
Abstract
Objective:
Schizophrenia is associated with impairment in prospective memory, the ability to remember to carry out an intended action in the future. It has been established that cue identification (detection of the cue event signaling that an intended action should be performed) and intention retrieval (retrieval of an intention from long-term memory following the recognition of a prospective cue) are two important processes underlying prospective memory. The purpose of this study was to examine prospective memory deficit and underlying cognitive processes in patients with first-episode schizophrenia.
Methods:
This study examined cue identification and intention retrieval components of event-based prospective memory using a dual-task paradigm in 30 patients with first-episode schizophrenia and 30 healthy controls. All participants were also administered a set of tests assessing working memory and retrospective memory.
Results:
Both cue identification and intention retrieval were impaired in patients with first-episode schizophrenia compared with healthy controls (ps < 0.05), with a large effect size for cue identification (Cohen’s d = 0.98) and a medium effect size for intention retrieval (Cohen’s d = 0.62). After controlling for working memory and retrospective memory, the difference in cue identification between patients and healthy controls remained significant. However, the difference in intention retrieval between the two groups was no longer significant. In addition, there was a significant inverse relationship between cue identification and negative symptoms (r = −0.446, p = 0.013) in the patient group.
Conclusion:
These findings suggest that both cue identification and intention retrieval in event-based prospective memory are impaired in patients with first-episode schizophrenia. Cue identification and intention retrieval could be potentially used as biomarkers for early detection and treatment prognosis of schizophrenia. In addition, addressing cue identification deficit through cognitive enhancement training may potentially improve negative symptoms as well.
Introduction
Cognitive deficits predict poor functional outcome in schizophrenia (Liu et al., 2013; Sharma and Antonova, 2003). It has been well established that episodic memory and working memory are both impaired in patients with schizophrenia (Liu et al., 2013; Sharma and Antonova, 2003). However, memory involving the ability to remember to carry out intended actions in the future, i.e., prospective memory (PM) (Einstein and McDaniel, 1990; Kliegel et al., 2008), is relatively less studied in patients with schizophrenia. PM includes event-based and time-based subtypes (McDaniel and Einstein, 1992). Event-based PM refers to the ability to remember to execute an intention when an event/cue appears, whereas time-based PM refers to the ability to remember to execute an intention at a specific time or after a period of delay (McDaniel and Einstein, 1992). Moreover, the cognitive process for PM includes four stages, namely intention formation, intention retention, intention initiation and intention execution (Kliegel et al., 2011; McDaniel and Einstein, 1992). Cue identification and intention retrieval are two important components underlying the intention initiation stage of PM (McDaniel and Einstein, 1992). Cue identification refers to the detection of cue event (e.g. supermarket) signaling that an intended action should be performed, while intention retrieval means the retrieval of an intention (e.g. buying bread) from long-term memory following the recognition of a prospective cue (Kliegel et al., 2008; McDaniel and Einstein, 1992; Simons et al., 2006). Studies suggest that cue identification and intention retrieval belong to prospective and retrospective components respectively in event-based PM, and rely on distinct brain systems (Burgess et al., 2011; Kliegel et al., 2011; McDaniel and Einstein, 2011; West, 2011).
Growing evidence has consistently identified event-based PM deficits in patients with chronic schizophrenia (Altgassen et al., 2008; Au et al., 2014; Henry et al., 2007, 2012; Kumar et al., 2005; Raskin et al., 2014; Shum et al., 2004; Ungvari et al., 2008; Wang et al., 2008a, 2008b; Woods et al., 2007; Zhuo et al., 2011) and first-episode schizophrenia (Lui et al., 2011, 2015; Zhou et al., 2012, 2013). It has been suggested that patients with schizophrenia exhibit PM deficits, especially in event-based PM (Ordemann et al., 2014; Wang et al., 2009). However, the nature of PM deficits in patients with schizophrenia remains to be elusive. While some studies suggest that event-based PM deficit in schizophrenia is a primary deficit rather than secondary consequence of other cognitive impairments (Henry et al., 2007; Lui et al., 2015; Wang et al., 2008a; Woods et al., 2007; Zhuo et al., 2013), other studies have found event-based PM deficit to be associated with other cognitive deficits such as impaired retrospective memory (Xiang et al., 2010; Zhou et al., 2012).
Since PM is a complex cognitive function involving multiple processes, it is important to examine the specific components of PM deficit in patients with schizophrenia. Two previous studies (Wang et al., 2008a; Woods et al., 2007) have examined the components of PM deficit in patients with schizophrenia. However, these two studies only adopted post-hoc analysis to control for recall of PM task requirements after finishing the PM test, and the results indicated that PM deficits in schizophrenia patients might be due to intention initiation deficit (Wang et al., 2008a; Woods et al., 2007). It should be noted that no study had specifically examined the underlying cue identification and intention retrieval processes directly in patients with schizophrenia.
Previous studies suggest that neurocognitive deficits are modestly correlated with negative symptoms (Dibben et al., 2009; Dominguez Mde et al., 2009). A meta-analysis also reported that PM is correlated significantly with negative symptoms, duration of illness and antipsychotic medication dosage, but not with positive symptoms (Wang et al., 2009). However, this meta-analysis only included studies with chronic schizophrenia patients. Zhou et al. (2012) found that event-based PM deficit in patients with first-episode schizophrenia was inversely correlated with negative symptoms, but not with positive symptoms. However, others (Lui et al., 2011, 2015; Zhuo et al., 2013) did not find any significant correlation between event-based PM, negative symptoms and positive symptoms in patients with first-episode schizophrenia.
The purpose of this study was to examine cue identification and intention retrieval components in the intention initiation stage of event-based PM in patients with first-episode schizophrenia. We hypothesized that both components would be impaired in this patient population.
Method
Participants
This study was conducted at the Shanghai Mental Health Center, Shanghai Jiao Tong University School of Medicine. A total of 30 patients (22 with first-episode schizophrenia, 8 with schizophreniform disorder) were recruited. Those diagnosed with schizophreniform disorder at the time of study enrollment were subsequently diagnosed with schizophrenia 6 months later. All patients were in stable clinical condition and were taking antipsychotic medications. None of them received long-acting antipsychotic medications or electroconvulsive therapy.
All patients met the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) (American Psychiatric Association [APA], 1994) diagnostic criteria for schizophrenia or schizophreniform disorder. The diagnosis was confirmed by a research psychiatrist (C.J.) using the MINI plus v 5.0 (Sheehan et al., 1998). Exclusion criteria included (1) inability to provide informed consent; (2) current substance abuse; (3) personality disorders; (4) mental retardation; (5) significant medical conditions including severe cardiovascular, hepatic and renal diseases and (6) pregnancy or breastfeeding.
A total of 30 healthy controls were recruited from the local community. All of them completed a structured clinical interview with a research psychiatrist (C.J.) using the MINI plus v 5.0. Those with other Axis I mental disorders, neurological diseases, or a positive family history of mental illness were excluded.
Clinical symptoms were assessed using the Positive and Negative Syndrome Scale (PANSS) (Kay et al., 1987, 1989) and the Clinical Global Impression (CGI)-severity scale (Guy and Bonato, 1976). This study was approved by the Institutional Review Board of the Shanghai Mental Health Center. Written informed consent was obtained from all participants.
Measures
Prospective memory
Event-based PM computerized tasks were designed based on the dual-task paradigm of Einstein and McDaniel (1990). Participants were required to undertake a task in which PM trials were embedded in an ongoing task. Two types of PM conditions were used, one with high cue identification and low intention retrieval demand (the cue identification condition), and one with low cue identification and high intention retrieval demand (the intention retrieval condition) (Simons et al., 2006). The PM tasks were designed and modified based on previous PM studies (Burgess et al., 2011; Chen et al., 2007; den Ouden et al., 2005; McDaniel et al., 2011; Simons et al., 2006; Wang et al., 2008a; Zhuo et al., 2011, 2013).
The ongoing task was a simple figure judgment task, which was identical for both cue identification and intention retrieval PM conditions. A triangle in yellow and an irregular polygon in yellow were presented on the screen side by side (Figure 1). Irregular shapes were used to avoid recognition at first glance, and the triangle was presented randomly to the left or right of the irregular polygon with equal probability. Participants were instructed to indicate whether the irregular polygon was presented to the left or right of the triangle, and then to press the ‘G’ or ‘H’ key, respectively. The presentation of the stimulus was subject-paced with a maximum of 3000 ms, and the inter-trial interval was varied randomly between 1000 and 1500 ms, which ensured variable onset times of the trials (Simons et al., 2006).
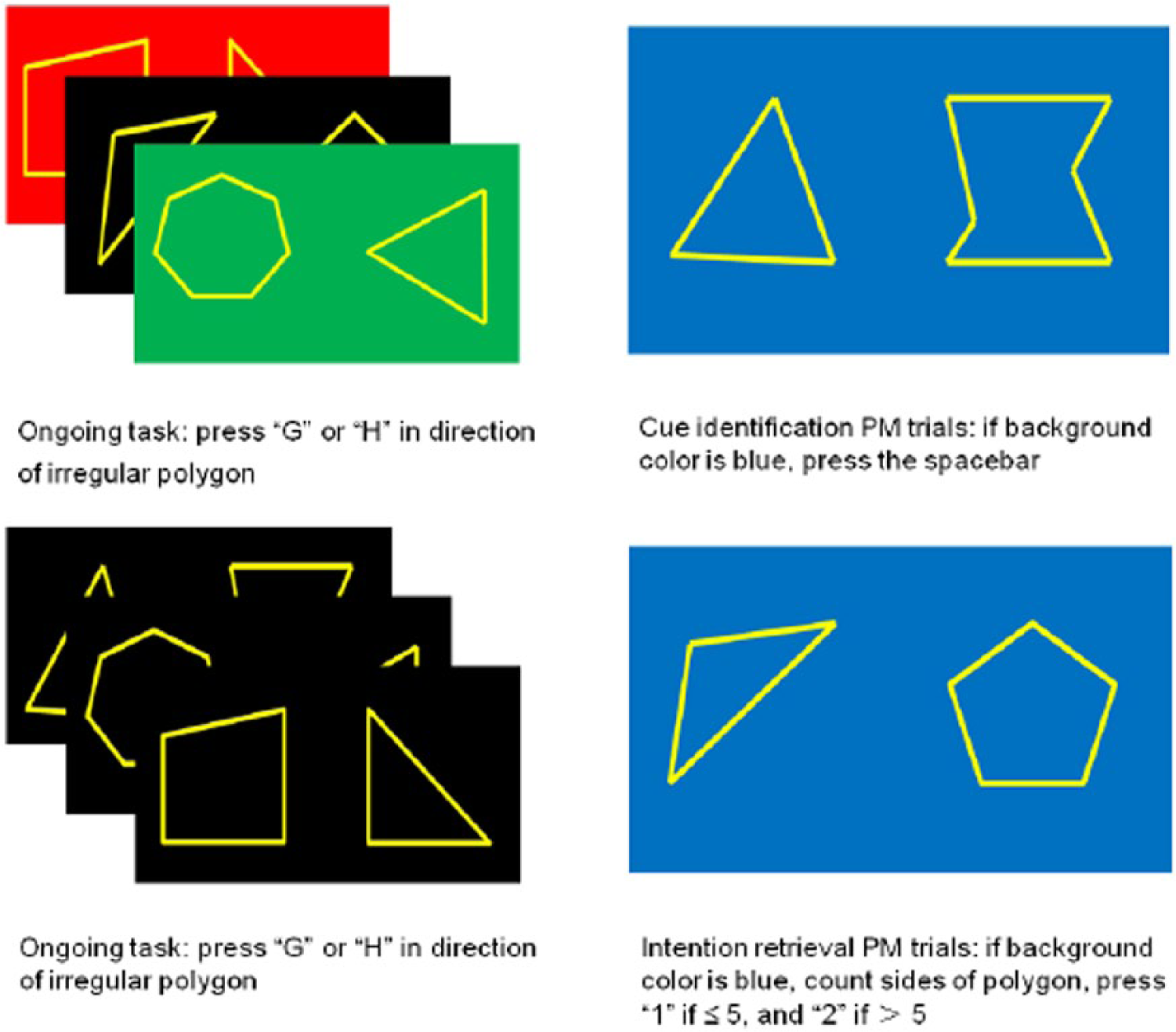
Schema for the cue identification and intention retrieval conditions: (1) above row indicates the ongoing trials and PM trials in the cue identification condition and (2) bottom row indicates the ongoing trials and PM trials in the intention retrieval condition.
In the cue identification condition, PM trials were embedded in an ongoing task. The background color of the screen varied between black, red, blue and green. PM trials had a blue background color. For the ongoing task, participants were instructed to make the judgment while ignoring the background color. However, once the background color became blue, they were required to suspend the judgment and instead press a third key to indicate the presence of a PM cue. As a result, the cue identification demand was relatively high and the intention retrieval demand was low. There were 120 ongoing trials and 5 PM trials in this condition. The accuracy (proportion of hits) and reaction time (RT) were recorded for the cue identification condition and the ongoing task.
In the intention retrieval condition, the background color of the screen was either black (96%) or blue (4%), and the trials in which the background color was blue were PM trials. As a result, it was easier for participants to detect the PM cue from the ongoing task. However, the intention retrieval demand increased significantly as the participants were required to determine the number of sides of the shape other than a triangle, and press one key if this number was five or less, and another key if this number was larger than five. There were 120 ongoing trials and 5 PM trials in this condition. Similarly, the accuracy and RT were recorded for the intention retrieval condition and the ongoing task.
Working memory
The Spatial Span Task and the Letter Number Span Task from the MATRICS Consensus Cognitive Battery (Kern et al., 2008; Nuechterlein et al., 2008) were used to measure non-verbal and verbal working memory respectively. The Spatial Span Task included forward and backward sections, and participants were required to remember the spatial position of blocks as far as possible. The total score was the sum of the forward and backward total scores. The Letter Number Span Task involved a mixed series of alternating numbers and letters, for which participants were instructed to respond to by first saying the numbers in order (from the smallest to the largest), then stating the letters in alphabetical order. The longest correct sequence was recorded.
Retrospective memory
Free Image Recall from the China Clinical Memory Scale Group (1996) was used to assess retrospective memory. This task included two sets of pictures, with 15 pictures in each set. During each set, 15 pictures were first consecutively presented (4 s per picture, interval 2 s) to the participants, who were then required to recall the name of the pictures as far as possible. The score was the total items correctly recalled from the two sets of pictures.
Procedure
The working memory tests were used as delay tasks and were administered to all participants after the introduction of the PM task and before the formal PM task. The orders of the Spatial Span Task and the Letter Number Span Task were counterbalanced. The cue identification PM condition and the intention retrieval PM condition were also counterbalanced. Clinical assessments were completed on the same day of the neurocognitive assessments.
Data analysis
Demographic characteristics were compared between patients and healthy controls using t test for continuous variables and chi-square test for categorical variables. PM, working memory and retrospective memory were compared between the two groups using t test, and effect sizes were calculated using Cohen’s d (Cohen, 1988). The accuracy of the two components was further analyzed using repeated-measure analysis of variance (ANOVA) with PM component (cue identification versus intention retrieval) as within-subject factor and Group (patients versus healthy controls) as between-subject factor. Since working memory and retrospective memory have been shown to have significant correlation with PM (Kliegel et al., 2008, 2011; McDaniel and Einstein, 2011; Wang et al., 2008b; West, 2011; West et al., 2006), these two cognitive functions were controlled for as covariates using univariate analysis of covariance (ANCOVA) to examine the nature of the cue identification deficit and the intention retrieval deficit in patients with first-episode schizophrenia. Pearson correlations were used to examine the relationships between PM, demographic variables and clinical characteristics in patients.
Results
Demographic and clinical characteristics
Table 1 shows the demographic and clinical characteristics of the patients with first-episode schizophrenia and healthy controls. There were no significant differences between patients and healthy controls in age, gender and education. A total of 25 patients were treated with second generation antipsychotic medications (11 with risperidone, 6 with olanzapine, 5 with quetiapine, 2 with aripiprazole and 1 with paliperidone), 1 patient with conventional antipsychotic medication (perphenazine), and 4 with a combination of both. Drug choices and dosages were determined based on the treating psychiatrists’ clinical judgment. The average dose in chlorpromazine equivalence (CPZ eq) was 321 ± 173 mg/day.
Demographic and clinical characteristics of the study sample.
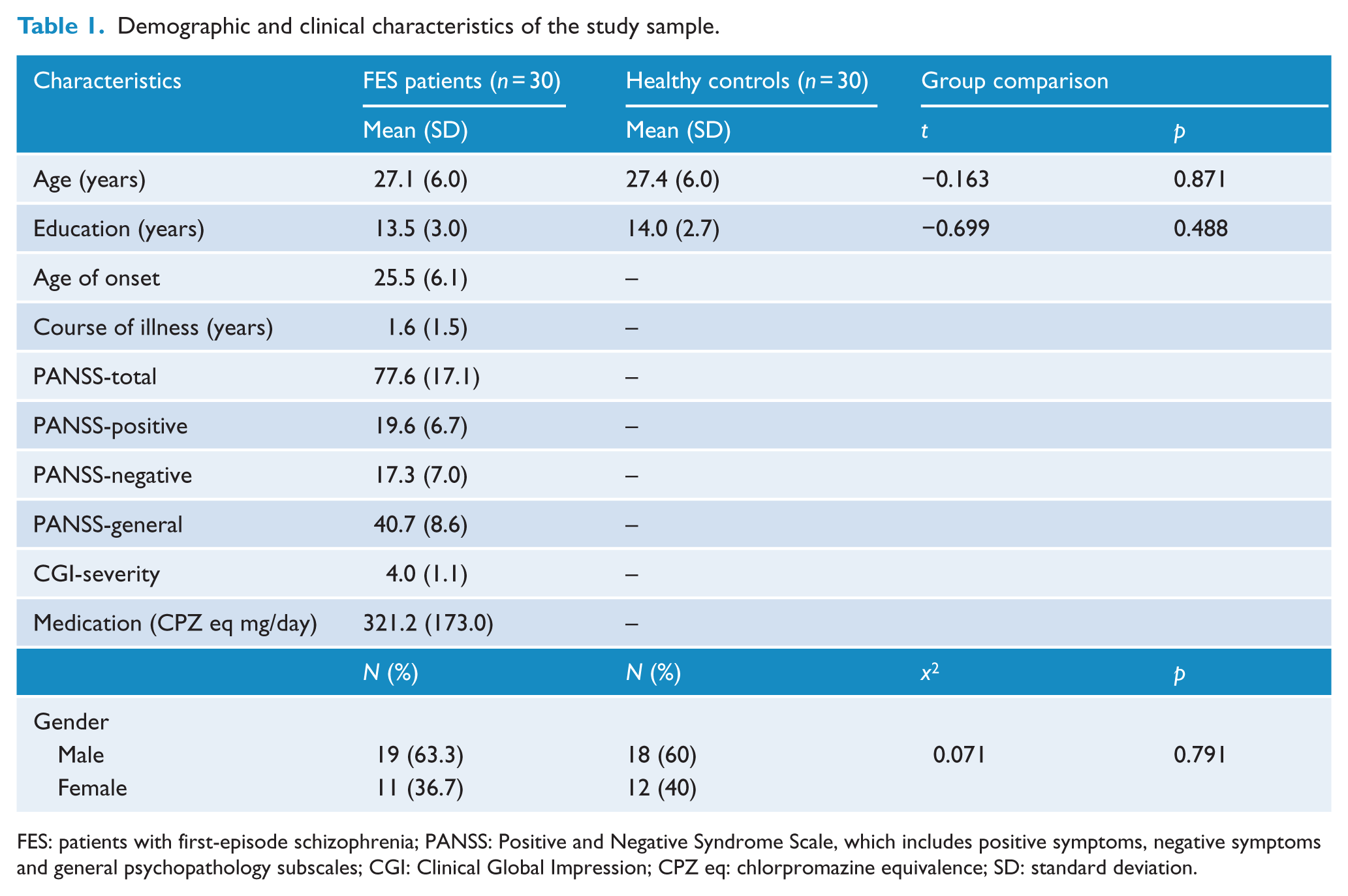
FES: patients with first-episode schizophrenia; PANSS: Positive and Negative Syndrome Scale, which includes positive symptoms, negative symptoms and general psychopathology subscales; CGI: Clinical Global Impression; CPZ eq: chlorpromazine equivalence; SD: standard deviation.
PM and other memory performances
The accuracy and RT of patients with first-episode schizophrenia and healthy controls during the cue identification and intention retrieval conditions are summarized in Table 2. Significant differences were found between patients with first-episode schizophrenia and controls in accuracy and RT of cue identification and the ongoing task (ps < 0.05), with patients performing poorer in cue identification and the ongoing task than healthy controls. For intention retrieval, patients with first-episode schizophrenia were less accurate but had similar RT compared to healthy controls. Patients with first-episode schizophrenia also showed poorer performance in the ongoing task than healthy controls (both accuracy and RT).
Accuracy and RT (ms) of the two study groups during the cue identification and intention retrieval conditions.
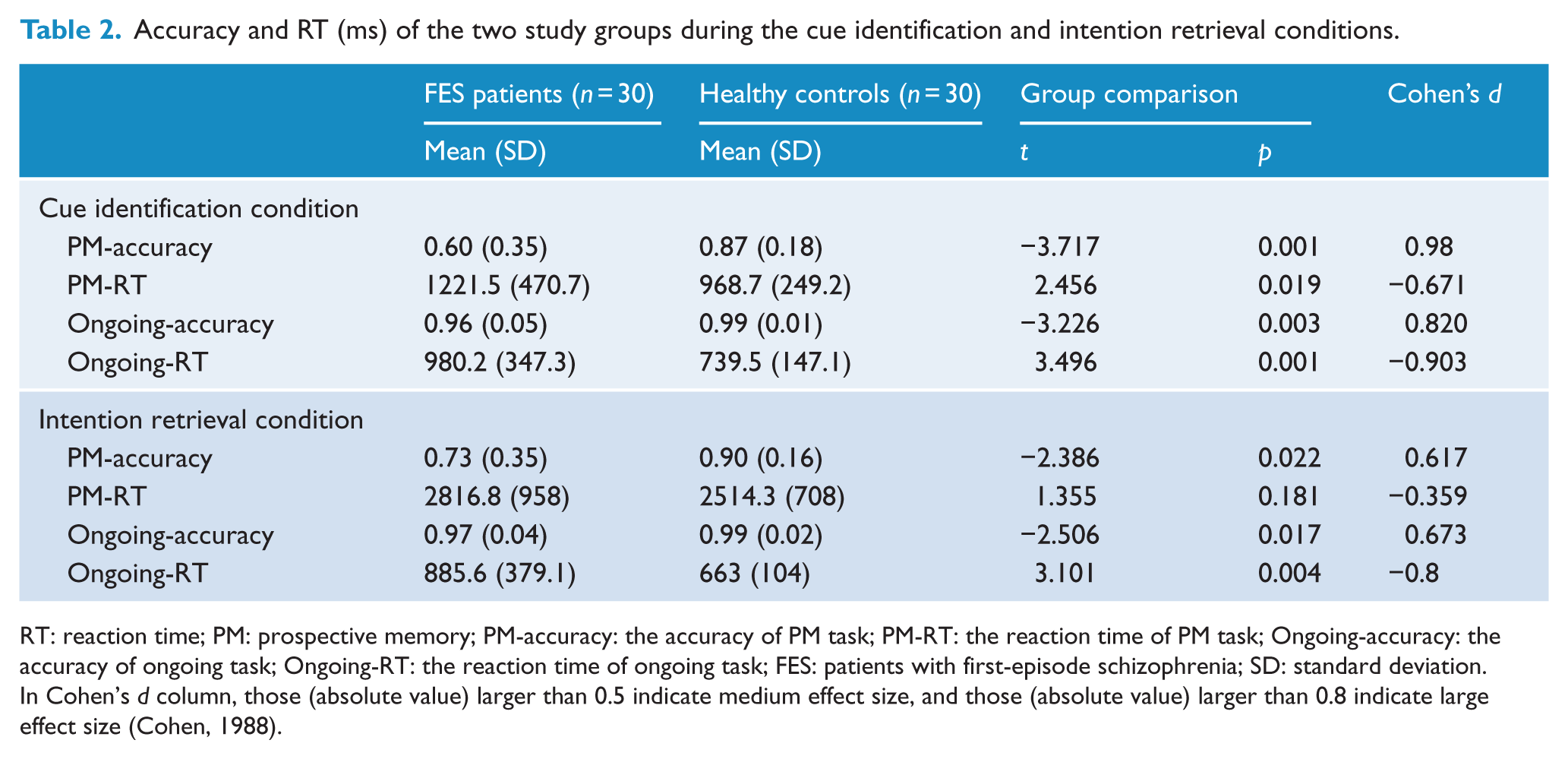
RT: reaction time; PM: prospective memory; PM-accuracy: the accuracy of PM task; PM-RT: the reaction time of PM task; Ongoing-accuracy: the accuracy of ongoing task; Ongoing-RT: the reaction time of ongoing task; FES: patients with first-episode schizophrenia; SD: standard deviation.
In Cohen’s d column, those (absolute value) larger than 0.5 indicate medium effect size, and those (absolute value) larger than 0.8 indicate large effect size (Cohen, 1988).
The results from repeated-measure ANOVA indicated that there was a significant main effect of group, F(1, 58) = 13.357, p = 0.001), and a marginal main effect of PM component, F(1, 58) = 3.921, p = 0.052. However, there was no interaction between the two factors, F(1, 58) = 1.668, p = 0.202.
For working memory performances, patients with first-episode schizophrenia performed significantly poorer than healthy controls in the Spatial Span (t = −2.428, p = 0.019) and the Letter Number Span Task (t = −2.580, p = 0.012) (Table 3). For retrospective memory performance, patients with first-episode schizophrenia also performed significantly poorer than healthy controls in Free Image Recall (t = −2.927, p = 0.005).
Working memory and retrospective memory performances in FES patients and healthy controls.
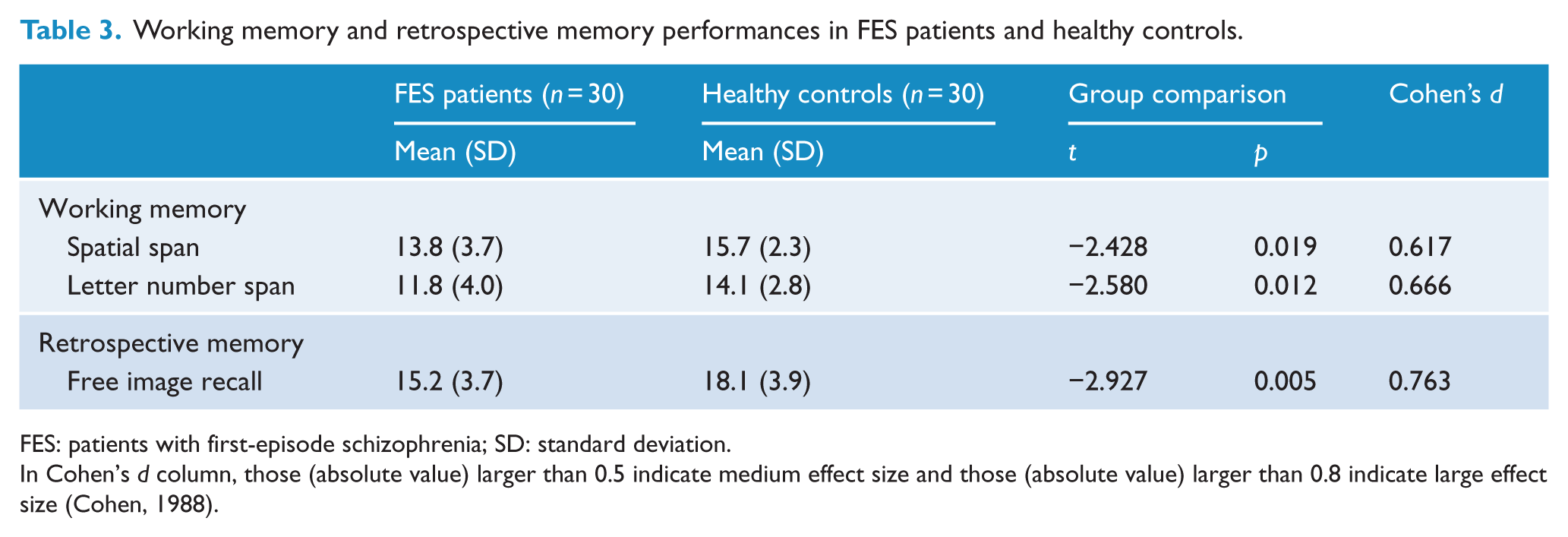
FES: patients with first-episode schizophrenia; SD: standard deviation.
In Cohen’s d column, those (absolute value) larger than 0.5 indicate medium effect size and those (absolute value) larger than 0.8 indicate large effect size (Cohen, 1988).
After controlling for working memory (non-verbal and verbal) and retrospective memory, the difference in cue identification PM performance (accuracy) between patients with first-episode schizophrenia and healthy controls was significant (p = 0.033). The results remained significant even after adding years of education as a covariate (p = 0.032).
However, after controlling for working memory and retrospective memory, no significant difference was found for intention retrieval PM performance (accuracy) between patients and healthy controls (p = 0.498). This was also the case after controlling for working memory, retrospective memory and years of education (p = 0.479).
Relationships between PM, demographic and clinical variables
Cue identification was significantly and inversely correlated with negative symptoms (r = −0.446, p = 0.013), but not with positive symptoms (r = 0.158, p = 0.405). No demographic variable showed significant correlation with cue identification (ps > 0.05) in patients with first-episode schizophrenia.
No significant correlations were found between intention retrieval, positive symptoms and negative symptoms (ps > 0.05). No demographic variable showed significant correlation with intention retrieval (ps > 0.05).
Discussion
Our findings show that the cue identification component and the intention retrieval component in event-based PM are impaired in patients with first-episode schizophrenia, with a large effect size for cue identification (Cohen’s d = 0.98) and a medium effect size for intention retrieval (Cohen’s d = 0.62). These findings are consistent with previous studies in patients with first-episode schizophrenia (Lui et al., 2011, 2015; Zhuo et al., 2013) and a meta-analysis (Wang et al., 2009). After controlling for working memory and retrospective memory, the performance difference in the cue identification component of event-based PM between patients and healthy controls remained significant, while no significant difference was found between the two groups for the intention retrieval component of event-based PM. These findings suggest that cue identification deficit of event-based PM is already present in the early stage of schizophrenia and may be a primary deficit, while intention retrieval deficit may be a secondary deficit confounded by impairment in working memory and retrospective memory.
To our knowledge, this study is the first to explore cue identification and intention retrieval processes in event-based PM deficit in first-episode schizophrenia patients. Preliminary studies from Woods et al. (2007) and Wang et al. (2008a) indicate that event-based PM deficit in patients with schizophrenia is primarily contributed by deficit in the intention initiation stage of PM, which further involves two processes, i.e., cue identification and intention retrieval, and may rely on different brain systems (Burgess et al., 2011; Kliegel et al., 2011; McDaniel and Einstein, 2011; West, 2011). Cue identification deficit is related to ‘When’, i.e., schizophrenia patients cannot detect the cue promptly on presentation. However, intention retrieval deficit is related to ‘What’, i.e., schizophrenia patients forget the action entirely (Kliegel et al., 2008, 2011; McDaniel and Einstein, 1992, 2011; Simons et al., 2006; Wang et al., 2008a; West, 2011; Woods et al., 2007). Our results suggest that the ‘When’ problem in patients with first-episode schizophrenia appears to be independent of working memory and retrospective memory impairments.
Another finding is that cue identification deficit in patients with first-episode schizophrenia was inversely correlated with negative symptoms. This finding is consistent with those reported in patients with chronic schizophrenia (Wang et al., 2009) as well as first-episode schizophrenia (Zhou et al., 2012). Our study specifically examined cue identification and intention retrieval components of PM, which have not been well studied in first-episode schizophrenia. The finding of a relationship between cue identification and negative symptoms may have great clinical implications. For example, cue identification may be incorporated in the cognitive enhancement training programs with potential benefit of improving negative symptoms (Eack et al., 2009, 2013; Hogarty et al., 2004).
This study has several limitations. First, PM is a complex cognitive function involving multiple processes and may be correlated with many other cognitive functions, such as working memory, retrospective memory, cognitive flexibility and attention (Kliegel et al., 2008, 2011; Lui et al., 2011, 2015). In the present study, cognitive flexibility and attention were not measured and controlled for. Second, although patients with first-episode schizophrenia were recruited in this study, all of them were taking antipsychotic medications, and this might have confounded the results. Third, the sample size was relatively small for correlational analyses, which means that we might have missed some relationships. Finally, this study used laboratory PM tasks with relatively low ecological validity.
In conclusion, our results suggest that both cue identification and intention retrieval of event-based PM in patients with first-episode schizophrenia are impaired. Cue identification deficit appears to be present even in the early stage of the illness, while intention retrieval deficit may be a consequence of deficits in working memory and retrospective memory. Cue identification and intention retrieval could be potentially used as biomarkers for early detection and treatment prognosis of schizophrenia. In addition, addressing cue identification deficit through cognitive enhancement training may potentially improve negative symptoms as well.
Footnotes
Acknowledgements
The authors would like to acknowledge those patients taking part in this study and the support of the funding sources.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This work was supported by National Natural Science Foundation of China (81371479), Shanghai Municipal Natural Science Foundation (11ZR1431600), Shanghai Municipal Health and Family Planning Commission (20134006, 2014ZYJB0002), Shanghai Municipal Hospital Appropriate Technology Programme (SHDC12014214), Shanghai Clinical Center for Mental Disorders (2014), Shanghai Key Laboratory of Psychotic Disorders (14K03), Early Psychosis Program of Shanghai Mental Health Center (2013-YJTSZK-05). Raymond Chan was supported by the Science Foundation of Shanghai Mental Health Center (SMHCRSD01) and the Beijing Training Project for the Leading Talents in S & T (Z151100000315020). These funding agents had no role in the study design, collection, analysis and interpretation of the data, writing of the manuscript, or decision to submit the paper for publication.