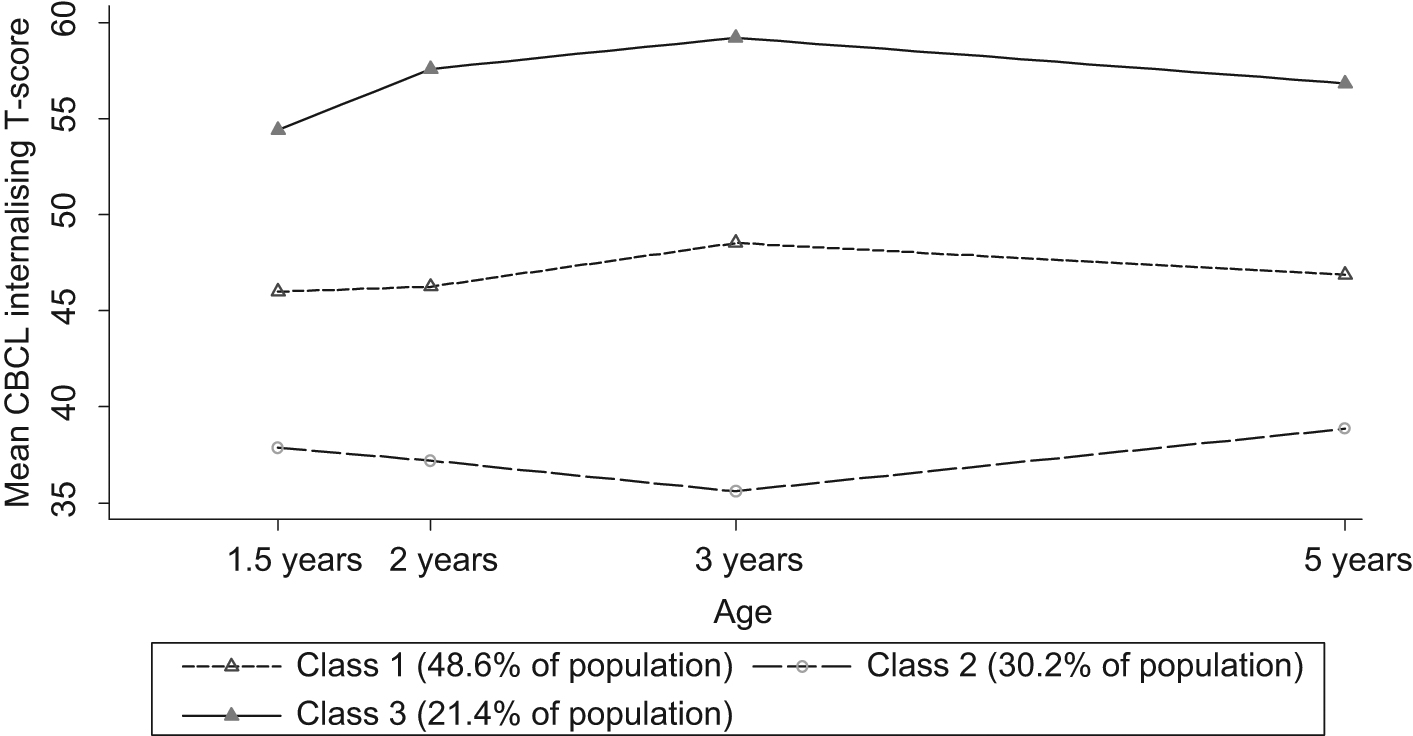
Groups of Australian children with different latent profiles of internalising symptoms (T-scores).
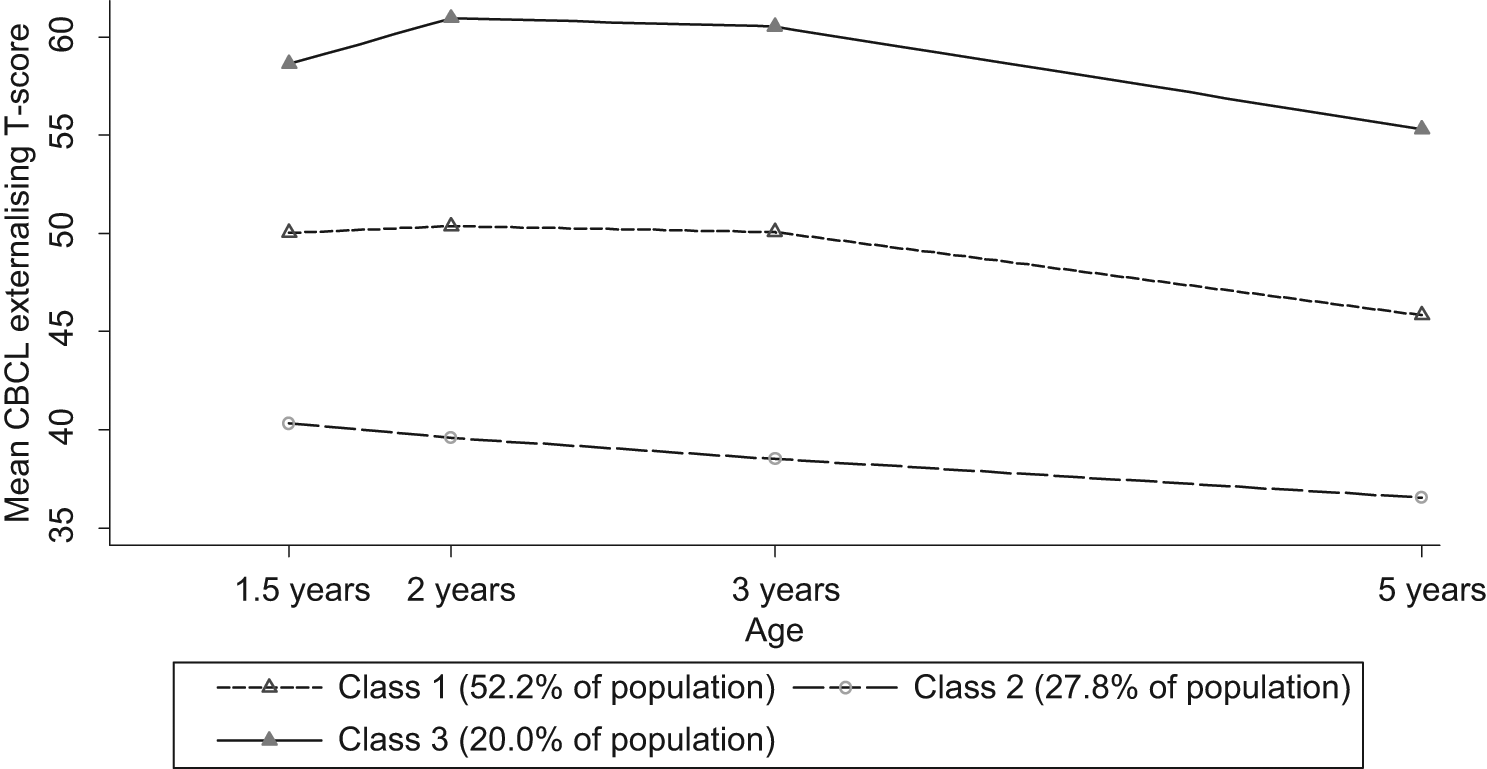
Groups of Australian children with different latent profiles of externalising symptoms (T-scores)
Early aetiology of 5-year-old internalising and externalising behaviours
The regression analysis results include the 396 participants (54%) providing full data from infancy (listwise deletion analysis). Table 3 shows the results for the regression model predicting the 5-year internalising behaviours (CBCL raw scores), which explain 21.8% of the variation. The most consistent (across time points) and cumulative (increasing risk) predictors of internalising behaviours were maternal stress and harsh discipline. Further statistically significant predictors of internalising behaviours were having no older siblings, single parenthood, maternal substance misuse and lower maternal expectations of their preschool child’s developmental abilities (the findings for nurturing parenting appeared mixed).
Early childhood aetiological risks for 5-year-old mental health behaviours
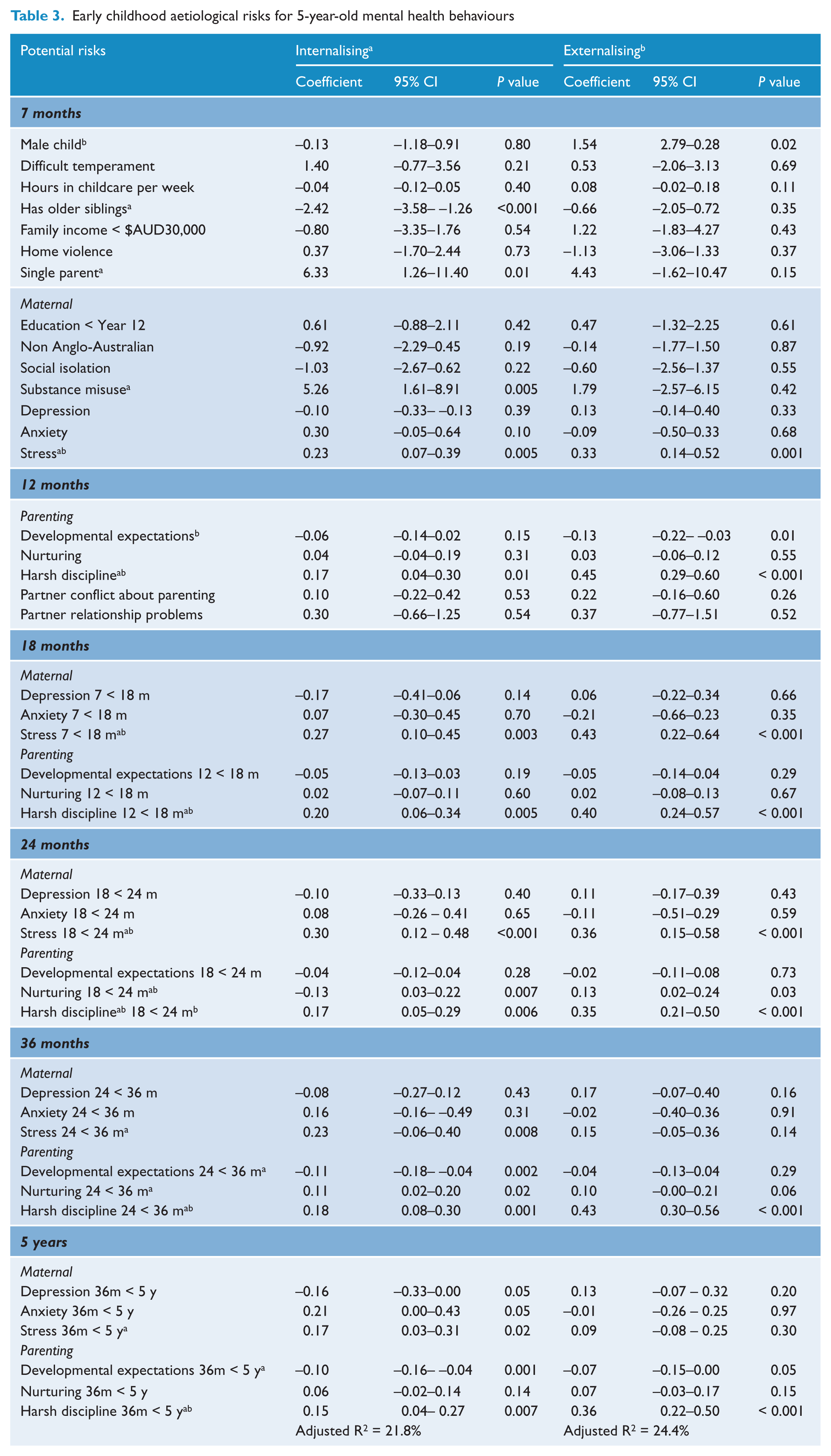
Table 3 also shows the regression model predicting the 5-year externalising behaviours (CBCL raw scores), which explain 24.4% of the variation. As for the internalising behaviours, the most consistent and cumulative predictors of externalising behaviours were harsh discipline and maternal stress. Further statistically significant predictors of externalising behaviours were being male and lower maternal expectations of a toddler’s developmental abilities.
Discussion
This study presents Australian population-based, longitudinal findings on young children’s mental health. In this sample, the prevalence of the mental health problems of 5-year-olds on the CBCL was 8–12% for internalising problems and 6–7% for externalising problems. Latent class analyses indicated that around one in five of these young children had consistently high symptoms (elevated above the CBCL normative mean) across early childhood development to 5 years (approximately when many Australian children start school). The data suggest children with persistent difficulties can be identified even prior to the toddler years. Contextually, longitudinal regression analyses showed that consistent and cumulative predictors of internalising and externalising behaviours were harsh discipline and maternal stress across early childhood development.
The strengths of this study are its data from infancy through to 5 years of age, with detailed, psychometrically sound and repeated measures of early childhood internalising and externalising symptoms, different parenting interactions and various aspects of maternal mental health, family functioning and socio-demographic characteristics. The study also has the following limitations. First, the sample was not representative of all Australian families with young children, since only 69% of eligible births were recruited, of which 68% were retained at age 5 years. Although a recruitment rate of 69% from birth records is a high rate for population surveys (Bayer et al., 2007; Reuband and Blasius, 1996), 30% of babies of unknown risk status were not included. Families recruited into the study were also slightly more likely to be retained at age 5 years if English was the main language spoken in the home, parents had completed tertiary education and household income was above $AUD60,000 per annum.
A second limitation is that only mothers were included as informants. Maternal mental health may influence the perception of child behaviour, potentially inflating the apparent association between variables. However, well-validated measures of child and maternal mental health were used (Achenbach and Rescorla, 2000; Lovibond and Lovibond, 1995). Mothers are also the most frequent primary caregivers in early childhood and so they are best able to observe behaviour across contexts (van Zeijl et al., 2006). A third limitation is that observational longitudinal designs can suggest but not determine causal directions of influence. Nevertheless, some randomised controlled trials (RCTs) of parenting interventions have demonstrated the causal impacts of parenting changes on young children’s externalising and internalising outcomes (Rapee et al., 2005; Shaw et al., 2006).
The findings have practical implications for developing prevention programs at a population level for children’s mental health. Latent class analysis highlighted a group of children with elevated symptoms from early toddlerhood to age 5 years, which points to a window for prevention very early on in life. Similarly, regression findings indicated that prevention could start in the early years of life, when smacking and yelling begin forecasting the internalising and externalising behaviours that are then witnessed at 5 years of age.
The results for ‘nurturing’ parenting practices appeared mixed. Recent literature noted confounding between ‘nurturing’ and ‘overinvolved/protective’ parenting interactions, with the latter being a risk factor for a child internalising difficulties (Bayer et al., 2006). To illustrate, a parent who quickly and anxiously gathers up a child in their arms when a stranger enters the room could be interpreted as providing nurturing, in contrast to overprotection. Therefore, future population studies should directly measure overinvolved/protective parenting interactions to determine the strength of this risk factor (Bayer et al., 2006; Rapee et al., 2010).
Internationally and in Australia, population-level RCTs of parenting and family support strategies in early childhood are under way (Bayer et al., 2011; Shaw et al., 2006). Family Check-Up (Connell et al., 2008; Shaw et al., 2006) starts prevention at toddler age with a targeted family support program for child externalising problems, maternal depression and financial stress. Cool Little Kids (Bayer et al., 2011) starts prevention at a preschool age with a parenting program to prevent shy/sensitive children from developing internalising problems during the transition from preschool to school. These programs have demonstrated efficacy in initial RCTs.
Conclusion
The findings from this population-based Australian sample highlight that children with persistent mental health symptoms can be identified in the early toddler years. They also highlight that maternal stress and harsh discipline are important risk factors throughout early childhood for developing internalising and externalising difficulties by the time children reach the age of 5. Population-level prevention trials targeting these risks are under way. The clinical implications of these findings are that primary health care professionals who see young families could inquire about a toddler’s socioemotional problems and consider referring families to evidence-based parenting programs. Additionally, policymakers can develop family support initiatives in the early years by drawing on prevention trial findings.
Box 1.
What is known
Mental health is an international public health issue. In childhood, problems primarily consist of externalising (conduct) and internalising (emotional) problems. At a population level these affect a substantial proportion of youth.
What is new
Groups of young children exist in the Australian population with persistently elevated internalising and externalising symptoms from infancy to age 5 years. The most consistent predictors of the mental health behaviours of 5-year-olds are family contextual risks throughout the early childhood period (i.e. harsh discipline and maternal stress).
What is clinically relevant
Effective population approaches to children’s mental health that start very early in life are needed, and these should focus on alleviating maternal stress and improving parenting interactions.
Footnotes
Acknowledgements
We would like to thank the families of the Victorian cities of Glen Eira, Greater Geelong, Kingston, Maribyrnong, Nillumbik and Stonnington who took part in this research.
Funding
This follow-up study was supported by an Equity Trustees grant, an Australian Rotary Health postdoctoral fellowship, National Health and Medical Research Council (NHMRC) Public Health Capacity Building Grant postdoctoral fellowships and a NHMRC Career Development Award.
Declaration of interest
The authors declare no conflict of interest regarding the publication of the manuscript. Dr Jordana Bayer had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. HH, JB and MW were involved in the formulation and design of the study and obtained the necessary funding. JB, MM and NA were involved with the acquisition of study data. OU performed the statistical analysis with assistance from JB and MM. JB, OU and MM are responsible for the interpretation of the data. JB and MM drafted the manuscript with critical revision from OU, HH, MW and NA.