
Abstract
Objective:
To (1) estimate the lifetime and 12-month prevalence of self-harm without suicide intent in young people aged 12–17 years, (2) describe the co-morbidity of these behaviours with mental illness and (3) describe their co-variation with key social and demographic variables.
Method:
A nationally representative random sample of households with children aged 4–17 years recruited in 2013–2014. The survey response rate was 55% with 6310 parents and carers of eligible households participating. In addition, 2967 (89%) of young people aged 11–17 completed a self-report questionnaire with 2653 of the 12- to 17-year-olds completing questions about self-harm behaviour.
Results:
In any 12-month period, about 8% of all 12- to 17-year-olds (an estimated 137,000 12- to 17-year-olds) report engaging in self-harming behaviour without suicide intent. This prevalence increases with age to 11.6% in 16- to 17-year-olds. Eighteen percent (18.8%; 95% confidence interval [CI] = [14.5, 23.0]) of all 12- to 17-year-old young people with any mental health disorder measured by parent or carer report said that they had engaged in self-harm in the past 12 months. Among young people who were measured by self-report and met criteria for the Diagnostic and Statistical Manual of Mental Disorders’ major depressive disorder almost half (46.6%; 95% CI = [40.0, 53.1]) also reported that they had engaged in self-harm in the past 12 months. Suicide risk among those who self-harm is significantly elevated relative to the general population.
Conclusion:
The demonstrated higher risks in these young people for continued harm or possible death support the need for ongoing initiatives to reduce self-harm through mental health promotion, improved mental health literacy and continuing mental health reform to ensure services are accessible to, and meet the needs of families and young persons.
Introduction
In their systematic review of fatal and non-fatal repetition of self-harm, Owens et al. (2002) observed that ‘national suicide prevention strategies ought to be based on up-to-date research into non-fatal self-harm’. While their attempt to provide a precision estimate of the relationship between self-harm and subsequent suicide was frustrated by the quality of the data available to their meta-analysis, the authors were able to note that suicide risk among self-harm patients was higher by a magnitude of ‘hundreds’.
In Australia, population estimates of suicidal behaviour in children and adolescents were first published in 2000 based on 1998 data (Sawyer et al., 2000). The most recent data published in this issue (Zubrick et al., submitted) show that, in any 12-month period, about 2.4%, or 41,400 young people aged 12–17 years will have made a suicide attempt. About 7.5% will report having suicidal ideation, 5.2% making a plan and less than 1% (0.6%) receiving medical treatment for an attempt (Zubrick et al., submitted). These rates of suicidal behaviour and suicide mortality conceal the more prevalent morbidity associated with self-inflicted injury, or ‘self-harm’.
Population data on Australian non-suicidal self-harm in Australian youth are scant. Martin et al. (2010) published the first population data describing non-suicidal self-harm among a random sample of 12,006 Australian adults aged 18–100 (N = 10,531) and children aged 10–17 (N = 1475). For females, self-injury peaked at 15–19 years (4.0%) and 20–24 years (3.6%). For males, self-injury peaked at 10–14 years (2.3%) and 15–19 years (2.2%); it then declined with age for both sexes (Martin et al., 2010). Broadly then, while the above estimates provide Australian population benchmarks for self-reported suicidal behaviours, the prevalence of self-harming behaviours in young people has been limited and otherwise has remained out of the scope of previous Australian child and adolescent mental health surveys (Sawyer et al., 2000).
The phenomenology of, and agreement about, the definition of self-harming behaviours has had a vexing career. Currently, self-harm is a term that encompasses several phenomena with proposed criteria for self-harm defining ‘non-suicidal self-injury’ (NSSI) (American Psychiatric Association, 2013). Clarity and agreement in defining self-harming behaviours is lacking with the meaning and threshold of ‘intention’ a matter of particular ambiguity and dispute (Australian Human Rights Commission, 2014). Nock et al. (2006) have noted the diagnostic heterogeneity of adolescents engaging in NSSI with the significant overlap between non-suicidal self-harm and suicide attempts (Nock et al., 2006) while others have suggested that adolescents engaging in non-suicidal self-harm who also attempt suicide can be differentiated from adolescents who only engage in non-suicidal self-harm on measures of suicidal ideation, reasons for living and depression (Muehlenkamp and Gutierrez, 2007). Because of the greater prevalence of self-harm and its links with many common determinants of psychological distress (e.g. drug and alcohol use, depression and violence) (Brausch and Gutierrez, 2010) and its known association in elevating the risks for eventual suicide, the monitoring of population rates of self-harm is seen to be critical for causal analysis, the estimation of burden and the support of prevention initiatives (Nock, 2012).
While definition of self-harm remains in dispute, what is not disputed is the need for better information about its prevalence and associated risks. In the 2014 report of the Australian National Childrens’ Commissioner, self-harm was given particular prominence with the Commissioner noting
… the paucity of data in Australia about the wellbeing of children and young people in a range of critical domains. The dearth of information in the area of intentional self-harm and suicidal behaviour has implications for policy development, the design of interventions and for the evaluation of the effectiveness of these interventions. (Australian Human Rights Commission, 2014: 63)
We report here the national estimates of self-harm behaviour collected on Australian young people aged 12–17 years in the 2013–2014 second Child and Adolescent Survey of Mental Health and Wellbeing (i.e. Young Minds Matter–YMM). Specifically, our aims are to: (1) estimate the lifetime and 12-month prevalence of non-suicidal self-harming behaviours in Australian young people aged 12–17 years, (2) describe the co-morbidity of these behaviours with mental illness and (3) describe the co-variation of these estimates with key social and demographic variables. These descriptions add to the extant literature by providing the first contemporary, community-based Australian population estimates of lifetime and 12-month prevalence for self-reported self-harm in young people.
Methods
The design, sampling and survey interview methods are described extensively elsewhere (Hafekost et al., submitted; Lawrence et al., submitted). Briefly, the survey employed area-based random sampling with voluntary recruitment and consent of households in scope where there was at least one child aged 4–17 years. One child was randomly selected for inclusion where there was more than one eligible child in the household. The overall response rate to the survey was 55% with 6310 parents and carers of eligible households participating in the survey. In addition, 2967 or 89% of young people aged 11–17 in these participating households completed a youth self-report questionnaire with 2653 of the 12- to 17-year-olds specifically completing questions about self-harm behaviour.
We examined the sample for its representativeness. Comparison with 2011 Census data showed that the YMM sample was broadly representative of the Australian population in terms of major demographic characteristics (Hafekost et al., submitted). The sample was found to include a higher proportion of children aged 4–7 years than would be expected based on random sampling with 34.2% of the main sample aged 4–7 years, compared with the 29.4% in the 2011 Census. There was also a lower proportion of families with only one eligible child, with 37.9% of all participating families having one child compared with 45.8% of those in the 2011 Census. However, in all other regards, no differences were noted with respect to area-level socio-economic indicators (i.e. Socio-economic indexes for areas [SEIFA]), population distribution, age, sex and country of birth of the total population of 4- to 17-year-olds in Australia and demographic characteristics, including household income, family type, household tenure, parent/carer education and labour force status of families with children aged 4–17 years. We concluded that the achieved sample was broadly representative of the Australian population.
Survey data have been weighted to represent the full Australian population of 4- to 17-year-olds, and to adjust for patterns in non-response. In particular, families with more than one child aged 4–17 years were found to be more likely to participate in the survey. Additionally, 16- to 17-year-olds were specifically oversampled. The weighting accounts for these factors. Survey estimates and associated confidence intervals have been calculated using the method of Taylor Series Linearisation (Wolter, 2007). The association between self-harm and mental disorders was examined using logistic regression, using the SAS SURVEYLOGISTIC procedure to account for the clustered nature of the sample design and the use of survey weights. All analyses were conducted using Statistical Analysis System (SAS) software (SAS Institute Inc., 2014).
Ethics approval
The survey obtained the approval of the Australian Government Department of Health Departmental Ethics Committee for the conduct of the survey.
Measures
A self-report questionnaire was completed in the home by survey participants aged 11–17 years. Consenting participants completed the questionnaire in private using a tablet computer. All responses were confidential and not shared with the consenting parent. The questions about self-harming behaviours were restricted to those young people aged 12–17 years, and they comprise the sample reported here. The full text of the questions is shown in Table 1.
Items used in the second national mental health survey of child and adolescent mental health and wellbeing to measure self-harm behavior.
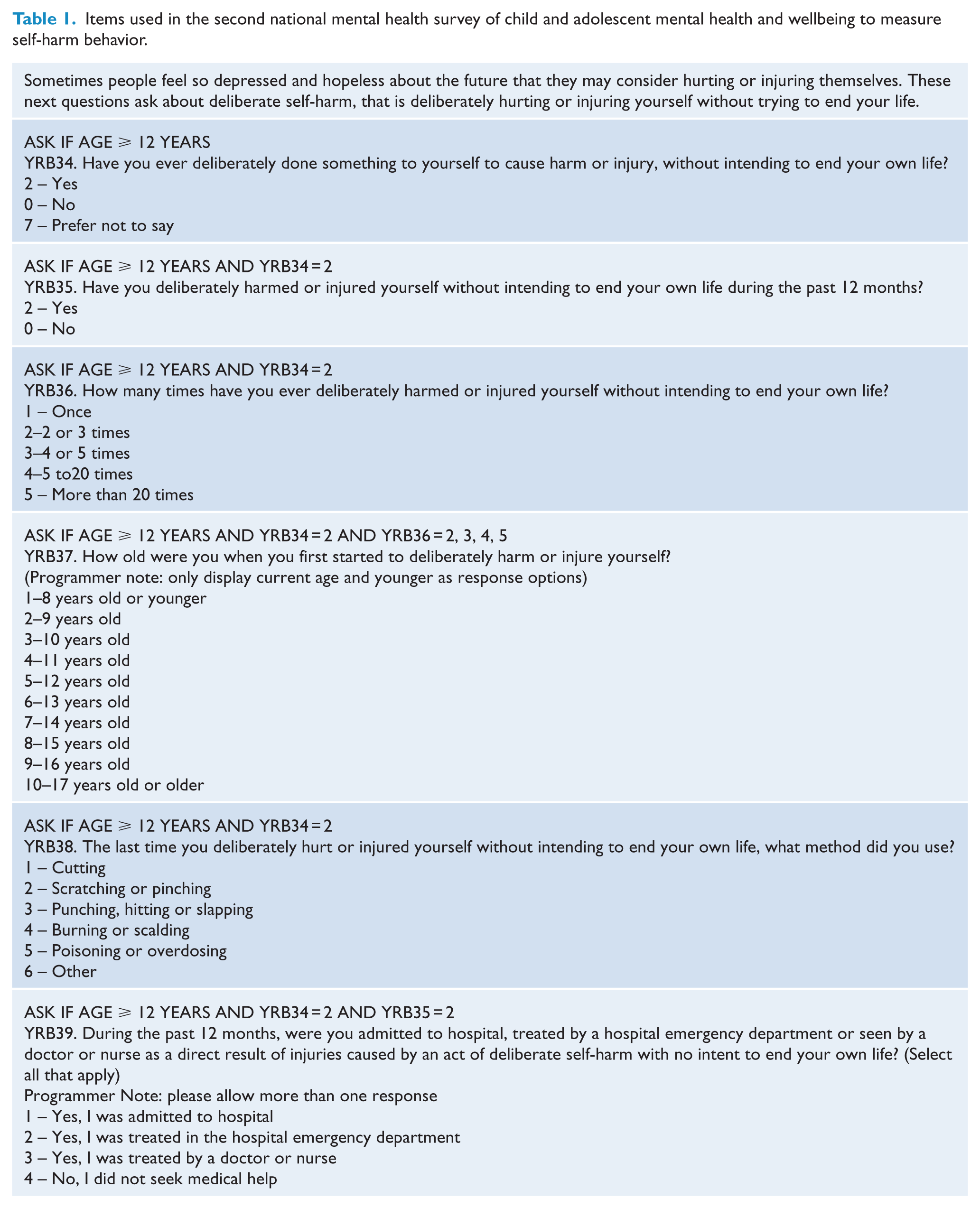
The questions about non-suicidal self-harm probed the 12-month and lifetime occurrence of deliberate self-harm or injury without intending to end life; the number of times such acts had ever occurred; their age of onset; the most recent method of harm; and whether the respondent had been admitted to hospital, an emergency department or treated for self-harm in the past 12 months (Table 1). 1 Several instruments were reviewed for possible sources of items (Harriss et al., 2005; Harriss and Hawton, 2005; Klonsky and Glenn, 2009). Some of these instruments restricted the scope of the harm behaviours to only include individuals requiring medical attention, while other item sets were too long and detailed for a survey format. As a result, the questions finally employed for measuring self-harming behaviours, while drawing upon these sources, had to be specifically worded and tailored for the survey. The initial screening question included a ‘Prefer not to say’ option in addition to the ‘No’ and ‘Yes’ response categories. Young people who selected this option were sequenced out of the item set.
Mental disorders were measured using the Diagnostic Interview Schedule for Children Version IV (DISC) (Fisher, Shaffer and Piacentini, 1993). The DISC implements the criteria for mental disorders set out in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) (American Psychiatric Association, 2013). These criteria are based on clinically significant sets of symptoms that are associated with impaired functioning by young people with the disorders. The DISC contains several modules, not all of which were used in YMM. Seven modules were used in the survey – social phobia, separation anxiety disorder, generalised anxiety disorder, obsessive-compulsive disorder, major depressive disorder, attention-deficit/hyperactivity disorder (ADHD) and conduct disorder. Parents and primary carers were administered all of these modules in order to ascertain the parent-/carer-reported prevalence for each of these disorders. Young people were also administered the major depressive disorder module.
Results
All questions about self-harm were gathered directly from young people aged 12 years and over. A total of 201 (7.5%) young people reported ‘prefer not to say’ and are not included in the results below. Table 2 contains the unweighted sample sizes differentiated by age and sex for all respondents completing the self-harm questions. In subsequent tables, data have been weighted to produce population estimates.
Unweighted sample sizes for self-harm among 12- to 17-year-olds by sex and age group.
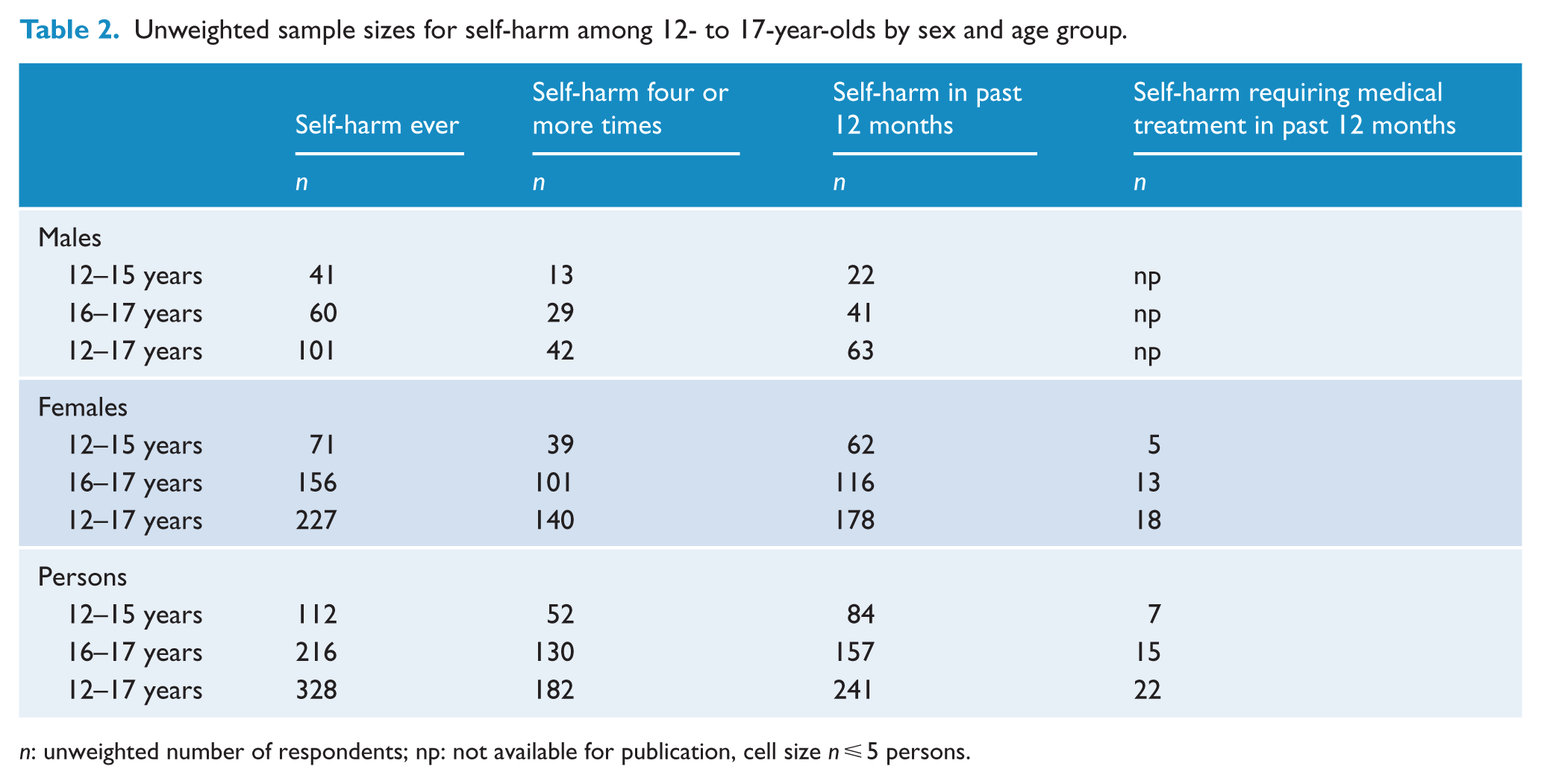
n: unweighted number of respondents; np: not available for publication, cell size n ⩽ 5 persons.
Self-harm, age and sex
Lifetime self-harm was reported by 10.9% (95% confidence interval [CI] = [9.7, 12.2]) of all respondents aged 12–17 years with a 12-month prevalence among this group of 8.0% (95% CI = [6.9, 9.1]) (Table 3). Relative to 12- to 15-year-olds, significantly higher proportions of 16- to 17-year-olds reported having ever self-harmed (8.2%; 95% CI = [6.7, 9.8] vs 16.1%; 95% CI = [14.1, 18.2]), having ever done so four times or more (3.8%; 95% CI = [2.7, 5.0] vs 9.8%; 95% CI = [8.1, 11.5]) and having self-harmed within the previous 12 months (6.2%; 95% CI = [4.8, 7.5] vs 11.6%; 95% CI = [9.9, 13.4]). About 1% (95% CI = [0.4, 1.2]) of all young people received medical treatment for self-harm in the previous 12 months.
Self-harm among 12- to 17-year-olds by sex and age group.
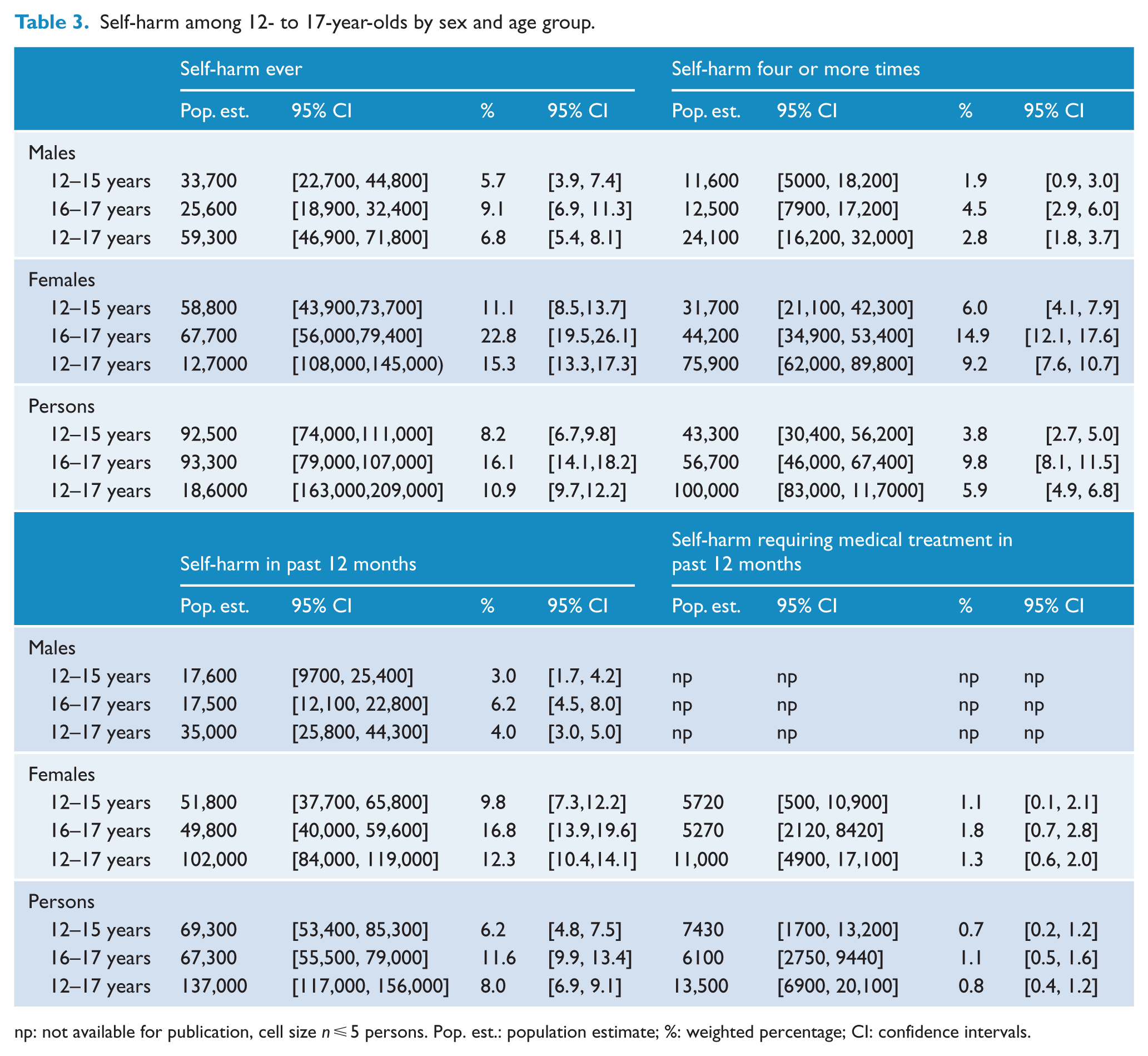
np: not available for publication, cell size n ⩽ 5 persons. Pop. est.: population estimate; %: weighted percentage; CI: confidence intervals.
Sex differences in these proportions were significant for both age groups (Table 3). Among 12- to 15-year-olds, higher proportions of females than males reported having ever self-harmed (11.1%; 95% CI = [8.5,13.7] vs 5.7%; 95% CI = [3.9, 7.4]), having self-harmed four or more times (6.0%; 95% CI = [4.1, 7.9] vs 1.9%; 95% CI = [0.9, 3.0]) and having self-harmed within the last 12 months (9.8%; 95% CI = [7.3, 12.2] vs 3.0%; 95% CI = [1.7, 4.2]). Among 16- to 17-year-olds, higher proportions of females than males reported having ever self-harmed (22.8%; 95%CI = [19.5, 26.1] vs 9.1%; 95% CI = [6.9, 11.3]), having self-harmed four or more times (14.9%; 95% CI = [12.1, 17.6] vs 4.5%; 95% CI = [2.9, 6.0]) and having self-harmed within the last 12 months (16.8%; 95% CI = [13.9, 19.6] vs 6.2%; 95% CI = [4.5, 8.0]).
Self-harm and mental disorder
Self-harming behaviour was highly prevalent among young people with parent-/carer-reported mental disorders or, particularly, where reported by themselves (Table 4). Eighteen percent (18.8%; 95% CI = [14.5, 23.0]) of all 12- to 17-year-old young people with any parent- or carer-reported diagnosis of anxiety, ADHD, conduct disorder or major depressive disorder reported engaging in self-harm in the past 12 months. This compared with 6.3% (95% CI = [5.3, 7.3]) of young people without any of these parent- or carer-reported diagnoses. Among young people who reported that they had DSM major depressive disorder, almost half (46.6%; 95% CI = [40.0, 53.1]) also reported that they had engaged in self-harm in the past 12 months. This compared with 4.4% (95% CI = [3.5, 5.2]) among young people without self-reported major depressive disorder.
Young people 12–17 years: self-harm and self-harm requiring medical treatment, by mental health status and sex.
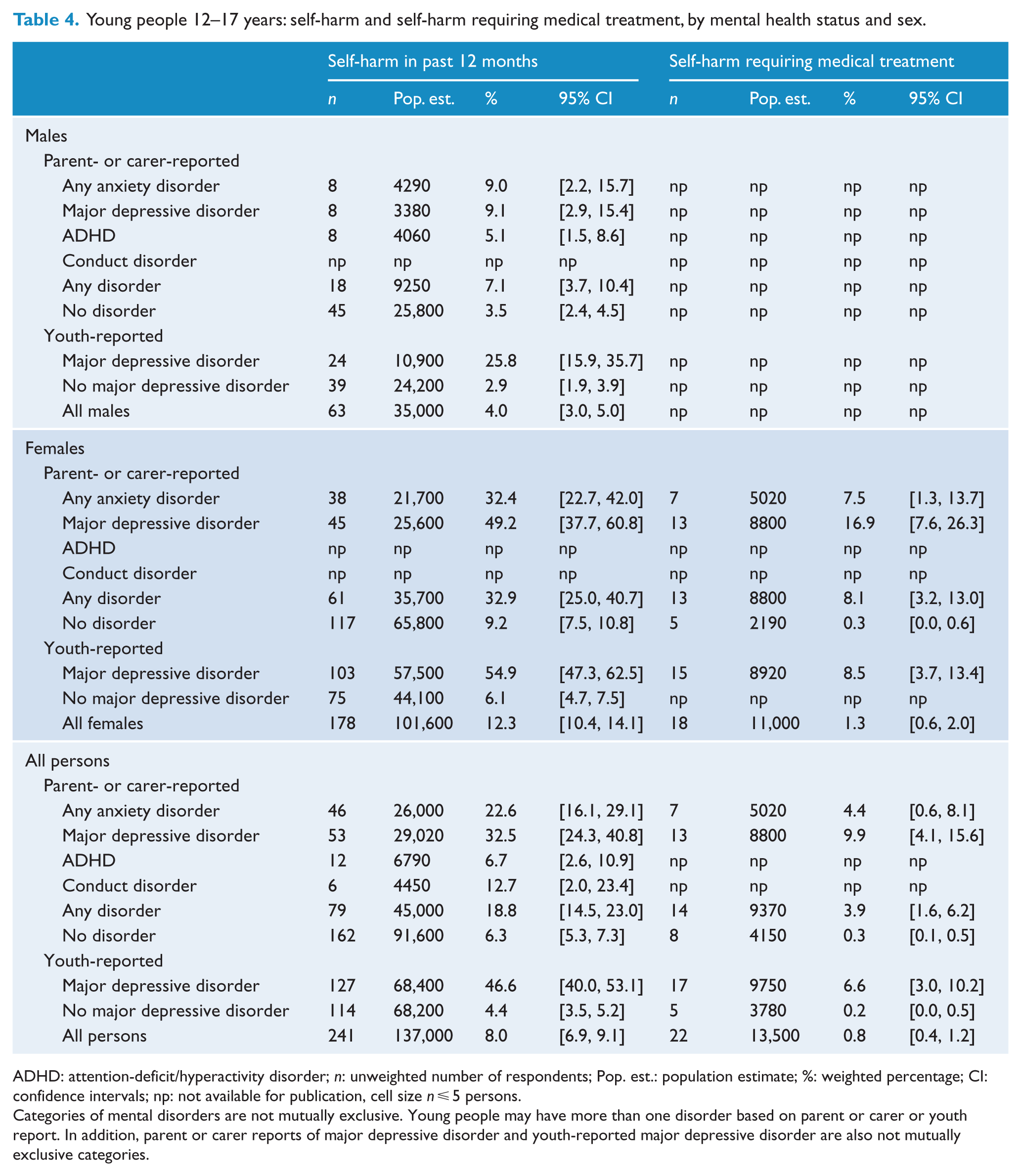
ADHD: attention-deficit/hyperactivity disorder; n: unweighted number of respondents; Pop. est.: population estimate; %: weighted percentage; CI: confidence intervals; np: not available for publication, cell size n ⩽ 5 persons.
Categories of mental disorders are not mutually exclusive. Young people may have more than one disorder based on parent or carer or youth report. In addition, parent or carer reports of major depressive disorder and youth-reported major depressive disorder are also not mutually exclusive categories.
Self-harm was more prevalent in the previous 12 months among those young people with a major depressive disorder (32.5%; 95% CI = [24.3, 40.8]) as reported by their parent or carer. This was followed, in order of magnitude of prevalence by those with anxiety disorders (22.6%; 95% CI = [16.1, 29.1]), conduct disorder (12.7%; 95% CI = [2.0, 23.4]) and ADHD (6.7%; 95% CI = [2.6, 10.9]) again based on parent and carer report (Table 4).
Females with a DISC diagnosis of major depressive disorder based on information in their own self-report had a significantly higher prevalence of 12-month self-harming behaviour than males (54.9%; 95% CI = [47.3, 62.5] vs 25.8%; 95% CI = [15.9, 35.7]). Significantly higher prevalence of 12-month self-harm was also seen for females with anxiety disorders based on parent or carer reports (32.4%; 95% CI = [22.7, 42.0] vs 9.0%; 95% CI = [2.2, 15.7]) than for males. The prevalence of ADHD and conduct disorders was too small among females and/or males to allow comparative estimation.
This overall high prevalence of self-harming behaviours among young people with mental disorders conceals striking variability when the data are stratified by type of disorder, informant (parent/carer or the young person), age and sex (Table S1). In all cases where mental disorder was present, the young people with the highest proportions of self-harming behaviours were female and older (aged 16–17 years vs 12–15 years). For example, among those young people with a self-reported DSM diagnosis of major depressive disorder identified using the DISC module, lifetime self-harm among 16- to 17-year-olds was reported by 62.2% (95% CI = [54.0, 70.3]) of females and 50.5% (95% CI = [37.0, 64.0]) of males. In the 12- to 15-year-olds, these proportions were 59.6% (95% CI = [45.8, 73.4]) for the females and 20.3% (95% CI = [2.9, 37.8]) for the males. Similarly, with respect to parent or carer reports of any DSM diagnosis of anxiety, lifetime self-harm among 16- to 17-year-olds was reported by 46.8% (95% CI = [34.6, 59.0]) of females and 21.1% (95% CI = [8.3, 33.9]) of males. In the 12- to 15-year-olds, these proportions were 28.2% (95% CI = [13.4, 42.9]) for the females and 12.2% (95% CI = [1.1, 23.4]) for the males. Proportions for the remaining disorders in these groups are presented in the supplementary table (S1).
Self-harm methods
Readers would be understandably interested in the methods of self-harm used by young people. Young people aged 12–17 years were asked about the methods of self-harm (see Table 1) and 69.2% of them reported cutting the last time that they self-harmed. We were unable to produce weighted estimates differentiated by age, gender and method owing to insufficient cell sizes.
Co-variation with social and demographic variables
Self-harm behaviour exhibited strong associations with mental disorder as well as with family composition, family income, parent and carer education and employment, family functioning and geographic location. Because these relationships typically co-occur, we provide an analysis of them using univariate and multivariate logistic regression. The quantitative information in these tables is voluminous and as a result, they are provided in a supplementary table (Table S2).
Lifetime self-harm, mental disorders and socio-demographic variables
Young people aged 12–17 years who had ever engaged in any self-harm were compared with those young people who had not done so (Table S2).
In univariate analyses, lifetime self-harm was significantly associated with youth-reported major depressive disorder (odds ratio [OR] 13.1; 95% CI = [9.6, 18.0]), parent- or carer-reported major depressive disorder (OR 5.0; 95% CI = [3.4, 7.3]), anxiety disorder (OR 3.3; 95% CI = [2.2, 4.8]) and conduct disorder (OR 2.5; CI = [1.1, 5.7]). The odds of reporting lifetime self-harm, relative to young people living in their original families were elevated in all other family types: step-family (OR 3.4; 95% CI = [2.1, 5.4]), sole parent family (OR 2.0; 95% CI = [1.5, 2.7]), blended family (OR 1.9; 95% CI = [1.1, 3.3]) and other family type (OR 2.9; 95% CI = [1.2, 7.1]). Lowest family income (i.e <$52,000 pa) and poor family function were both associated with youth-reported self-harm (OR 1.6; 95% CI = [1.1, 2.3]; and OR 2.4; 95% CI = [1.5, 4.0]). The other social and demographic variables were not significantly related to lifetime self-harm.
In multivariate analysis, lifetime youth-reported self-harm was principally associated with either youth- or parent-/carer-reported major depressive disorder (OR: 10.4; 95% CI = [7.5, 14.3] and OR: 2.1; 95% CI = [1.4, 3.1]) but not parent-reported anxiety disorders, conduct disorder or ADHD. Only family type and poor family function remained significant in the adjusted model with all other social and demographic variables being non-significant.
12-month self-harm, mental disorders and socio-demographic variables
While there were slight differences in the strength of the univariate associations between youth-reported 12-month self-harm, mental disorders and socio-demographic variables, the pattern of association with youth- and/or parent-/carer-reported major depressive disorder, anxiety, lowest family income, family types other than original family and poor family function was comparable with that found for lifetime self-harm.
Multivariate analysis of youth-reported 12-month self-harm again produced odds ratios of a similar magnitude and a pattern of associations similar to that seen in lifetime youth-reported self-harm. In other words, 12-month self-harm was associated with youth- or parent-/carer-reported major depressive disorder (OR: 12.1; 95% CI = [8.7, 16.7] and OR: 2.4; 95% CI = [1.6, 3.7]). Only family type and poor family function remained significant in the adjusted model with all other social and demographic variables being non-significant.
Self-harm frequency and medical treatment
Young people were asked if they had ever harmed themselves four or more times and whether any of these episodes had required medical treatment. Again, results were very similar to those described for the prevalence of lifetime and 12-month self-harm.
In univariate analyses, a higher frequency of self-harm (⩾4 times) was significantly associated with higher odds ratios for youth-reported major depressive disorder (OR: 17.7; 95% CI = [12.1, 25.7]), parent-/carer-reported major depressive disorder (OR: 7.5; 95% CI = [4.7, 11.8]), conduct disorder (OR: 4.0; 95% CI = [1.5, 10.6]) and any anxiety disorder (OR: 3.9; 95% CI = [2.4, 6.3]). Relative to original families, the odds of frequent self-harm were higher in all other family types and in those with poor family function. All other socio-demographic variables were not significant.
In multivariate analysis, most of these associations were attenuated to non-significance. However, a higher frequency of self-harm was significantly associated with adjusted higher odds ratios for youth-reported major depressive disorder (OR: 13.1; 95% CI = [8.9, 19.2]), and parent-/carer-reported major depressive disorder (OR: 2.8; 95% CI = [1.8, 4.6]).
Self-harm occasioning medical treatment was relatively rare and even with a robust sample size, we were unable to estimate a multivariately adjusted model. Univariate estimation revealed the odds of 12-month self-harm requiring medical attention to be significantly higher for those young people with self-reported or parent-reported major depressive disorder and any anxiety disorder. Young people from sole parent families, poor families and families with less-than-very-good family functioning also had significantly higher odds of reporting medical treatment for self-harm.
Relationship between self-harm, suicidal behaviour and mental disorder
We have previously reported the survey results for suicidal behaviour (Zubrick et al., this issue). Along with the data reported here, we are able to assess the relationships between self-harm, suicide and mental disorder.
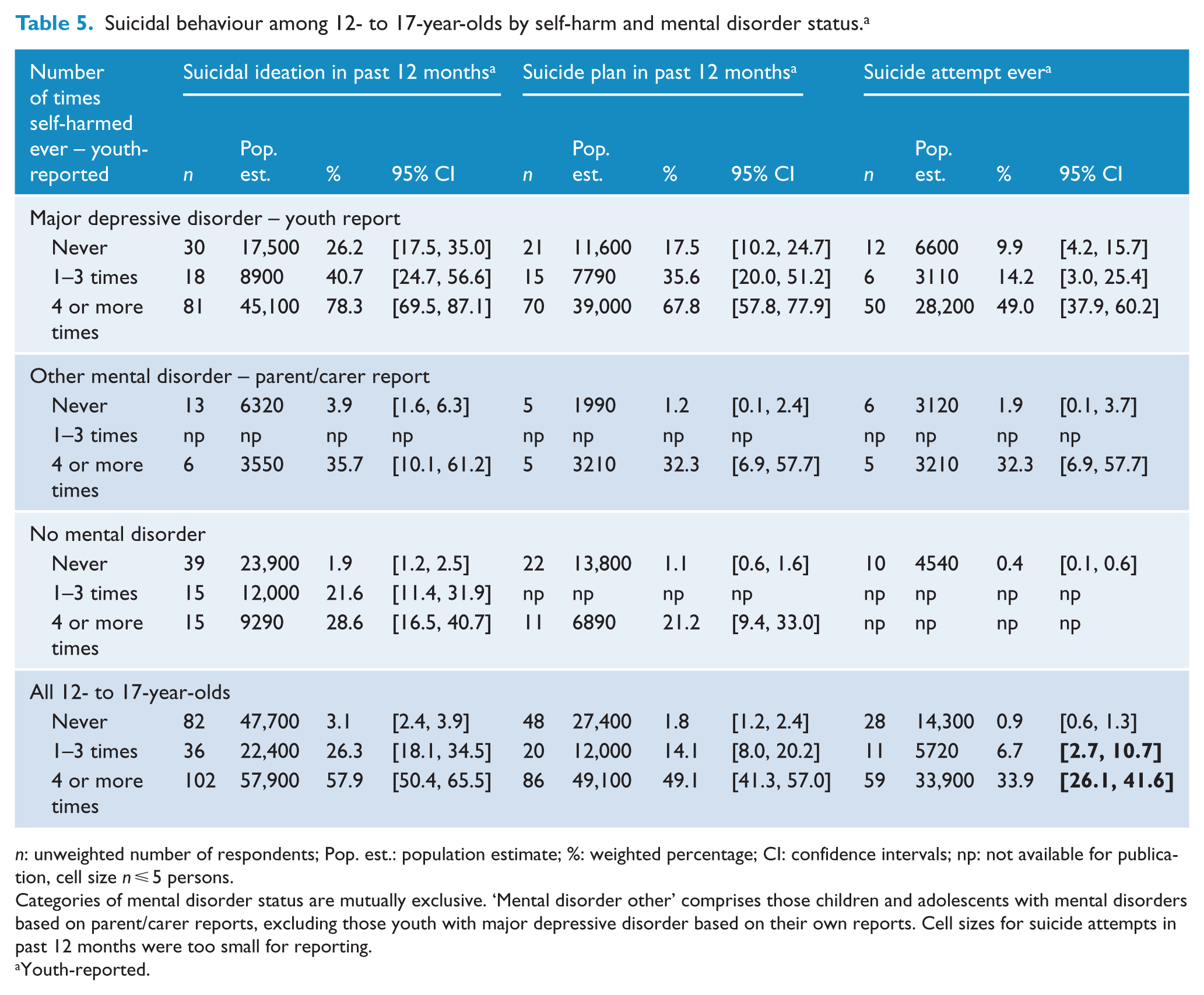
There is a strong association between youth-reported non-suicidal self-harm and youth-reported suicide behaviours (Table 5). Greater frequency of non-suicidal self-harm behaviour was associated with significantly higher proportions of young people who also reported suicidal behaviour. These proportions became strikingly high in the presence of mental disorders – particularly major depressive disorder.
Suicidal behaviour among 12- to 17-year-olds by self-harm and mental disorder status. a
n: unweighted number of respondents; Pop. est.: population estimate; %: weighted percentage; CI: confidence intervals; np: not available for publication, cell size n ⩽ 5 persons.
Categories of mental disorder status are mutually exclusive. ‘Mental disorder other’ comprises those children and adolescents with mental disorders based on parent/carer reports, excluding those youth with major depressive disorder based on their own reports. Cell sizes for suicide attempts in past 12 months were too small for reporting.
Youth-reported.
Starting first with those young people with no mental disorder, 21.6% (95% CI = [11.4, 31.9]) of those who had self-harmed 1–3 times also had suicidal ideation. The remaining estimates for suicide plan in the last 12 months and lifetime suicide attempt were not calculated owing to too few cases to produce reliable estimates.
In contrast though, for young people aged 12–17 years with self-reported DISC-IV major depression, 40.7% (95% CI = [24.7, 56.6]) of those who had ever engaged in self-harm between 1–3 times also reported that they had suicidal ideation in the past 12 months; 35.6% (95% CI = [20.0, 51.2]) reported making a suicide plan in the last 12 months, and 14.2% (95% CI = [3.0, 25.4]) had ever attempted suicide. When self-harm was reported occurring four or more times among young people aged 12–17 years with self-reported DISC major depression, then 78.3% (95% CI = [69.5, 87.1]) reported they had suicidal ideation in the past 12 months; 67.8% (95% CI = [57.8, 77.9]) reported making a suicide plan in the last 12 months and 49.0% (95% CI = [37.9, 60.2]) had ever attempted suicide.
Discussion
These results describe the Australian phenomenology of self-harming without suicidal intent in young people aged 12–17 years and provide national estimates of self-harming reported by them. Our aims were to estimate the prevalence of self-harming behaviours, describe their co-morbidity with mental disorders and describe their co-variation with key social and demographic variables. There are several features of these that merit comment.
First, with respect to non-suicidal self-harming, in any 12-month period, about 8% of all 12- to 17-year-olds report engaging in self-harming behaviour. This equates to about 137,000 young people. The prevalence of self-harming increases with age and 11.6% of 16- to 17-year-olds had engaged in self-harm within the last 12 months. Second, the prevalence of self-harming within any 12-month period is very high for young people with a mental disorder. It is 34.8% in young people aged 16–17 years with a mental disorder and it is the highest, 51.3%, where the young person has met the DSM-IV criteria for a major depressive disorder based on their responses on the DISC.
Third, social and demographic correlates of self-harm persist and show commonalities with those seen in suicidal behaviour – in both magnitude and pattern (see Zubrick et al., submitted). After sex, age and mental health, family structure and function remain the major correlates of self-harm. In unadjusted models, significantly higher proportions of self-harming behaviours are observed in families with low income, low parent/carer education, families in which the sole or both parents are unemployed and sole parent families and where family function is reported as poor. This would suggest that efforts at addressing social disadvantage and/or at reducing barriers to provision and access to mental health care for this segment of the Australian population might produce onward reductions in prevalence of self-harm.
Fourth, most, but not all, of these socio-economic determinates become non-significant once the young person’s mental health status is included. Typically, across self-harm behaviours, the presence of a mental disorder shows the single and largest association with lifetime and 12-month self-harm, with only sole parent family status and poor family functioning remaining significant.
Fifth, these data give support to the Owens et al. (2002) report that suicide risk among those who self-harm is greatly and significantly elevated relative to the general population. Our findings particularly show this increases even more so in the presence of major depressive disorder. These associations would support the inclusion of the monitoring of self-harm, and indicators of its treatment and prevention in national suicide prevention strategies.
Sixth, our questions to the young person about self-harm were specifically phrased to denote non-suicidal self-harm (i.e ‘ … deliberately done something to yourself to cause harm or injury, without intending to end your own life?’ (italics added)). While it is not possible to discern what the young person actually interpreted this to mean, we would note, that for many of them who did report self-harm behaviours without intending to end their life, they also went on to report having engaged in high levels of suicidal behaviour including making a suicide attempt(s). While practitioners and mental health professionals may wish to distinguish between self-harm without suicidal attempt, the findings here suggest a substantial blurring of this boundary in the behaviours of young people based on their self-reports. In short, however, measured, self-harm when reported carries substantial risk of concomitant suicidal behaviour.
Finally, there are some results that are not significant that should be noted. The survey was a national survey and not designed to produce State or jurisdictional estimates. It was however, possible to produce estimates distinguishing major cities from inner and outer regional areas and remote and very remote areas. None of these distinctions produced statistically significant differences in the proportions of young people engaging in self-harm.
There are of course limitations to this report. First, the sheer quantity and relative depth of the information collected in the survey precludes a comprehensive profiling of the results. This report principally presents the prevalence of self-harm and their social and demographic correlates. Other features of these behaviours with respect to methods and important risk factors (i.e. drugs and alcohol) are not described here but are clearly relevant. Second, these results rely entirely on self-reported data with all the caveats that apply to uncertain reliability, social desirability and incomplete information. There are limits to what can be inferred without in-depth interviewing and developmental assessments. Third, the achieved response rate of the survey was 55%. While our analyses of the characteristics of our responders relative to the Australian population suggests that the YMM sample is broadly representative of the Australian population, there may be differences and biases that remain uncorrected or unknown and that affect the generalizability of findings. Finally, even with a robust sample, some cell sizes remain too small resulting in estimates with large confidence intervals or insufficient data to produce any estimate.
Australia has made a concerted and sustained effort over 20 years to improve the range, distribution, access and quality of mental health care. Many of these efforts have explicitly sought to address the promotion of mental health and the prevention and treatment of mental disorders for younger Australians. Among Australian young people, mental disorders affect about 14%, and the overall prevalence has remained essentially stable over the past 16 years (see Lawrence et al., this issue). Some may be disappointed by this, while others might regard this as an achievement in an era where mental health and mental disorders have had a prominence in health care delivery and in the public promotion and awareness of their importance, their signs and the need for their prompt care.
These findings establish national Australian estimates for self-harm behaviours and against which future comparisons might be made. In considering the demonstrated higher risks in these young people for continued harm or possible death, these findings encourage and support ongoing initiatives for the reduction of self-harm through mental health promotion, improved mental health literacy and continuing reform of mental health services to ensure such services are accessible to, and meet the needs of families and young persons.
Footnotes
Acknowledgements
The authors wish to express their gratitude to the 6310 families who participated in the survey.
Declaration of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The second Australian Child and Adolescent Survey of Mental Health and Wellbeing was funded by the Australian Government Department of Health. The survey was funded by the Australian Government Department of Health. Professors Lawrence and Zubrick are supported by a Centre of Excellence grant from the Australian Research Council (CE140100027).