
Abstract
Objective:
To derive planning estimates for the provision of public mental health services in Queensland 2007–2017.
Method:
We used a five-step approach that involved: (i) estimating the prevalence and severity of mental disorders in Queensland, and the number of people at each level of severity treated by health services; (ii) benchmarking the level and mix of specialised mental health services in Queensland against national data; (iii) examining 5-year trends in Queensland public sector mental health service utilisation; (iv) reviewing Australian and international planning benchmarks; and (v) setting resource targets based on the results of the preceding four steps. Best available evidence was used where possible, supplemented by value judgements as required.
Results:
Recommended resource targets for inpatient service were: 20 acute beds per 100,000 population, consistent with national average service provision but 13% above Queensland provision in 2005; and 10 non-acute beds per 100,000, 65% below Queensland levels in 2005. Growth in service provision was recommended for all other components. Adult residential rehabilitation service targets were 10 clinical 24-hour staffed beds per 100,000, and 18 non-clinical beds per 100,000. Supported accommodation targets were 35 beds per 100,000 in supervised hostels and 35 places per 100,000 in supported public housing. A direct care clinical workforce of 70 FTE per 100,000 for ambulatory care services was recommended. Fifteen per cent of total mental health funding was recommended for community support services provided by non-government organisations.
Conclusions:
The recommended targets pointed to specific areas for priority in Queensland, notably the need for additional acute inpatient services for older persons and expansion of clinical ambulatory care, residential rehabilitation and supported accommodation services. The development of nationally agreed planning targets for public mental health services and the mental health community support sector were identified as priorities.
Introduction
Mental health service planning involves determining the strategies, time frames, indicators and targets, and resources required to implement the vision and objectives articulated by a mental health policy (World Health Organization, 2004). Agreed gold standards to guide mental health planning are not currently available at either the national or international level. In the absence of planning standards, there are two ways to approach the task. The first is to use normative data. The normative approach assumes that service provision levels in place elsewhere, particularly in areas that are believed to have ‘good’ mental health services, or similar demographic and political structures to our own, provide a sound basis to make judgements about local requirements. The second, ‘ideal’, approach involves an empirical, population health approach. Decisions regarding the configuration and delivery of services are based on reliable, current information about the prevalence and severity of mental disorders in the community, levels of mental health treatment need, treatments that are likely to be effective in addressing this need, and the resources required to deliver these treatments (Andrews et al., 2001a; World Health Organization, 2004).
In reality, there are few examples of empirically-based planning (Andrews and the Tolkien II Team, 2007; Boardman and Parsonage, 2007; Goodman, 1998; Lesage et al., 2003; Lund and Flisher, 2006; Mental Health Commission, 1998; New South Wales Department of Health, 2001). A review of mental health plans from Australia, New Zealand, England, Canada and the USA found that while 20 plans defined core mental health services, only four cited resource targets for these core services (Pirkis et al., 2007). Only two plans derived resource targets from models based on epidemiological data combined with evidence regarding best practice. The majority rested on normative data describing resources such as inpatient beds and staffing profiles already in use in other jurisdictions or countries. Australian states and territories develop their own input planning parameters and do not always make these overt for others to use and compare. Similarly, planners in other countries rarely publish the norms and targets they use in developing their mental health services. More commonly, services are developed incrementally, often in response to the prevailing pressures of the day, and without the assistance of explicit or implicit planning norms.
Based on the current state of practice, mental health service planning often requires an approach that combines empirical evidence with good planning models, supplemented by value judgements and expert opinion. This paper describes the approach taken to generate resource targets for the provision of core public mental health services in Queensland for the period 2007–2017, to inform the development of the Queensland Plan for Mental Health 2007–2017 (Queensland Health, 2008). Although this work was undertaken 5 years ago, and the Australian mental health service system has changed since then, it is one of few published descriptions of the norms and targets used in a mental health service planning exercise.
Methods
We sought to generate resource targets for five core mental health service components – inpatient services, adult residential rehabilitation services, supported accommodation, ambulatory care mental health services, and community support services. These components were selected because: (i) there was broad consensus, in Australia and within the published mental health planning literature, that the component is an essential element of a specialised mental health service system, and (ii) resource targets were specified to a sufficient extent to allow recommendations to be made for developing Queensland mental health services over the next 10 years (Pirkis et al., 2007). We used a five-step process guided by the health planning literature and examples of empirically-based planning (Green, 2007; New South Wales Department of Health, 2001; Thornicroft and Tansella, 1999; Andrews and the Tolkien II Team, 2007; World Health Organization, 2003). Details of each step, and the data sources and key assumptions used in each, are described below.
1. Quantifying mental health treatment need
The first step required us to quantify the population requiring mental health services. We began by deriving estimates of the community prevalence of mental disorders in Queensland by age group and severity. Because comprehensive age- and severity-specific prevalence data for Queensland were not available, these were derived from the New South Wales planning document Mental Health Clinical Care and Prevention Model: a population health model (MH-CCP Version 1.11) (New South Wales Department of Health, 2001). MH-CCP incorporates data gathered in the Australian National Survey of Mental Health and Well Being augmented by other local and international surveys to fill gaps in available Australian epidemiological data. The MH-CCP model relies principally on data from the USA for the 18 years + population; estimates for the child and adolescent population are based on UK and Australian data. MH-CCP grouped severity into three levels (severe, moderate and mild), based largely on criteria developed by the US National Advisory Mental Health Council that take into account diagnosis, disability and duration of symptoms. We aggregated the prevalence estimates into three categories (0–17, 18–64 and 65+ years), corresponding to the major mental health program types in Australia. The prevalence estimates were derived at a national level, then applied to the Queensland population age structure (Australian Bureau of Statistics, 2005).
We then estimated the proportion of people with a mental disorder in each severity group who received treatment in various parts of the health system. There was no single source from which to derive these figures. We used Queensland-specific data from the National Mental Health Report 2007 (Department of Health and Ageing, 2007), supplemented by data from Queensland Health, to estimate the numbers of people seen by public and private sector mental health services. We used reports from the 1997 National Survey of Mental Health and Wellbeing (NSMHWB) to estimate the numbers of people seen by general practitioners alone (Andrews et al., 2001b; Sawyer et al., 2000), and other health services (Andrews et al., 2001a). Adjustments were made to allow for duplicated person counts. Severity was apportioned using methods specific to each sector. (Further details are provided in the footnotes to Table 2.)
2. Benchmarking Queensland service provision levels
In the second step, we compared the level and mix of specialised mental health services in Queensland against available ‘benchmarks’ (i.e., reference points or standards against which performance or achievements can be assessed (World Health Organization, 2012)), from the most recently published national data, on the following measures: designated psychiatric beds, full-time equivalent (FTE) direct care staff in ambulatory services, and community accommodation support services. Limited comparisons of private sector mental health services were made on measures of psychiatric hospital beds, Medicare-funded consultant psychiatrist attendances and prescription of psychiatric pharmaceuticals subsidised by the Pharmaceutical Benefits Scheme (PBS). Program and staffing figures were derived from the National Mental Health Report 2007 (Department of Health and Ageing, 2007), supplemented by data provided by Queensland Health.
3. Analysis of 5-year trends in public sector mental health service utilisation
In the third step, we evaluated the impact of the planning benchmarks set under the first Queensland Ten Year Mental Health Strategy (Queensland Health, 1996) developed in 1996. We examined 5-year trends in the utilisation of Queensland public mental health services. Inpatient mental health service utilisation data were provided by Queensland Health from the Queensland Health Admitted Patient Data Collection (QHAPDC) (Data Services Unit QH, 2005). Diagnoses were grouped using classifications developed for the Mental Health Classification and Service Costs Project (Buckingham et al., 1998). Ambulatory mental health service utilisation data were provided by Queensland Health from the Mental Health Activity Data Collection. These were adjusted for over-counting due to lack of a unique state-wide person identifier and to take account of improvements in compliance with recording of contacts over the years of observation (as recommended by Queensland Health). All data were provided in de-identified, aggregated form.
4. Review of published planning benchmarks for core service components
The fourth step involved reviewing published resource targets for the core service components. These were identified from a review of government-endorsed mental health plans (Pirkis et al., 2007) and supplementary searches. To allow ‘side by side’ comparisons, resource targets were standardised by converting the raw target figures into age-specific rates for Queensland, then converted to rates per 100,000 total population. Because planning documents varied in the ways in which services were labelled or defined, some degree of interpretation was required to map the core component categories. Where required (e.g., where a plan cited total numbers of inpatient beds without acute/non-acute ratios), apportioning rules were applied, based on existing precedents in Queensland or other jurisdictions, or supplementary information about the mental health services available within the relevant country or jurisdiction. (Further detail is provided in the footnotes to Table 7.)
5. Setting resource targets
The final step involved synthesising the information gathered in the previous four steps to set resource targets for the five core service components.
Results
1. Quantifying mental health treatment need
Table 1 shows that approximately 16.6% of Queenslanders (approximately 647,000 people in 2004–05) are affected by mental disorders in any one year: 9.6% with mild, 4.5% with moderate, and 2.5% with severe disorders. These estimates exclude dementia and alcohol- and drug-related disorders, except where these are concurrent with another mental disorder, as these fall outside the remit of public mental health services.
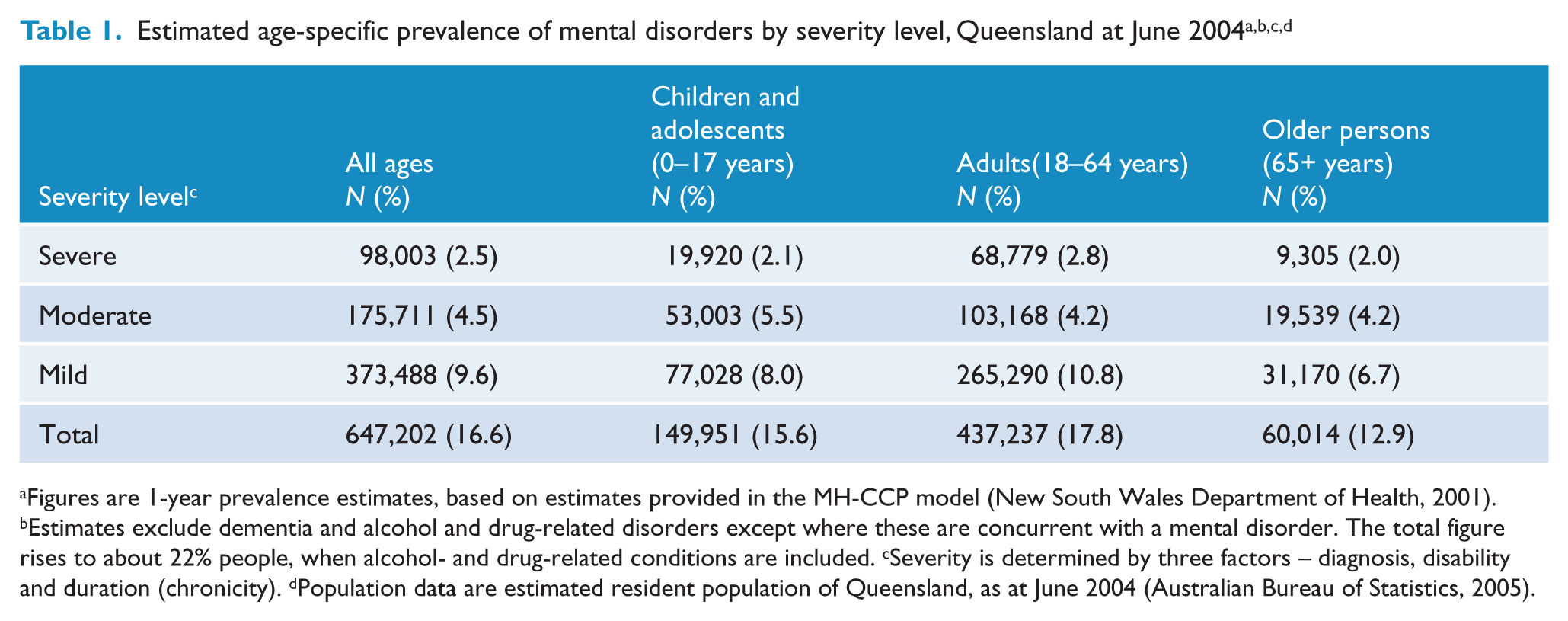
Figures are 1-year prevalence estimates, based on estimates provided in the MH-CCP model (New South Wales Department of Health, 2001).
Estimates exclude dementia and alcohol and drug-related disorders except where these are concurrent with a mental disorder. The total figure rises to about 22% people, when alcohol- and drug-related conditions are included.
Severity is determined by three factors – diagnosis, disability and duration (chronicity).
Population data are estimated resident population of Queensland, as at June 2004 (Australian Bureau of Statistics, 2005).
Table 2 shows the estimated numbers of people treated by various parts of the health system in 2004–05. The 2.5% of Queensland’s population (almost 100,000 people) who experience severe mental disorders are the primary target of the state’s public mental health system. However people with disorders of mild or moderate severity are also of interest because public mental health services may provide treatment to this group in areas where there is an undersupply of other providers. In addition, individuals with disorders of mild severity may be at risk of developing more severe symptoms and disability (Kessler et al., 2003) and are therefore a focus for early intervention. Just over half (52%) of those with severe mental disorders were estimated to be clients of public mental health services. About a quarter of the treated severe group were seen only by their GP (about 23,000 people), suggesting a need for additional specialist mental health services and consultation support by the system. Arguably, this group needs to be considered as a priority for improved service delivery, together with the 4000 people with severe disorders not currently seen by any health service.
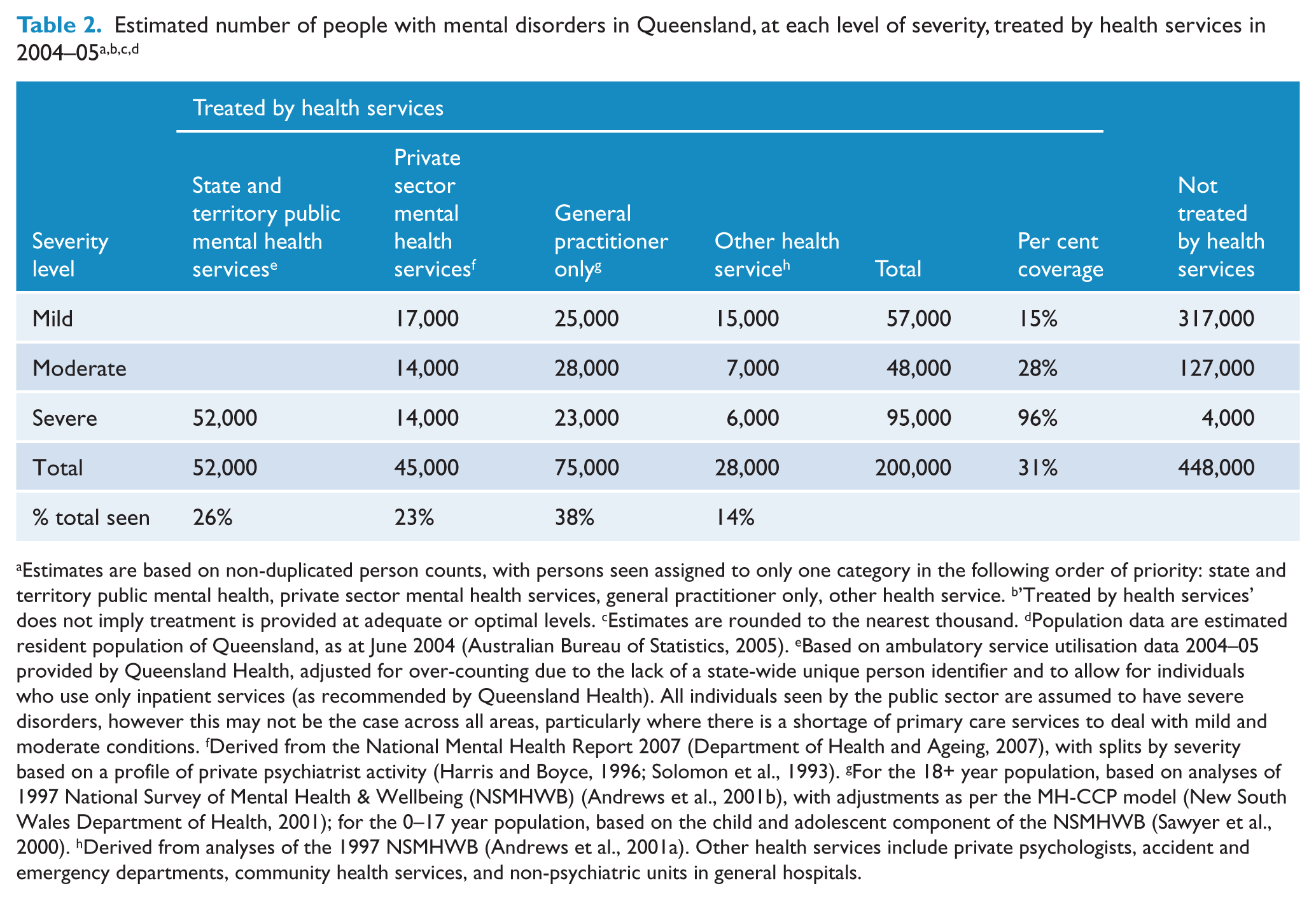
Estimates are based on non-duplicated person counts, with persons seen assigned to only one category in the following order of priority: state and territory public mental health, private sector mental health services, general practitioner only, other health service.
’Treated by health services’ does not imply treatment is provided at adequate or optimal levels.
Estimates are rounded to the nearest thousand.
Population data are estimated resident population of Queensland, as at June 2004 (Australian Bureau of Statistics, 2005).
Based on ambulatory service utilisation data 2004–05 provided by Queensland Health, adjusted for over-counting due to the lack of a state-wide unique person identifier and to allow for individuals who use only inpatient services (as recommended by Queensland Health). All individuals seen by the public sector are assumed to have severe disorders, however this may not be the case across all areas, particularly where there is a shortage of primary care services to deal with mild and moderate conditions.
Derived from the National Mental Health Report 2007 (Department of Health and Ageing, 2007), with splits by severity based on a profile of private psychiatrist activity (Harris and Boyce, 1996; Solomon et al., 1993).
For the 18+ year population, based on analyses of 1997 National Survey of Mental Health & Wellbeing (NSMHWB) (Andrews et al., 2001b), with adjustments as per the MH-CCP model (New South Wales Department of Health, 2001); for the 0–17 year population, based on the child and adolescent component of the NSMHWB (Sawyer et al., 2000).
Derived from analyses of the 1997 NSMHWB (Andrews et al., 2001a). Other health services include private psychologists, accident and emergency departments, community health services, and non-psychiatric units in general hospitals.
2. Benchmarking Queensland service provision levels
Comparison of the level and mix of specialised mental health services available in Queensland against national levels showed four key findings. Firstly, the number of inpatient beds increased by 6.7% between 2001 and 2005, less than population growth during this time (9.2%) (Table 3). While the provision of inpatient beds matched, or was above, national average levels for general adult, child and adolescent and forensic services, specialist older persons’ mental health program beds were provided at only half the average of other jurisdictions (Table 4).
Number of designated public sector 24-hour staffed psychiatric beds by target population and beds per 100,000 and number of direct care FTE staff employed in public sector ambulatory mental health services, June 2001 to June 2005, Queensland a
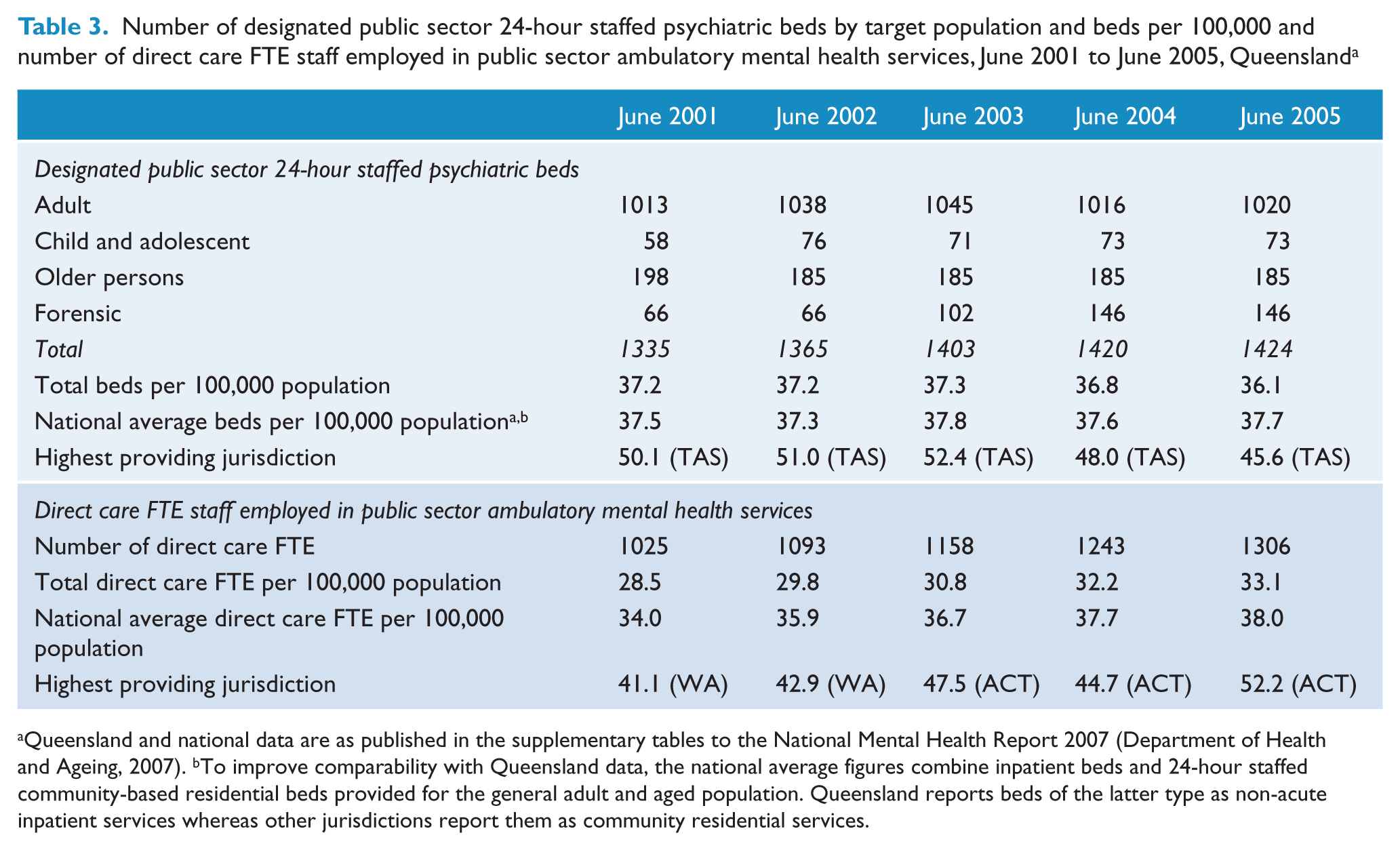
Queensland and national data are as published in the supplementary tables to the National Mental Health Report 2007 (Department of Health and Ageing, 2007).
To improve comparability with Queensland data, the national average figures combine inpatient beds and 24-hour staffed community-based residential beds provided for the general adult and aged population. Queensland reports beds of the latter type as non-acute inpatient services whereas other jurisdictions report them as community residential services.
Selected indicators of mental health service provision for Queensland compared to the national average, June 2005 a
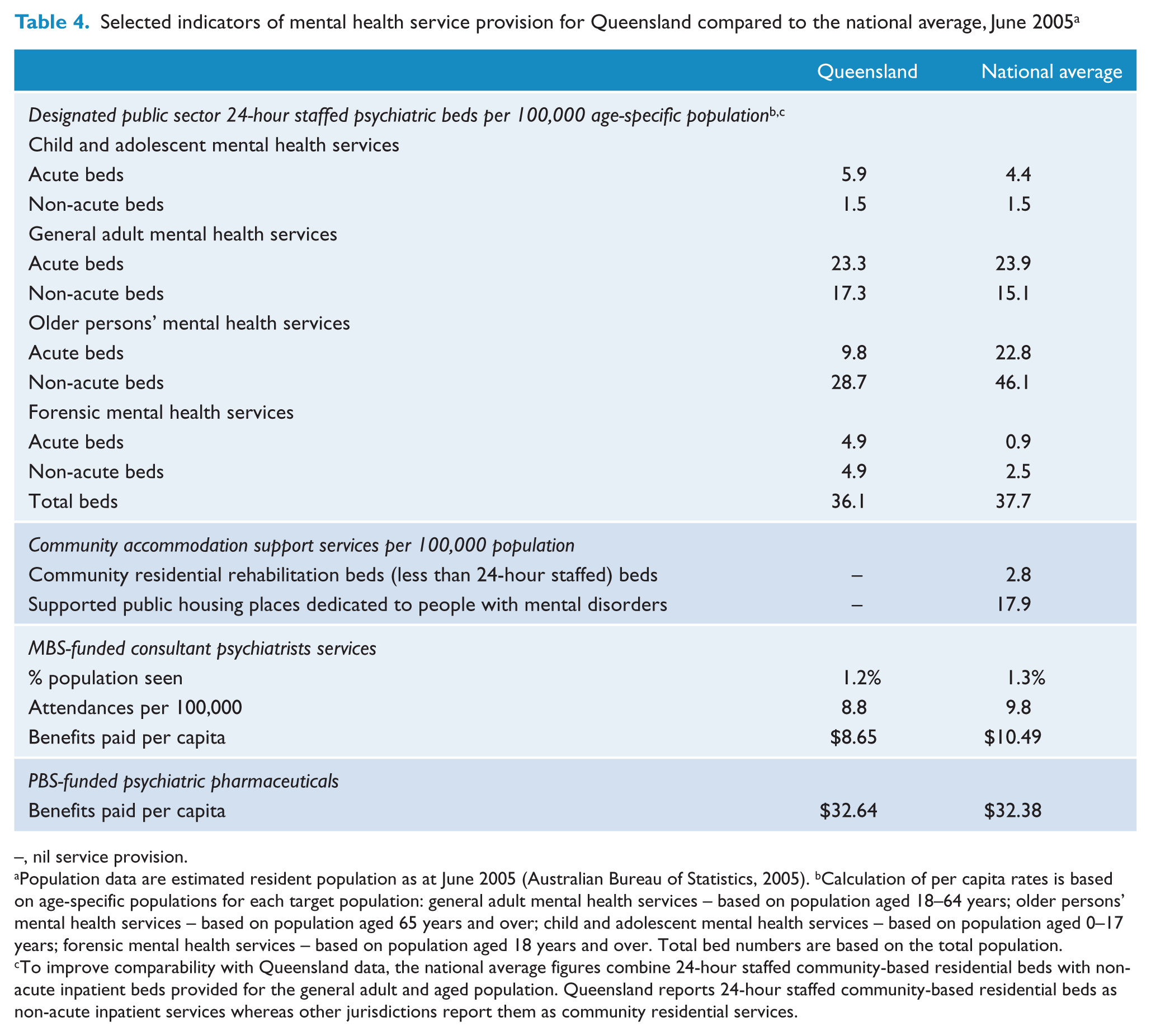
–, nil service provision.
Population data are estimated resident population as at June 2005 (Australian Bureau of Statistics, 2005).
Calculation of per capita rates is based on age-specific populations for each target population: general adult mental health services – based on population aged 18–64 years; older persons’ mental health services – based on population aged 65 years and over; child and adolescent mental health services – based on population aged 0–17 years; forensic mental health services – based on population aged 18 years and over. Total bed numbers are based on the total population.
To improve comparability with Queensland data, the national average figures combine 24-hour staffed community-based residential beds with non-acute inpatient beds provided for the general adult and aged population. Queensland reports 24-hour staffed community-based residential beds as non-acute inpatient services whereas other jurisdictions report them as community residential services.
Secondly, ambulatory care staffing increased by 27.4% between 2001 and 2005 (Table 3) but remained the lowest of all Australian jurisdictions (Department of Health and Ageing, 2007). Staffing levels at June 2005 were 13% below the national average and 37% lower than the highest providing jurisdiction. A 15% increase in Queensland’s ambulatory care services would be needed to reach 2005 national average levels.
Thirdly, Queensland’s investment in community support services managed by the non-government organisations (NGOs) in 2004–05 ($24.4 million) represented 6.4% of its annual mental health funding, equivalent to the national average (6.3%) (Department of Health and Ageing, 2007). About 70% of this funding was administered outside the health portfolio and managed by Disability Services Queensland; over 100 services were funded. Judged by national comparative data, Queensland’s provision of the range of accommodation-related services typically managed by NGOs is low. Community residential services, staffed on a less than 24-hour basis, were not available (Table 4). In other jurisdictions, these services filled an important gap in providing residential rehabilitation to people who do not require the intensive support available in services clinically staffed on a 24-hour basis. Similarly, the provision of supported public housing places was undeveloped (Table 4). In other jurisdictions, these places provided dedicated public housing accommodation to people disabled by mental disorders who are able to live relatively independently if appropriate support is made available.
Fourthly, private psychiatric beds comprised 22.5% of all psychiatric beds in Queensland, approximating the national average (22%) (Department of Health and Ageing, 2007). Commonwealth-funded Medicare Benefits Schedule (MBS) service provision by Queensland private psychiatrists in 2005 was 12% below the national average. Psychiatric drugs subsidised by the Pharmaceutical Benefits Scheme (PBS) approximated the national average (Table 4). As in other jurisdictions, the majority of these medications are prescribed by GPs.
3. Analysis of 5-year trends in public sector mental health service utilisation
In 2004–05, 15,332 people (or 0.4% of Queenslanders) received inpatient services from a designated psychiatric unit collocated in an acute hospital (that is, a unit that receives dedicated funding for the provision of psychiatric care), or from a non-designated unit (e.g. a unit in a general hospital) for a principal diagnosis of a mental disorder. Designated units provided the majority of inpatient services (83.3% of persons seen, 87.4% of episodes, and 95.8% of patient days) in 2004–05.
There were three main findings regarding trends in inpatient service utilisation. Firstly, overall growth in demand had kept pace with population growth. Table 5 shows that, after adjusting for population growth, the total number of persons admitted and episodes per annum remained relatively constant from 2000–01 to 2004–05. In addition, non-designated units did not appear to be capturing an overflow of demand from designated units.
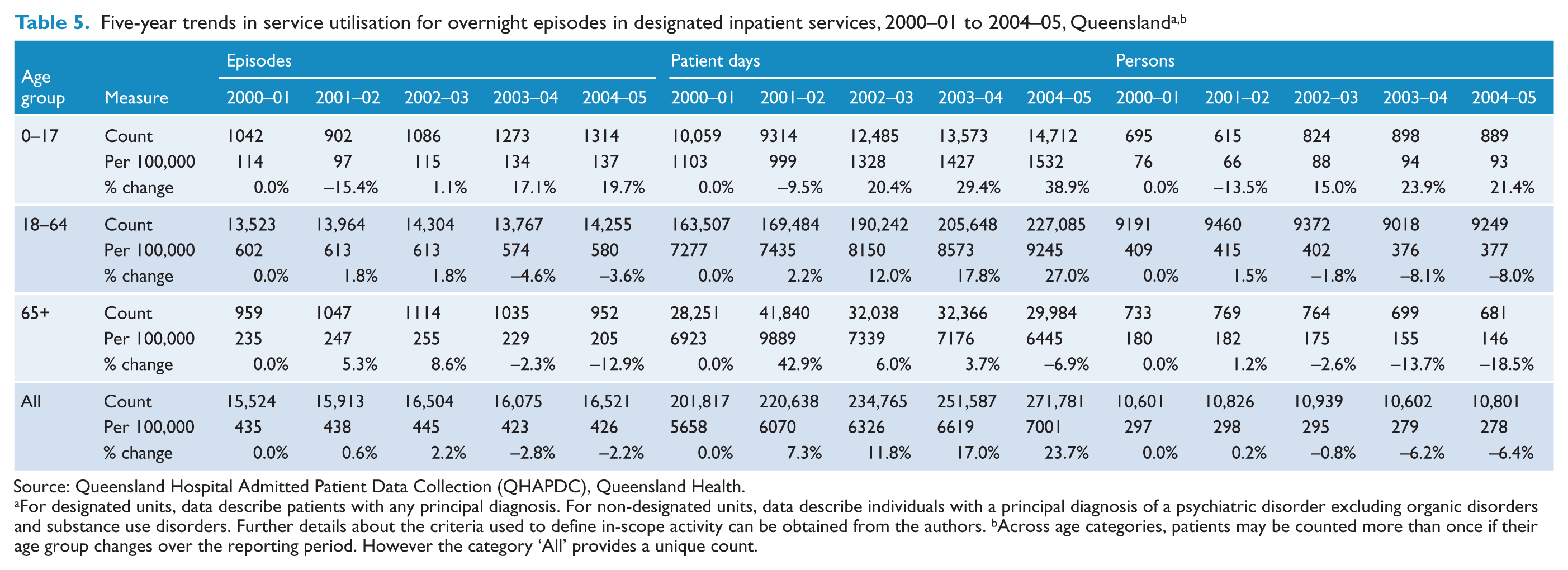
Source: Queensland Hospital Admitted Patient Data Collection (QHAPDC), Queensland Health.
For designated units, data describe patients with any principal diagnosis. For non-designated units, data describe individuals with a principal diagnosis of a psychiatric disorder excluding organic disorders and substance use disorders. Further details about the criteria used to define in-scope activity can be obtained from the authors.
Across age categories, patients may be counted more than once if their age group changes over the reporting period. However the category ‘All’ provides a unique count.
Secondly, the existing benchmarks did not match demand among older persons. Among those aged 65+, the number of persons admitted decreased by 19% and episodes provided decreased by 13% from 2000–01 to 2004–05. This contrasts with more modest decreases among 18–64-year-olds (8% and 4%), and substantial increases among 0–17-year-olds (20% and 21%, respectively) (Table 5).
Thirdly, although the overall number of beds appears adequate, increasing length of stay (LoS) has taken up increased bed capacity. Although median length of stay remained relatively stable across all age groups, average LoS across all age groups increased by 6.6% from 2000–01 to 2004–05. This was driven by increases of 13.2% among 0–17-year-olds and 8.2% among 18–64-year-olds (compared to a decrease of 2.0% in those aged 65+). The percentage of episodes lasting more than 35 days increased by 9.9% (from 7.1% to 7.8%). In addition, the percentage of overnight episodes where the patient was involuntary for all or part of the episode increased by 5.7% (from 45.4% in 2000–01 to 48.0%). These changes suggest that the observed increase in patient days is, in part at least, due to an increase in case complexity and an increase in the proportion of episodes of long duration.
With respect to ambulatory care services, we estimated that 62,243 persons (1.6% of Queenslanders) received at least one contact with ambulatory mental health services in Queensland in 2004–05. During that period, 50,749 (1.3% of Queenslanders) were seen for ongoing treatment and a further 11,494 (0.3% of the population) were seen for assessment only. Analyses suggested that the overall number of persons seen by ambulatory mental health services per capita may have increased by 18% from 48,528 in 2000–01 to 62,243 in 2004–05. However, these data should be interpreted with caution, given the nature of the adjustments made in the calculation of these estimates.
4. Review of published planning benchmarks for core service components
Planning benchmarks were identified from seven sources: government planning documents from New South Wales (New South Wales Department of Health, 2001), South Australia (Department of Human Services, 2002), Queensland (Queensland Health, 1996), Western Australia (Office of Mental Health, 2004) and New Zealand (Mental Health Commission, 1998); plus two empirically-based planning exercises developed in Australia (Andrews and the Tolkien II Team, 2007) and England (Boardman and Parsonage, 2005). Table 6 shows the planning benchmarks mapped to the five core service components, as well as the current levels of provision of each of these components in Queensland and nationally.
Current service provision, planning benchmarks and recommended targets for Queensland 2006–2017, per 100,000 total population a
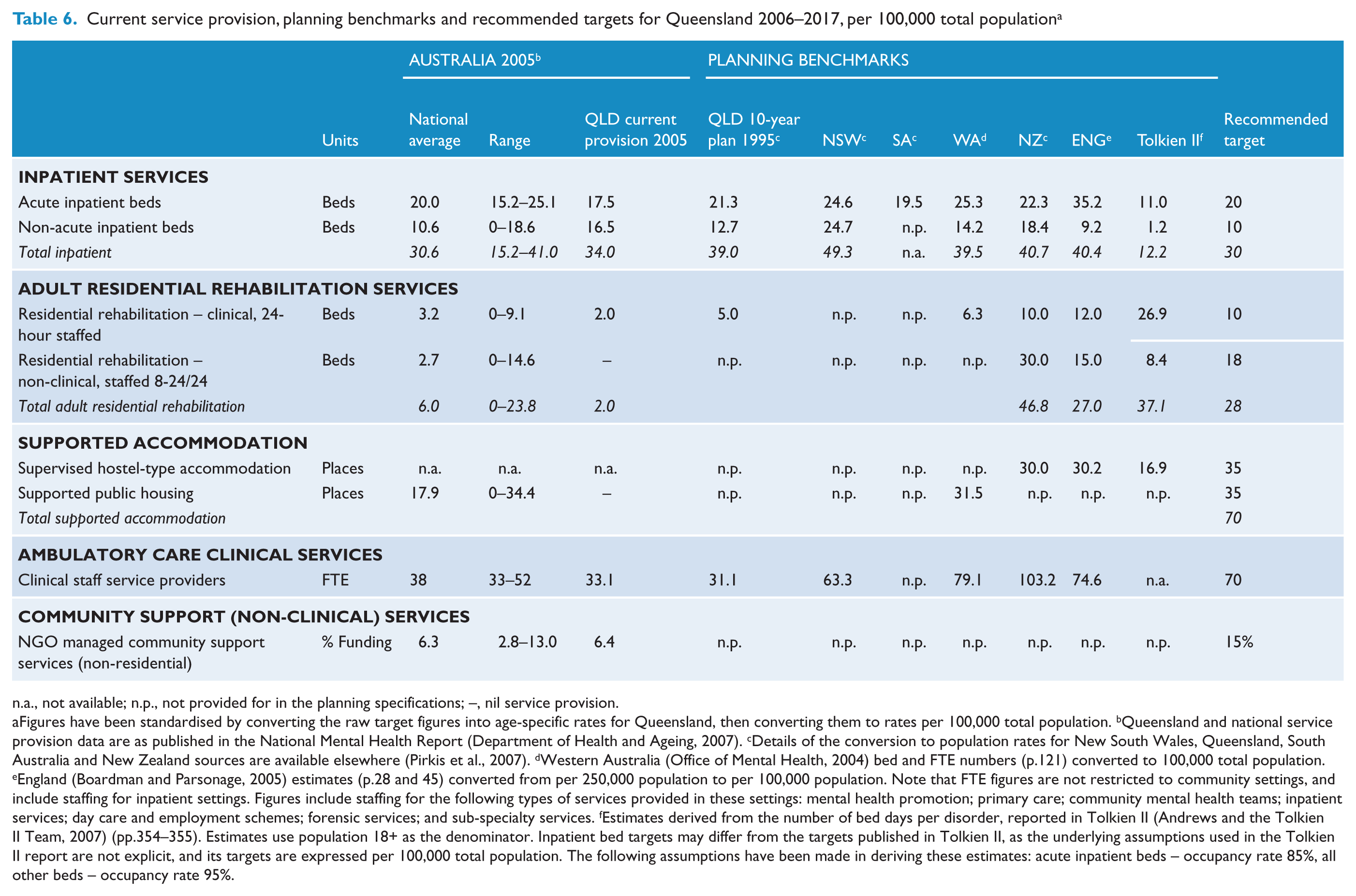
a., not available; n.p., not provided for in the planning specifications; –, nil service provision.
Figures have been standardised by converting the raw target figures into age-specific rates for Queensland, then converting them to rates per 100,000 total population.
Queensland and national service provision data are as published in the National Mental Health Report (Department of Health and Ageing, 2007).
Details of the conversion to population rates for New South Wales, Queensland, South Australia and New Zealand sources are available elsewhere (Pirkis et al., 2007).
Western Australia (Office of Mental Health, 2004) bed and FTE numbers (p.121) converted to 100,000 total population.
England (Boardman and Parsonage, 2005) estimates (p.28 and 45) converted from per 250,000 population to per 100,000 population. Note that FTE figures are not restricted to community settings, and include staffing for inpatient settings. Figures include staffing for the following types of services provided in these settings: mental health promotion; primary care; community mental health teams; inpatient services; day care and employment schemes; forensic services; and sub-specialty services.
Estimates derived from the number of bed days per disorder, reported in Tolkien II (Andrews and the Tolkien II Team, 2007) (pp.354–355). Estimates use population 18+ as the denominator. Inpatient bed targets may differ from the targets published in Tolkien II, as the underlying assumptions used in the Tolkien II report are not explicit, and its targets are expressed per 100,000 total population. The following assumptions have been made in deriving these estimates: acute inpatient beds – occupancy rate 85%, all other beds – occupancy rate 95%.
5. Setting the resource targets
Table 7 summarises the recommended resource targets. The rationale for, and resource implications of, the recommended targets are discussed below.
Resource implications of the recommended targets for Queensland service provision
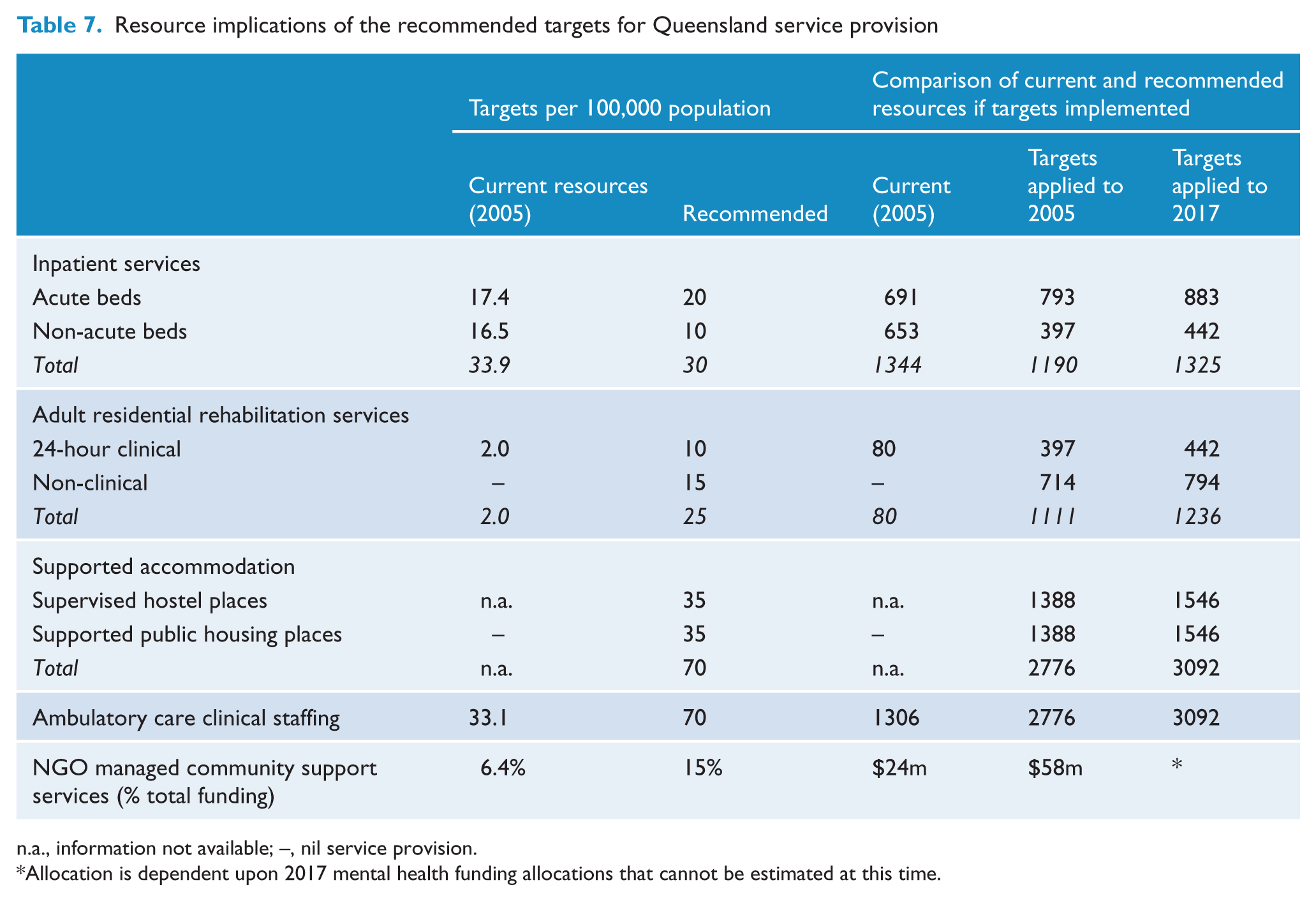
n.a., information not available; –, nil service provision.
Allocation is dependent upon 2017 mental health funding allocations that cannot be estimated at this time.
(i) Inpatient beds
Acute inpatient beds
Since the commencement of Australia’s National Mental Health Strategy in 1992, jurisdictions have converged toward an acute bed provision level of around 20 per 100,000 population, the recommended level. The lower planning benchmark recommended by the Tolkien II report (11.0 beds per 100,000) (Andrews and the Tolkien II Team, 2007) is not inclusive of all disorders and age groups and does not include provision for unpredictable crisis admissions. It also assumes optimal practice and hence is unlikely to constitute an achievable planning norm. The upper benchmark proposed by the Sainsbury Centre in England (35.2 beds per 100,000) (Boardman and Parsonage, 2005) reflects traditionally higher acute inpatient service provision and a relative absence of private sector inpatient options in England. The Sainsbury Centre target decreases from 35 to 26 beds per 100,000 when adjusted to take account of Australia’s private sector provision, closer to the recommended level. That said, pressures on acute psychiatric inpatient units within all jurisdictions, resulting in high occupancy rates and lack of access to services to consumers in acute need, have raised doubts about whether current acute inpatient service levels are adequate. This largely reflects broader failures of the system, and particularly, inadequate provision of service elements that offer alternatives to inpatient care (Andrews, 2005).
Non -acute beds
The diversity in service provision and planning norms for non-acute inpatient provision within Australia stems from different rates of progress between jurisdictions in addressing the legacy of large stand-alone psychiatric hospitals and differences in the extent to which community-based residential rehabilitation alternatives to long-term hospital care are specified as core service components within service plans. The recommended benchmark (10 beds per 100,000) matched the national average level, but was 65% below Queensland provision in 2005. The recommendation was justified on the expectation that, in a balanced service system, non-acute inpatient services are required by a relatively small number of individuals who need longer-term rehabilitation or care in a secure setting. The majority of bed-based rehabilitation should be delivered in community residential settings. Recommended levels for non-acute inpatient services therefore need to be examined in the context of related services, particularly 24-hour clinically staffed residential units. Both Victoria and Tasmania have already moved in the direction of locating most bed-based, 24-hour services within community residential units (Department of Health and Ageing, 2007).
(ii) Adult residential rehabilitation services
The resource targets for this component focus on the general adult population (16–64 years) and do not cover requirements for older persons’ services. Benchmarks for aged residential mental health care depend largely on broader policy decisions about the relative roles of the aged care and specialised mental health sectors. Queensland is one of several Australian jurisdictions that place responsibility for most longer-term residential mental health care for older persons within the aged care sector. The recommended benchmarks were higher than all Australian jurisdictions and substantially above Queensland 2005 levels, in recognition of the broad consensus that residential alternatives to inpatient care require priority development across Australia.
Residential rehabilitation – clinical, 24-hour staffed
The recommended planning benchmark for these services (10 beds per 100,000) was based on a notional 40:60 split of the overall residential bed target between clinical and non-clinically staffed units. It represented a five-fold increase over Queensland service levels in 2005.
Residential rehabilitation – non-clinical
Based on the experience of other jurisdictions, the majority of residential rehabilitation services can be delivered in units staffed by non-clinical workers and managed by NGOs. The recommended target (18 beds per 100,000) was approximated by the leading Australian jurisdiction in this area (ACT) and fell within the range of benchmarks summarised in Table 6. Queensland had no funded services of this type within its public mental health system at the time this work was undertaken.
(iii) Supported accommodation
Two technical obstacles limited the precision of estimates for this component. The first is that planning benchmarks for supported accommodation were poorly delineated in all planning documents reviewed in this project. In particular, there were few guides to determining an appropriate split between supervised hostel accommodation and supported housing places. Further, responsibility for supported accommodation is variably distributed between health and other human service portfolios. Thus, the extent to which accommodation is provided by government is often hidden because it is not included in either mental health planning targets or the various statistics published by governments on mental health service provision levels.
The recommended targets and relative splits between the two core accommodation elements were based on evidence that most mental health consumers prefer independent living to group living arrangements where, if assistance is required, it is provided on a visiting, in-home basis (National Mental Health Housing Association, 2004; NSW Health Department, 2002; Sainsbury Centre for Mental Health, 1997). The targets recognised that a significant number of mental health consumers are disabled to the extent that independent housing is impractical. For these people some level of supervision with day-to-day activities is necessary.
Supervised hostel-type accommodation
The resource targets allocated 50% of total supported accommodation places to supervised hostels (35 places per 100,000). These places represent a special subset of the broader category of private residential services (boarding houses, hostels) that are operated by the for-profit and not-for-profit private sectors in all Australian jurisdictions. While they do not usually attract government subsidies, there is increasing recognition that governments have a responsibility to provide funding to increase the level of care provided by operators who provide accommodation to a significant number of people disabled by mental disorders. Two Australian states (Victoria and Western Australia) had taken this lead in this area; similar steps had not been taken in Queensland.
The recommended target translates to approximately 1400 subsidised hostel places when applied to the 2005 Queensland population. Information about the number of people with mental disorders accommodated in the private hostel-style residential system was not available for Queensland, or for other jurisdictions, but was expected to be significant.
Supported public housing
Precedent for these services in Queensland was established by Project 300, a landmark initiative that focused on resettling up to 300 long-term patients from stand-alone psychiatric hospitals (Meehan et al., 2001). The principles underpinning this model of service delivery have also been endorsed in several Queensland Government housing policy-related papers (Queensland Department of Housing, 2000, 2001). Recommended targets for supported public housing (35 places per 100,000) would require major resource investments if implemented. However, both the direction for service development and the level of services needed are consistent with national and international trends.
Under the COAG National Action Plan on Mental Health (Council of Australian Governments, 2006), several Australian states and territories committed additional funds to expanding community accommodation options that involve some form of partnership between public housing providers and specialist mental health services. Of particular relevance, Victoria – the second leading provider in this area with 29 places per 100,000 in 2005 - has committed $39 million to the non-government sector over 5 years to expand home-based support services. New South Wales (23 places per 100,000 in 2005) similarly has committed $59 million to expand its Housing Accommodation and Support Initiative. Western Australia, with 18 places per 100,000 available in 2005, announced that it will establish an additional 60 housing units per year for its Independent Living Programme. The Queensland Government committed $20 million in capital funding to procure accommodation for people with mental disorders linked to in-home support provided through NGOs.
(iv) Ambulatory care clinical services
The recommended target (70 clinical workers per 100,000) was based on the view that Australia has significantly under-estimated the public sector clinical workforce needed to provide modern, comprehensive mental health services in the community. At the commencement of the National Mental Health Strategy, when the workforce comprised 19 workers per 100,000, a target of 30 per 100,000 was widely regarded as the ‘ideal’ (Andrews, 1991). Although this target was achieved by most jurisdictions by the mid-1990s, substantial gaps remained (AHMAC National Mental Health Strategy Evaluation Steering Committee, 1997). By 2005, national average service provision reached 38 clinical workers per 100,000 but the available planning benchmarks supported the view that this level is not adequate to meet demands in any jurisdiction.
(v) NGO-managed community support (non-clinical) services
The lack of planning benchmarks for the NGO sector is partly due to the fact that the diverse range of service types covered by the sector (such as mutual support groups, day programs, home visiting programs, support services for carers, and ‘drop-in’ recreational services) cannot be distilled to a simple planning metric. However there is broad consensus that these services are essential components of a publicly funded mental health system (Pirkis et al., 2007).
The recommended target (15% of total mental health funding) indicates the broad quantum of investment needed to develop a system of care that balances the clinical care and broader community support needs of mental health consumers. It also recognises the need to develop an alternative mental health sector workforce that complements and, in specific areas, can substitute for the clinical professions. Reliance on clinical health professionals alone will be insufficient to bridge mental health workforce gaps over the next 5–10 years.
The ACT and Victoria were the highest providing jurisdictions in 2004–05 (Department of Health and Ageing, 2007), at 13.0% and 10.2% respectively (approximately double the Queensland level of 6.4%). New Zealand invests approximately 30% of its mental health investment in community support services provided by the NGO sector (New Zealand Mental Health Commission, 2004). Along with other jurisdictions, Queensland has also committed to substantial increases to the sector as part of its contribution to the COAG National Action Plan on Mental Health.
Discussion
This paper outlines the process for developing resource targets for the provision of core public mental health services in Queensland over the period 2007–2017. Resource targets for five core mental health service components were recommended, based on Australian and international precedents and best available evidence regarding levels of community mental health need, supplemented by value judgements and expert opinion as required.
The recommended targets pointed to specific priority areas. Firstly, the shortfall in acute inpatient beds (13% below the recommended 20 beds per 100,000) was fully attributable to the relative lack of acute inpatient services for older people. Specialist older persons’ inpatient beds were provided by Queensland at only half the average of other jurisdictions. Future expansion in acute bed capacity, beyond that required for general population growth, needs to focus largely on expansion of specialist services for the older population. Secondly, given that most bed-based rehabilitation should be delivered in community residential settings, a reconfiguration of services was recommended to increase the number of 24-hour clinically staffed residential beds (from 2 to 10 per 100,000) and reduce non-acute inpatient beds (from 20 to 10 per 100,000). Thirdly, to establish non-clinical residential rehabilitation services (18 beds per 100,000), staffed by non-clinical workers and managed by NGOs. Fourthly, to allocate resources to the establishment of supported public housing models of service delivery. Fifthly, to make available additional positions to build to a doubling of the ambulatory care clinical workforce. Sixthly, to develop an alternative mental health sector workforce to support the recommended expansion of the NGO sector.
Both locally and internationally, there have been repeated calls for more evidence-based approaches to mental health planning and greater scrutiny of the way in which government decisions about investment in mental health services are made (Chisholm et al., 2007; Rosenberg et al., 2012; World Health Organization, 2004). Health planners must make the bases for their planning estimates transparent and policy-makers must be able to demonstrate and debate the evidence upon which their decisions are made (Chipps et al., 2000). This paper makes a contribution towards greater transparency in mental health planning by describing the assumptions, data sources, methods and findings used to develop resource targets for public mental health services in Queensland, which subsequently informed policy decisions by government. The resource targets recommended by this project were endorsed by the Queensland Government and specified in the current Queensland Plan for Mental Health (Queensland Health, 2008) which guides that state’s service planning for the 19-year period 2007–2017.
Methodological considerations
The recommendations were prepared with several caveats. Firstly, the present paper describes a service development planning exercise, which applies best available evidence to quantify the need for mental health services and to determine the average quantum of resources required to meet that need for a large (state) population, while at the same time being flexible enough to allow for the needs of local populations and variations in service provision costs, such as in rural and remote Australia, at the implementation stage. The targets are suggested as guidelines for identifying the broad directions and priorities for service development, rather than strict planning formulas. The implementation of the targets was beyond the scope of this project.
Secondly, the resource targets were specified at a ‘whole of population’ level and did not drill down to age-specific treatment populations. The targets would need to be interpreted flexibly when applied to smaller populations (e.g., Queensland districts), taking into account the local service context and sociodemographic factors known to affect community need for mental health care.
Thirdly, there was no single authoritative source for many of the estimates presented in this paper, for example, the age- and severity-specific disorder prevalence (derived from MH-CCP which, in turn, used local and international sources to ensure complete coverage of the population), and the proportions of individuals receiving care from different parts of the health system. We have drawn on multiple sources, and where necessary, made informed estimates where the data were ambiguous or incomplete. In some cases, we relied on studies of small size or inadequate coverage, however, as already noted, this represents the reality of mental health service planning. Nonetheless, this raises questions about the implications of relying on data from multiple, including overseas, sources and how the availability of data required for population mental health planning could be improved. Relying on multiple information sources is usual practice in population health planning. The combined use of survey and administrative data provides an optimal estimation of the population need for mental health care because it maximises the advantages of each (Drapeau et al., 2011). For example, service- or program-based registers or databases can provide detailed information about the population who use those services and the amount or nature of the services they receive, but do not contain information about people who did not use those services. Population surveys, on the other hand, may provide a more detailed profile of the population’s mental health status (e.g., their diagnostic profile or other indicators of need) but may not be able to capture detailed information about the use of particular service types or programs, and may be subject to recall bias and social desirability. Bringing together multiple sources may introduce uncertainty in the estimates obtained, although uncertainty can be measured and uncertainty intervals placed around these estimates (see Pirkis et al. (2011) for an example). Some instances of uncertainty, an example in this paper being uncertainty in the overlap between persons using Commonwealth and state mental health services, could potentially be addressed by record linkage across relevant service datasets (Pirkis et al., 2011). There are other strategies that may be useful for improving the availability of the data necessary for planning. One option might be the development of a national research agenda driven by mental health planning requirements. This might include, for example, greater alignment of the epidemiological and service utilisation information collected in national surveys with the information required for mental health service planning. It might also involve targeted research projects to gather information not otherwise available, for example a nationally representative profile of the characteristics of individuals receiving privately funded psychiatric care.
Fourthly, this paper presents the results of a planning exercise carried out in 2006, prior to availability of data from the 2007 NSMHWB and the introduction of major reforms to the primary mental health care sector. Queensland data regarding primary care activity were not readily available at the time, however even if they were they may not necessarily have provided an accurate basis for prediction of future activity. Initiatives included as part of the Council of Australian Governments (COAG) Action Plan for Mental Health (Council of Australian Governments, 2006), notably the introduction of the Better Access to Psychiatrists, Psychologists and GPs through the Medicare Benefits Schedule initiative, have resulted in substantially increased levels of primary mental health care activity (Whiteford et al., 2008) which could not have been predicted, but need to be monitored over time. However, these changes have occurred largely outside the public sector with which this paper is principally concerned, and their impact on public sector service provision is likely to have been minimal. This paper also does not take account of more recently published planning documents in which resource targets have been specified (Department of Health and Children, 2006; South Australian Social Inclusion Board, 2007). Revision of the estimates would need to take into account the impact of moving inputs such as changes to rates and patterns of mental health service utilisation. Moreover, progress towards these targets is monitored and was recently reported in the Queensland Plan for Mental Health 2007–2017 Four Year Report (Queensland Health, 2008) released in October 2011. The resource targets recommended by this project also provided a basis for subsequent work conducted by our group to develop resource targets for the Queensland mental health community support sector (Siskind et al., 2012).
Future directions
The targets recommended in this study were based on interpretation of trends in national and international planning. They are imprecise and will need to be tested against experience as new services are developed. The absence of nationally agreed planning targets for mental health services is acknowledged as a shortcoming of Australia’s National Mental Health Strategy to date. This has been largely due to concerns about structural differences between jurisdictions and the political risk entailed in agreeing to national planning targets. This deficit is set to be addressed under the Fourth National Mental Health Plan – An agenda for collaborative government action in mental health 2009–2014 (the Fourth Plan) (Australian Health Ministers, 2009), endorsed by all jurisdictions on 4 September 2009. Under the Fourth Plan, the Commonwealth and all state and territory governments have committed to develop a national service planning framework that establishes targets for the mix and level of mental health services, including primary care and community support services. To achieve this, the Department of Health and Ageing has funded a 2-year National Mental Health Service Planning Framework Project, jointly led by the NSW Ministry of Health and Queensland Health. The project will build on the New South Wales MH-CCP models and is due to be completed in 2013. We found considerable controversy about service definitions and boundaries, particularly with respect to supported accommodation and community residential rehabilitation services. These issues will be addressed within the National Mental Health Service Planning Framework and by a related national project led by the Australian Institute of Health and Welfare to develop a taxonomy of specialised mental health community support services.
Footnotes
Funding
This project was funded by the Mental Health Branch, Queensland Health.
Declaration of interest
AG was the Executive Director of the Mental Health Alcohol and Other Drugs Directorate, Queensland Health. All other authors declare no conflict of interest.