
Abstract
Objective:
Adverse childhood experiences are well-recognized risk factors for a variety of mental health issues, including depression, suicide attempts and non-suicidal self-injury. However, less is known about whether childhood adversity, in the form of low parental care, overprotection and abuse, is associated with suicide attempt and non-suicidal self-injury within a sample of depressed adults.
Method:
The sample of outpatients (n = 372) was drawn from two randomized depression trials. Childhood adversity variables, depression severity, age of first depressive episode (major depression episode onset), lifetime suicide attempt and non-suicidal self-injury were recorded at baseline. The association between variables and outcome measures was examined using partial correlations, univariate and multivariate logistic regressions.
Results:
Low maternal care was significantly associated with suicide attempt; low paternal care was associated with non-suicidal self-injury; overprotection was not associated with either outcome. Other risk factors for suicide attempt were major depression episode onset and baseline depression severity. Major depression episode onset was also a risk factor for non-suicidal self-injury. Abuse, regardless of how it was measured, was not significantly associated with either behaviour after adjusting for its correlations with low maternal or paternal care.
Conclusion:
In this sample of depressed adults, the quality of ongoing, intra-familial relationships, as measured by levels of parental care, had a greater impact on suicide attempt and non-suicidal self-injury than abuse. As the findings were not a priori hypotheses, they require replication. Although the cross-sectional study design limits causal determination, the findings suggest different childhood risk factors for suicide attempt and non-suicidal self-injury and underscore the impact of low parental care on these two behaviours. These findings signal to clinicians the importance of asking specifically about suicide attempts, and non-suicidal self-injury, as well as levels of parental care in childhood. When endorsed, low parental care may be considered an important factor in contextualizing a patient’s depression and potential risk for suicide and non-suicidal self-injury.
Introduction
Research highlights the experience of childhood adversity as a risk factor for developing depression (Alloy et al., 2006) and other mental health issues in adulthood (Thabrew et al., 2012). Two studies, reporting on more than 60,000 people in 22 countries, estimated that 25–44% of adult mental health disorders were related to the experience of childhood adversity (Green et al., 2010; Kessler et al., 2010). Childhood physical and sexual abuse are particular risk factors for developing adult depression (Maniglio, 2010; Zlotnick et al., 2001).
In addition, childhood sexual abuse (CSA) has been identified as a particular risk for suicide attempts (SAs) and non-suicidal self-injury (NSSI; Maniglio, 2011; Romans et al., 1995; Ystgaard et al., 2004). The World Mental Health survey of 21 countries found that CSA was associated with an increase in the odds of making a SA (range: 2.9- to 10.9-fold increase), depending on the victim’s age at the time of the abuse (Bruffaerts et al., 2010).
However, not all researches agree on CSA’s role with respect to suicidal behaviour. In a sample of depressed outpatients, SAs were not independently related to a history of CSA (Zlotnick et al., 2001). Similarly, in a meta-analysis of 45 studies reporting on NSSI, researchers concluded that CSA does not play a central role but is ‘modestly related’, due to correlations with the same psychiatric risk factors (Klonsky and Moyer, 2008). Kaess et al. (2013) suggested that the associations found between abuse and SA or NSSI might be due to the influence of high-risk family environments on abuse rather than the abuse itself.
Defined many ways in the literature, childhood adversity is examined in three categories in this study. The first two are the experiences of low parental care or overprotection, as measured by the Parental Bonding Instrument (PBI; Parker, 1979), and the third is abuse, whether psychological, physical or sexual. Very few studies examine the specific combination of low parental care and overprotection, measured separately for mother and father, in association with SA. Even fewer examine these adverse childhood experiences in relation to NSSI in adults with depression. The primary associations reported were between low parental care from both parents or just one’s mother and adult suicidal behaviours (Beautrais, 2002; Dale et al., 2010; Ehnvall et al., 2008; Goldney, 1985; Heider et al., 2007).
In terms of differentiating risk factors between SA and NSSI with respect to childhood adversity, some evidence exists for low maternal care or the combination of low parental care and overprotection to act as a particular risk for suicidal behaviours (Adam et al., 1994; Ehnvall et al., 2008; Freudenstein et al., 2011; Wichstrøm, 2009). One study which explicitly examined NSSI in adolescents and young adults reported that maternal antipathy and neglect, as measured by the Childhood Experiences of Care and Abuse–Questionnaire (CECA-Q; Bifulco et al., 1994), were significantly related to NSSI, over and above experiences of childhood abuse (Kaess et al., 2013). Within the adolescent literature, the overall association reported is between affectionless control (low care combined with overprotection) and suicidal behaviour (Adam et al., 1994; Freudenstein et al., 2011).
Given the paucity of studies examining the relationship between adverse childhood experiences and SA or NSSI, we sought to examine whether low parental care, overprotection or abuse measured three ways was associated with an increased risk for SA and NSSI in adult outpatients with depression. While much of the literature reports an association between abuse, SA and NSSI, a smaller amount reports the association between these behaviours and low levels of parental care, together with overprotection. Given our previous findings on response to depression treatment using the same variables (Johnstone et al., 2009, 2013), we hypothesized that low parental care may contribute as great a risk factor as abuse for SA and NSSI. We also sought to examine whether the risk factors for SA differed from those associated with NSSI, based on the three adverse childhood experiences examined. While SA and NSSI may be jointly conceptualized as self-harm behaviours that fall along a continuum (Andover and Gibb, 2010; Hargus et al., 2009), we hold the view that patients engage in SA and NSSI for different reasons, and some research supports this position (Favazza, 1998; Muehlenkamp, 2005; Nock, 2005). As such, we hypothesized that the risk factors for the two behaviours may differ as well. We did not form an a priori hypothesis regarding differing risk factors, but through intentionally asking about SA and NSSI separately, we sought to answer the question.
Methods
Sample
Depressed outpatients were invited to participate in two consecutive studies conducted in a university-based clinical research unit. The first 195 eligible patients were enrolled in a randomized control trial of medication comparing fluoxetine and nortriptyline, while the second intake of eligible patients (177) were randomized to either cognitive behavioural therapy (CBT) or interpersonal psychotherapy (IPT) for depression. Between the two trials, 372 patients participated (133 men, 239 women). Patients were recruited over several years, with similar recruiting strategies, investigators and clinicians for both trials. For details regarding patient recruitment versus enrolment for the medication trial, see Joyce et al. (2002), and for the psychotherapy trial, see Luty et al. (2007). All patients were provided with study details and gave written consent prior to participation. Psychiatric inclusion criteria for both studies included a principal and current diagnosis of a non-psychotic major depression episode (MDE), based on Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) criteria (American Psychiatric Association, 1994). Patients had to be 18 years or older and had to be medication-free, except for birth control pills or an occasional hypnotic, for a minimum of 2 weeks. Psychiatric exclusion criteria for both studies included schizophrenia, a history of mania, but not hypomania, severe alcohol and/or drug dependence or severe antisocial personality disorder which may interfere with study adherence. However, no patient assessed for possible inclusion was excluded due to alcohol or drug dependence or antisocial personality disorder. Patients with a major medical illness were also excluded. Both studies were approved by the Canterbury Ethics Committee, New Zealand.
Measures
Depression severity at baseline, prior to treatment randomization, was assessed by the clinician-rated Montgomery–Åsberg Depression Rating Scale (MADRS; Montgomery and Åsberg, 1979). Patients were also asked about their age at the time of their first depressive episode. The childhood variables measuring experiences of low care and overprotection were derived from the PBI (Parker, 1979; Parker et al., 1979). The PBI is a 25-question self-report measure which asks respondents to rate the level of care and protection received from their mother and father, independently, in the first 16 years of life. Responses are coded 0–3: very unlike, moderately unlike, moderately like and very like, with scores ranging from 0 to 36 on the care scale and from 0 to 39 on the protection scale. Patients with high care scores reported experiencing a caring and affectionate relationship with that parent; those with low scores reported experiencing emotional neglect or rejection. Conversely, high protection scores indicated the experience of overprotection or being controlled by the parent rated, while low scores indicated the patient felt able to make independent decisions and differentiate from the parent. The PBI has been used for three decades around the world, is a reliable and valid measure of childhood experiences (Murphy et al., 2010; Wilhelm et al., 2005) and has been found to be stable regardless of mood state (Gerlsma et al., 1993; Wilhelm et al., 2005).
The abuse measures resulted from a structured, nurse-administered interview and assessed for the presence, frequency and type of abuse a patient may have experienced in childhood. The structured questions were identical to the ones used by Fergusson et al. in a longitudinal study of more than 1000 New Zealanders (Fergusson et al., 2008). Open-ended questions were asked of patients about psychological, physical or sexual abuse or threat of abuse before the age of 16 years. The questions were worded, ‘Before 16, were you ever: Threatened with abuse by someone; emotionally or psychologically abused; beaten so badly you had to see (or should have seen) a doctor’. Responses were collapsed into three frequencies for each category questioned: 0 (no abuse), 1 (occurring 1–3 times), 2 (occurring 4 or more times). Total abuse scores ranged from 0 (no abuse) to 12 (repeated abuse reported for all six questions). For analytical purposes, the abuse scores were collapsed into three categories: ‘none’ for a zero score, ‘some’ for scores of 1–4 and ‘severe’ for scores 5+. The CSA variable was derived from the same interview as the abuse variable but included only those questions relating to sexual abuse. The three CSA categories asked about were non-contact sexual abuse, such as exposure to or being forced to watch sexual activity; contact sexual abuse, such as unwanted sexual touching or attempted intercourse; and sexual intercourse or rape. In reporting the CSA variable, ‘none’ was recorded if the patient reported no sexual abuse. ‘Severe’ was defined as any sexual abuse involving intercourse, more than three reports of contact sexual abuse or a combined score of five or more instances of non-contact and contact sexual abuse. ‘Some’ was defined by any report of non-contact sexual abuse and/or three or fewer incidents of contact sexual abuse.
Outcome measures
The two categorical outcome measures, lifetime SA and NSSI, resulted from structured questions asked by the psychiatrist at baseline. Patients were first asked, ‘Have you ever attempted suicide?’ An affirmative response was followed by questions about number of attempts, intent, age of most serious attempt and potential lethality. Next, patients were asked, ‘Have you ever deliberately harmed yourself, for example, to relieve tension or feel better?’ If ‘yes’, patients were asked how often they had engaged in such behaviour and what methods were used. An affirmative response was coded as one; a negative response was coded as zero. Asking about SA separate from NSSI opened up the possibility of examining for different risk factors for the two behaviours.
Further to the creation of the two categorical outcome measures, the relationships between these two behaviours were examined. This was accomplished by creating one new variable with four categories. The first category recorded the number of patients who did not report making a SA or engaging in NSSI. The second category recorded the patients who reported making a SA but not engaging in NSSI. The third category recorded those who engaged in NSSI but never made a SA. Finally, the fourth category recorded those patients who reported engaging in both behaviours. The creation of this post hoc variable was undertaken for informational purposes and to increase the understanding around these behaviours as separate, but interrelated. As the numbers in each cell were small, statistical power was an issue, so formal, comparative analyses were not performed on this post hoc variable.
Trial procedures
At baseline, the patients were interviewed and completed the self-report measures. Following the assessment, eligible patients were randomized into either the medication trial or the psychotherapy trial. Because the specific nature of the two trials is not relevant for the outcomes of this paper, the details of both trials are outlined elsewhere. Medication trial details can be found in Joyce et al. (2002) and details for the psychotherapy trial in Luty et al. (2007).
Statistical analyses
The data were analysed using the Statistical Package for the Social Sciences (SPSS, v.19, IBM Corporation, 2012). The analyses reported represent an exploratory examination of childhood adversity as risk factors for lifetime SA and NSSI among a depressed sample. Descriptive statistics were used to quantify baseline variables and the two outcome measures. Independent t-tests and chi-square were used to compare the variables as appropriate. Yates Continuity Correction values for chi-square were used as a more conservative measure of outcome for 2 × 2 tables. Effect sizes were calculated using either φ coefficient or r2, as appropriate. Initial analyses were conducted using univariate logistic regressions with the demographic, clinical and childhood variables for the two outcome measures. Given the inter-correlations among childhood adversity variables, partial correlations were used to examine whether an observed relationship between a childhood variable and an outcome measure was influenced by a confounding childhood variable. Partial correlations were also conducted for highly correlated demographic and clinical variables such as age, MDE onset and MADRS. Based on the results from the partial correlations, the variables shown to make a significant, independent contribution were included in the multivariate model. To further assess the variables’ predictive ability, forced-entry multivariate logistic regressions with all the variables significant in univariate analyses were conducted for SA. A backward stepwise regression confirmed the results. To illustrate statistical findings, the maternal and paternal care variables were categorized into tertiles.
Results
Total sample characteristics
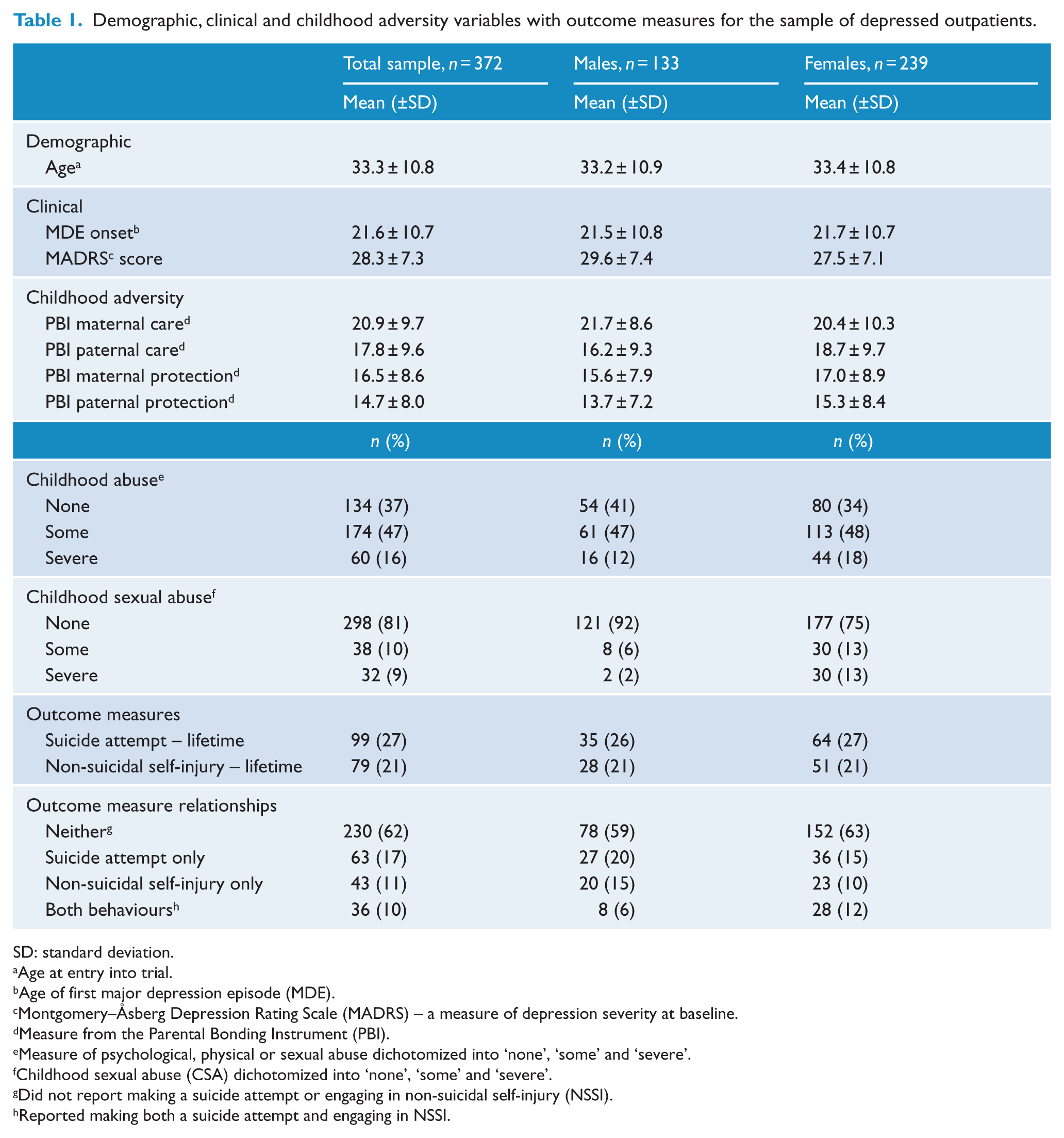
Table 1 presents the demographic, clinical and childhood adversity variables and two outcome measures for the total sample of 372 outpatients with depression. These data are shown by gender as well. A total of 27% of the total sample reported making a lifetime SA; 21% reported engaging in NSSI. For reference, the number and percentage of patients who reported none, one or both of these behaviours is presented as well. A total of 62% of the total sample did not report making a SA or engaging in NSSI, while 10% of the sample reported both behaviours. A total of 17% reported making only a SA and 11% reported only engaging in NSSI.
Demographic, clinical and childhood adversity variables with outcome measures for the sample of depressed outpatients.
SD: standard deviation.
Age at entry into trial.
Age of first major depression episode (MDE).
Montgomery–Åsberg Depression Rating Scale (MADRS) – a measure of depression severity at baseline.
Measure from the Parental Bonding Instrument (PBI).
Measure of psychological, physical or sexual abuse dichotomized into ‘none’, ‘some’ and ‘severe’.
Childhood sexual abuse (CSA) dichotomized into ‘none’, ‘some’ and ‘severe’.
Did not report making a suicide attempt or engaging in non-suicidal self-injury (NSSI).
Reported making both a suicide attempt and engaging in NSSI.
Comparing variables by gender within the total sample
In Table 1, data are compared by gender within the total sample. No significant differences were found in demographic or clinical variables or in the outcome measures. However, differences between the genders existed for two of the childhood adversity variables. Among the PBI scores, only paternal care was significantly different, with women reporting higher care from their fathers, t(370) = −2.35, p = 0.02. In addition, more women reported experiencing CSA, 26%, compared to 8% of men, χ2(2, n = 368) = 18.79, p < 0.01. No significant differences were noted for the other childhood adversity variables in relation to gender within the total sample.
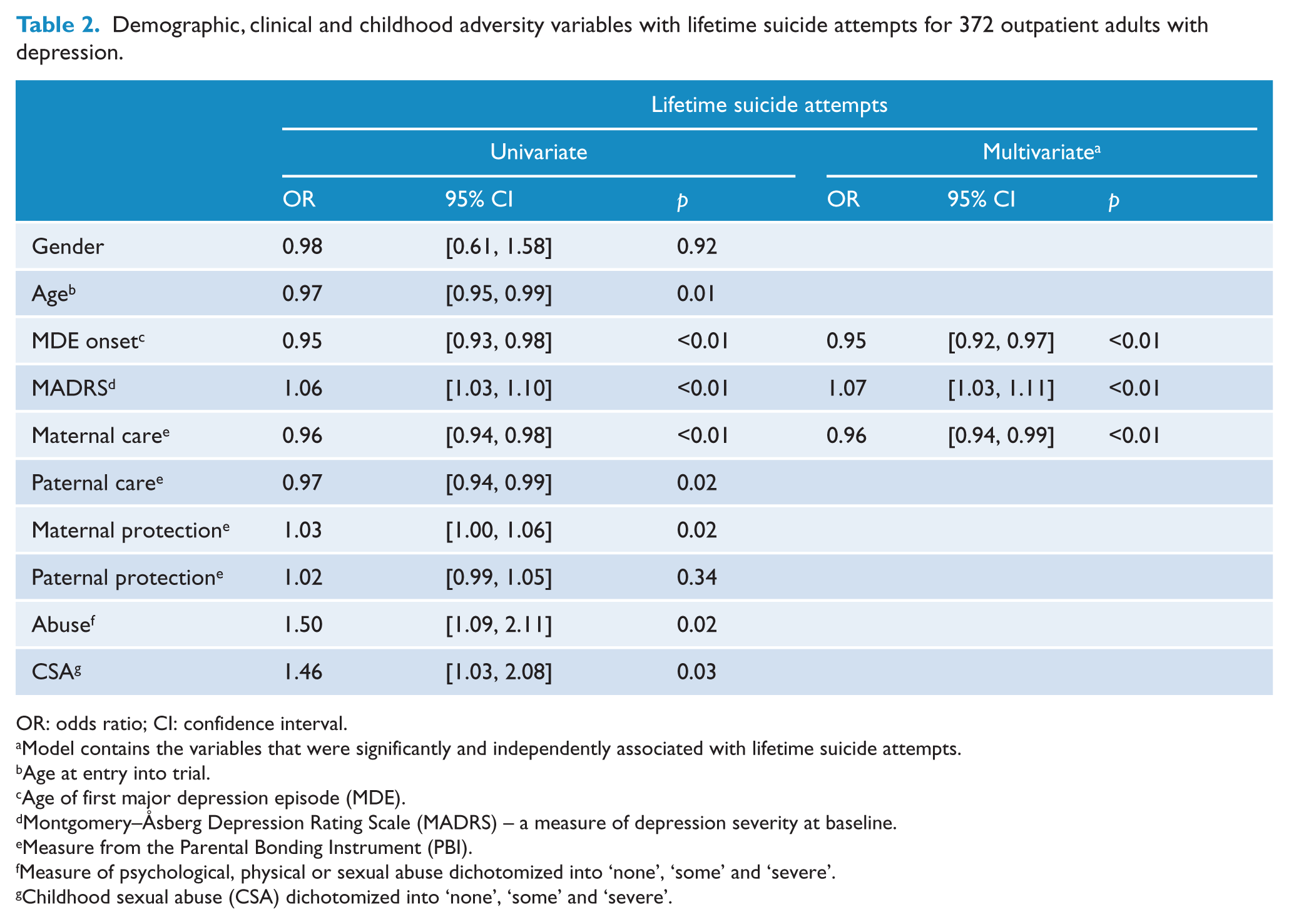
Predictors of lifetime suicide attempts
Table 2 shows the univariate and multivariate associations for the demographic, clinical and childhood variables with lifetime SA. In univariate analyses, eight variables were significantly associated with SA: age, age of first MDE onset, MADRS score, maternal care, paternal care, maternal protection, abuse and CSA.
Demographic, clinical and childhood adversity variables with lifetime suicide attempts for 372 outpatient adults with depression.
OR: odds ratio; CI: confidence interval.
Model contains the variables that were significantly and independently associated with lifetime suicide attempts.
Age at entry into trial.
Age of first major depression episode (MDE).
Montgomery–Åsberg Depression Rating Scale (MADRS) – a measure of depression severity at baseline.
Measure from the Parental Bonding Instrument (PBI).
Measure of psychological, physical or sexual abuse dichotomized into ‘none’, ‘some’ and ‘severe’.
Childhood sexual abuse (CSA) dichotomized into ‘none’, ‘some’ and ‘severe’.
As the childhood adversity variables are inter-correlated, partial correlations among these variables with SA were conducted. Only maternal care had an independent influence on SA, and any observed relationship among the other childhood adversity variables with SA could be explained by their association with low maternal care. Given that MDE onset and age are also highly correlated, a partial correlation between these two variables with SA was conducted. Results indicated that MDE onset had an independent influence on SA, and the observed relationship between age and SA was influenced by MDE onset. Partial correlations between MDE onset and MADRS showed that the two variables made significant, independent contributions to SA.
To create the most parsimonious multivariate model for predicting SA, we entered the three variables that demonstrated an independent association with SA: MDE onset, MADRS and maternal care. This model was significant, χ2 = 40.94, p < 0.01, and explained 11–16% of the variance in SA. The only independent adverse childhood predictor of SA was maternal care (odds ratio [OR] = 0.96, 95% confidence interval [CI]: [0.94, 0.99], p < 0.01). As maternal care was examined as a continuous variable, the OR is small.
To visually illustrate the association among maternal care levels and SA, maternal care was categorized into tertiles. Figure 1 shows the percentage of patients who reported a SA by maternal care levels in tertiles. When maternal care in tertiles was included in the multivariate analyses with MDE onset and MADRS, the whole model was significant χ2(4, n = 352) = 39.88, p < 0.01. Those who reported low maternal care (scores ⩽ 15) were 2.3 times more likely to have attempted suicide in comparison to those with high maternal care (scores ⩾ 26; 95% CI: [1.26, 4.24], p = 0.01).
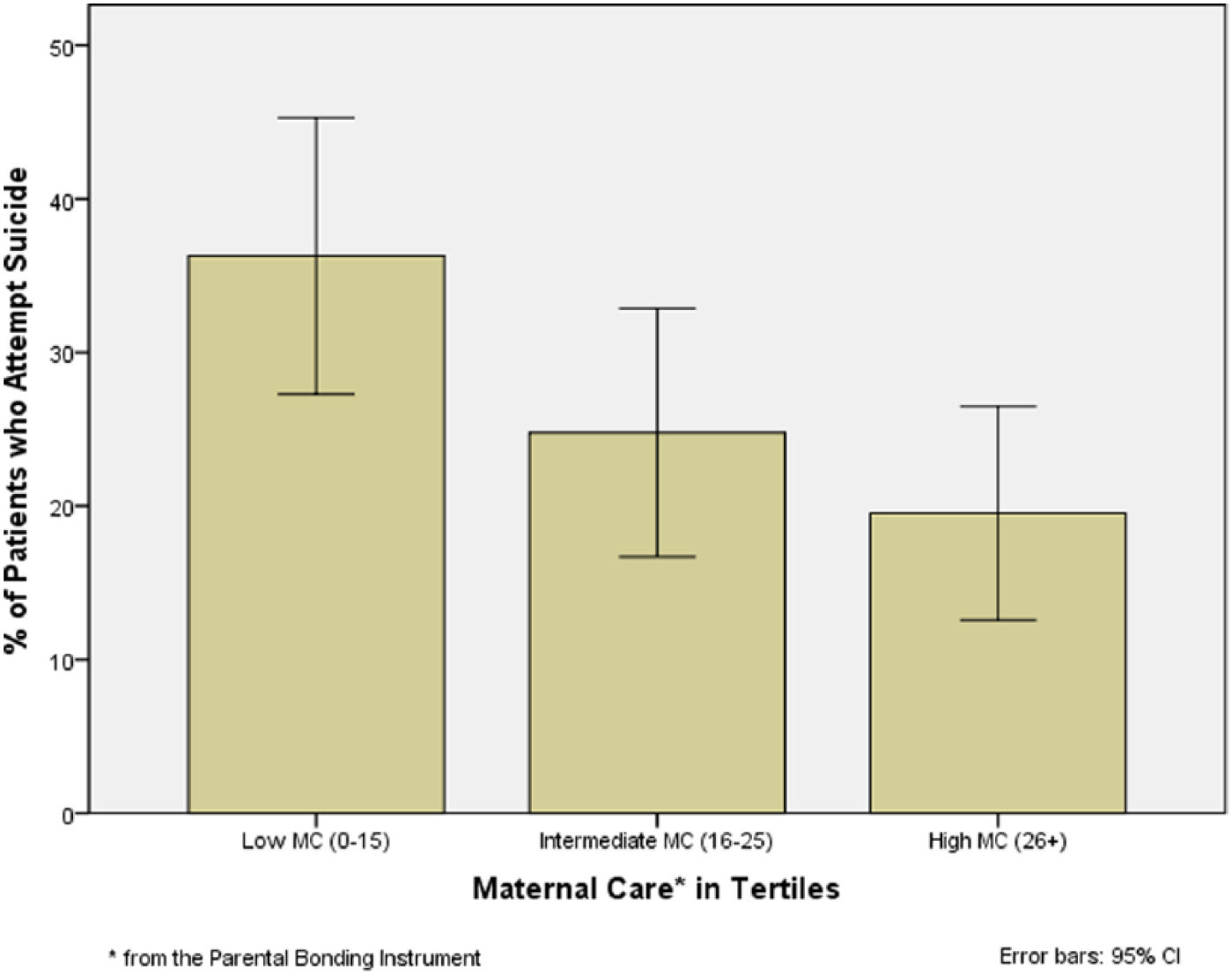
Lifetime suicide attempts by maternal care in tertiles.
Predictors of NSSI
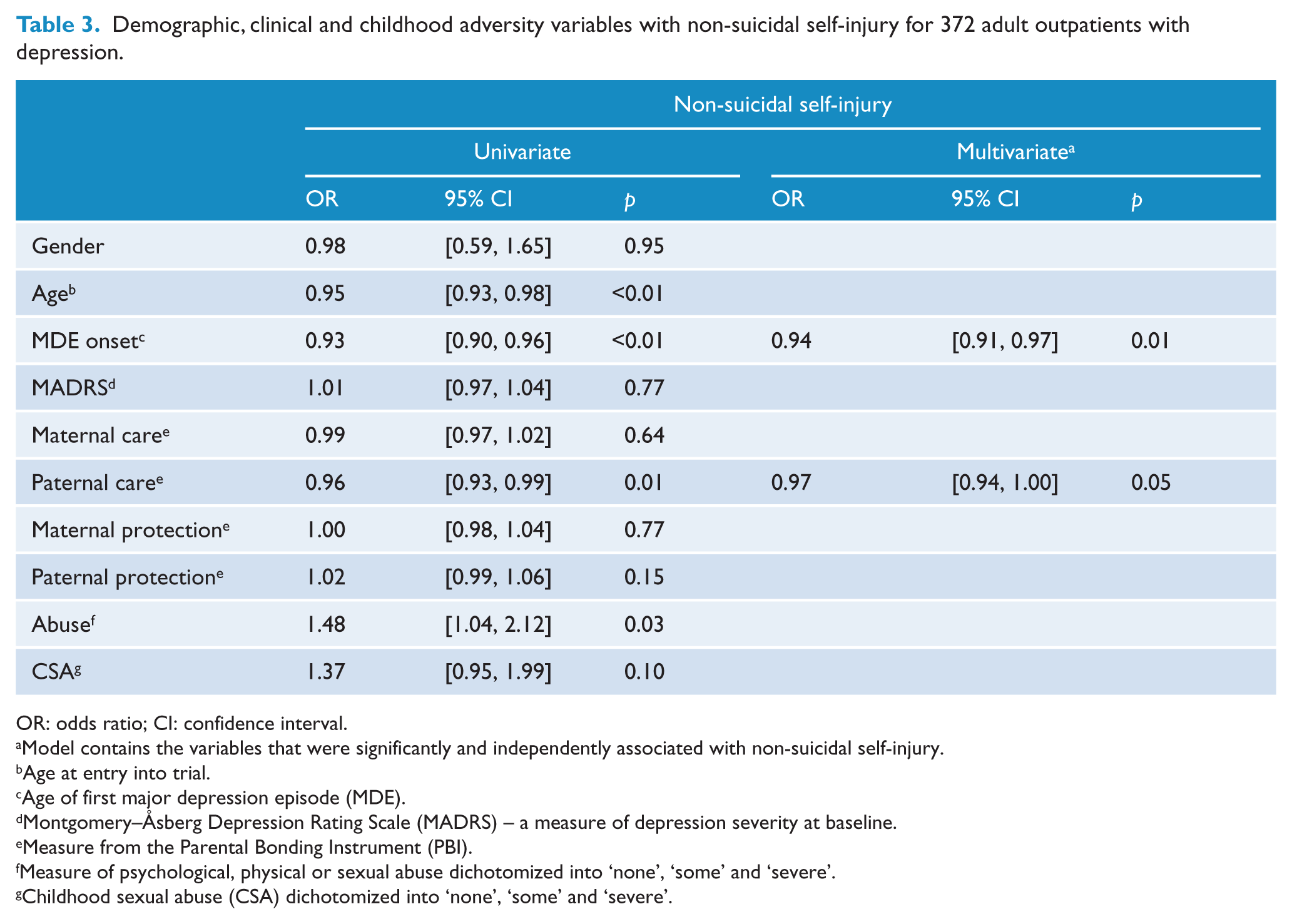
Table 3 presents the univariate and multivariate analyses for the demographic, clinical and childhood adversity variables with NSSI. In the univariate model, age, MDE onset, paternal care and abuse were associated with NSSI. Given their inter-correlations, partial correlations were conducted between paternal care and abuse with NSSI. The results showed that the observed univariate relationship between abuse and NSSI was no longer significant. The apparent association between the two could be explained by abuse’s association with low paternal care. A partial correlation was also conducted between age and MDE onset. The results showed that only MDE onset made a significant, independent contribution to NSSI.
Demographic, clinical and childhood adversity variables with non-suicidal self-injury for 372 adult outpatients with depression.
OR: odds ratio; CI: confidence interval.
Model contains the variables that were significantly and independently associated with non-suicidal self-injury.
Age at entry into trial.
Age of first major depression episode (MDE).
Montgomery–Åsberg Depression Rating Scale (MADRS) – a measure of depression severity at baseline.
Measure from the Parental Bonding Instrument (PBI).
Measure of psychological, physical or sexual abuse dichotomized into ‘none’, ‘some’ and ‘severe’.
Childhood sexual abuse (CSA) dichotomized into ‘none’, ‘some’ and ‘severe’.
Given the results of the partial correlations, only paternal care and MDE onset were entered in a forced-entry multivariate logistic regression as predictors of NSSI. The whole model was significant, χ2 = 25.56, p < 0.01. The only independent childhood adversity predictor was paternal care (OR = 0.97, 95% CI: [0.94, 1.00], p = 0.05). The OR is small because the level of paternal care was examined as a continuous variable.
For the purpose of illustration, Figure 2 shows the percentage of patients who reported NSSI by paternal care levels in tertiles. When this variable was included in the forced-entry multivariate analyses with MDE onset, the whole model was significant, χ2 = 29.71, p < 0.01. Those reporting paternal neglect (scores ⩽ 14) were 2.7 times more likely to engage in NSSI than those with high paternal care (scores ⩾ 23; 95% CI: [1.30, 5.48], p = 0.01).
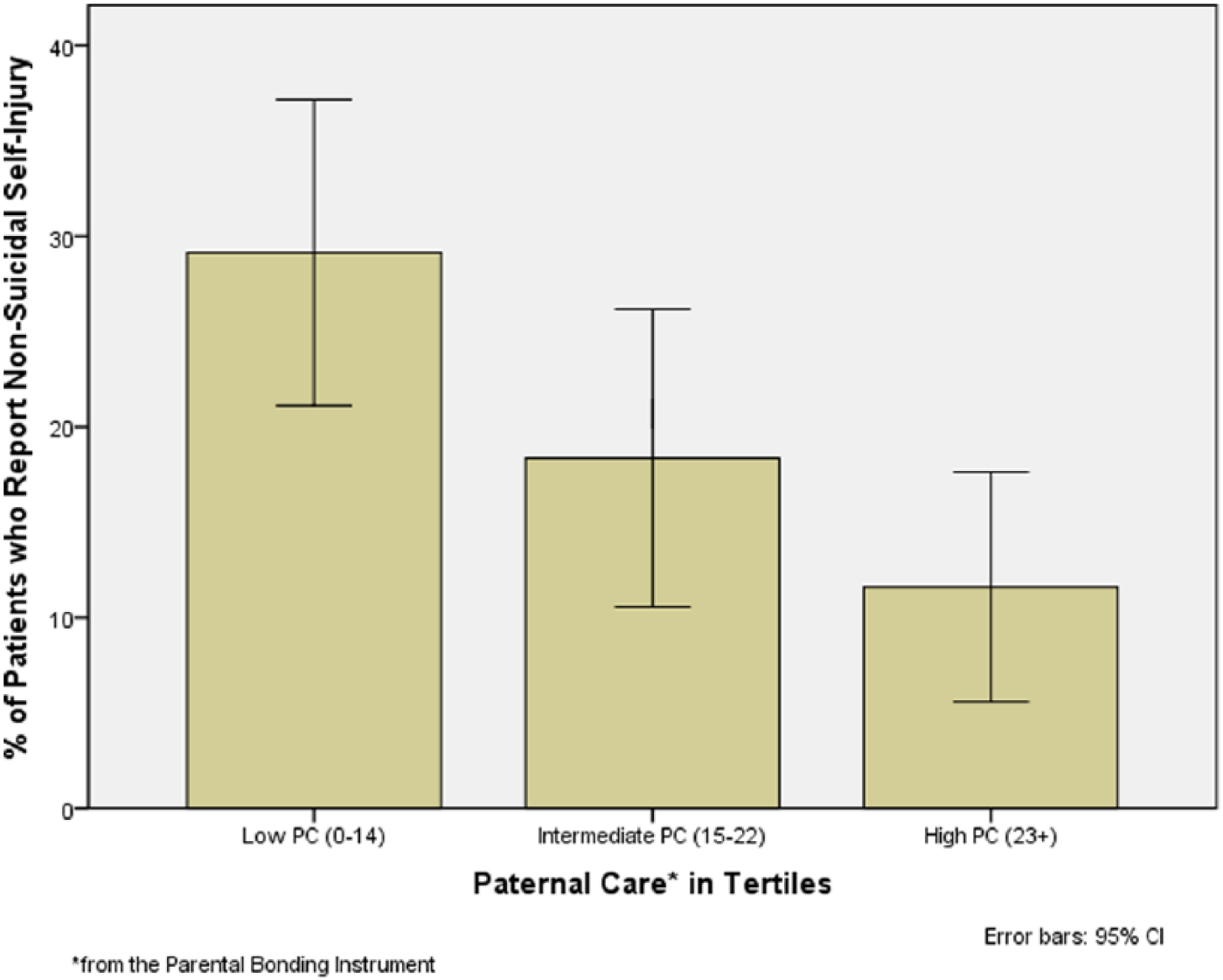
Non-suicidal self-injury by paternal care in tertiles.
Discussion
This study examined adult outpatients with depression and reported two key findings: low maternal care from one’s mother was associated with increased SA, while low paternal care was associated with higher rates of NSSI. Indeed, low parental care was the only adverse childhood experience which remained significantly associated with SA and NSSI in the multivariate models. Counter to our hypothesis, abuse, regardless of its form, was not independently associated with either behaviour after adjusting for its correlations with low maternal or paternal care.
The association between low maternal care and increased SA, as reported in this paper, aligned with the literature on adults, which also reported an association between suicidal behaviour and low parental care (Beautrais, 2002; Dale et al., 2010; Ehnvall et al., 2008; Goldney, 1985; Heider et al., 2007).
Looking specifically at the maternal care finding, a psychological model, which provides a construct for the association between low maternal care and SA, is the Interpersonal Theory of Suicide (Van Orden et al., 2010). This theory posits that the highest risk for a SA occurs when an individual experiences a sense of thwarted belongingness and perceived burdensomeness, together with hopelessness regarding these two situations (Van Orden et al., 2008). Consistent with attachment theory (Bowlby, 1977), thoughts of not belonging and being a burden to others may flourish in an adult who experienced low maternal care. Further lending support to the concept of perceived burdensomeness in relation to SA, as suggested by Van Orden et al. (2008), women with borderline personality disorder (BPD) who made a SA reported their intention was to ‘make others better off’ (Brown et al., 2002).
Another key finding was the association of low paternal care with NSSI. This original finding has some support in the literature, although more studies report on adolescent, rather than adult outcomes, and do not examine paternal care associations separate from maternal care (Wichstrøm, 2009). The study that most closely approximated the low paternal care finding reported here examined deliberate self-harm in a group of non-clinical undergraduate students. The experience of low care from both parents and paternal insecure attachment were independently associated with self-harm for women but not men in multivariate analyses (Gratz et al., 2002). Also bearing some similarity, in a study of hospitalized adolescents, emotional neglect from either parent was associated with self-mutilating behaviour (Lipschitz et al., 1999). Interestingly, overprotection was not examined as a potential risk factor in either of these studies.
This paper also reported that age of first MDE onset was associated with SA and NSSI. This finding mirrors the results found in the larger body of suicide literature (Beautrais et al., 2006). A first depressive episode occurring in childhood, adolescence or early adulthood increases the risk for a SA in comparison to a first episode occurring later in life (Nock et al., 2008). With respect to NSSI, if the self-harming behaviour is conceptualized as an attempt to regulate emotion and relieve tension in the context of early depression onset, a younger patient with depression may engage in these behaviours in the absence of more functional mood-coping strategies. Countering the typical finding that MDE onset is associated with SA and NSSI, a study examining an outpatient sample with bipolar disorder reported early depression onset predicted NSSI but not SA (Moor et al., 2012). As this paper counters the typical findings of the international literature, it may reflect a unique aspect of the population studied, or it may be identifying a distinction between SA and NSSI.
Another finding worth noting was the absence of association between depression severity and engaging in NSSI. In contrast, depression severity was strongly associated with SA. In a SA, the patient reportedly wishes to die, a desire influenced by the severity of depression or mental state at the time (Beautrais et al., 2006; Nock et al., 2008). NSSI, however, is characterized more generally as a maladaptive attempt to regulate emotion (Mangnall and Yurkovich, 2008) and, as such, may be less influenced by a particular mood state as measured by depression severity.
The last key finding in this study, that abuse, whether measured broadly as psychological, physical or sexual abuse, or specifically as CSA, was not independently associated with SA or NSSI in multivariate analyses. This result did not support our hypothesis and counters a number of other studies which report an association between abuse, SA and NSSI (Romans et al., 1995; Spinhoven et al., 2009; Ystgaard et al., 2004). It is likely that, as some researchers have suggested, abuse occurs within a context of a pre-existing low care or neglectful environment (Spinhoven et al., 2009) as evidenced by a longitudinal study of mothers at risk for parenting problems. Neglectful mothers were found to do little to protect their child from danger (Egeland & Erickson, 1987). In a review of 177 studies involving more than 65,000 participants, CSA was found to be one of several childhood risk factors for suicide and NSSI (Maniglio, 2011); however, family dysfunction (Wilkinson et al., 2011) and high-risk family environments (Kaess et al., 2013) were hypothesized to interact with CSA to increase risk.
Several factors limit the study’s findings. As the hypotheses were not a priori, the results require replication. The cross-sectional study design limits the ability to determine causality. The retrospective measures used, although found to be relatively stable over time and mood state (Wilhelm et al., 2005), are subject to memory bias, as well as potential reporting bias. A patient may be reluctant to disclose NSSI or SA in a face-to-face interview. The definition and measurement of childhood adversity, SA and NSSI differ among studies making comparisons difficult. In addition, the range of childhood adversities examined is narrower than in other studies. Given that this study reports on outpatient adults, the results may not generalize to other populations.
These findings bring to light the association between low parental care, a form of childhood adversity characterized by emotional neglect and an increased risk of SA and NSSI in adults with depression. As well, different childhood risk factors for the two behaviours are delineated. This finding was possible because the patients were asked specifically and separately about SA and NSSI. Although abuse features prominently in the research as a risk factor for SA and NSSI, it was not independently associated with either of the behaviours in this sample of adult outpatients with depression. It appears that in this sample, the quality of ongoing, intra-familial relationships had a greater impact than abuse on SA and NSSI, a hypothesis echoed by others (Dubowitz, 2006). These findings signal to clinicians the importance of asking specifically about SA and NSSI, as well as about levels of parental care in childhood. When endorsed, low parental care may be considered an important factor in contextualizing an adult patient’s depression and potential risk for suicide and NSSI.
Footnotes
Acknowledgements
The authors would like to thank the researchers, therapists and clinicians who worked on these studies. As well, we extend a special thank you to all those who participated in the research trials.
Declaration of interest
Dr Suzanne Luty received travel assistance and conference support from Eli Lilly.
Funding
This study was funded by grants from the Health Research Council of New Zealand. The Clinical Research Unit of the Department of Psychological Medicine, Christchurch, is supported by the University of Otago and the Mental Health Division of Canterbury Health. Jeanette Johnstone was supported by a scholarship from the University of Otago.