
Abstract
Objective:
A population health approach to mental health service planning requires estimates that align interventions with the needs of people with mental illness. The primary objective was to estimate the number of people in Australia living with severe and persistent mental illness who have complex, multi-agency needs. The secondary objective was to describe the possible service needs of individuals with severe mental illness.
Methods:
We disaggregated the estimated 12-month prevalence of adults with severe mental illness into needs-based sub-groups, using multiple data sources. Possible service needs of 1825 adults with psychotic disorders and 334 adults with severe past-year affective and/or anxiety disorders were described using data from the 2010 Survey of High Impact Psychosis and 2007 National Survey of Mental Health and Wellbeing, respectively.
Results:
Using best available data, we estimated that 3.3% of adults experience a severe mental illness each year, of whom one-third (1.1% of adults) experience a persistent mental illness that requires ongoing services to address residual disability. Among those with severe and persistent mental illness, one-third of adults (0.4% or 59,000 adults in 2015) have complex needs requiring multi-agency support to maximise their health, housing, social participation and personal functioning. Survey of High Impact Psychosis data indicated that among adults with psychotic disorders, use of accommodation (40%), non-government (30%) services and receipt of income support (85%) services were common, as were possible needs for support with socialising, personal care and employment. National Survey of Mental Health and Wellbeing data indicated that among individuals with severe affective and anxiety disorders, receipt of income support (37%) was common (information on accommodation and non-government support services was not available), as were possible needs for financial management and employment support.
Conclusion:
Agreed indicators of complex, multi-agency needs are required to refine these estimates. Closer alignment of information collected about possible service needs across epidemiological surveys is needed.
Introduction
International mental health reform has continued over the past 50 years (Adams et al., 2009), with the most notable changes being the shift in the organisation and delivery of mental health services from institutional care to community-based services (Fakhoury and Priebe, 2007). In Australia, this reform started in the 1950s at a state level, with coordination at a national level from 1992 with the introduction of a National Mental Health Strategy (Whiteford, 1992). From early in the Strategy, the need to provide not only clinical but also a range of non-clinical services including housing, vocational training, social and disability supports for those with significant psychiatric disability was recognised (Whiteford, 1994). However, attempts to provide coordinated clinical and support services for persons with severe and persistent mental illness have been compromised by the involvement of multiple levels of government and funding bodies with poor inter-agency collaboration (Mental Health Council of Australia, 2005). Individuals with severe and persistent mental illness with complex, multi-agency needs present the greatest challenges for coordinated delivery of mental health treatment and intensive support services and require a complex care planning response (Council of Australian Governments, 2006). However, there is little information available to clearly define this group and estimate its size in Australia.
In population surveys, it is common to consider the severity of a mental illness, and this can include defining those with diagnoses of mental illness as mild, moderate and severe. In the most commonly used survey instrument, the World Mental Health Composite International Diagnostic Interview (CIDI), severity is defined using an algorithm developed by the World Mental Health Survey Initiative. In the most recent Australian survey using the CIDI (Slade et al., 2009a), to be classified as severe required meeting criteria for a 12-month mental disorder plus one of the following in the previous 12 months: an episode of mania, a suicide attempt, at least two areas of severe role impairment on the disorder-specific Sheehan Disability Scales (Buist-Bouwman et al., 2008) or overall functional impairment at a level equivalent to a Global Assessment of Functioning (GAF) score of 50 or below (Kessler et al., 2005). Classification as moderate required a 12-month mental disorder and moderate role impairment for one domain on the Sheehan Disability Scales. Other cases of 12-month mental disorder were categorised as mild.
Individuals with severe mental illness are a diverse group with a range of different service needs. For planning purposes, it is useful to differentiate sub-groups based on need. Some have severe but episodic mental illness, with periods of remission or minimal symptoms between acute episodes. For others, illness is persistent, with a chronic, disabling course. Some of this latter group may live with their families or in long-term private residential care. Others, however, have disengaged from social or family networks and require not only clinical treatment but also extensive support from public disability services to maintain their lives outside of institutional care, including accommodation, clothing, food and vocational assistance (Whiteford, 1994). This sub-group of individuals has been referred to as having a ‘severe and persistent mental illness with complex needs’, services for which are often delivered by multiple agencies.
There have been numerous attempts to define severe and persistent mental illness. The US National Institute of Mental Health (NIMH) developed a definition of severe mental illness that incorporates the diagnosis, symptom intensity and duration, and the degree of disablement caused to social, personal and occupational functioning (National Advisory Mental Health Council, 1993). Individuals with certain diagnoses such as schizophrenia are automatically classified as severe, and others such as those with past-year major depressive disorder require additional indicators of severity such as psychiatric hospitalisation in the past year. In the Unites States, ‘severe and persistent mental illness’ was first defined in the Wisconsin statutes and repeated in subsequent legislation (Government of Wisconsin, 2014). According to this definition, severe and persistent mental illness means
a mental illness which is severe in degree and persistent in duration, that causes a substantially diminished level of functioning in the primary aspects of daily living and an inability to cope with the ordinary demands of life, that may lead to an inability to maintain stable adjustment and independent functioning without long-term treatment and support and which may be of lifelong duration. (Government of Wisconsin, 2014: 2)
Others have attempted to describe this group according to a diverse range of clinical and other needs including for disability support services. For example, in the United Kingdom, individuals eligible for an Enhanced Care Plan may be identified by a range of characteristics, including clinical mental health service needs (such as a high risk of relapse and associated history of multiple hospitalisations, a history of long-term (>1–2 years) contact with services, contact with child and adolescent mental health services, difficulty engaging with services, detainment under a Mental Health Act, frequent co-morbid substance use and a risk of self-harm or violence towards others); social support service needs (such as significant impairments in social, personal and occupational functioning that require intensive, ongoing support; an absence of functional family and social support networks; and significant reliance on a carer); housing and employment support service needs (such as homelessness or unstable housing, and reliance upon housing and employment agencies); and criminal justice service needs (Department of Health, 2008; The Sainsbury Centre for Mental Health [SCMH], 1998; UK Department of Health, 1990).
In Australia over the past decade, a number of Commonwealth government programmes have been implemented with the intended aim of addressing the fragmented service delivery system for people with severe and persistent mental illness – these include the Personal Helpers and Mentors Service (PHaMS) (Australian Government Department of Social Services, 2014) and Partners in Recovery (PIR) (Department of Health, 2012). To support the establishment of these programmes, estimates were made of the number of adults who have severe and persistent mental illness, and within this group, the proportion who have complex, multi-agency needs. The method described in this paper informed the estimates used in the design of these programmes. These estimates have subsequently been used elsewhere in Australia to quantify the need for mental health and community support services among persons with severe and persistent mental illness (Siskind et al., 2012), to guide the implementation of specialised community support services such as the Commonwealth Day-to-Day Living in the Community Programme (Healthcare Planning and Evaluation, 2010), to estimate the number of people likely to require individualised supports under Tier 3 of the National Disability Insurance Scheme (Productivity Commission, 2011) and to identify priorities for mental health system reform and reallocation of funds in the National Mental Health Commission’s (NMHC) (2014) National Review of Mental Health Programmes and Services report, in order to shift from high-cost care towards more coordinated, integrated packages of comprehensive support services.
The aims of this paper were
To estimate the number of adults living with severe and persistent mental illness who have complex, multi-agency needs,
To describe the possible service needs of individuals with severe mental illness to inform national mental health service planning efforts.
Methods
Estimating the number of adults living with severe and persistent mental illness who have complex, multi-agency needs
Estimates of the number of adults living with severe and persistent mental illness who have complex, multi-agency needs were obtained via a three-step modelling exercise drawing on multiple existing data sources. These data sources are summarised in Table 1.
Summary of source data for estimating the size of target populations with severe mental illness.
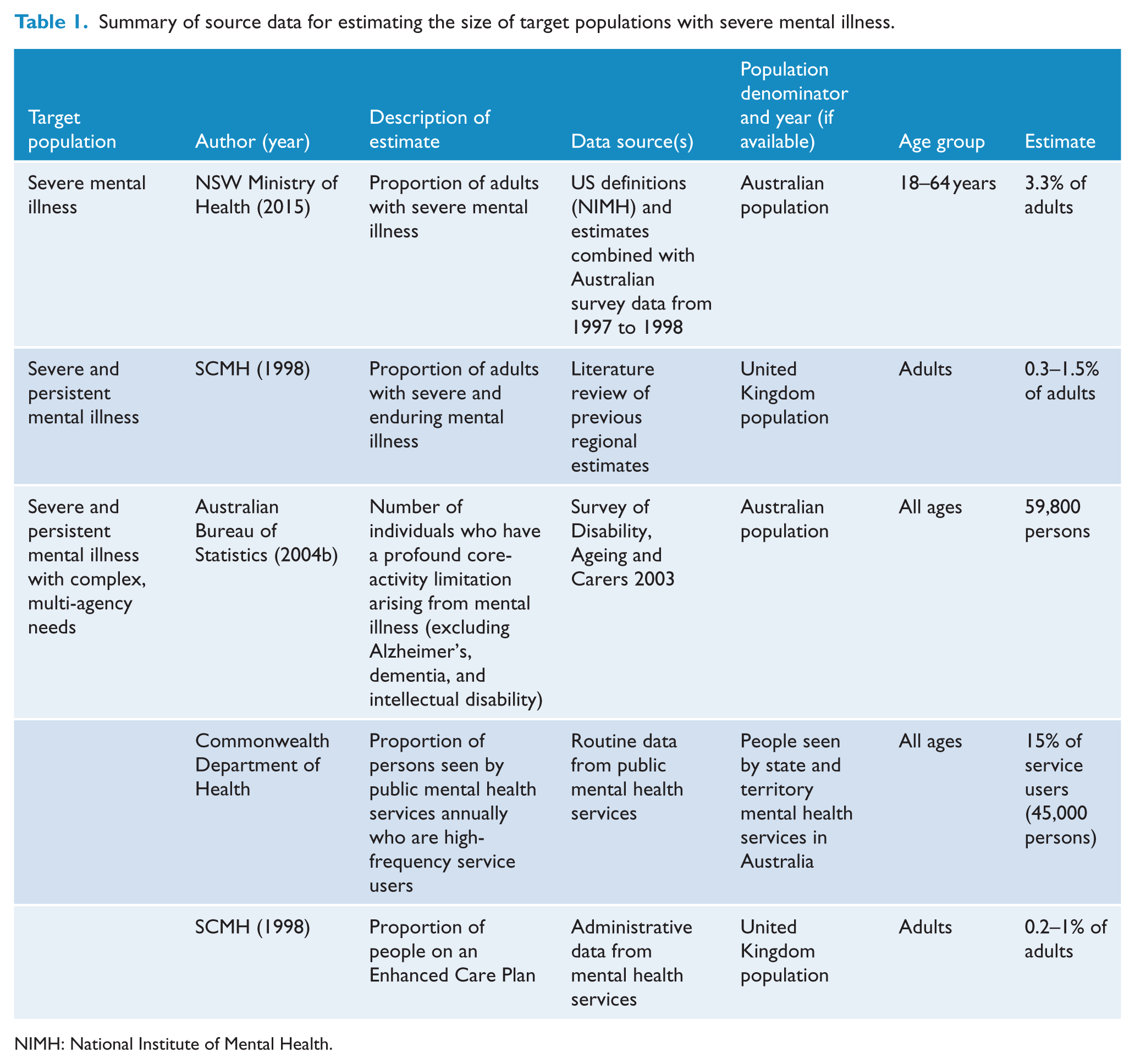
NIMH: National Institute of Mental Health.
Step 1. Estimating the size of the adult population with severe mental illness
Past-year estimates of the prevalence of severe mental illness in Australia, by age group (0–17 years, 18–64 years, 65+ years), were drawn from the National Mental Health Service Planning Framework AUSv1 (NMHSPF; NSW Ministry of Health, 2015). The NMHSPF prevalence estimates were based on a previous NSW planning model, which applied the NIMH definition of severe mental illness, described previously (National Advisory Mental Health Council, 1993). Within this definition, severity is judged according to the type of disorder the person has (diagnosis), the intensity of the symptoms they are suffering, the length of time they have experienced those symptoms, especially whether they have been present in the past 12 months, and the degree of disablement that is caused to social, personal and occupational functioning. Some diagnoses, particularly schizophrenia and other psychoses, are usually assigned to the severe category if they have been present in the previous year, but any disorder which has extreme impacts on an individual (e.g. as evidenced by a psychiatric inpatient admission, psychotic symptoms or a GAF scale rating of 50 or less) can be classed as severe. The NMHSPF prevalence estimates are based primarily on the Australian Burden of Disease study (AusBOD; Begg et al., 2007). AusBOD sourced estimates from Australian epidemiological surveys conducted in 1997–1998, supplementing these with overseas surveys to fill gaps in the diagnostic coverage of the Australian surveys. We converted NMHSPF prevalence estimates to number of people using the June 2015 Australian Estimated Resident Population (Australian Bureau of Statistics [ABS], 2016).
Step 2. Estimating the proportion of people living with severe mental disorders whose disorders are persistent
The definition for severe and persistent mental illness from the Wisconsin Statutes (Government of Wisconsin, 2014) was used to guide the estimation of the proportion of adults with severe mental disorders who have a persistent illness. Estimates were drawn from a number of sources, including international literature on the trajectories and long-term course of illness and functioning among persons with a severe mental disorder (Goldman et al., 1981; Harding et al., 1987; Warner, 1985), and a UK estimate of the number of adults with severe and enduring mental illness, based on a literature review of regional estimates (SCMH, 1998).
Step 3. Estimating the proportion of people with severe and persistent mental illness who have complex, multi-agency needs
Estimates of the size of the population of people with severe and persistent mental illness who have complex, multi-agency needs were drawn from a number of sources. These included the following:
The ABS 2003 Survey of Disability, Ageing and Carers (SDAC) estimate of the number of individuals who have a profound core-activity limitation (i.e. being unable to do, or always needs help with, a core-activity task, including communication, mobility or self-care; ABS, 2004a) arising from mental illness, excluding Alzheimer’s, dementia and intellectual disability (ABS, 2004a);
Analyses of individuals seen by state and territory mental health services (collated for National Mental Health reporting);
Estimates of the number of people on an Enhanced Care Plan in the United Kingdom (SCMH, 1998).
Describing the possible service needs of individuals with severe mental illness
We developed a description of the possible service needs of individuals with severe mental illness using published data and purpose-designed analyses of Australian epidemiological survey data. The absence of an agreed definition and criteria for severe, persistent and complex mental illness prevented the identification and analysis of a group that could be considered the same as that for whom the numbers were estimated in the first aim of this paper. However, a list of indicators of possible service needs was derived from defining characteristics of people with severe and persistent mental illness who have complex, multi-agency needs, as suggested in the literature. Suitable indicators were sought from each data source to match this list. The percentage of each sample who reported data consistent with these indicators was estimated.
To describe the possible service needs of adults with psychotic disorders, we sourced published data from the 2010 Survey of High Impact Psychosis (SHIP; Morgan et al., 2012). SHIP is a nationally representative survey of 1825 people aged 18–64 years with psychotic disorders who were in contact with state mental health services or mental health non-government organisations during the census month in 2010 or with state mental health services in the preceding year. Diagnosis of psychosis was determined according to International Classification of Diseases–10th revision (ICD-10) criteria using the Diagnostic Interview for Psychosis (DIP-DM) semi-structured clinical interview.
To describe the possible service needs of Australian adults with severe affective and anxiety disorders, we analysed data from the 2007 National Survey of Mental Health and Wellbeing (NSMHWB) (Slade et al., 2009b). The NSMHWB is a nationally representative household survey of 8841 Australian adults (60% response rate) aged 16–85 years conducted in 2007. Diagnoses of past-year affective disorders (depression, dysthymia and bipolar affective disorder) or anxiety disorders (panic disorder, agoraphobia, social phobia, generalised anxiety disorder, obsessive-compulsive disorder and post-traumatic stress disorder) meeting ICD-10 criteria were established using the World Mental Health Survey Initiative Composite International Diagnostic Interview (WMH-CIDI) 3.0. Severity of disorder (mild, moderate or severe) was determined using an algorithm based on disorder-specific role impairment and other clinical information, taking into account all disorders experienced in the past year (Slade et al., 2009b). For this paper, we focused on people aged 18–64 years. In the 2007 NSMHWB, 4.0% (95% confidence interval [CI] = [3.4%, 4.6%]; n = 334) of respondents in this age group met criteria for a past-year ICD-10 affective or anxiety disorder and were classified as ‘severe’.
We analysed 2007 NSMHWB Basic Confidentialised Unit Record File (April 2009) data using Stata, version 11 (StataCorp). Replicate weights were applied to the data to account for the differential probability of survey selection and to ensure conformity to known population distributions.
Results
Estimating the number of adults living with severe and persistent mental illness who have complex, multi-agency needs
A summary of the estimated number of Australians with severe mental illness, in total and disaggregated by type of need, is shown in Figure 1. Approximately 3.1% of the overall population had a severe disorder in a year, with a slightly higher rate (3.3%) among the adult population. An estimated 496,000 Australian adults had a severe mental illness in 2015.
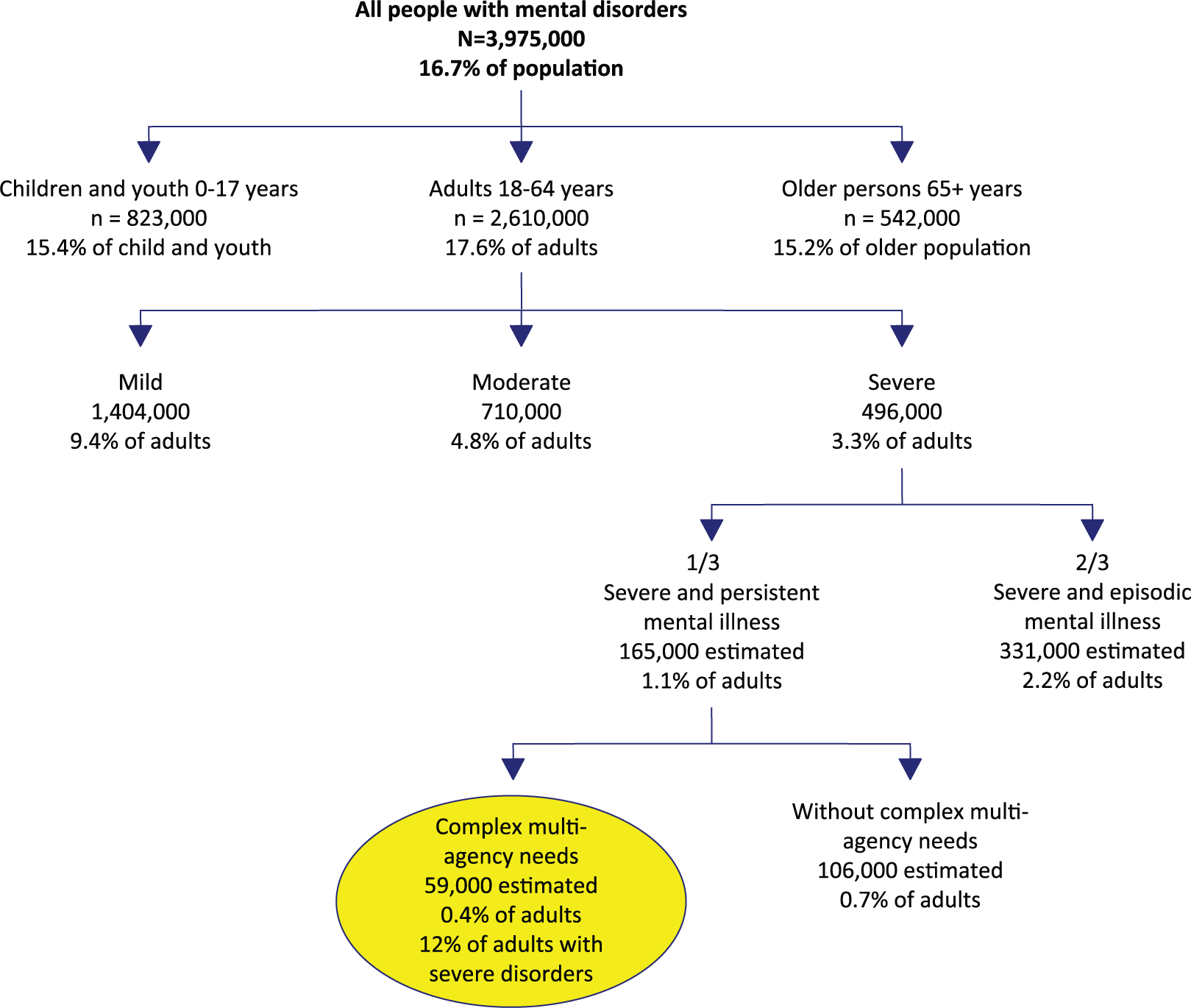
Summary of the estimates.
Approximately one-third of those with severe disorders (1.1% of the adult population, or approximately 165,000 Australian adults in 2015) were estimated to be affected by a severe and persistent mental illness that requires ongoing services. This split was drawn from a number of sources, including international estimates on the percentage of persons with a severe mental disorder who experience ongoing, persistent impairments in functioning, which range from 24% to 40% (Goldman et al., 1981; Harding et al., 1987; Warner, 1985). The estimate of one-third also draws on UK estimates suggesting that 0.3–1.5% of UK adults have ‘severe and enduring mental illness’ (SCMH, 1998).
Approximately 0.4% of the adult population, or 12% of adults with severe mental disorders and one-third of adults with severe and persistent mental disorders, were estimated to have a severe and persistent mental illness and complex, multi-agency needs. This group was equivalent to 59,000 Australian adults in 2015. This estimate was the best approximation based on combination of available source data. Data from the 2003 SDAC indicated that in 2003, there were 59,800 Australians with a profound core-activity limitation arising from mental illness (ABS, 2004b). Local studies of persons attending Australian state and territory mental health services suggested that 15% (n = 52,500) of individuals treated annually (n = 350,000) were high-frequency users of services (data provided by Commonwealth Department of Health). Finally, UK data suggest that between 0.2% and 1% of adults are on an Enhanced Care Plan, with variation between geographic areas correlated strongly with social disadvantage (SCMH, 1998).
Describing the possible service needs of individuals with severe mental illness
The possible service needs of people with severe mental illness in Australia were described using samples derived from two separate epidemiological surveys. The 2010 SHIP sample mainly comprised individuals with a diagnosis of non-affective psychosis (69.5%), but also with affective psychosis (30.6%). A significant minority (39.4%) reported the onset of psychotic disorder before the age of 20 years. Three in 10 (30.5%) were classified as having a continuous chronic course of illness, with a further 31.8% having multiple episodes with only partial recovery between episodes.
The 2007 NSMHWB sample of people with severe mental illness comprised individuals with severe affective disorders (79.6%) and/or severe anxiety disorders (78.7%). The majority (86.4%) of this group reported their disorder began 2 or more years ago, and 69.0% reported the onset of their disorder(s) before age 20. Two-thirds (67.0%) reported their symptoms as being present in the last month. This has previously been defined as an indicator of chronicity (Andrews et al., 2001).
Table 2 summarises the possible service needs and service use of the above groups. Among people with psychotic disorders (SHIP), use of accommodation (40%), non-government services (30%) and receipt of income support (85%) were common. Among those with severe affective and/or anxiety disorders (NSMHWB), receipt of income support (37%) was common; however, information on accommodation and non-government support services was not available. Data were also available on characteristics that may be indicative of service needs. Among the sample with psychosis, possible needs for support in areas of socialising, personal care and employment were highlighted. In the sample with severe affective and anxiety disorders, possible needs in the areas of financial management and employment were indicated.
Indicators of possible service needs among 2010 SHIP and 2007 NSMHWB participants with severe mental disorders.
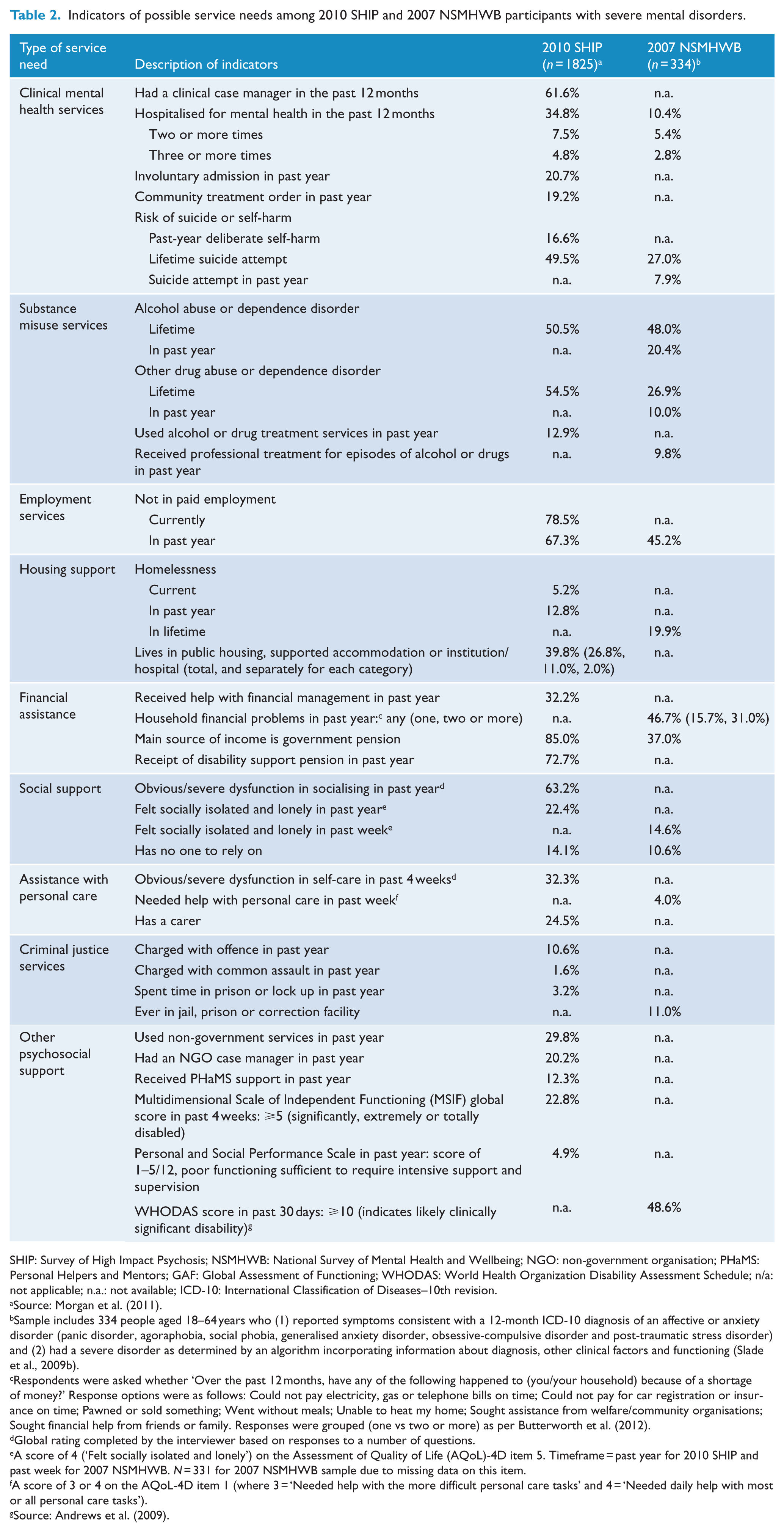
SHIP: Survey of High Impact Psychosis; NSMHWB: National Survey of Mental Health and Wellbeing; NGO: non-government organisation; PHaMS: Personal Helpers and Mentors; GAF: Global Assessment of Functioning; WHODAS: World Health Organization Disability Assessment Schedule; n/a: not applicable; n.a.: not available; ICD-10: International Classification of Diseases–10th revision.
Source: Morgan et al. (2011).
Sample includes 334 people aged 18–64 years who (1) reported symptoms consistent with a 12-month ICD-10 diagnosis of an affective or anxiety disorder (panic disorder, agoraphobia, social phobia, generalised anxiety disorder, obsessive-compulsive disorder and post-traumatic stress disorder) and (2) had a severe disorder as determined by an algorithm incorporating information about diagnosis, other clinical factors and functioning (Slade et al., 2009b).
Respondents were asked whether ‘Over the past 12 months, have any of the following happened to (you/your household) because of a shortage of money?’ Response options were as follows: Could not pay electricity, gas or telephone bills on time; Could not pay for car registration or insurance on time; Pawned or sold something; Went without meals; Unable to heat my home; Sought assistance from welfare/community organisations; Sought financial help from friends or family. Responses were grouped (one vs two or more) as per Butterworth et al. (2012).
Global rating completed by the interviewer based on responses to a number of questions.
A score of 4 (‘Felt socially isolated and lonely’) on the Assessment of Quality of Life (AQoL)-4D item 5. Timeframe = past year for 2010 SHIP and past week for 2007 NSMHWB. N = 331 for 2007 NSMHWB sample due to missing data on this item.
A score of 3 or 4 on the AQoL-4D item 1 (where 3 = ‘Needed help with the more difficult personal care tasks’ and 4 = ‘Needed daily help with most or all personal care tasks’).
Source: Andrews et al. (2009).
Discussion
Using data from multiple sources, we show how the estimate that 0.4% of Australian adults experience severe and persistent mental illness with complex multi-agency needs in any given year was generated. This equated to approximately 59,000 Australians aged 18–64 years in 2015.
In generating these estimates, we have drawn on multiple sources, and where necessary, made informed estimates where the data are unavailable or incomplete. We have also compared our estimates to more recently published data. Using multiple data sources enabled us to triangulate the findings, consistent with internationally recognised best practice in health programme evaluation (Ovretveit, 1998); the convergence in our estimates lends support to their validity.
For example, our estimate of the proportion of people living with severe mental disorders whose disorders are persistent (Step 2) falls within the range suggested by previous studies. For example, data from the 2010 SHIP suggest that 30.5% of adults with psychotic disorders have a chronic course of illness (Morgan et al., 2011). Data from a representative community survey in Canada estimated that 1.5% of adults meet criteria for a 12-month chronic major depressive disorder (i.e. most recent episode lasting longer than 2 years) (Blanco et al., 2010), equivalent to 26.5% of all individuals with 12-month major depression (Rubio et al., 2011). Of those with chronic major depression, around half reported scores more than 1 standard deviation lower than the normative mean on a measure of mental disability (Blanco et al., 2010; Rubio et al., 2011), a criterion that has previously been used to denote moderate or severe disability (Andrews and Tolkein II Team, 2007). A US study estimated that 4.7% of US adults had persistent depressive or anxiety disorders (i.e. diagnosis present on two occasions, 32 months apart), of whom about half met the above criterion for moderate or severe mental disability (Young et al., 2008). Furthermore, a longitudinal analysis of recovery trajectories among persons with serious mental illnesses (including schizophrenia, schizo-affective disorder, bipolar disorder or affective psychosis) in the United States identified that 24% of the sample experienced an illness trajectory that was characterised by persistently high mental and physical health symptoms, poorer overall functioning, lower rates of employment and higher rates of mental health service use, that showed no change over a 2-year period (Green et al., 2013).
Similarly, our estimates of the proportion of people with severe and persistent mental illness who have complex, multi-agency needs (Step 3) were compared to more recent Australian and Italian studies. The most recent SDAC provides a revised figure of 68,500 Australians living with a profound core-activity limitation arising from mental illness in 2012 (ABS, 2013). Further analysis of SHIP survey participants has shown that 30% of people with psychosis in contact with services in the census month were receiving both public community mental health and non-government support services and that 42% of these had a chronic course of illness (Harvey et al., 2015). While the SHIP analysis defined this group by their use of multi-agency services rather than needs, the similarity of the size of this group to our estimates lends them support. In Italy, Ruggeri et al. (2000) developed and tested two operationalised definitions of severe and persistent mental illness. They found that a ‘narrow’ definition – which classified persons as severe if they had a diagnosis of psychosis, a treatment duration of more than 2 years and scored 50 or below on the GAF scale – only selected a small group of persons with psychotic disorders. Alternatively, they tested a ‘wider’ definition which captured a broader diagnostic spectrum by applying the latter two criteria only (Ruggeri et al., 2000). Ruggeri et al. (2000) estimated the number of people with severe mental illness by applying these criteria to samples of people in contact with community mental health services in South London and South Verona. Parabiaghi et al. (2006) applied Ruggeri et al.’s (2000) wider definition of severe and persistent mental illness to data from a longitudinal study of people with severe mental illness in the South Verona community mental health service. These studies classified between 9% and 20% of adults in contact with community mental health services, or approximately 0.2% of the adult population, as having a persistent and disabling disorder (Parabiaghi et al., 2006; Ruggeri et al., 2000).
Limitations
It is important to make clear several features of these estimates and associated potential limitations. First, our estimates are derived from data on people with the most complex needs and those with severe and persistent mental illness during a 12-month window. People with persistent mental illness but less severe disability and those with severe but episodic mental illness are not included. Some of these individuals will require short or longer term non-clinical support services. Second, the absence of an agreed definition and criteria for severe, persistent and complex mental illness prevented an analysis of the same group in both aims of this paper. We chose to profile the type of needs that people with severe mental illness have using the available data to help inform future definitional work and guide the collection of data to profile service needs. Third, some people with complex multi-agency needs will receive assistance solely through informal family support; however, we are unaware of any estimates of the size or needs of that population.
Fourth, our estimates relied primarily on data from samples in contact with clinical mental health services, and hence may not reflect the profile of people who receive services solely provided through non-health sectors, such as non-government organisations, or the criminal justice system. It also does not consider employment or vocational services, but the need for those services applies more broadly to people with mental disorders, particularly those with severe disorders, as indicated by our analyses of the possible service needs of this group.
However, in all the above points, their impact upon the estimate produced here will have been to make it a conservative one. To that extent, planning based on these figures will not be an inflated estimate of the need for services for this group.
We have relied on international data (primarily from Italy and the United Kingdom), and differences in the health and welfare systems in these countries compared to Australia may limit the translatability of estimates from those sources. Furthermore, much of the available data are more than a decade old, and although there is evidence that the prevalence of mental disorders has not changed over that time (Whiteford et al., 2013), these data will not reflect possible changes in service systems. The 2010 SHIP found that compared to the first Australian Low Prevalence Disorders Survey conducted in 1997–1998, use of community-based mental health services and non-government support services had increased and that there appeared to be improvements in the course of illness and housing stability. However, rates of financial disadvantage, social isolation and unemployment were similar across the two surveys, suggesting no improvement over time, and co-morbid substance use disorders actually increased (Carr et al., 2012).
Also, we acknowledge that to some extent, the number of people with complex needs will be somewhat determined by the availability of existing services and support networks – if these services adequately address the needs of this population, they may not present with such complicated issues because their needs are already being met.
Implications
Agreed indicators of persistence and complex service needs are required to inform service planning for this population. Previous Italian studies used ‘service contact ⩾ 2 years’ to indicate persistence of disorder (Parabiaghi et al., 2006; Ruggeri et al., 2000); however, an equivalent measure was not available for the Australian 2010 SHIP or 2007 NSMHWB. A number of indicators of possible service needs could not be assessed using the available data sources, for example, disengagement from services. An agreed definition of what constitutes ‘complex needs’ (and whether this should be determined by number, type or intensity of needs) is not available.
Greater alignment across epidemiological surveys of the information collected about actual service use and possible service needs of individuals with severe mental illness is crucial. For example, the wording, timeframe and measures used differed between the 2010 SHIP and the 2007 NSMHWB on key items such as need for clinical mental health services (case management and involuntary admissions were captured in 2010 SHIP, but not 2007 NSMHWB), homelessness (recorded for current/past year in 2010 SHIP vs lifetime in 2007 NSMHWB), contact with criminal justice services (spent time in prison measured as past year in 2010 SHIP vs lifetime in the 2007 NSMHWB) and general assessments of health and disability (e.g. the WHODAS was included in the 2007 NSMHWB but not 2010 SHIP).
Conclusion
It is critical for service planning that methods for enumerating the populations in scope for new mental health reforms, matched to their support needs, continue to be refined. Developing clearer definitional criteria, and applying these to understanding the service needs of people with severe and persistent mental illness, should be a focus of further research.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Health and Medical Research Council (NHMRC) Centre for Research Excellence in Mental Health Systems Improvement (APP1041131). L.D. is supported by an NHMRC principal research fellowship (APP1041742). E.S. is supported by an NHMRC early career research fellowship (APP1104600). The National Drug and Alcohol Research Centre at UNSW Australia is supported by funding from the Australian Government under the Substance Misuse Prevention and Service Improvements Grant Fund. None of these funders had any role in the conceptualisation or conduct of this review.