
Abstract
Suicide among children and young adolescents is extremely rare. Recent estimates suggest that, internationally, suicide rates for children aged 5–14 years are of the order of 1–2 deaths per 100 000 [1]. These rates are significantly lower than suicide rates for youth aged 15–24 years which range, for selected developed countries, from to 7–27 deaths per 100 000 [1]. Nevertheless, concerns are emerging in a number of countries that the rate of suicide among children aged less than 15 years may be increasing [2–5]. Furthermore, rates of child and young adolescent suicide appear to be increasing while suicide rates among youth 15 years and older are declining or stabilizing [6].
While absolute numbers of child and young adolescent suicides may be small these trends suggest the need to know more about the epidemiology and characteristics of children who die in this way. However, the rarity of child and young adolescent suicide has imposed limitations on both the numbers of studies of child suicide and the ways in which such studies have been able to be conducted.
In the quarter century since Shaffer's landmark 1974 study of 30 children aged 12–14 years who died by suicide in England and Wales [7] few studies have focused on suicide in children and early adolescents, despite an exponential growth in studies of youth suicide (15–24 years). Shaffer's study was based on review of coroner, school, medical and social service records for children who died between 1962 and 1968, and identified two profiles of suicide risk: (i) a socially isolated child of high intelligence, whose mother was mentally ill; (ii) a child who tended to be aggressive, impulsive and often in trouble at school.
A series of studies has reported on the demographic features of child suicide using data from death certificates. Roesler examined death certificate data for 37 children aged 5–14 years who died by suicide in Minnesota (USA) from 1990 to 1994 and offered some comments on prevention strategies based on his finding that a majority who died had used a firearm [2].
In a series of papers in the 1980s Kosky examined a range of issues related to childhood suicidal behaviour among young Australians [8–10]. These studies suggested that most children dying by suicide and making suicide attempts were male, and most used violent methods. Significant proportions of children with suicidal behaviour were poor academic achievers and had been exposed to problematic family circumstances including intrafamilial violence, parental separation and divorce, and welfare dependency.
Often children have been included in studies of youth aged less than 20 years, but, because they have constituted only a small minority in these studies, few, if any, comparisons have been drawn between older and younger adolescents. Lee and colleagues reviewed 31 cases of suicide from 1988 to 1998 among young people aged 11–17 years in Charleston (USA) [5]. Most victims were older, male, white, used a firearm and 26% had a documented history of mental illness. Byard and colleagues compared age, gender and method features of 48 cases of suicide aged 13–16 years in South Australia from 1987 to 1997 with 70 cases aged 11–16 years from San Diego County (USA) [11]. Methods of suicide differed between the two countries with firearms used more often in San Diego than South Australia. Within South Australia methods differed by age, with older adolescents more likely than younger adolescents to die by hanging or vehicle exhaust gas. Thompson examined demographic features of 190 suicides aged 20 or younger in Manitoba (Canada) from 1971 to 1982 [12]. Of these, 22 were aged less than 15 years. Hanging was associated with the 12–14-year-old group, but, overall, few comparisons were drawn between the older and younger adolescents in this sample.
Hoberman and Garfinkel compared 208 older (15–19 years) and 21 younger (≤?14 years) adolescents who died by suicide in Minnesota (USA) from 1975 to 1985, using data extracted from medical examiners records [13]. Younger adolescents were more likely to be described as impulsive, angry, nervous and conduct disordered while older adolescents were more likely to be seen as sad, despairing, depressed or substance abusing; younger adolescents were more likely to die by hanging while older adolescents tended to use firearms; suicide precipitants were more commonly school problems and/or an argument with a parent for younger, rather than older, adolescents.
A series of psychological autopsy studies of adolescent suicide has included children aged less than 15 years but the small numbers of such deaths have tended to preclude comparisons between older and younger adolescents [14–17]. However, Shaffer and colleagues, in a study of 120 suicides aged less than 20 years, reported that the prevalence of mental disorders, particularly substance abuse, increased with age, and noted that it was their impression that younger adolescents tended to die by suicide in circumstances which suggested they had misjudged the repercussions of a stressful event or crisis [18].
Recently Groholt and colleagues comprehensively compared risk factors and characteristics for suicide between 14 children (< 15 years) and 115 adolescents (15–19 years) who died by suicide in Norway from 1990 to 1992 [19]. Compared with older adolescents, younger suicides were more likely to die by hanging, and their deaths were less likely to be preceded by mental disorder, suicidal ideation or a precipitant life stress. The authors concluded that the substantially lower risk of suicide in younger, compared with older, adolescents might be best explained by younger adolescents having less exposure to the known risk factors for suicide.
In New Zealand suicide among children and adolescents aged less than 15 years is rare but appears to have increased during the last few years, at the same time that the suicide rate for youth aged 15–24 years seems to be stabilizing [20]. In 1998 the rate of suicide among 10–14-year-olds was 4.4 deaths per 100 000. Comparisons suggest that this rate is higher than those for a series of comparable developed countries [1].
To monitor this emerging trend it is useful to examine the characteristics of child and young adolescent suicides in New Zealand. To date no studies have done this. This study describes the epidemiology and characteristics of childhood and young adolescent suicide in New Zealand during the 10-year period from 1989 to 1998.
Method
Cases
The cases were all 61 children and young adolescents aged less than 15 years who received coroner's verdicts of suicide in New Zealand during the 10-year period from 1989 to 1998.
Data collection
Data were collected for each case by review of coronial files. These files contained police reports (based in most cases on interviews conducted with family members) and coroner's inquest findings. The amount of information contained within these files varied, reflecting differences in practices for investigation of these deaths in different coronial jurisdictions. However, all files contained basic demographic data in a structured police record including age, gender, method of suicide, and most files contained information concerning precipitating circumstances. Information regarding family circumstances, and the mental health, psychological and behavioural charactersitics of the individual were recorded less consistently.
From these files a series of measures were derived as follows.
1. Demographic data: age, gender, date of birth, date of death, ethnicity (Caucasian, Maori, Pacific peoples), geographical place of residence (North Island, South Island), territorial local authority.
2. Circumstances of death: method of suicide, presence of a suicide note, suicide site, post-mortem and toxicological examination.
3. Psychosocial circumstances: living arrangements (with/not with intact biological family), social welfare care.
4. Physical and mental health history: physical health problems, prior threats of suicide, previous suicide attempt, family history of suicide, mental health problems, recent mental health care.
5. Psychosocial stresses or precipitants: disciplinary crisis, school problems, argument with family member, recent death of close family member.
Results
Demographic description
During the 10-year period from 1989 to 1998 a total of 61 children and young adolescents aged less than 15 years died by suicide in New Zealand. Table 1 shows the number and rate of deaths each year. Suicide in this age group is extremely rare. On average, there were six suicides each year. However, the number of such deaths seems to be increasing. During the 5 years from 1989 to 1993 there were an average 4.2 deaths each year, whereas, for the most recent 5-year period, 1994–1998, there were, on average, eight deaths each year. In 1998 (most recent data) there were 12 deaths.
Numbers and rates of suicides aged less than 15 years
Figure 1 shows under 15-year-old suicides by age and gender. The risk of suicide increases with increasing age for both males and females, with more than twice as many deaths among 14-year-olds (57.4% of the total) than 13-year-olds (26.2%). The clear majority of deaths (83.6%) were aged 13 or 14 years. Suicide was extremely rare among those aged 12 and younger. Suicides were overwhelmingly male (72.1%). The male: female ratio was 2.8:1. No girls younger than 12 died by suicide in the 10-year period.
Age and gender of suicides aged less than 15 years (1989–1998). ▪, boys; □, girls.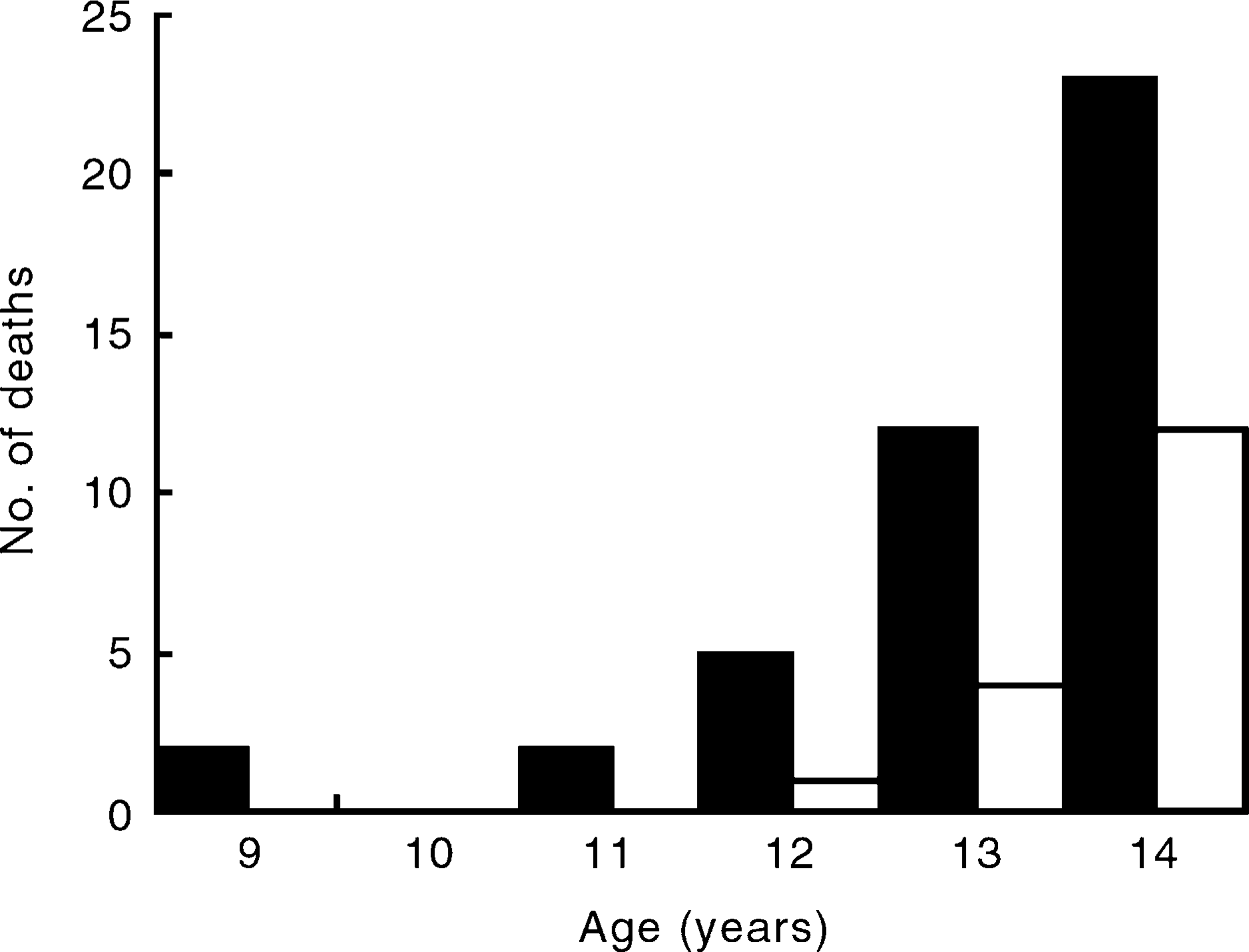
Table 2 summarizes selected demographic and risk features of those who died. The majority were Maori (57.4%); 26.2% were Caucasian and 6.6% were Pacific peoples. Ethnicity was not recorded in just under 10% of cases. Of females who died by suicide, 64.7% were Maori; of males, 54.6% were Maori.
Rates (%) of demographic and risk features of suicides aged less than 15 years
Changes in recording ethnicity during the 10-year study period preclude comparison of Maori and non-Maori suicide rates for the entire period. However, 1997 data suggest that the Maori rate of suicide in the 10–14 years age group was 6.6 per 100 000 (males, 9.7; females, 3.4); by comparison, the rate of suicide for the total population aged 10–14 years was 2.9 per 100 000 (males, 3.6; females, 2.3).
Most deaths occurred in the North Island (88.5%). In total, 75% of New Zealanders live in the North Island. Four Territorial Local Authorities recorded five or more young adolescent suicides during the 10-year study period: Manukau and Franklin in South Auckland, Napier and Lower Hutt. This high North Island representation is also reflected in the large proportion of Maori child deaths: most Maori (87.5%) live in the North Island.
Method of suicide
Hanging was, overwhelmingly, the most common method of suicide (78.7%). Firearms accounted for six (9.8%) deaths, and poisoning accounted for a further five (8.2%) deaths.
Circumstances of the death
The majority of suicides took place at the child's place of residence (86.9%), often when family were present in the house or on the property. Of all deaths, 32.8% occurred in the house, 26.2% in garages and 27.9% occurred outside.
One-third of children (32.8%) left suicide notes. The content of these notes usually included a reason or explanation for the suicide. Often the young person indicated that they believed they were going to a better place, sometimes to be with a family member who had died. The content of notes often suggested that the child had had an unhappy life. Comments included the following: ‘I've had an unhappy life. People have been waiting for me to die’, ‘I feel unwanted by people’, ‘I've gone to a special place where I can live happily with my father’, ‘I'll never leave you in your time of misery’, ‘I am going to where my father is. It will be a better place than this’.
Five of the 61 deaths appear to have involved suicide pacts or groups. The five involved in pacts were all females.
Post-mortem examinations were conducted in most cases (90.2%), but toxicological investigations were conducted less often (27.9%), and usually, only in cases where it was suspected that the child had taken an overdose. Toxicology to check for the presence of psychoactive drugs including, in particular, alcohol or cannabis, was not undertaken routinely.
Psychosocial circumstances
Only one-third of those who died were living with intact biological families (32.8%). A significant minority (45.9%) were living in single parent or stepparent families; six (9.8%) were living with relatives (grandparents or aunts or uncles); two were in social welfare homes. The living arrangements were not recorded for five children.
Those who died had a high rate of contact with child welfare authorities. These data were not recorded consistently in coronial files, but the names of those who died were checked against the Department of Child, Youth and Family Services (CYFS) database and the available information suggested that one in four (24.6%) of those who died had a current or lifetime history of contact with social welfare authorities. This is likely to be an underestimate. Some children were State wards under the guardianship of the Department of Social Welfare at the time of their death. In addition, records indicated that at least another eight children were receiving care from adolescent mental health services or counselling from school guidance counsellors at the times of their deaths. Taken together, these findings suggest that at least one in three (37.7%) of the children who died were known to school, mental health and/or welfare authorities to have significant problems.
In a number of cases it appeared that children who died by suicide had suffered recent family deaths. While these data were not recorded consistently and are likely to be a significant underestimate, records indicated that at least one in seven (14.8%) had experienced the deaths of siblings, parents or close relatives. A family history of suicide (in a parent, sibling or cousin) was noted in at least six cases (9.8%), and in one case, a child recreated his brother's suicide, using the same method and place.
In several cases it appeared that a child suicide death followed, within 2 to 3 weeks, a similar child suicide death within the neighbourhood.
Few children appeared to have significant physical health problems at the time of their death. Several were noted to have had academic and learning difficulties at school. Data relating to substance-abuse problems were recorded infrequently. At least 10 (16.4%) children were reported to have had care for mental health problems from general practitioner, school counselling and/or mental health services. Eight (13.1%) children were noted to have made prior suicide attempts. One in four (23%) was reported to have made threats of suicide within the year prior to their death.
In most cases (70.5%) the immediate precipitant to the suicide was recorded as being an argument with a family member (usually a parent or parent figure) and/or a disciplinary crisis (26.2%). In most cases, these arguments appeared to be about relatively minor issues, not significantly different in type or severity from usual disagreements for children of this age. However, it was notable that, in most cases, these arguments occurred in the context of a disruption (actual or threatened) or transition in the child's living or schooling arrangements or in the context of serious family problems. Typical situations included, for example, transition from social welfare care to home, from the care of one parent to another (when these parents were living apart), removal or suspension from school, or changing schools. The clear impression was that the seemingly trivial argument or crisis provoked an extreme reaction (suicide) in disadvantaged and troubled children with few or fragile family and social supports and affiliations, particularly when these supports were threatened. Often these suicide attempts appeared impulsive, with few children appearing to take precautions against being discovered (in contrast to adult suicide deaths) and many took place in the family home while family was present.
In cases where there was no indication of an immediate precipitant to the suicide, records indicated that the deaths tended to occur in the context of recent family deaths, mental health problems, family transitions, or knowledge of suicide by another child or by a family member.
Discussion
Bearing in mind the limitations of the data, this paper sought to describe, in a preliminary way, the features of recent young adolescent suicide deaths in New Zealand, given emerging concerns about increased numbers of such deaths.
The profile of risk that emerged was of a young adolescent male, Maori, not living with both biological parents, often with social welfare involvement, who made an impulsive suicide attempt, most often by hanging, in the context of age-normative precipitants, most commonly an argument with a parent or parent figure, or a disciplinary crisis. Compared with older youth (15–24 years) younger adolescents who die by suicide appeared less likely to have mental health problems [14–19].
The predominance of Maori in child suicide statistics stands in contrast to the predominance of non-Maori in youth (15–24 years) suicide. In 1998 only 30% of the total number of youth suicides were Maori, whereas 57% of young adolescent suicides in this study were Maori. There is a need for further investigation of the Maori predominance in young adolescent suicide.
Throughout the data there are clear hints which suggest that the population of young adolescents who die by suicide frequently come from extremely disadvantaged and problematic family backgrounds. This view is supported, for example, by the clearly disproportionate number of children who were in contact with social welfare authorities. This view was also reinforced by reading of the incidental material gathered during the course of this investigation and particularly the suicide notes of children. These notes frequently conveyed the impression of extremely distressed and vulnerable children being reared in very difficult circumstances. There is a need to verify these impressions with an in-depth investigation of the familial, social and mental health circumstances of young adolescents who die by suicide.
The findings of this study are consistent with previous reports to the extent that the majority of those who died were male, died by hanging and tended to make impulsive attempts in the context of family arguments or crises [2], [3], [5], [11],[13–19]. However, this study conveys the clear impression, more than most previous reports, that those at risk tend to come from problematic family situations characterized by impaired child-rearing practices. In this respect the present study yields a risk profile which closely resembles that described for child and young adolescent suicide in Australia [8–9]. These findings are consistent with the concept of the ‘expendable child’ described by Sabbath [21]. Sabbath suggested that the immature cognitive functioning style of children makes them vulnerable in times of family stress to the (egocentric) view that their families will be better off without them. Children in problematic families which are exposed to multiple and severe stresses and are unable to provide a supportive environment may respond to stress poorly, impulsively, and, in extreme cases, with suicidal behaviour [21], [22].
The relatively small but conspicuous group of disadvantaged children and young adolescents in social welfare care is at particularly high risk of suicide. These findings provide a strong argument for strengthening mental health services, targeting suicide prevention services and monitoring suicide risk among youth that are receiving welfare services.
Most deaths occurred by hanging. As might be expected, given their age and the limited range of methods available, the proportion of deaths by hanging for children (78%) was higher than has been found for 15–24-year-olds (60%) [23]. The predominance of hanging and the ubiquitous availability of the means for hanging pose severe limitations on the extent to which restricting access to means of suicide can be an effective approach to reducing suicide in this age group. Nevertheless, it remains a best-practice recommendation that responsible adults should remove any apparent means of suicide in cases where a young adolescent is perceived be at risk of suicide.
Previous studies have suggested that there may be, in some cases, an unwillingness to classify some deaths in children and young adolescents as suicides, with the view that children are incapable of formulating concepts of death and suicide [10], [24], [25]. More generally, there is broad acceptance that child suicide statistics are probably underrecorded because of such beliefs [10],[24–26]. The notes left by the children in this study clearly indicate the intent of their action, and their awareness of suicide and death. While some caution needs to be attached to the findings of this uncontrolled study, nevertheless, they suggest that talk or threats of suicide among children and young adolescents should be regarded seriously and there should be clear recognition among caregivers, teachers, counsellors and others that children of this age know enough about suicide to commit suicide, although they may not clearly appreciate the finality and permanence of death [25].
Most of those aged less than 15 who die by suicide are young adolescents aged 13 and 14 years. This suggests that the term ‘child suicide’, used commonly, is misleading and should be avoided. It seems more appropriate to report official numbers and rates of such deaths for the age band ‘10–14 years’ rather than the often used ‘0–14 years’, or ‘5–14 years’, in order to convey more accurately the age group most at risk.
The death of a child or young adolescent by suicide is a devastating event for families [26–27]. While there is an obvious need for police inquiries of such deaths (since children are vulnerable and homicide needs to be excluded), there is also a need to establish, parallel to police investigations, protocols for conducting, first, an inquiry into the circumstances of the death (including family composition, living arrangements, school circumstances, involvement with mental health and welfare services, precipitants to the suicide) by gathering data from family, welfare, school and other relevant authorities. Second, there is a need to provide support to parents, families, schools and communities in the aftermath of such deaths. Because young adolescent suicide deaths occur so rarely it is unlikely that most police or coroners will have established protocols to deal with such cases. There is a need to develop a protocol for child and youth suicide deaths which integrates these three strands of police inquiry, psychological autopsy and postvention support.
Systematic data collection for coronial inquiry would assist in further study of young adolescent suicide deaths. While, currently, the quality and extent of information contained within coronial files is highly variable, improved, systematic collection of data at the point of coronial inquiry probably represents the best opportunity to examine and monitor young adolescent suicide deaths. The small population base of New Zealand, together with the rarity of young adolescent deaths, limits the type of studies that may be undertaken to clarify the preliminary findings of this report. A psychological autopsy study, for example, in which information was obtained from interviews with parents, doctors, teachers and others, would be required to run over many years, and nationally, in order to collect an adequate number of cases. The best opportunity for further study of these cases might be provided by conducting an annual mortality review or audit of the suicide death of each child aged less than 15 years with this review conducted by examination of coronial files by a committee which includes a suicidologist, paediatrician, a child and adolescent psychiatrist, a coroner and a representative of child welfare services. The current review of coroners and the proposed establishment of a coronial database may facilitate the development of such an approach in New Zealand.
There are two caveats that need to be placed on the findings of this study. First, the results are based on a relatively small number of cases and this clearly limits the precision of the analysis. Second, the study lacks a comparison group of non-suicidal control subjects. Ideally a stronger research design would involve a case–control study in which children and young adolescents who die by suicide are contrasted with a comparable series.
It is important to recognize that suicide is a very rare event in children and young adolescents. Nevertheless, the results of this study suggest that if we are to stem an apparently rising rate of suicide in this age group we will need to make strong efforts to ensure that young adolescents (and particularly those most disadvantaged, distressed and vulnerable) receive the adequate and supportive care and protection to which their youth entitles them.
Footnotes
Acknowledgements
The assistance of the Department of Courts, the New Zealand Health Information Service, and Child, Youth and Family Services is gratefully acknowledged.