
Abstract
Objective:
A key step in informing mental health resource allocation is to identify the predictors of service utilisation and costs. This project aims to identify the predictors of mental health-related acute service utilisation and treatment costs in the year following an acute public psychiatric hospital admission.
Method:
A dataset containing administrative and routinely measured outcome data for 1 year before and after an acute psychiatric admission for 1757 public mental health patients was analysed. Multivariate regression models were developed to identify patient- and treatment-related predictors of four measures of service utilisation or cost: (a) duration of index admission; and, in the year after discharge from the index admission (b) acute psychiatric inpatient bed-days; (c) emergency department (ED) presentations; and (d) total acute mental health service costs. Split-sample cross-validation was used.
Results:
A diagnosis of psychosis, problems with living conditions and prior acute psychiatric inpatient bed-days predicted a longer duration of index admission, while prior ED presentations and self-harm predicted a shorter duration. A greater number of acute psychiatric inpatient bed-days in the year post-discharge were predicted by psychosis diagnosis, problems with living conditions and prior acute psychiatric inpatient admissions. The number of future ED presentations was predicted by past ED presentations. For total acute care costs, diagnosis of psychosis was the strongest predictor. Illness acuity and prior acute psychiatric inpatient admission also predicted higher costs, while self-harm predicted lower costs.
Discussion:
The development of effective models for predicting acute mental health treatment costs using existing administrative data is an essential step towards a workable activity-based funding model for mental health. Future studies would benefit from the inclusion of a wider range of variables, including ethnicity, clinical complexity, cognition, mental health legal status, electroconvulsive therapy, problems with activities of daily living and community contacts.
Introduction
There is increasing agreement that, in an environment of resource constraints, mental health service allocation should be informed by the costs and benefits of health interventions (Roberts and Jackson, 2013). A key step in informing mental health resource allocation is to identify the factors that predict mental health-related service utilisation and treatment costs. Acute treatment services are one area of particular importance. During periods of high illness acuity, people living with mental illness may present to acute services such as acute psychiatric inpatient units and emergency departments (EDs). Acute mental health services are a core component of the mental health service system and account for a high proportion of Australian public mental health service costs (Department of Health and Ageing, 2013).
Studies have examined a range of patient-related and treatment factors that may be predictive of mental health treatment costs, or service utilisation measures that may serve as proxies for cost, such as duration of psychiatric admission. A systematic review of predictive studies of these mental health care costs (Jones et al., 2007) found that age, diagnosis, sex, previous psychiatric service utilisation and past psychiatric history were the most consistent predictors of future service costs or utilisation, being significant in over half of the included studies. The review also noted that in some studies diagnosis and disease severity were not strongly predictive and explained little variation in costs, and that the direction of effect of age, sex and diagnosis differed between studies.
A 2013 review of mental health treatment costs (Harris et al., 2013) identified additional predictors that have been consistently found in recent predictive and cross-sectional studies, namely: ethnicity (Han et al., 2011; Robst, 2009; Rothbard et al., 2005; Wu et al., 2012); employment status (Alimohamed-Janmohamed et al., 2010; Baca-Garcia et al., 2008; Donisi et al., 2011); education status (Alimohamed-Janmohamed et al., 2010; Grigoletti et al., 2010; Han et al., 2011); accommodation arrangements (Fontanella, 2008; Grigoletti et al., 2010; Salize et al., 2009); marital status (Bonizzato et al., 2000; Han et al., 2011); illness severity (Fontanella, 2008; Salize et al., 2009; Warnke et al., 2011); risk of harm to self or others (Boot et al., 1997; Buckingham et al., 1998; Cromwell et al., 2005; Drozd et al., 2006; Fontanella, 2008); comorbid substance abuse (Seder, 2010); and functional impairment or disability (Alimohamed-Janmohamed et al., 2010; Amaddeo et al., 2007; Baca-Garcia et al., 2008; Forma et al., 2009).
There have been only limited attempts to date to evaluate predictors of acute mental health service use or cost in the Australian context. The 1998 Mental Health Classification and Service Costs (MH-CASC) project used data from 22 participating Australian public and private integrated mental health services, and identified clinical severity, psychosocial functioning, age, diagnosis and activities of daily living (ADLs) as predictors of the cost of acute and community episodes of service (Buckingham et al., 1998). MH-CASC attempted to create a casemix classification for Australia. Although this was not adopted in Australia, it led to the introduction of the National Outcomes and Casemix Collection (NOCC), a set of routine outcome measures for use by all Australian state and territory mental health services.
Kisely et al. (2000) subsequently analysed MH-CASC data from two west Australian public mental health services and identified receipt of pension, past inpatient care, schizophrenia, and poorer functional ability as predictors of longer duration of care; and receipt of pension, involuntary status, inpatient stay, higher illness acuity and poorer functional ability as predictors of higher community and acute treatment costs (Kisely et al., 2000).
More recently, the Australian Independent Hospital Pricing Authority (IHPA) commissioned a report involving an analysis of mental health service cost drivers from routine administrative data (Eagar et al., 2013). Predictors of costs for inpatient service episodes (excluding residential care) included diagnosis, complications and comorbidities, Mental Health Act status, symptom severity, functioning and the occurrence of procedures and electroconvulsive therapy (ECT).
Carr et al. (2004) used purpose collected survey data from the 1997 Low Prevalence Disorders Study survey to examine total mental health costs for people with psychosis, which were the sum of acute and community service costs and indirect government and societal costs (Carr et al., 2004). Completion of high school, sex, age, a non-English-speaking background, family and support, previous marriage, illness onset and chronicity, self-harm and current symptoms were associated with change in total costs.
Few studies have focused solely on predictors of acute service cost or have looked at costs over an extended period, rather than per episode of care. By examining predictors of acute costs over a 1-year period, there is the potential to identify strategies that may reduce patients’ acute mental health service needs and avert the high associated costs.
This paper aims to identify predictors of mental health-related acute service utilisation and acute service costs in the 12 months following acute psychiatric inpatient admission (identified for this study as the index admission), using a sample of mental health service patients admitted to Queensland acute metropolitan public mental health facilities from 2006 to 2009. The perspective of the study was from that of the government, as the funder of public sector mental health services. Only direct health service costs relating to treatment of acute mental illness were included.
This study aimed to identify patient- and treatment-related factors that predict:
the duration of index acute psychiatric inpatient admission;
the number of acute psychiatric inpatient bed-days in the year after discharge from index admission;
the number of ED presentations for mental health patients in the year after discharge from index admission; and
acute mental health-related service costs for the index admission and year after discharge from index admission.
Methods
Sample and data sources
The sample comprised 1757 unique patients with an index admission to any one of the four public acute mental health units in two contiguous hospital districts covering all of the inner and outer north and west of greater metropolitan Brisbane (a population of approximately 1,000,000 people or approximately half of the population of greater metropolitan Brisbane), between April 2006 and March 2009. These patients had been selected as controls for previous retrospective quasi-experimental studies of sub-acute and non-acute supported housing programs (Siskind et al., 2013, 2014).
Controls were drawn from all mental health patients admitted to the four hospitals in the time period, and were first matched with intervention participants on sex, diagnostic group (psychosis, anxiety disorder, affective disorder or other) and time of intervention. Diagnoses were based on the International Classification of Diseases, 10th Revision (ICD-10) coded administrative discharge diagnoses for the index admission, drawn from the Queensland Hospital Admitted Patient Data Collection (QHAPDC). Diagnoses were divided into Psychosis (ICD-10 codes F20–29) and Other (ICD-10 codes: affective disorders (F30–39), anxiety disorders (F40–43), personality disorders (F60), pervasive developmental disorders (F84), and substance use disorders (F10–19)). Only the primary coded diagnosis was used. From this matched group, a random sample was drawn. Ethics approval was granted from the Metro South Human Research Ethics Committee (HREC), University of Queensland School of Population Health Research Ethics Committee and Queensland Health Research and Governance Unit.
The dataset of included patients was drawn from three linked, de-identified administrative datasets: QHAPDC, which contained socio-demographic factors, hospital admissions and bed-days; the Consumer Integrated Mental Health Application dataset, which contained routinely collected illness acuity measures including data on problems with living conditions, self-harm and substance abuse; and the Emergency Department Information System dataset, which contained the number of presentations to EDs.
Data were extracted on the included patients for the year before the index admission date, and for a year following the index admission discharge date.
Outcome variables
This study examined predictors of three service utilisation variables: (1) duration of index admission, which was defined as the number of acute psychiatric inpatient bed-days for the index admission to any of the four acute mental health units included in this study; (2) acute psychiatric inpatient bed-days in the year after discharge, which was defined as the cumulative number of bed-days for acute psychiatric inpatient admissions to any public acute psychiatric inpatient unit in Queensland; and (3) ED presentations in the year after discharge, which was defined as the number of presentations to EDs in any public ED in Queensland.
The study also examined predictors of the total cost for acute mental health service utilisation, which was calculated as the sum of the per diem costs of acute psychiatric inpatient bed-days during the index admission, sum of the per diem costs of acute psychiatric inpatient bed-days in the year after discharge from the index admission, plus the episode costs of the total ED presentations in the year after index admission. Using hospital inpatient and ED pricing data for Queensland, the reimbursable per diem cost of an acute psychiatric inpatient bed-day in 2009 was estimated to be AU$1111.82, and the episode cost of an ED presentation was estimated to be $601.05 (Siskind et al., 2013). These costs were based on the hospital remuneration for provided services.
Predictor variables
Potential predictor variables were identified from the literature, and corresponding variables identified in our data extract. These were: age (continuous); sex (dichotomous); primary diagnosis at discharge from index admission (psychosis vs other); indigenous status (indigenous vs non-indigenous); marital status (single vs married/de facto); illness acuity (i.e. severity of symptoms), as indicated by the highest total Health of the Nation Outcome Scale (HoNOS) (Wing et al., 1998) score in the year before the index admission (continuous); self-harm, as indicated by the highest score on question 2 of HoNOS in the year before the index admission (continuous); substance abuse, as indicated by the highest score on question 3 of HoNOS in the year before the index admission (continuous); problems with living conditions, as indicated by the highest score on question 11 of HoNOS in the year before the index admission (continuous); acute psychiatric inpatient bed-days in the year before the index admission (continuous); and the number of ED presentations in the year before the index admission (continuous).
Statistical analyses
A series of regression analyses was performed to identify patient- and treatment-related predictors of each of the four outcome variables described above. Cross-validation has been identified as a best practice approach for predicting service costs (Jones et al., 2007). The dataset was randomly split into two equally sized sets. The first set was used as a ‘training’ set to test individual candidate predictor variables and to build a multivariate model. The second set was used as a ‘validation’ set to evaluate the predictive capability of the multivariate model (Kilian et al., 2002). Service utilisation and cost data can be challenging to analyse as they usually have non-normal heteroscedastic distributions and over-dispersed count variables (Jones et al., 2007). Negative binomial regression is a statistical method for examining predictive relationships with a count-dependent model. It can be used with non-normal heteroscedastic distributions and over-dispersed count variables that cannot be transformed to approximate normality (Elhai et al., 2008).
None of the three service utilisation outcome variables were normally distributed, each having a skewed distribution and a long right tail and could not be transformed to approximate normality. Using the ‘training’ set, a series of univariate negative binomial regression analyses were run using the predictor variables for each of three service utilisation outcomes: duration of index admission (in days); number of days spent in an acute psychiatric hospital in year after discharge from the index admission (in days); and number of ED presentations in the year after the index admission. Predictor variables associated with a change in each outcome variable at or below the 0.05 probability level in the univariate analyses were selected for use in subsequent multivariate models. Using the ‘validation’ set, a multivariate negative binomial analysis for each of the three service utilisation outcomes was conducted using the selected predictor variables. Model goodness of fit could not be estimated, as R2 cannot be calculated from a multivariate negative binomial analysis.
The total mental health service cost data was not normally distributed, with a skewed distribution and a long right tail, but was able to be log transformed to improve the performance of the regression model (Diehr et al., 1999). Ordinary least squares univariate regression analyses were run on the log transformed total acute mental health service cost data using the predictor variables and the ‘training’ data set. Predictor variables at or below the 0.05 probability level in the univariate analyses were selected for use in subsequent multivariate models. A multivariate ordinary least squares regression model using the selected predictor variables on log transformed total mental health service costs was conducted using the ‘validation’ set. B values were exponentiated to aid interpretation. An R2 value was calculated for the model to provide an estimate of the goodness of fit.
Results
Within the two similarly sized groups, the ‘training’ group had 879 unique patients with an acute psychiatric inpatient admission in the study period, while the ‘validation’ group had 878 unique patients. There was no statistically significant difference between the two groups on any of a range of demographic, diagnostic and functional status, service utilisation, or cost variables, as shown in Table 1. Costs were highest for the index admission, followed by the costs for acute psychiatric inpatient bed-days and ED presentations in the year after the index admission.
Demographics and service utilisation.
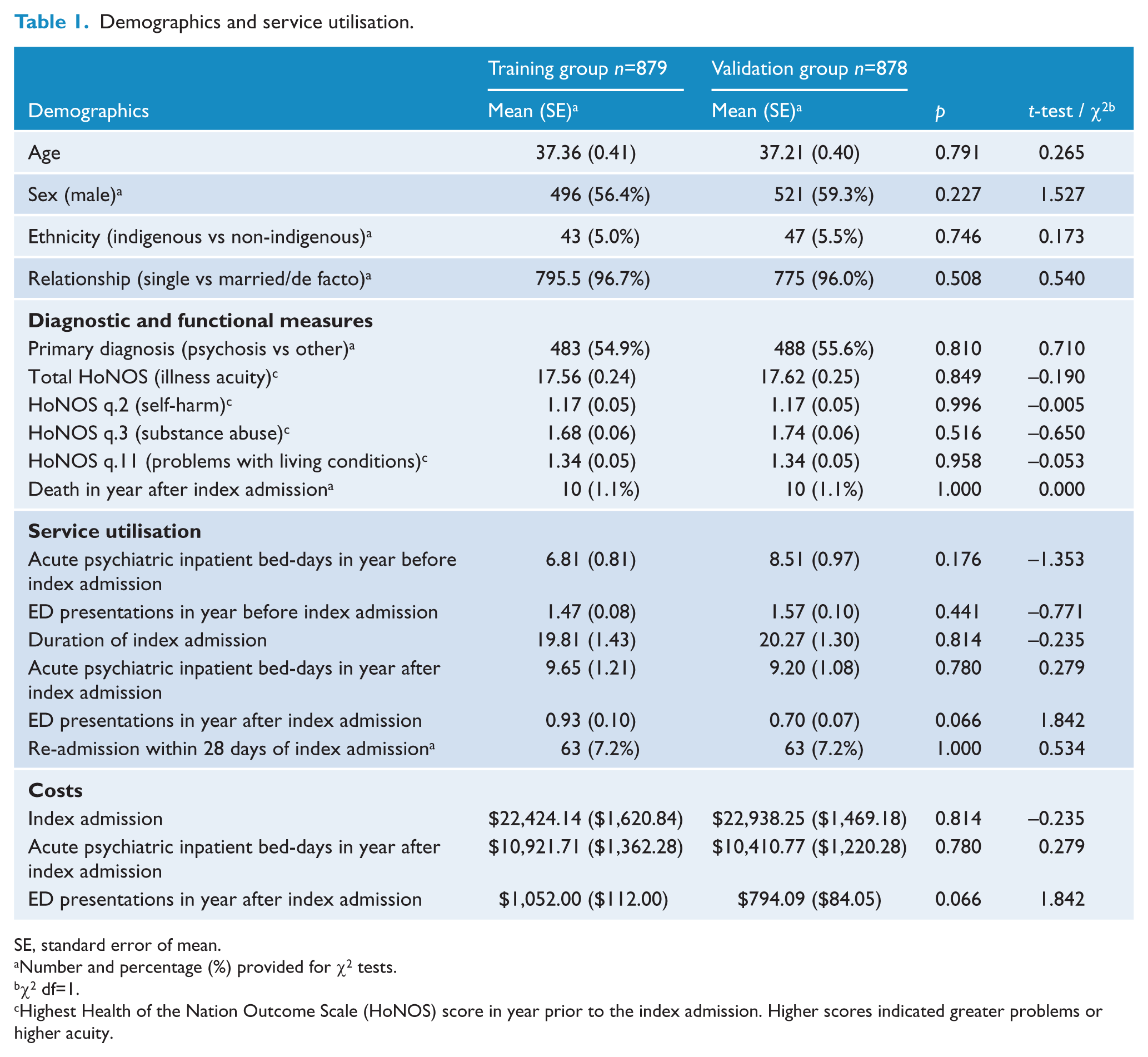
SE, standard error of mean.
Number and percentage (%) provided for χ2 tests.
χ2 df=1.
Highest Health of the Nation Outcome Scale (HoNOS) score in year prior to the index admission. Higher scores indicated greater problems or higher acuity.
Predictors of service utilisation
In univariate analyses undertaken to identify predictor variables associated with a change in duration of index admission, at or below the 0.05 probability level, age, primary diagnosis, ethnicity, self-harm, problems with living conditions, acute psychiatric inpatient bed-days in the year before the index admission and ED presentations in the year before the index admission were identified. Predictor variables associated with a greater number of acute psychiatric inpatient bed-days in the year after discharge, at or below the 0.05 probability level, were primary diagnosis, total HoNOS, problems with living conditions and acute psychiatric inpatient bed-days in the year before the index admission. Predictor variables associated with a greater number of ED presentations in the year after discharge, at or below the 0.05 probability level, were primary diagnosis, sex, total HoNOS and ED presentations in the year before index admission.
Separate multivariate negative binomial regression models were developed for each of the three service utilisation outcomes. For each model, predictor variables included were those associated with the outcome at or below the 0.05 probability level. Results are shown in Table 2. Significant predictors of duration of index admission were primary diagnosis, self-harm, problems with living conditions, acute psychiatric inpatient bed-days in the year before the index admission and ED presentations in the year before the index admission. The duration of the index admission for patients with psychotic disorders was 1.63 times greater than for those with other diagnoses. For every 1 point increase on question 2 of HoNOS (self-harm), the duration of index admission decreased by 15.7%, while for every 1 point increase on question 11 of HoNOS (problems with living conditions), the duration of index admission increased by 8.6%. For every additional acute psychiatric inpatient bed-day in the year before the index admission, the duration of the index admission increased by 0.9%. For every additional ED presentation in the year before the index admission, the duration of the index admission decreased by 6.6%.
Predictors of service utilisation using multivariate negative binomial regression a .
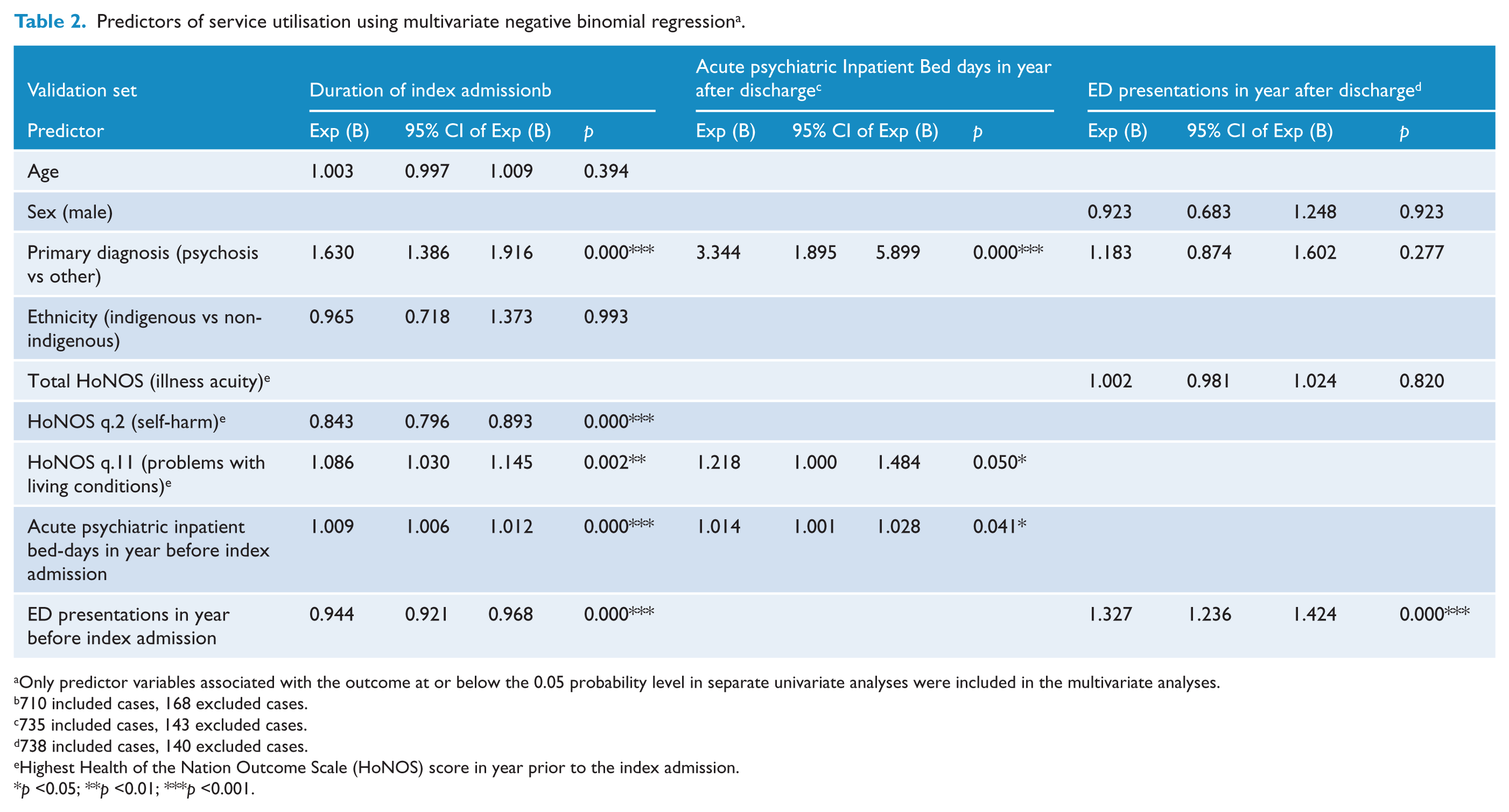
Only predictor variables associated with the outcome at or below the 0.05 probability level in separate univariate analyses were included in the multivariate analyses.
710 included cases, 168 excluded cases.
735 included cases, 143 excluded cases.
738 included cases, 140 excluded cases.
Highest Health of the Nation Outcome Scale (HoNOS) score in year prior to the index admission.
p <0.05; **p <0.01; ***p <0.001.
Significant predictor variables in the multivariate negative binomial regression of number of acute psychiatric inpatient bed-days in the year after discharge were primary diagnosis, problems with living conditions and acute psychiatric inpatient bed-days in the year before the index admission. The number of acute psychiatric inpatient bed-days in the year after discharge was 3.34 times greater for patients with psychotic disorders than for those with other diagnoses. For every 1 point increase on question 11 of HoNOS (problems with living conditions), the number of acute psychiatric inpatient bed-days in the year after discharge increased by 21.8%. For every additional acute psychiatric inpatient bed-day in the year before the index admission the number of acute psychiatric inpatient bed-days in the year after discharge increased by 1.4%.
The only significant predictor variable in the multivariate negative binomial regression of number of ED presentations in the year after discharge was ED presentations in the year before the index admission. For every additional ED presentation in the year before the index admission, the number of ED presentations in the year after discharge increased by 32.7%.
Predictors of acute mental health care costs
In univariate analyses, predictor variables associated with a change in log transformed total acute mental health service cost, at or below the 0.05 probability level, were age, primary diagnosis, illness acuity, self-harm, problems with living conditions, acute psychiatric inpatient bed-days in the year before the index admission and ED presentations in the year before the index admission.
A similar procedure was used to develop a multivariate ordinary least squares regression model for total acute mental health care costs. Results are shown in Table 3. Significant predictors of log transformed total acute mental health service costs were primary diagnosis, illness acuity, self-harm and acute psychiatric inpatient bed-days in the year before the index admission. Total acute mental health costs were twice as high for patients with psychosis diagnoses compared to other diagnoses. For every 1 point increase on total HoNOS score, the total acute mental health costs increased by 2.3%. For every 1 point increase on question 2 of HoNOS (self-harm), the total acute mental health costs decreased by 13.4%. For every additional acute psychiatric inpatient bed-day in the year before the index admission, the total acute mental health costs increased by 0.8%. The model explained 21.8% of the variance (R2 = 0.218) of transformed total acute mental health service costs. This was similar to the explanatory power of the model when applied to the training set, which had an R2 of 0.226.
Multivariate linear regression of log transformed total acute service costs a .
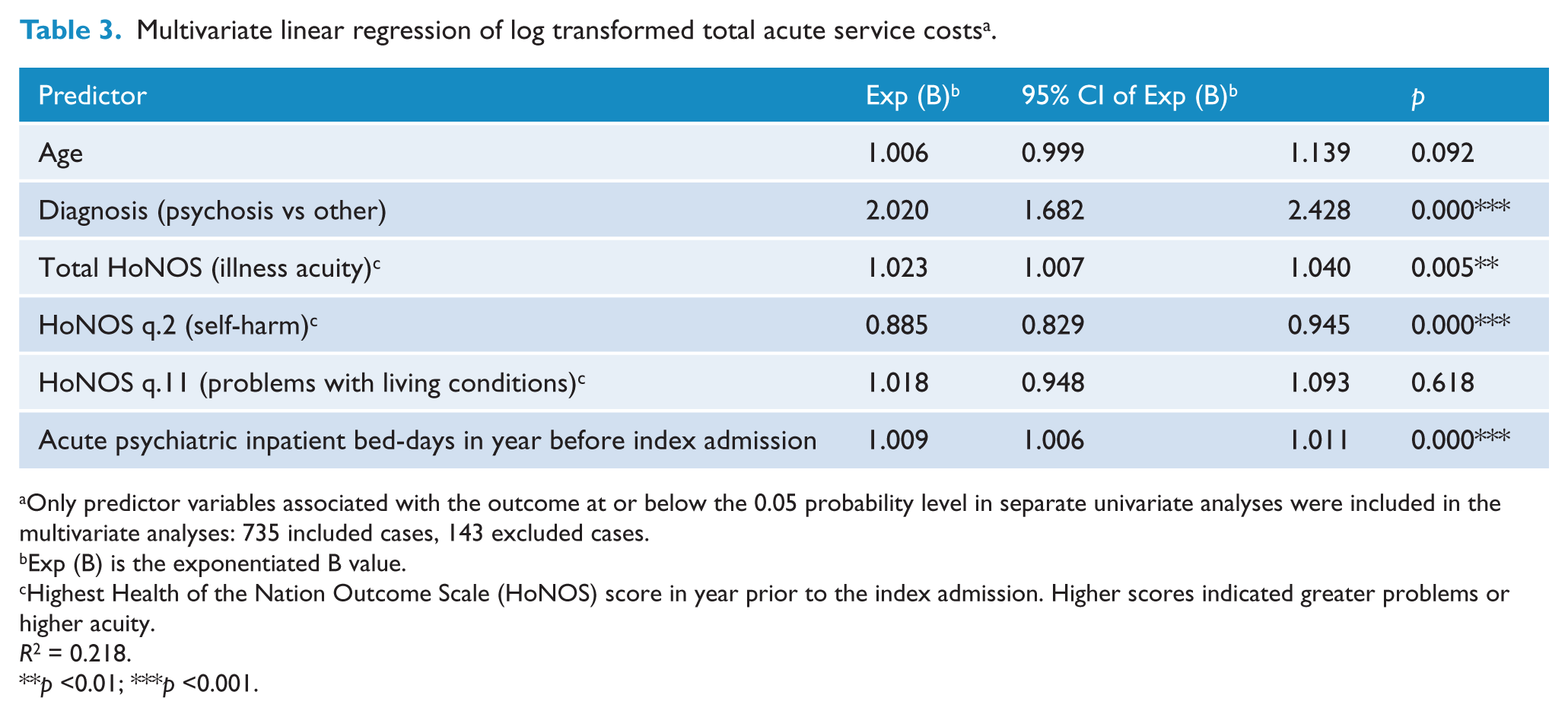
Only predictor variables associated with the outcome at or below the 0.05 probability level in separate univariate analyses were included in the multivariate analyses: 735 included cases, 143 excluded cases.
Exp (B) is the exponentiated B value.
Highest Health of the Nation Outcome Scale (HoNOS) score in year prior to the index admission. Higher scores indicated greater problems or higher acuity.
R2 = 0.218.
p <0.01; ***p <0.001.
Missing data
As shown in the footnotes to Tables 2 and 3, between 16% and 19% of patients were excluded from each multivariate analysis due to missing data. Missing data were primarily due to incomplete HoNOS ratings. In the Validation Group, 14.0% of HoNOS question 2, 17.2% of HoNOS question 3, 16.3% of HoNOS question 11 and 15.9% of total HoNOS had missing values. Patients with at least one missing total HoNOS or missing individual HoNOS question (n=154) were compared to patients with complete HoNOS data (n=724). There was no statistically significant difference between these groups in terms of sex, ethnicity, relationship status, ED presentations in the year before the index admission, duration of acute psychiatric inpatient index admission, or acute psychiatric inpatient bed-days in the year after the index admission. Patients with missing HoNOS data were significantly less likely to have had an acute psychiatric inpatient admission in the year before the index hospitalisation (8.4% vs 28.6%, χ2 = 27.46, p <0.001), and were more likely to have a non-psychotic diagnosis (55.8% vs 42.0%, χ2 = 9.87, p = 0.002).
Discussion
Principal findings
This study found that a diagnosis of psychosis, greater problems with living conditions and prior acute psychiatric inpatient admissions predicted greater acute psychiatric inpatient bed-days both during the index admission and in the year after discharge. A higher number of reports of self-harm and ED presentations predicted a shorter index inpatient episode length of stay. The identification of patient characteristics that influence acute service utilisation and costs can inform the development and implementation of interventions that may reduce patients’ needs for acute mental health services and avert the high cost of services associated with extended admissions and readmissions. Four key findings from this study, and their implications for clinicians and service administrators, are discussed below.
First, problems with living conditions were identified as predictors of both extended admissions and readmissions. This is consistent with findings from other studies (Fontanella, 2008; Grigoletti et al., 2010; Salize et al., 2009). Programs that address access to suitable housing and improved social support should reduce problems arising from suboptimal living conditions (Siskind et al., 2013, 2014). Services run by government and/or non-government agencies such as sub-acute short-term housing or respite options could assist health services in reducing treatment costs.
Second, although ED presentations predicted shorter length of stay, they also were the only variable predictive of ED presentations, with each ED presentation predicting a one-third increase in the number of ED presentations in the year after discharge. Two other studies found that the presence of comorbid conditions is predictive of higher ED use (Bagalman et al., 2011; Wu et al., 2012). Younger age was examined in one study and found to be a positive predictor of ED use (Bagalman et al., 2011). While it would be challenging to create a funding model for ED presentations with prior ED presentations as the sole predictor, this information may be of use to service managers looking for strategies to reduce unnecessary emergency presentations. There has been a 3.6 per annum increase in Australian ED presentations over the past 10 years (Lowthian et al., 2012). ED avoidance programs focusing on robust relapse prevention and crisis planning could reduce these presentations, which in turn could assist in meeting National Emergency Access Targets.
Third, the largest driver of acute mental health costs was a diagnosis of psychotic disorder, but illness acuity, and prior acute psychiatric inpatient admissions also drove costs. The predictors of total acute cost were similar to the predictors of inpatient service usage, as inpatient services were the largest contributor to total acute costs. Community-based programs that avert or substitute for inpatient care for people with psychotic disorders, high illness acuity and histories of high service use may assist in reducing acute service costs.
Fourth, one unexpected finding was that patients who had self-harmed in the year prior to the index admission had lower service costs. In contrast, a study by Carr et al. (2004) of people with psychosis found that self-harm predicted higher mental health care cost (including acute and community costs). In contrast to Carr et al. (2004), our study was not solely limited to patients with psychotic disorders. Self-harm was significantly correlated with non-psychotic diagnoses, which may explain why service costs for the self-harm group differed from Carr et al. (2004). It is possible that patients with clinically significant self-harm and higher rates of ED presentations have an illness course characterised by brief crises requiring a shorter duration of admission, allowing them a more rapid return to community living. Having a better understanding of the diagnostic and demographic variables associated with this subgroup could lead to interventions that could lower service costs.
It is also worth considering how the findings of this study relate to the broader literature on predictors of mental health care costs. Comparison with previous studies is hampered by variations in the methods and diagnostic or service inclusions used by different studies that may affect the findings observed. As shown in one previous review (Harris et al., 2013), mental health cost studies have used a wide range of cost outcomes which may affect the findings observed. Nonetheless, the predictors identified in the current study were broadly similar to the most commonly identified factors in previous studies, such as patient illness factors including diagnosis, level of function, symptom severity, risk of harm to self or others and treatment history, and other patient characteristics including age, ethnicity, employment and socio-economic factors (Harris et al., 2013).
Our model was able to explain 21.8% of the variation in acute costs based on the R2, a measure of model goodness of fit. The R2 values from relevant international studies in the review by Jones et al. (2007) ranged from 0.6% to 71%, with nearly all models explaining less than 40% of the variance in cost, leaving much of the variation in mental health service utilisation and cost unaccounted for by current models. Of the two studies identified by Jones et al. (2007) with an R2 greater than 40%, duration and quantity of past psychiatric service use explained a large amount of the variance in the models (Ginsberg et al., 1997; Mirandola et al., 2004). The Ginsberg et al. (1997) study focused on acute costs (inpatient and day hospital). Eagar et al. (2013) were able to explain 52% of variation in inpatient costs, with a model including ECT usage, cognitive problems, depressed mood, problems with ADLs, mental health legal status, clinical complexity, separation mode, referral to other care, procedure flag, and stay category. Our study was based on a secondary analysis of existing data and, as such, did not have access to these additional variables.
Strengths and weaknesses of the study
This study is one of the few that uses Australian administrative mental health data extracts to identify predictors of acute mental health service costs. Much of the literature in this area has examined mental health service data from the United States, where mental health services and health financing arrangements differ markedly from those in Australia. Most other studies have not specifically examined acute treatment costs.
One of the strengths of our approach was the use of a split sample cross-validation approach. Cross-validation was identified as best practice in the Jones et al. (2007) study. Jones et al. noted that few other studies had used cross-validation and, of those that had, the size of the split samples was small. Our study had a comparatively large sample size, increasing the statistical power and the probability of generating meaningful results.
However, a number of limitations should be taken into account when interpreting the findings of the current study. The data used in this study were sourced from de-identified administrative data-extracts of all public mental health patients in Queensland and included patients who had been used as controls for previous studies (Siskind et al., 2013, 2014). They were selected to be controls and had been matched to the sample of intervention patients based on the presence of an acute psychiatric inpatient admission as well as diagnosis, sex and time periods. It is possible that patients with psychotic diagnoses (55.3%) and men (56.4%) may be over-represented in this sample. Sex and diagnosis were included in the regression analysis and may have, in part, mitigated these biases. There may be other undetected differences between the patients included in our costs analysis and the broader acute public hospital inpatient group. The data were drawn from metropolitan facilities, and may not be generalisable to regional or remote settings.
There are inherent limitations with administrative data, including missing data and risk of recording bias. The datasets used primarily for billing, including inpatient data and ED presentations, provided close to a complete capture of data. Some of the predictor variables may not have been optimal proxy measures for what they attempt to capture, notably the HoNOS individual questions relating to substance abuse, self-harm and problems with living conditions. This could weaken the predictive power of the model and lower the R2.
Some patients had missing total HoNOS or individual HoNOS ratings. Patients with missing HoNOS data were less likely to have had a previous acute psychiatric inpatient admission and less likely to have a psychotic diagnosis. This has face validity, as an acute psychiatric admission is a HoNOS collection occasion, and non-psychotic patients may be less likely to be in case management, and hence less likely to have HoNOS collected. Prior acute psychiatric inpatient admission and diagnosis of a psychotic disorder were found to be predictors of future acute psychiatric inpatient admissions, longer index admissions and higher total costs. If some patients with prior psychiatric hospitalisations and non-psychotic diagnoses were excluded from the regression analysis, it may have led to an underestimate of the strength of association between those variables, resulting in more conservative findings.
The costs data only included hospital-based acute service costs (per diem acute psychiatric inpatient bed-day and ED visits) and were calculated as a cost-weighted sum of these. We were not able to include acute community services such as crisis assessment teams, as the quality of the collected data on contact with community mental health services was so inconsistent as to be unusable (Siskind et al., 2013, 2014). Crisis teams have been shown to reduce acute psychiatric inpatient bed-days (Burns et al., 2001). The use or non-use of these services may have been predictive of inpatient bed-days. Enhancing the quality of community data collection could allow the derivation of costs for crisis team services.
Our research has looked specifically at acute service costs, but the costs of severe and persistent mental illness extend to societal costs, particularly costs associated with lost productivity (Neil et al., 2014). Including these costs would have been preferable, but was beyond the scope of the data available.
Predictor variables identified in previous studies such as involuntary treatment, clinical interventions such as ECT, socio-economic factors, ethnicity, education and employment were not available for this study. As noted above, improved quality of community contact data would allow the extent of engagement with community mental health services to be included as a potential predictor.
Functional impairment has previously been identified as a predictor of service costs. A measure of functional impairment such as the Life Skills Profile (LSP) (Rosen et al., 1989) is mandated for collection in public sector mental health services and could potentially be used to highlight specific areas of focus for interventions to improve individual functional ability. This is presently untenable as the current quality and coverage of collection is too poor to allow use of the LSP.
Implications for National Mental Health Reform
In 2011, the Council of Australian Governments (COAG) endorsed a new National Health Reform Agreement that included requirement for a nationally consistent system of activity-based funding (ABF) for all public hospital care, including mental health services (Council of Australian Governments, 2011). An ABF system assigns a set ‘efficient price’ for a given health procedure or diagnostic category, also referred to as a Diagnostic Related Group (DRG). The IHPA has been tasked with assigning a ‘national efficient price’ to each hospital-based service episode (Rosen et al., 2012). The IHPA is also responsible for the classification systems used in ABF for all public hospital care and has determined that a new mental health classification system is required. The current proposal is to use modified DRGs for pricing acute mental health services, until this new classification is developed (Rosenberg and Hickie, 2013). However, unlike the majority of acute health services, diagnosis is not a good predictor of mental health service resource use. DRGs are only able to explain approximately 16% of the variation in length of stay for acute mental health overnight episodes (National Casemix and Classification Centre, 2012). This is the lowest statistical performance of DRGs across all major illness types (National Casemix and Classification Centre, 2012).
With the introduction of the new ABF casemix classification for mental health expected in July 2014, the need to identify drivers of the costs of acute mental health service utilisation is pressing (Solomon, 2014).
This evaluation of cost drivers can inform debate on mental health funding models within the national ABF framework. The database used in this evaluation reflects the real world data that will be used for mental health funding, and as such is highly relevant to policy development. The current system of administrative data collection needs improvement if this data is to be used for ABF. Notably, the quality of data associated with community episodes of care is particularly poor, and will need significant improvements before predictive models of community care costs could be developed (National Casemix and Classification Centre, 2012). ABF should drive improved service transparency with growth driven by evidence-based services targeted at improving patient outcomes. Without data on cost drivers to guide ABF models, there is an increased risk that imperfect funding models will drive inefficient service growth.
Conclusions
We identified that diagnosis of psychosis, illness acuity and prior acute psychiatric inpatient admission predicted higher acute mental health service cost, while self-harm predicted lower costs, but the predictor variables included in this study could only explain 21.8% of the variation in costs. For ED presentations, the only predictive variable was prior ED presentations.
Enhancing treatment programs and implementing models of service, including hospital avoidance programs, may assist in reducing acute service costs. Improving quality of routine data collection could assist in identifying additional predictors of acute service use, and increase the percentage of explainable variation in acute service cost.
Future studies would benefit from the inclusion of a wider range of variables such as contact with community services, ethnicity, ECT, cognition, problems with ADLs, mental health legal status and a marker for clinical complexity. The development of models for predicting acute mental health treatment costs using existing administrative data is an essential step towards a workable ABF model for mental health.
Footnotes
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.