
Abstract
Objective:
Economic recessions and severe weather events are often associated with increased suicide rates. The Global Dairy Crisis 2015/2016 led to an economic downturn in the New Zealand dairy farming industry and, coupled with droughts in some regions and floods in others, raised fears about increased suicide rates among farmers. However, little was known about suicides in the farming sector. This study reviews characteristics of recent farm-related suicides in New Zealand and assesses the extent to which financial stresses contributed to the deaths.
Methods:
Data were abstracted from coroners’ records for a consecutive series of 185 people in farm- and agriculture-related occupations who died by suicide between 2007 and 2015 and for whom coronial inquiries had been completed.
Results:
Farm suicides were heterogeneous: six distinct risk profiles were identified. Financial stresses made negligible contributions to farm suicides. Overall, risk factors for farm suicides differed little from risk factors for suicide in the general population. However, suicide risk in farmers was exacerbated by ready access to firearms: almost 40% of farm suicides involved firearms, compared to 8% in the general population over the same time. Among farm suicides, young male farm labourers predominated, rather than farm owners or managers. For many young men, relationship losses, acute alcohol intoxication and ready access to a firearm formed a common constellation of risk factors.
Conclusions:
While coroners’ records are variable and do not record specific information about financial stresses and weather events, it was clear that these issues made a negligible contribution to farm suicides. A range of rural suicide prevention initiatives are needed to address various farm suicide risk profiles. In particular, young male labourers often had no contact with health services prior to death, suggesting that rural suicide prevention efforts need to be positioned within community, farming and sports organisations, as well as health and social service providers.
Introduction
While suicide rates are typically higher in rural New Zealand and in farm workers (Gallagher et al., 2008; Ministry of Health, 2015), these groups were never a focus of suicide prevention until the Global Dairy Crisis of 2015/2016 halved international milk prices and exerted financial stresses on many farmers. The dairy industry is New Zealand’s largest export earner so these economic stresses, coupled with severe droughts and floods in some regions, generated extensive political, policy and public concern about the possibility of higher suicide rates in farmers. However, there was little information about farm suicides to guide the development of interventions to minimise suicide risk.
To address this gap, this study used coroners’ records to examine the demographic risk factors, characteristics and precipitating factors of a consecutive series of individuals in farm-related jobs who died by suicide in New Zealand. Deaths occurred between mid-2007 and early 2015 (the date for which most recent suicide data were available).
Methods
Data sources and sample selection
Suicide data were obtained from the Office of the Chief Coroner. All deaths which are suspected suicides are reported to a coroner. Suicide deaths are those deemed ‘intentional, with the intent of taking one’s own life’ by individual coroners. Coroners’ reports for all deaths determined to be suicides are collected centrally by Coronial Services, with this database maintained by the Ministry of Justice. Information contained within the coronial database includes demographic characteristics of the decedent, occupation, method of suicide and circumstances of the death.
Occupational category is assigned, by Ministry of Justice coders, to people aged 15 and over, on the basis of ‘usual occupation’, according to the Australian and New Zealand Standard Classification of Occupations (ANZSCO) (2013). For farming, an hierarchical classification of occupation with five levels of coding reflects skill level and farming type.
For this study, Ministry of Justice staff searched the coronial database for all deaths from 1 July 2007 to the search date (30 June 2016) with completed coronial verdicts of suicide and with farm-related and agriculture-related occupations. Deaths which were suspected suicides waiting for coronial verdicts were not included.
Suicides were included if their ANZSCO-coded occupation at death was ‘Farmers and farm managers’ or ‘Farm, forestry and garden workers’, ‘Farm hands and assistants’, ‘Skilled Animal and Horticultural Workers’, and ‘Factory Process workers’, or their ‘usual occupation’ was coded as farm- or agriculture-related (e.g. ‘retired farmer’, arborist, pruner, farmhand, shepherd, share-milker). All forms of employment were included (full-time/part-time/‘employed with no further details on hours of employment’). Unemployed and retired farmers were included because they often remain living and working on farms, and continue to be affected by farm-related stressors.
To supplement statistical coronial records, the Certificate of Coronial Findings was reviewed for each case. This narrative summary provides the reasons for the coroner’s verdict of suicide. Each Certificate was interrogated to obtain information to assist in understanding the precipitants and circumstances of the death. To record data, a data abstraction form constructed for previous suicide studies was used (Beautrais, 2001).
Classifications of occupation assigned by coronial data coders to each case were checked by the researcher against information in each Certificate of Coronial Findings to ensure, within the limits of the information available, that no dairy farmers or dairy farm workers were overlooked by having been assigned generic codes of ‘Farm, Forestry and Garden Worker’, ‘Livestock Farmer’, for example, rather than the more specific codes of ‘Dairy Cattle Farmer’ or ‘Dairy Cattle Farm Worker’.
Analysis
Variables included in the analysis spanned: demographic characteristics, circumstances of the death, physical illness, history of suicidal behaviour, psychiatric diagnoses, history of psychiatric inpatient and outpatient care, contact with health professionals prior to death, history of problematic alcohol and/or drug use, history of criminal offending or legal charges, recent stressful life events including farm-related financial or weather stressors. Because there were missing or unknown values for some variables, data were analysed by simple descriptive statistics.
Results
Farm suicide trends
To provide background to the study, data were obtained from the Office of the Chief Coroner to examine trends in farm suicides. These data included provisional figures up to 30 June 2016: 2007/2008, 29 farm suicides; 2008/2009, 29; 2009/2010, 26; 2010/2011, 24; 2011/2012, 22; 2012/2013, 17; 2013/2014, 20; 2014/2015, 26; 2015/2016, 17. While the numbers are small, these data suggest declining annual numbers of farm suicides from 2007/2008 to 2015/2016.
Study of coroners’ records
Farm-related suicides – employment characteristics
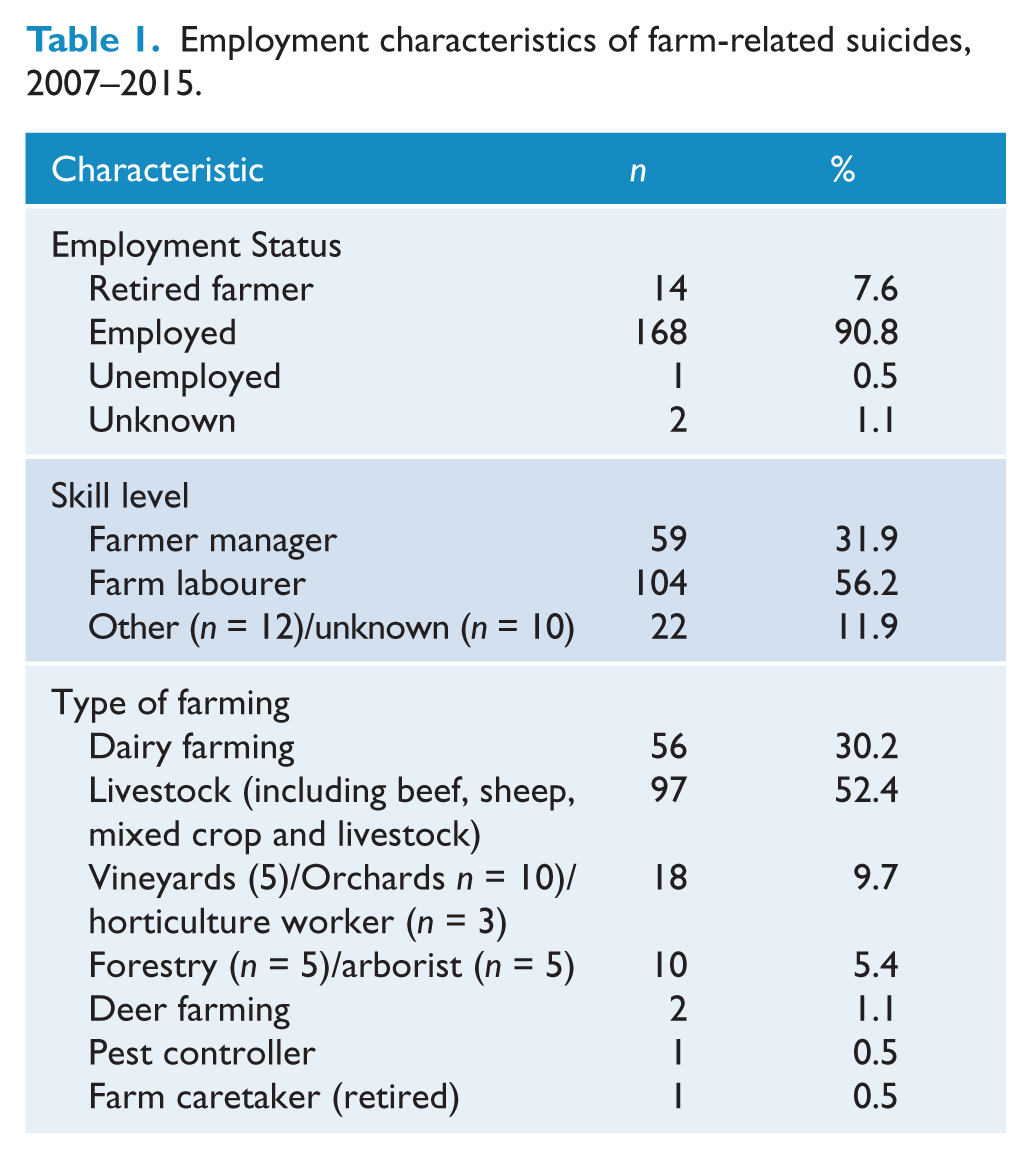
Table 1 shows occupational status, skill level and type of farming for all farm and agriculture-related suicides (referred to hereafter as ‘farm suicides’). Only one person was recorded as being unemployed. Almost twice as many suicides (104/185, 56.2%) were people employed as farm labourers compared to those who were farm owners or managers (59/104, 31.9%). Suicides in the dairy industry accounted for one-third (56/185, 30.2%) of all farm suicides.
Employment characteristics of farm-related suicides, 2007–2015.
Farm suicides – demographic characteristics
Table 2 shows age and gender characteristics of the 185 farm suicides. Suicides were overwhelmingly male (169/185, 91.4%); 16/185 (8.6%) were female. Mean age at death for all suicides was 42.1 years (range: 15–89 years; males: 42.4 years (range 15–89 years) and females: 39.5 years (range 16–60 years). While the ages of those who died ranged from 15 to 89 years, overall, suicides were young: one quarter (24.8%) was aged <25 years, one-third (32.4%) was aged <30 years and almost one half of the sample (47.6%) was aged <40 years.
Farm-related suicides, 2007–2015, by age and gender.
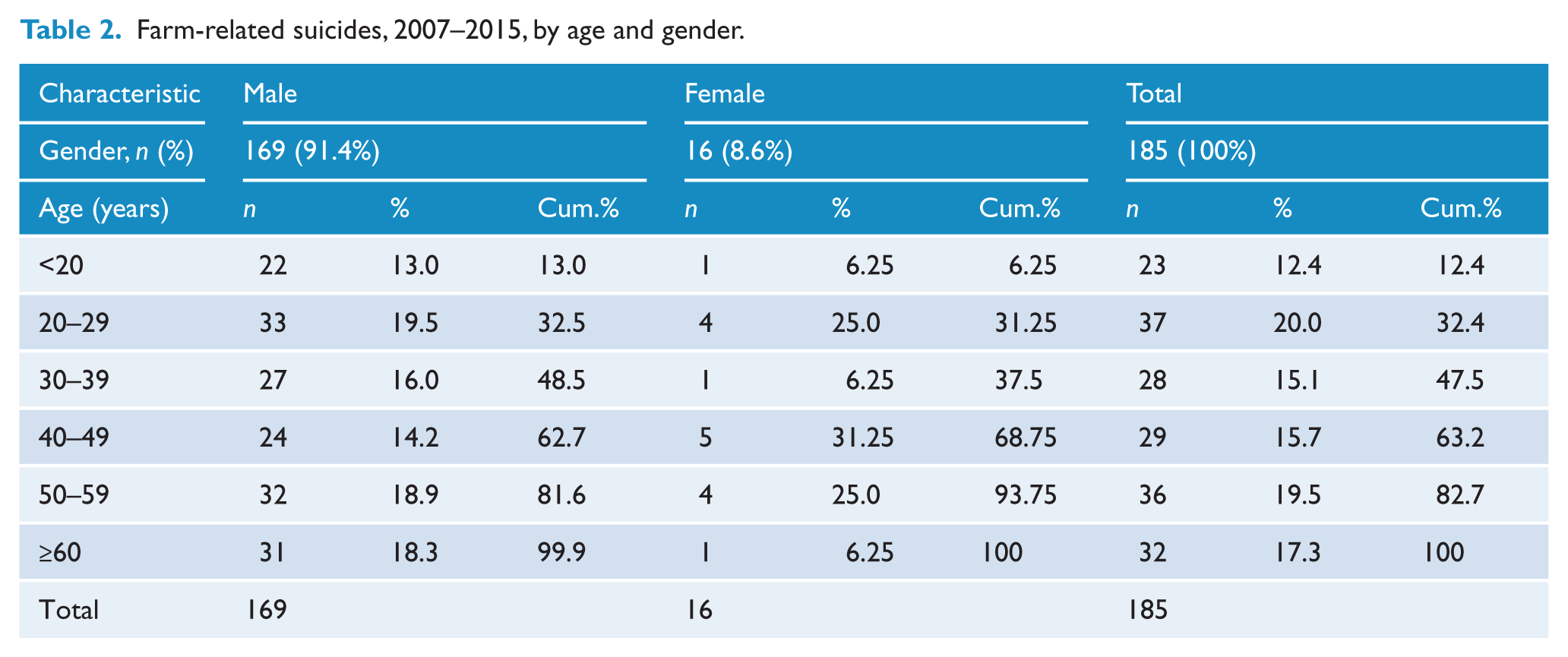
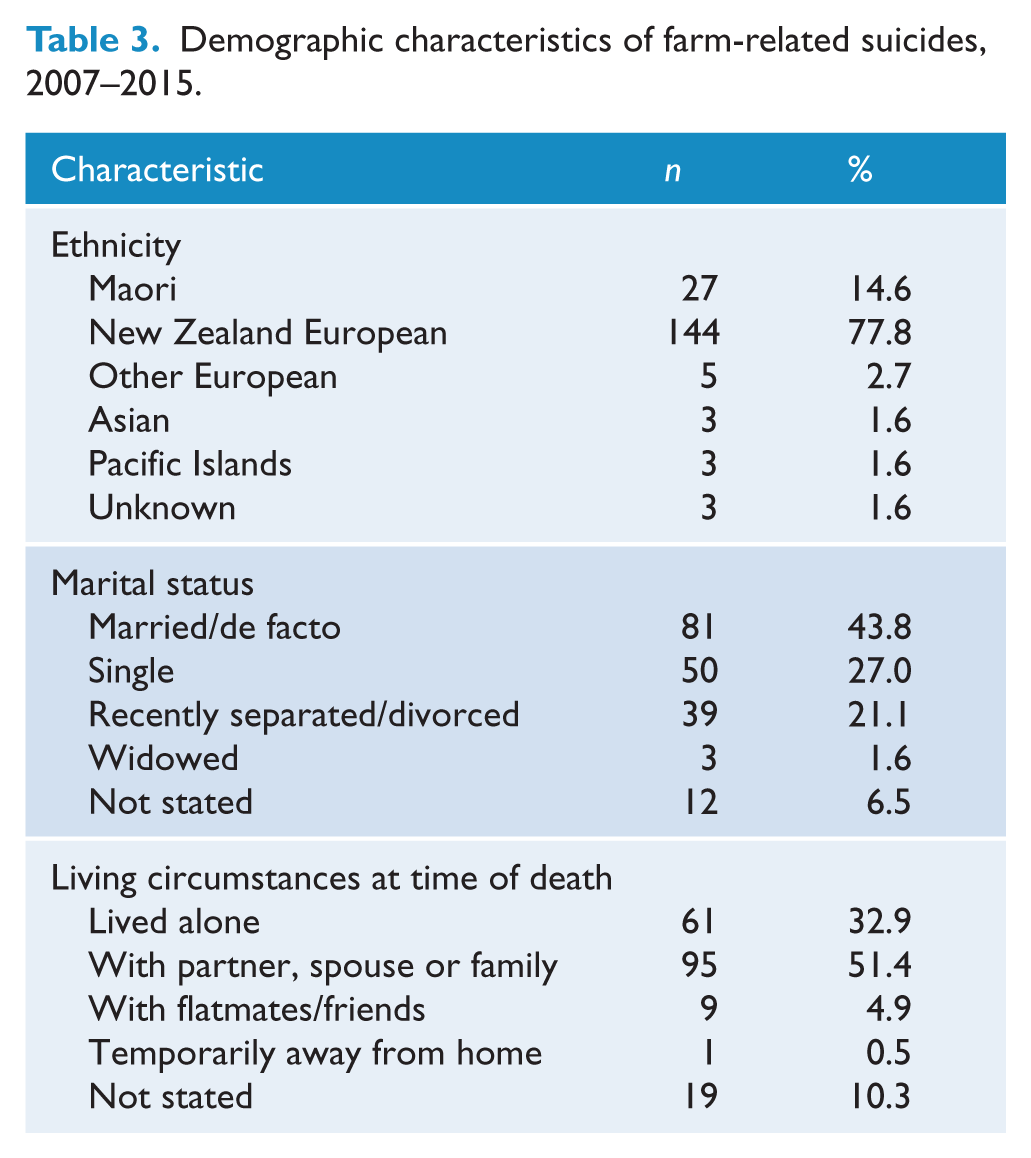
Table 3 shows demographic characteristics of farm suicides. Most were New Zealand Europeans (78%). While 44% were in a marital partnership, one in five (21%) of those who died was recently separated or divorced. One third of those who died by suicide lived alone.
Demographic characteristics of farm-related suicides, 2007–2015.
Dairy farm suicides
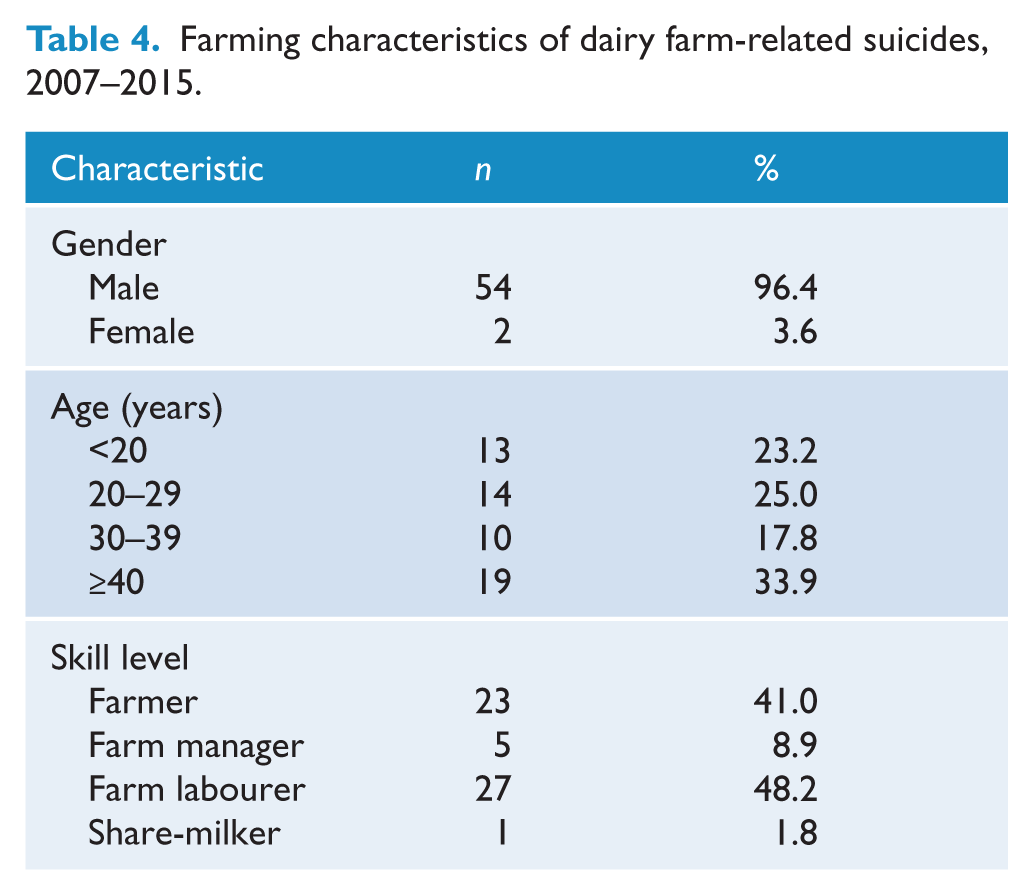
Suicides in the dairy industry accounted for one-third (56/185, 30.2%) of all farm suicides. Of these, 54/56 (96.4%) were male (Table 4). Most were young: almost a quarter (13/56, 23.3%) was teenaged, and almost half (27/56, 48.2%) were aged less than 30 years. Ten (17.8%) were aged 30–39 years, and one-third (19/56, 33.9%) was aged 40 or older. Almost half (27/45, 48%) were farm labourers; 23/56 (41%) were described as ‘farmers’ (presumably including farm owners), 5 were farm managers and 1 was a share-milker.
Farming characteristics of dairy farm-related suicides, 2007–2015.
Suicide risk factors and precipitants
Based on all available information the single most important factor contributing to the suicide death was determined. The most common precipitant was existing mental illness (53/185 people, 28.6%). Relationship breakups or separations were common, occurring in 20% (n = 37). The other precipitating factors included the following: conflict or arguments (n = 15, 8.1%), physical health problems (n = 23, 12.4%), legal charges or issues (n = 10, 5.4%), acute alcohol or drug intoxication (n = 6, 3.2%), life ‘struggles’ or accumulated problems (n = 4, 2.1%), work problems (n = 2, 1.1%) and the recent death of a family member or friend (n =2, 1.1%). In 16 cases (8.6%), there were a variety of other reasons. In eight cases (4.3%), coronial records provided insufficient data to determine a reason or precipitant for the death. Severe weather events were scarcely mentioned.
Financial problems were the leading factor contributing to 9/185 (4.8%) suicides. These problems were related to personal or family debts, costs incurred with vehicles or fines, being unable to sell a lifestyle property or poor business decisions made prior to the onset of the dairy farm crisis or made on farms which were not dairy farms. There was no indication from the information contained within coroners’ records that financial stresses exerted on dairy farmers were the major factor contributing to any suicides. While the absence of information in coronial records does not mean that financial stresses may not have occurred, in most cases the major precipitant of the suicide was very clear from these records, and these records clearly indicated that financial stresses did not have the major role in the death.
Health care characteristics
Information in coroners’ files relating to healthcare is not recorded consistently. Such data are more likely to be recorded for major events such as hospital admissions, or health problems requiring medical care. Coroners’ files are less likely to contain information about recent general practitioner (GP) visits, or prescribed medications. Despite these limitations, information in coronial files about healthcare supported the finding that existing mental health problems made significant contributions to suicide in many cases: 49 people (26.5%) were recorded as having had contact with a mental health provider for a psychiatric problem within the year prior to their death. Almost half of all cases (83/185, 44.9%) had a lifetime history of treatment for a psychiatric illness, 38 (22%) were recorded as having made at least one previous suicide attempt and 72 people (39.9%) had communicated suicidal intent within the last year to family and/or healthcare professionals.
Means of suicide
Figure 1 shows the methods of farm suicides and compares methods of farm suicides with those used by the total New Zealand population, for the year 2012 (most recent year for which data were available). The most common method of farm suicide was hanging (45.9%), followed closely by firearms (39.5%). Vehicle exhaust gas was used by 7.6%, while poisoning and overdose accounted for 4.9%. Firearms were almost five times more likely to be used by those in farm-related occupations (39.5%) than in the general population (8.4%, χ2 = 15.1; df = 1; p < 0.0001).
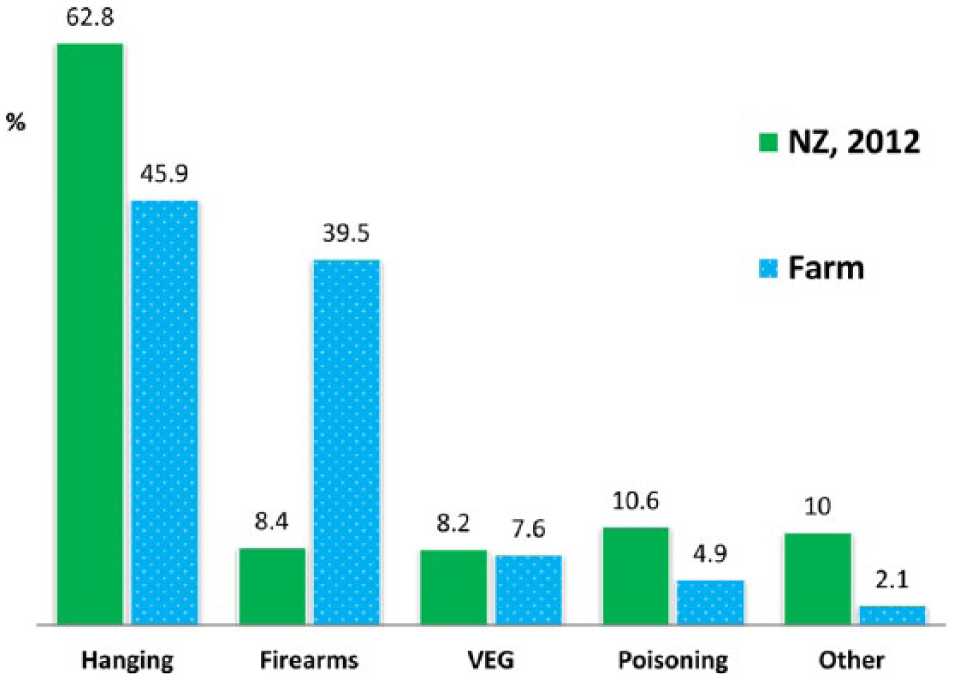
Fraction of all suicides (for New Zealand total population, 2012, and farm-related suicides, 2007–2015) by method of suicide.
Risk profiles
Farm suicides were a heterogeneous group; it was possible to identify six risk profiles (outlined in Box 1). These profiles differed in terms of age, living circumstances and major stresses contributing to suicide. The first profile was characterised by the youth of the decedents, the second was typified by young men with fragile relationships, whose failure often precipitated the suicide, a third was characterised by severe or terminal physical illness and a fourth was represented by older, often retired farmers with physical illnesses. Mental illness characterised a fifth group. The female suicides, most with mental illness, constituted the sixth category. Dairy farm suicides were distributed across the six risk profiles.
Common risk profiles for farm-related suicides.
1. A young farm labourer, often away from his family, may work in an isolated area, may live alone in farm accommodation. Social activities off-farm tend to involve drinking. Suicide typically occurs when he is home alone, sometimes intoxicated after a social event, and has access to a loaded firearm. Suicide may be precipitated by a rejection message from a potential or actual girlfriend. Usually, he has not seen a general practitioner (GP) prior to the death. Opportunities for intervention lie with encouraging harm minimisation alcohol policies in rural social activities, and with restricting on-farm access to lethal means of suicide, especially firearms.
2. A young labourer or farm manager, aged in 20s and early 30s, often with a young partner and young children. The relationship is often fragile and tumultuous and suicide may occur after his partner leaves or threatens to leave. Not all suicides are precipitated by relationship loss: other precipitants include legal crises, police charges or an argument at work likely to result in dismissal. He may be a vulnerable individual with a childhood history of disadvantage and dysfunction, may lack educational and job skills, and may have problems with alcohol/drug use. Suicides are typically by firearms if it is a livestock farm, or hanging. May be intoxicated. Some go to see a GP after a relationship break-up, are diagnosed with an adjustment disorder, may be prescribed sleeping tablets. Often no clear documentation re follow-up plans and screening for suicide risk. Intervention opportunities lie with healthcare contacts, and, since the young man often made suicide threats in the context of the precipitating crisis, encouraging partners, friends and workmates to refer vulnerable young men to crisis intervention services.
3. An older farmer, in his 50s, usually married, with an existing serious health problem (e.g. head injury, severe or terminal illness) likely to impact mobility or quality of life. Well known to GP and medical specialists. May have threatened suicide, saying he was not prepared to tolerate loss of mobility, pain or diminished quality of life. Typically uses firearm for suicide since, despite threats of suicide, the firearm remains available. Typically leaves a suicide note indicating that the severity of his physical condition had rendered life intolerable. Challenges for intervention lie with educating healthcare providers to better manage depression and palliative care in older, often independent men with severe and terminal illnesses.
4. An older often (part) retired farmer, with concerns about physical symptoms or decline. Fears becoming ill and dependent, and may have made threats that he would kill himself rather than endure such illness. Despite fears of serious illness may not have visited his GP. Others may visit their GP but are not reassured that they are not ill. Has retained a firearm even if he no longer farms, and uses it for suicide, surprising his family who often say that they had not taken his threats of suicide seriously.
5. Male with a risk profile dominated by severe, enduring mental illness, including depression, anxiety, psychosis and alcohol/drug dependence. Well-known to GP and mental health providers. Families well aware of their struggles with mental health problems. Histories of psychiatric admissions, prior suicide attempts and outpatient mental health care. Some attempt suicide when they come to see their mental health problems as intractable and unable to be ameliorated. May be readily overwhelmed by external, additional stressors. May have made poor (sometimes, financial) decisions in the past, perhaps, in part, because of their mental health problems. Might benefit from additional supportive or respite care when stressors emerge that they find burdensome on top of their mental health problems. Families and carers need access to respite care and to support for themselves.
6. Women who work on farms, often in casual or part-time labouring jobs. Often characterised by a burden of serious mental health problems and histories of family and childhood disadvantage and dysfunction. Most are well-known to healthcare providers, including mental health services and may have histories of inpatient care and suicide attempts. Some are challenging patients for mental health services. Nothing specific about farm work precipitates their suicide: may have farm jobs because of limited job skills, and mental health history. Opportunities for intervention lie with healthcare and social services, and provision of support to family and carers.
Discussion
Main findings
Risk factors for suicide in people in farm- and agriculture-related occupations differed little from risk factors for suicide in the general population (Beautrais et al., 2007; Turecki and Brent, 2016). Mental illness was the most common single major contributing factor to farm suicides. Beyond their role as the most salient precipitating factor in the suicide, mental health problems, particularly, depression, anxiety and substance abuse, were frequently present in people with other precipitating factors. Physical health problems were common, especially in older farmers. Stressful relationship, legal, work-related and financial problems contributed to suicide risk. A relationship breakup or separation often preceded suicide. All these risk factors have been shown to be associated with suicide risk in the general population (Turecki and Brent, 2016), and are not specific to farmers. Nevertheless, suicide rates for farmers are higher than national rates in New Zealand (Gallagher et al., 2008), and in countries with similar agricultural industries (Brown et al., 2014; Klieve et al., 2009; Lahti et al., 2014; Nance et al., 2010; Page and Fragar, 2002).
Hanging was the most common method of farm suicide, accounting for 45.9% of all deaths. In New Zealand, hanging was the most common method of suicide in the general population accounting for approximately 60% of all suicides each year. However, firearms were five times more often used in farm suicides than in the general population over the same period. Given that risk factors for farm suicides were similar to those for non-farm suicides, it appears that the farm environment exacerbates risk for farmers by providing ready access to a highly lethal method of suicide.
Restricting access to lethal methods is one of the most effective approaches to prevent suicide (Mann et al., 2005). While there are limited opportunities to restrict access to hanging, numerous studies have shown that access to firearms can be restricted in various ways, and that such restrictions reduce suicides by that method. In New Zealand, for example, the introduction of more restrictive firearms legislation (Arms Amendment Act, 1992, http://www.legislation.govt.nz/act/public/1992/0095/latest/DLM278351.html, accessed 09/04/2017) decreased the mean annual rate of firearm-related suicides by 46% (Beautrais et al., 2006).
Independently of other risk factors, access to firearms is associated with increased risk of suicide (Kellermann et al., 1992). Access to firearms is common on farms. The findings of this study suggest that a major opportunity for suicide prevention among farmers lies in the promotion of firearm safety and controlling access to firearms. Firearm safety can be promoted by farm workers themselves, and by their families, police, health providers and rural organisations. Inquiry about firearms, and, where appropriate, advocacy for their removal, should be a routine part of suicide risk assessment by rural healthcare providers. Police attending any call out to a farm can use it as an opportunity to check on firearm safety. The use of a farm armoury to restrict access to firearms to specific tasks at specific times might prevent some distressed people having immediate access to a highly lethal method of suicide.
Financial problems were reported as the major precipitant for suicide in less than 5% of farmers. These problems were not linked to financial stresses in the dairy industry. However, suicides in this study might not span the timeframe of maximum impact of low dairy farm pay-outs and associated financial pressures. To take account of this limitation, it would be helpful to extend the present study to include all farm suicides from 2015 to 2020. Expanding the study in this way would provide information about critical time periods for economic impact, including, for example, whether low pay-outs have an early or lagged impact on farmers, and whether they have a different impact at different times for farmers with different roles and financial responsibilities (e.g. farm owners vs. share-milkers or farm labourers).
Farm suicides were a highly heterogeneous group. This study identified six different suicide risk profiles. Most discussions of farm suicides, and many previous studies, have treated farmers as a homogeneous group, and media reports often conflate farm suicides with rural suicides. This study suggested that another source of heterogeneity is the type of farming. Different types of farming may be associated with different risks. For example, livestock farmers had ready access to firearms and tended to use those for suicide, whereas hanging was the dominant method for those who worked in viticulture or horticulture, where firearms are not typical work tools.
A key finding was the youth of farm suicides: 25% were aged less than 25 years and almost half were under 40. One quarter of dairy farm suicides involved teenagers. Approximately 20% of people involved in suicides in the general population are also aged less than 25 years. However, the youth involved in farm suicides warrant emphasis since, too often, a series of (incorrect) assumptions are made which exclude young men from farm suicide prevention programmes. These assumptions include that farm owners are at risk of suicide because of financial and weather events, and that intervention programmes should therefore be directed at this group. In this way, young labourers, and potentially modifiable risk factors which pertain to them, are excluded from intervention programmes.
Most of the young men who died by suicide were farm labourers; twice as many labourers as farm owners or managers died by suicide. While these findings are consistent with the fact that there are more labourers than owners or managers on farms, they also reflect the fact that, as with most occupations, those with fewest skills, and least education, are at higher risk of suicide than those with superior skills and education (Milner et al., 2013). However, with rare exceptions (Arnautovska et al., 2015), few studies have explored differences in suicide risk between farm owners/managers and farm labourers. Differences among farmer groups may mean that specific interventions could be targeted to at-risk sub-groups. For example, programmes developed in response to the recent threat of increased suicides among New Zealand farmers were directed at farm owners, based on the assumption that they would be most affected by economic and weather events. Farm labourers were not recognised as a vulnerable group, and opportunities to address potentially modifiable risk factors in this group were overlooked.
Findings from this study suggest value in a more detailed programme of research about farm suicide. Few studies have obtained comprehensive data. Most studies have relied on coronial files, which have limitations. Internationally, only two psychological autopsy studies of farmer suicide have tried to gather more extensive data, and both have serious shortcomings (see below) (Kunde, personal communication, 2016; Malmberg et al., 1997, 1999). A well-designed psychological autopsy study that included data from multiple sources and interviews with family members and healthcare providers could examine specific issues (e.g. the role of financial stresses, the impact of changing farm practices, sub-group differences in farmer risk, stresses on immigrant farm workers) and help to develop targeted rural support and suicide prevention programmes.
Strengths and limitations
This study has several strengths. It is the first study in New Zealand to examine farm suicides. It involved a national and relatively large sample. Coroners’ records were available for all cases; most records contained information from family members and some from GPs who had cared for the deceased.
However, there are some limitations. First, the study is based on coroners’ records which do not collect data in a consistent way and which vary in the type and amount of information contained. Second, the study may not cover the full period of maximum impact of economic stresses. Third, the study is limited to people whose usual occupation was coded as ‘farm-related’. This coding frame may have omitted some people whose usual occupation was not farm-related but who were, nevertheless, affected by economic stresses in the farming sector. Such omissions could, for example, include farmers’ partners and children who worked off-farm but lived on-farm. Fourth, the study was limited to farm-related suicides and did not seek to examine the impact of economic and weather stresses in the farming sector on rural service providers and businesses. Fifth, stresses in farmers and their families which did not result in suicide were not examined. It may be that some families experienced considerable economic stresses but were able to cope. Sixth, the study was not designed to assess whether the programmes that were implemented to provide support to farmers might have prevented suicides. Despite these limitations, this study is useful in highlighting the need to bring factual data to an emotive issue, to identify the farm-related populations at risk of suicide and opportunities for intervention and to provide information about the relative roles of specific stresses (including financial stresses) in farm suicides.
Comparison with previous findings
Elevated suicide rates among farmers are consistently reported in a number of countries, including New Zealand and Australia (Hirsch and Cukrowicz, 2014; Kennedy et al., 2014). In New Zealand, two studies have reported elevated suicide rates in farm-related occupations (Gallagher et al., 2008; Suicide Mortality Review Committee, 2016), but neither study explored the characteristics of the decedents in detail.
In Australia, recent prolonged droughts have prompted a number of studies of farm suicides (Arnautovska et al., 2014; Fragar et al., 2011; Kennedy et al., 2014). However, many studies have included only basic demographic data. Psychological autopsies are a valuable tool for gathering more comprehensive social, economic and psychological information by interviewing healthcare providers and family members of the deceased. It appears that, worldwide, only two psychological autopsy studies of farmer suicide have been attempted; both are small and have limitations. Malmberg and colleagues reported on a study of 84 farmer suicides in England, but only 69% of the decedents were working in farming at the time of their death and in only 28/84 cases were interviews conducted with relatives (Malmberg et al., 1997, 1999). In Queensland, researchers used an existing database of 50 suicide decedents aged 35 and older as the basis for a psychological autopsy of farmer suicide but conducted interviews for only 16 cases (Kunde, personal communication). The age restriction (>35 years) of the original study excluded a significant fraction of (younger) farm workers. Despite concern and research about farmer suicide, substantial gaps in knowledge remain. These gaps could potentially be addressed with a carefully conducted psychological autopsy study.
While studies of farmer suicide typically aggregate farmers across type of farming and skill level, some recent Australian research has recognised the heterogeneity of farming, and of farmers. An Australian-wide study of 921 suicides from 1988 to 1997 reported that 67.4% were farm managers in older age groups (55 + years) (Page and Fragar, 2002). A Queensland study found differences in risk factors for suicide between farm managers and labourers accounted for by age (Arnautovska et al., 2015). When age was taken into account, managers were more likely to have a psychiatric illness, while labourers were more likely to be facing pending unemployment. These findings differ from those found in the present study, and are likely explained by differences in types of farming, different skill levels among farmers, range of responsibilities and types of stresses.
A recent review summarised international literature about the impact of global changes in dairy farming on a range of health outcomes including mental health, stress, depression and suicide (Lunner Kolstrup et al., 2013). The authors highlighted gaps in knowledge about the mental health of dairy farmers and the psychosocial impact of their working conditions on mental health, and called for more systematic studies of these issues.
Implications for prevention
The 185 people in farm-related occupations who died by suicide were not a homogeneous group. They could be represented by six broad profiles which varied in terms of age, risk factors, suicide precipitants, physical health, mental health history, and contact with primary care and mental health services. In the absence of data such as these, rural suicide prevention programmes have tended to be broad and generic and not specific to type of farming, type of farmer, a specific region or problem or to specific risk profiles. The sub-groups evident in this study justify targeted prevention approaches.
In the group of young farm suicides, relationship problems, access to a firearm and, sometimes, intoxication, were a fatal combination. Few of this group had contact with a GP in the period prior to their death, suggesting that interventions for this group need to be delivered in settings other than primary care. Appropriate settings could include farming and industry events, and sports, leisure and local community activities. Relationship problems and substance abuse problems were common in this group, suggesting that (a) police might be involved on occasions and should be alert to suicide risks and (b) programmes in agricultural colleges and polytechs which strengthen personal coping skills could be helpful. Gatekeeper training to equip rural residents with the skills and confidence to recognise people who might be stressed or depressed and to refer them to appropriate resources could also help. Support and advice to young farmers could be offered via Internet programmes and Facebook groups. Farmer peer support groups should be educated about which farming groups are at high risk, and how to target appropriate support.
Older farmers with physical health problems and those with mental health problems were typically well known to primary care providers and to mental health services, suggesting that enhancing education for primary care providers about suicide risk assessment and management, and depression recognition and treatment, could be helpful. Improving rural mental health services, including crisis management, would seem sensible. For all health and social service providers, education about the importance of inquiry and counselling about access to firearms and other lethal means of suicide is important. At a community and industry level, making farmers, farm employers and peer support providers aware of the importance of firearm safety is an essential strategy. Strategies which focus on the need for safety rather than restrictions are likely to receive more support.
All these recommendations are consistent with current evidence for best practice for suicide prevention, recently scrutinised in this journal (Jorm, 2016). This evidence spans restriction of access to lethal means, education of primary care providers and gatekeepers, better treatment of depression and other mental illnesses (Goldney, 2016; Jones and Cipriani, 2016; Schaffer and Sinyor, 2016), and the introduction of multi-level approaches which aim to capitalise on additive and synergistic programmatic effects (Hegerl and Kohls, 2016; Krysinska et al., 2016; Pirkis, 2016). Suicide prevention programmes to benefit farmers and rural areas need to be implemented as part of broader rural health, and mental health, strategies. Within the rural context, this study reinforces the critical need for sound demographic and risk evidence to underpin investment decisions to ensure that the limited funding for rural suicide prevention is well-targeted.
Footnotes
Acknowledgements
We are grateful to the Office of the Chief Coroner for granting access to records.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided to the Rural Health Alliance of New Zealand (RHAANZ) by AgResearch, an independent research and development company (state owned) set up as a New Zealand Crown Research Institute (CRI).