
Abstract
Suicide prevention is an important issue for many countries, including New Zealand and Australia [1–4]. One approach to reducing suicide focuses on restricting access to potentially lethal means of suicide. A specific focus of many societies has been upon the restriction of access to firearms. This issue has been important in the USA where the majority of suicide deaths are the result of firearms [5, 6]. The availability of firearms may also play a significant role in suicidal behaviour among young people [7–9]. Young people with impulsive aggression, for example, have increased risks of suicidal behaviour [8, 10, 11] and restricting access to firearms may prevent impulsive suicide attempts made in situations of anger or distress.
Within New Zealand issues relating to access and storage of firearms were the subject of legislative change in 1992. Specifically, the Amendment to the Arms Act, 1992 [12] changed regulations involving access to firearms from a more liberal to a more restrictive regime. The history of these changes is as follows: In 1990 in New Zealand a lone gunman killed 13 people with a military-style semi-automatic (MSSA) weapon at Aramoana. In the late 1980s concern had grown about the adequacy of the existing legislation to take account of the increasing ownership of MSSAs, particularly in light of the use of these weapons in mass killings overseas. The Aramoana massacre led to a call for more restrictive firearms controls, and an amendment to the Arms Act was enacted on 27 October 1992, coming into force on 1 November 1992. Therefore, since 1992, in efforts to restrict the access of unsuitable people to firearms, the following provisions apply [12]: All firearms owners must have a photo-identified firearms licence that is valid for 10 years and must then be renewed. This licence is issued after: (i). the applicant has passed (with a score of at least 90%) a test of their knowledge of the Firearms Code (which describes regulations governing firearms ownership, use, safety and storage); (ii). the applicant achieves a 100% score on knowledge of seven basic rules of firearm safety; (iii) the applicant is assessed by the police as being a ‘fit and proper’ person to hold a firearms licence. (As part of this assessment, police interview, confidentially, two referees, including a partner or parent, and inspect the applicant's home to check firearm storage, security and social arrangements).
The Amendment also introduced more stringent security requirements for firearms to be kept in lockable cabinets or strongrooms, with these to be locked at all times when firearms are not in use. Ammunition is to be stored separately from guns, and ammunition is not to be sold to those not holding firearms licences.
Although there is no legal provision for a ‘stand-down’ period after application for a firearms licence, the requirements for referee interviews and home inspections effectively mean that licence applications typically take from 8 to 12 weeks to be granted. Restrictive, ‘endorsed’ licences are required by firearms dealers, collectors, owners of MSSAs and handguns. Only approximately 3% of all firearm licences are endorsed in this way. With the exception of these endorsed licences, handguns are illegal and the vast majority of firearms in New Zealand are long-barrelled rifles that are used for hunting, pest destruction or on farms. Recent estimates suggest that approximately 225 000 of New Zealanders (total population, 4 million) hold firearms licences [13].
The changes in legislation in 1992 provide a natural experiment that makes it possible to examine the impact of more restrictive legislation on rates of suicide, and particularly, on firearms-related suicides. This paper addresses these issues by:
Comparing rates of suicide by firearms before, during and after the implementation of the Amendment to the Arms Act, 1992. Examining the extent to which any changes in firearm-related suicides were evident for both youth (< 25 years) and adults (≥25 years). Examining the extent to which associations between changes in firearms legislation and changes in firearm-related suicides persisted after adjustment for trends in suicide. Exploring the extent to which any reduction in firearm-related suicides was evident in overall suicide rates.
Method
Assessment of changes in legislation
This study covers the 18-year period from 1985 to 2002. The major legislative change [12] came into force on 1 November 1992. Following the introduction of this legislation, concerns were expressed by New Zealand police about the need for resources to fully implement this law change because it required the relicencing of all licence holders [13]. This issue was addressed in a commissioned report reviewing firearms controls in New Zealand [13]. By most accounts, it would appear that, by the end of 1996, the legislative changes of the 1992 Amendment had been substantially implemented. Thus, for the purposes of this analysis, the period from 1985 to 2002 is divided into three epochs:
(1) 1985 to 1992 is the epoch prior to legislation; (2) 1993 to 1996 is the epoch of implementation; (3) 1997 to 2002 is the epoch of post-implementation.
Assessment of outcomes
To assess the outcomes of the legislative change data were gathered on the numbers of suicides in New Zealand over the period from 1985 to 2002 using information provided by the New Zealand Health Information Service (NZHIS) (pers. comm.). In addition, NZHIS supplied information about the age and gender distribution of all suicides (from all causes) for each year from 1985 to 2002.
Statistical analysis
Age-specific suicide rates per 100 000 of population were calculated for firearm-related suicides, non-firearm-related suicides and total suicides using population estimates obtained from Statistics New Zealand for the years 1985–2002. Separate estimates were calculated for youth (15–24 years), adults (25+ years) and the total population aged 15+ years. To test the effects of firearms legislation on the rate of firearmrelated suicide (Figure 1) the following model was fitted to the data for each population (youth, adult, total population):
Annual rates of firearm-related suicides, 1985–2002. (a) Total population 15+ years. (b) Youth 15–24 years. (c) Adults 25+ years.
To test for period effects in the overall rate of suicide following firearms legislation the overall suicide rates for each population (Figure 3) were modelled using a Poisson regression model of the form:

Finally, to further examine the extent to which changes in firearms legislation were associated with changes in the overall rates of suicide a series of alternative models were fitted to the data in Figure 3. These models included:
(a) A forecasting model. A time series model of the form
(b) A polynomial model. In this model overall rates of suicide were modelled as a quadratic function of time and measurement period to test whether period effects associated with changes in firearms legislation were apparent over and above broad time trends in overall suicide rates. This model was of the form,
(c) An auto-regressive model. In this model the overall rate of suicide in year t was modelled as a function of period and the rate of suicide in year t − 1,



The above models were fitted using both rate data and log rate data. All models were fitted using Stata 8 [14].
Results
Time trends in rates of firearm suicides
Figure 1 shows the annual rates of firearm suicides per 100 000 of population for the periods 1985–1992 (pre-legislation), 1993–1996 (legislation implementation) and 1997–2002 (post-implementation). Separate graphs are shown for youth (aged 15–24 years), adults (aged 25+ years) and the total population (aged 15+ years). Inspection of the figure shows that for all three populations there was clear evidence of a decline in firearm-related suicides following the introduction of the 1992 firearms legislation. This trend is most marked for youth suicide where prior to the legislation the average rate of firearm suicides was 3.8 per 100 000 of population, with this reducing to an average rate of 1.4 per 100 000 in the post-implementation period.
The contribution of firearm suicides to the overall suicide rate
Figure 2 shows the numbers of firearm suicides over the period 1985–2002 expressed as a fraction of the overall number of suicides in each year. Separate data are presented for youth, adults and the total population aged 15+ years. The figure shows the presence of a clear trend of decline in the contribution of firearm suicides to the total number of suicides following the 1992 firearms legislation. Prior to this legislation firearm deaths accounted for 18% of all suicides, whereas in the post-legislation period (1997–2002), firearm suicides accounted for 10% of all suicides. Again, these trends appear to be most marked for youth suicides.
Firearm-related suicides as a fraction of all suicides, 1985–2002. (a) Total population 15+ years. (b) Youth 15–24 years. (c) Adults 25+ years.
Modelling the effects of firearm legislation on the rates of firearm suicides
The results in Figures 1 and 2 clearly suggest that the introduction of the 1992 firearms legislation led to a detectable reduction in firearm suicides. To test this hypothesis a time series model was fitted to the data in Figure 1 (see Methods). This analysis modelled the annual rates of firearm suicide per 100 000 of population as a log linear function of (a) the annual rate of non-firearm suicides and (b) time period (i.e. pre-legislation; implementation; post-implementation). Separate models were fitted for youth, adults and the total population. The results of these analyses are summarized in Table 1, which shows model coefficients, standard errors and tests of significance for each model. The following conclusions may be drawn from this table.
Youth firearm suicide rates. The fitted model suggests that, independently of trends in non-firearm suicides, there were significant reductions in the rates of firearm suicide in the implementation (B = −0.50; SE = 0.23; p < .05) and post-implementation (B = −1.09; SE = 0.24; p < 0.001) periods. The model coefficients imply that, when compared with the prelegislation period, rates of firearm suicide were reduced by 39% in the implementation period and by 66% in the post-implementation period.
Adult firearm suicide rates. The model coefficients show that for adults there were significant reductions in the rate of firearm suicides in both the implementation period (B = −0.29; SE = 0.13; p < 0.05) and the post-implementation period (B = −0.49; SE = 0.08; p < 0.001). The model coefficients imply that, when compared with the pre-legislation period, the rates of firearm suicide were reduced by 25% during the implementation period and by 39% during the post-implementation period.
Total firearm suicide rates. Consistent with the findings for youth and adult firearm suicides, the model coefficients also show the presence of significant reductions in rates of firearm suicide in the total population for both the implementation (B = −0.35; SE = 0.15; p < 0.05) and post-implementation (B = −0.62; SE = 0.09; p < 0.001) periods. The model coefficients imply that, when compared with the pre-legislation period, the rates of firearm suicide in the total population were reduced by 30% during the implementation period and 46% during the post-implementation period.
Fitted model coefficients for firearm suicide rates.
Effects of firearm legislation on overall rates of suicide
Figure 3 shows the overall rates of suicide from all causes per 100 000 youth, adults and the total population aged 15+ years over the period from 1985 to 2002. Inspection of these graphs shows:
Youth rates. There was a general trend for total rates of suicide to increase during the pre-legislation and implementation periods but to show a decline during the latter part of the post-implementation period (after 1998).
Adult rates. Rates of suicide remained almost unaltered from the pre-legislation to implementation and post-implementation periods.
Total rates. There was a slight trend for overall rates of suicide to increase during the implementation of the firearms legislation and to reduce again to pre-legislation levels during the post-implementation period. Annual rates of suicide from all causes, 1985–2002. (a) Total population 15+ years. (b) Youth 15–24 years. (c) Adults 25+ years.
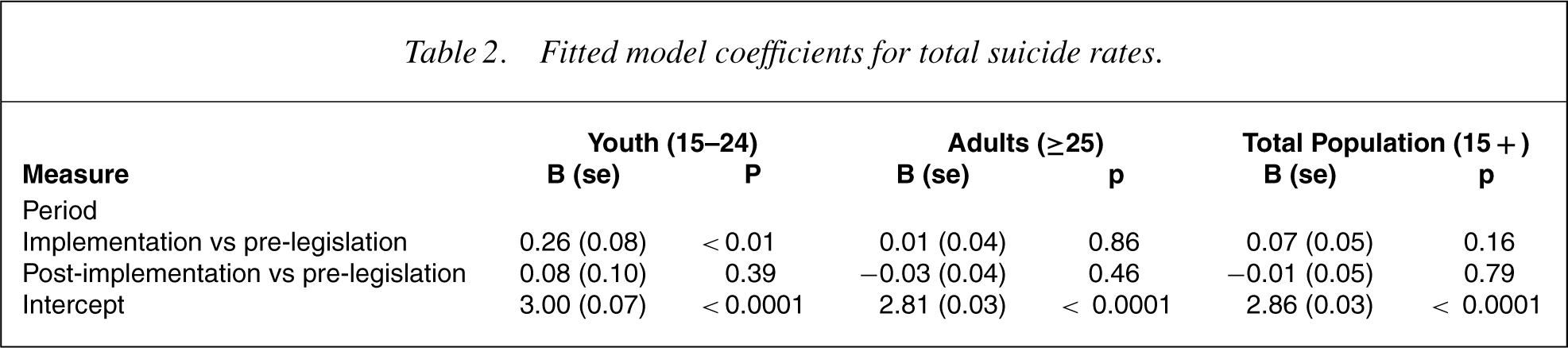
To examine the extent to which trends in overall suicide rates varied with period, time series models were fitted to the data in Figure 3. In these models the overall rate of suicide per 100 000 of population was modelled as a log-linear function of time period (pre-legislation; implementation; post-implementation). The results of these analyses are reported in Table 2, which shows model coefficients, standard errors and tests of significance. The analysis showed that for youth there was a significant increase in the total rate of suicide during the implementation period (B = 0.25; SE = 0.08; p < 0.01); however, total suicide rates in the post-implementation period were not significantly different from the pre-legislation period. For both the adult and total population analyses period was unrelated to overall rates of suicide. Therefore the trends evident for changes in firearm suicide rates following the firearms legislation were not directly translated into corresponding changes in overall rates of suicide.
Fitted model coefficients for total suicide rates.
To further examine the extent to which changes in firearm legislation may have produced changes in overall rates of suicide a series of models was fitted to the data in Figure 3. These models included:
(a) A forecasting model in which rates of suicide in the implementation and post-implementation periods were predicted from time trends in the pre-legislation period. (b) A polynomial model in which the overall rates of suicide were predicted using a polynomial function of time and a period variable. (c) An auto-regressive model in which the overall rate of suicide at time t was predicted from period and the rate of suicide at time t − 1.
All of these analyses failed to show any evidence to support the view that changes in firearms legislation had a detectable effect on overall rates of suicide.
Discussion
The results of this study provide strong support for the view that the introduction of the 1992 legislation had a significant impact on firearm-related suicides in New Zealand. Prior to this legislation there were almost 80 firearm suicides per annum. After legislation, this reduced to 52 suicides per annum. These trends were most marked for youth but were also evident for adults.
It is unlikely that the reduction in firearm-related suicides could be explained by trends in overall suicide rates because analysis suggested that following legislation there was a significant reduction in firearm-related suicide deaths as a fraction of all suicides. Irrespective of these issues of causation, it is quite clear that following the introduction of more restrictive firearms legislation, the rates of suicide by firearms reduced significantly in the face of a general trend for overall rates of suicide to increase.
There are some possible limitations of these findings. First, whereas the present study suggests that wellenforced restrictions of access to firearms may reduce suicides involving firearms the impact of these changes on overall suicide rates is not significant in this analysis. In particular, it could be suggested that the reduction in the rates of firearm-related suicides was associated with increases in the use of other methods as a result of method substitution in which restricted access to firearms led those attempting suicide to substitute other methods. However, given the available data (in particular, firearmrelated suicides constituted only 10% of all suicides by the end of the post-implementation period) it is not possible to test the extent to which substitution may have occurred. Second, the study does not include potential confounding variables (e.g. the introduction of selective serotonin reuptake inhibitors [SSRIs]); therefore it is not possible to explore the extent to which other time-related trends may have obscured the impact of the 1992 firearm legislation changes. Third, there is a need to be cautious in generalizing these results to another country's context. Specifically, the pattern and culture of firearm ownership in New Zealand is very different from that, say, in the USA, with New Zealand laws prohibiting ownership of handguns with the result that all legal firearms in New Zealand are long-barrelled rifles. For this reason the extent to which findings concerning the regulation of longbarrelled rifles can be generalized to handguns remains open to question.
The study fails to rule out alternative explanations for the decline in firearm-related suicides. Reasons for this include: (i) there is no suitable comparison group because the legislationwas applied to the total New Zealand population; (ii) multivariate analysis to control for confounders could not be conducted because relevant data (such as change in income or access to mental health services) were not available on suicide death certificates.
Nonetheless, within these limitations, the findings of this study are consistent with the view that the 1992 legislation, which restricted access to firearms, had the effect of decreasing access to firearms, and reducing firearm-related suicides. These findings add to a growing body of evidence that suggests that the regulation of firearm access may have positive effects in reducing use of firearms in impulsive suicide attempts, particularly by young males [15–25].
Consistent with findings from other studies, it appears that reductions in firearm-related suicides were not accompanied by parallel reductions in the overall suicide rate. These findings underscore the fact that restricting access to means of suicide should be viewed as an adjunct to suicide prevention approaches that focus on improving the identification, treatment and management of the psychiatric disorders that are the precursors to suicidal behaviour.
Footnotes
Acknowledgements
The Canterbury Suicide Project has been funded by grants from the Health Research Council, and supported by the Canterbury Area Health Board and Healthlink South. For this paper, the assistance of the staff of the New Zealand Health Information Service and of Inspector Joe Green, New Zealand Police, is gratefully acknowledged.