
Abstract
Purpose:
To examine whether there is an association between students self-reported suicide attempts and non-suicidal self-injury and exposure to suicidal behaviour among friends, family members or within school communities.
Methods:
A cross-sectional analysis of a nationally representative health and well-being survey of 8500 New Zealand high school students conducted from March through November 2012. Students’ self-reported suicide attempts and repeated non-suicidal self-injury was examined in relation to student reports of self-harming behaviour among friends and family as well as data from school administrators of completed suicides within the school community.
Results:
Almost 1 in 20 (4.5%) students reported a suicide attempt in the last 12 months and 7.9% reported repeated non-suicidal self-injury in the last 12 months. The risk of both suicide attempts and repeated non-suicidal self-injury was highest among females, students from homes with economic deprivation and among students reporting an episode of low mood in the previous 12 months. Students exposed to suicide attempts or completed suicide among friends and/or family members were at increased risk of reporting attempted suicide and repeated non-suicidal self-injury in the last year. There was no association between completed suicide in school community and students self-reported suicide attempts or repeated non-suicidal self-injury.
Conclusions:
Low mood and exposure to suicide attempts of friends and family members are associated with suicide attempts and repeated non-suicidal self-injury in New Zealand high school students. This research highlights importance of supporting adolescents with low mood and exposed to suicide of friends and family.
Keywords
Suicide attempts and non-suicidal self-injury (NSSI) are significant health issues among young people. Both are indicators of distress and both are risk factors for completed suicide, which is a leading cause of death among adolescents globally (Hawton et al., 2012; Ministry of Health, 2012). To date, there has been considerable research focusing on the demographic, psycho-social and environmental factors associated with suicide and self-harm behaviours in adolescents (Bridge et al., 2006; Fleming et al., 2007; Hawton et al., 2012; Miller and Eckert, 2010; Skegg, 2005). It is well understood that suicide behaviours do not occur in isolation, but rather are a behavioural response in the face of preceding risk and interactions with the physical and social environment (Bridge et al., 2006).
One important environmental risk factor is exposure to suicidal behaviours through the media. For centuries, there have been hypothesises and concerns about the contagion effects of suicide dating back to the publication of The Sorrows of Young Werther in 1774. Contagion-as-imitation (Cheng et al., 2014) suicide attempts have become known as the Werther effect (Phillips, 1985). The Werther effect is when the suicide rate increases following a highly publicized suicide attempt (Phillips, 1974) and has been demonstrated in some, but not all studies of celebrity suicides (Gould et al., 2003; Jobes et al., 1996; Stack, 2000; Sudak and Sudak, 2005). Of note, young people appear to be the most at-risk of contagion effects of suicide behaviours compared to other age groups. For example, Romer (Romer et al., 2006) looked at the influence of reports of suicide deaths in local television news or newspapers and found that it increased suicide clustering in adolescents under 25 years of age; suggestive of contagion via the media. More recent research has raised concerns around the influence of suicide websites in triggering imitation suicide behaviour in vulnerable adolescents, suggestive of yet another medium through which contagion occurs (Becker et al., 2004; Durkee et al., 2011).
There have been recent reviews that have highlighted clusters of suicide occurring within communities, institutions and families (Haw et al., 2013; Niedzwiedz et al., 2014). Young people and individuals within an institution such as a psychiatric hospital or school demonstrated more suicide clusters. Research using national mortality datasets have noted patterns suggestive of time space clustering of suicide deaths, but these are still thought to account for less than 2% of all suicide deaths (Gould et al., 1990, 1994). While contagion of suicide behaviours within the school environment remains a significant concern, there has been little systematic research apart from case studies of suicide deaths among school populations (Brent et al., 1989; Poijula et al., 2001).
However, research on this area is difficult due to a number of issues. Suicide is a rare event and distinguishing between contagion from random clustering is difficult. Furthermore, the definition of contagion has been used interchangeably with clustering in a significant portion of suicide literature and the two terms are not synonymous (Cheng et al., 2014). Cluster refers to a higher than expected incident of suicide within a defined group, geographical location or institution, whereas contagion relates to the mechanism, e.g., imitation leading to an increase in suicide and is not necessarily within a geographical location or institution. There are several other explanations, beside contagion, for clustering of suicide in setting such as schools, such as similar background demographic and risk characteristics of the school population or features of the school environment itself such as high rates of bullying (Manski, 2000). Reviewers have noted a lack of rigorous methodology employed in the majority of research in this area (Haw et al., 2013).
To better understand suicide and inform prevention efforts, researchers have turned to investigating self-harming behaviours, including suicide attempts and NSSI which are much more common among young people than completed suicide. Research has found increased risk of suicide attempts and self-harming behaviours among young people exposed to friends and family reporting deliberate self-harm (Brent et al., 1996; De Leo and Heller, 2004), and those exposed to a schoolmate’s suicide (Swanson and Colman, 2013). However, these studies have relied on student self-report and the definition of deliberate self-harm generally tends to blur the boundaries of attempted suicide. For example, the criteria used by the Child and Adolescent Self-harm in Europe group (De Leo and Heller, 2004) described deliberate self-harm as an act with a non-fatal outcome, but does not clearly delineate whether the initial act was with suicidal intention. The pathology and circumstances leading to deliberate self-harm is different to suicide. Individuals generally do not have suicide intent, and the behaviour itself serves multiple purposes (Briere and Gil, 1998; Suyemoto, 1998).
In this study, we aim to explore whether or not there is an association between exposure to suicide attempts and completed suicide among friends, family members or school communities and self-reported suicide attempts and NSSI among New Zealand high school students.
Methods
The data in this study are drawn from a nationally representative cross sectional survey of New Zealand secondary school students in 2012 (Youth’12, a part of Youth2000 a national repeated cross-sectional study of the health and wellbeing of New Zealand secondary school students). The full details and methodology of the survey are described previously (Clark et al., 2013). Students were randomly selected through a 2-stage cluster design whereby schools were first randomly selected to participate, followed by a random selection of students from participating schools. One-hundred and twenty-five composite and secondary schools out of a nationwide 493 schools were randomly selected and invited to participate in the study. Ninety-one schools (74% of invited schools) accepted the invitation and students from these schools were randomly selected from school rolls to participate. To maintain student confidentiality, in schools with more than 150 year 9 to year 13 students, 20% of the students were randomly chosen, whereas in school with less than 150 year 9 to year 13 students, 30 students were randomly selected and invited to take part in the Youth ‘12 survey. Ethics approval was gained from the University of Auckland Human Participants Ethics Committee (ref 2011/206).
In total, 12,503 students were invited to take part in the survey, of these 8500 students (68% of invited students) participated. The survey was delivered through small hand-held computers. Questions were presented on the screens and read out through a headset and students answered by touching the most suitable answer on the screen.
All schools that had taken part in Youth ‘12 were invited to participate in an additional survey of their senior management after the student survey had been conducted in 2012. A letter was sent to all principals asking for their consent to take part and who to contact in their school regarding participation. These nominated people were then contacted by phone and asked to fill in an online survey about their school. Of the 91 schools that participated in Youth ‘12, 1 school had subsequently closed and 80 schools agreed to take part in the senior management survey.
Demographic variables
Students self-reported age and sex. Ethnicity was determined by responses to a standard ethnicity question used in the New Zealand census. Students were able to choose from a list of 23 ethnicities as per the census. For analysis, students were categorised into one of six ethnic groups as per the New Zealand ethnicity prioritization method as: Maori, Pacific Island, Asian, other and Europeans.
Household socio-economic deprivation
The household level of socioeconomic deprivation was assessed through 9 indicators of socioeconomic deprivation: no car, no phone, no computer, their parent/s worry about not having enough money for food, more than two people sharing a bedroom, no holidays with their families, moving home more than twice that year, garages or living rooms used as bedrooms and no parent at home with employment. Students who reported at least 2 indicators of socioeconomic deprivation were categorised as being from homes with high levels of socioeconomic deprivation (Denny et al., 2016).
Suicide attempts and repeated NSSI
NSSI behaviours were assessed by the question, ‘During the last 12 months, have you deliberately hurt yourself or done anything you knew might have harmed you (but not kill you?)’, with response options, ‘Not at all’, ‘Yes – once’, ‘yes – two times’, ‘yes – 3–5 times’, ‘more than 5 times’. Students who reported self-harm 3 or more times were classified in the repeated NSSI group.
Suicide attempt was assessed by the question, ‘During the last 12 months have you tried to kill yourself (attempted suicide)?’. Students who reported ‘once or twice’ or ‘three or more times’ were classified having attempted suicide in the last 12 months.
Episode of low mood
Students were asked, ‘During the past 12 months was there ever a time you felt sad, blue or depressed for two weeks or more in a row?’. Students who responded ‘Yes’ were classified as having an episode of low mood.
Suicide attempts by family and peers
Exposure to the suicide attempts of close family and friends were assessed with two questions. ‘Has anyone in your family/whanau ever tried to kill themselves (attempted suicide)?’ and ‘Have any of your friends ever tried to kill themselves (attempted suicide)?’, with response options ‘Yes, within the last 12 months’, ‘Yes, more than 12 months ago’ and ‘no’.
School level measures
Traumatic events
Following the completion of the student survey, a questionnaire was sent round to all school principals and senior management asking about a range of school climate variables. Respondents in this survey were asked ‘Has your school experienced any sudden or unexpected deaths of staff members, students or ex-students in the past 12 months?’. Those with an affirmative response were asked ‘How many sudden or unexpected deaths has your school experienced this year?’ for ‘students’, ‘teachers’ and ‘ex-students’ and ‘How did these deaths occur?’ with response options that included suicide.
Analyses
Bivariate analyses were conducted using the survey procedures in the SAS software (version 9.2, SAS Institute, Cary, NC, 2008) to account for the clustering and weighting of the data. Prevalence estimates were derived using bivariate analyses to examine the simple associations between the demographic variables and self-harm and suicide behaviours. Generalized linear models accounting for nesting of students within schools were used to estimate the association between suicide attempts/self-harming behaviours and student and school-level variables. Analyses were undertaken to explore the amount of variation at the school-level compared to the individual-level using the intra-class correlation (ICC). This was calculated by estimating random intercept models for self-harming behaviours and suicide attempts with and without individual-level covariates. Generalized estimation techniques used maximum likelihood with adaptive Gauss-Hermite quadrature rule, using the GLIMMIX procedure in SAS version 9.2 (SAS Institute, Cary, NC). Differences were considered statistically significant at the p < 0.05 level.
Results
Overall, 4.5% of students attempted suicide at least once in the last 12 months (Table 1). Approximately 70% of these students had made one or two suicide attempts and 30% had made 3 or more suicide attempts in the previous 12 months. Females were twice as likely to attempt suicide compared with males. New Zealand European students were less likely to attempt suicide compared to students from Maori, Pacific, Asian or Other ethnicities (p < 0.01). The odds of suicide attempt were two times higher for Pacific students than for NZ European students. Students from homes experiencing economic deprivation were almost three times more likely to report a suicide attempt compared to peers from homes without socioeconomic deprivation. Age was not significantly associated with rates of suicide attempts.
Demographic variables and suicide attempt and repeated NSSI (n = 8500).
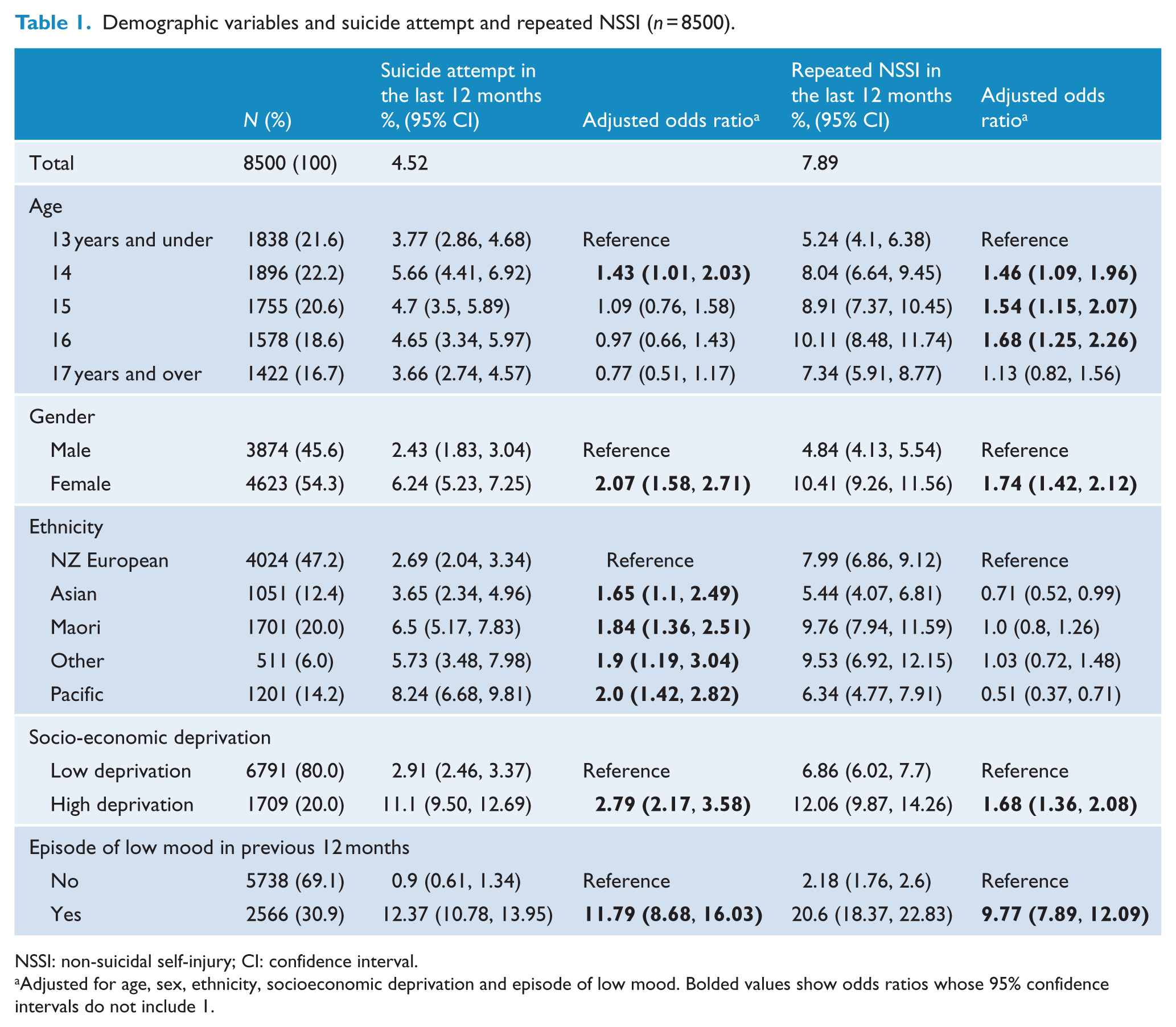
NSSI: non-suicidal self-injury; CI: confidence interval.
Adjusted for age, sex, ethnicity, socioeconomic deprivation and episode of low mood. Bolded values show odds ratios whose 95% confidence intervals do not include 1.
Almost one-quarter (24%) of students had deliberately hurt themselves, without suicide ideation, in the previous 12 months. Of these, 50.7% reported one episode of self-injury, 16.5% reported two episodes and 32.8% reported 3 or more episodes in the previous 12 months. Sixteen year-old adolescents had a significantly higher prevalence of repeated (3 or more episodes) NSSI compared to students aged 13 or under. Females were more likely to report repeated self-harm than males. Asian and Pacific students were less likely to report repeated self-harm behaviours compared to European students. Students from homes with high socioeconomic deprivation were almost twice as likely to report repeated NSSI compared to students from homes not experiencing socioeconomic deprivation.
After adjusting for confounding by socio-demographic variables, students reporting an episode of low mood in the previous 12 months were much more likely to report suicide attempts and repeated NSSI compared to students who did not report an episode of low mood.
The intraclass correlation for suicide attempts was 7%, suggesting that 7% of the variation in suicide attempts was between schools. Once age, sex, ethnicity, socio-economic deprivation variables and episode of low mood were controlled for the intraclass correlation dropped to 1.2%. This suggests that most of the observed variation between schools is due to demographic differences between schools influencing suicide attempts. The intraclass correlation for repeated self-harm behaviour was 2.9% which reduced to 1.6% once the same covariates were added to the model.
Figure 1 demonstrates the relationship between reported episode of low mood, repeated NSSI and suicide attempts in a venn diagram. There is significant overlap between episodes of low mood and both repeated NSSI and suicide attempts and also between repeated NSSI and suicide attempts. Overall, 2603 students (31.1%) reported an episode of low mood in the last 12 months. Of these students, 128 (4.9%) had attempted suicide without repeated NSSI, 191 (7.3%) attempted suicide and repeated NSSI and 345 (13.3%) students reported only repeated NSSI with their low mood, but no suicide attempts. The remaining 1939 (74%) students reported an episode of low mood without reporting repeated NSSI or suicide attempt. A small proportion of students who reported a suicide attempt (n = 48) or engaged in repeated NSSI (n = 188) or both (n = 11) did not report an episode of low mood in the last 12 months.
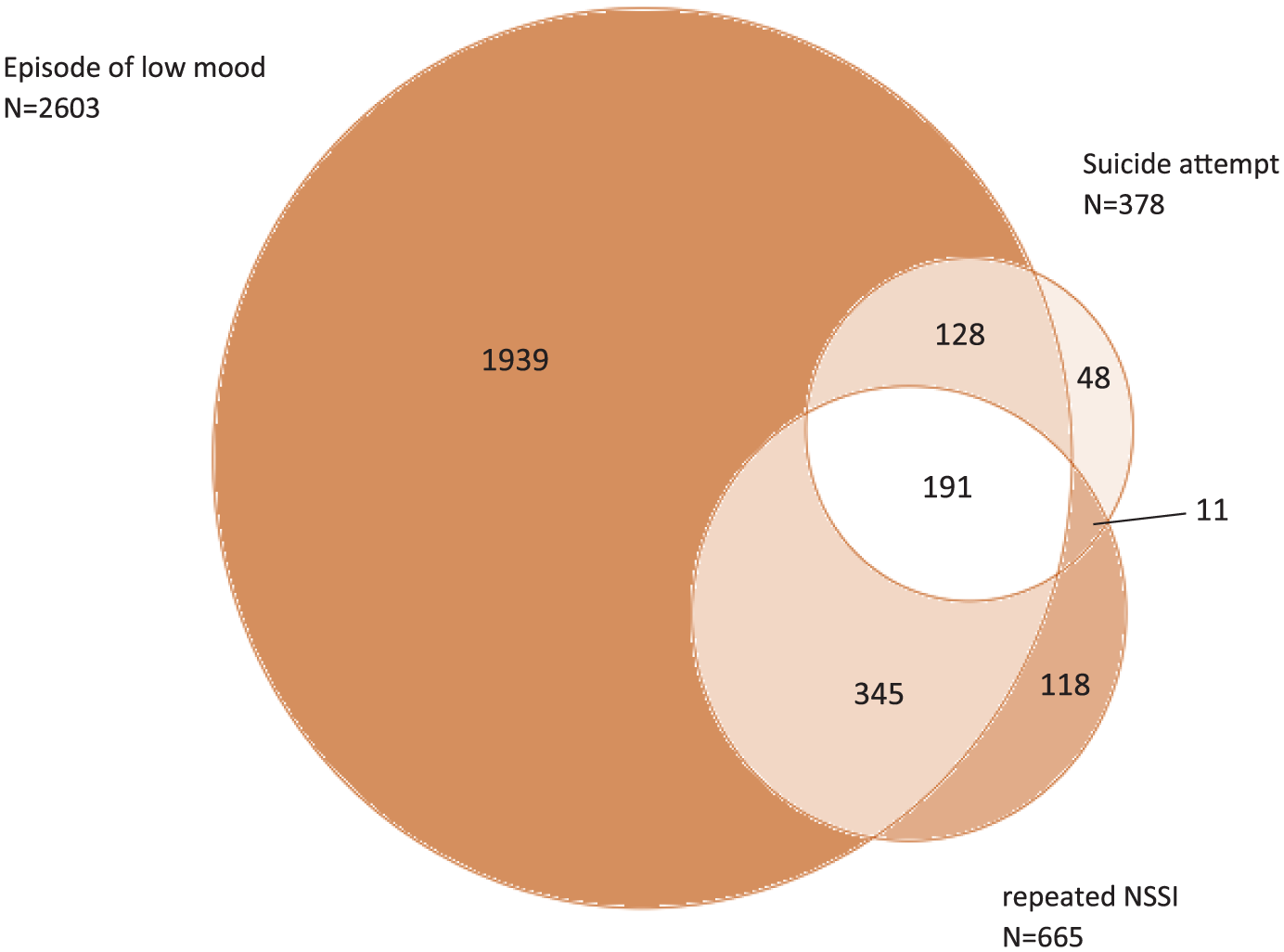
Venn diagram showing the relationship between low mood, suicide attempt and repeated NSSI 118.
Exposure rates to suicide attempts and completed suicide of family members and friends ranged from 3.3% to 15.9% (Table 2). Students exposed to a suicide attempt of a family member within the last year or more than 12 months ago were more likely to attempt suicide in the last 12 months compared to students not exposed to a suicide attempt by a family member. Students were also more likely to attempt suicide if exposed to a completed suicide of a family member within the last year or more than a year ago.
Individual risk factors and suicide attempt and repeated NSSI (n = 8500).
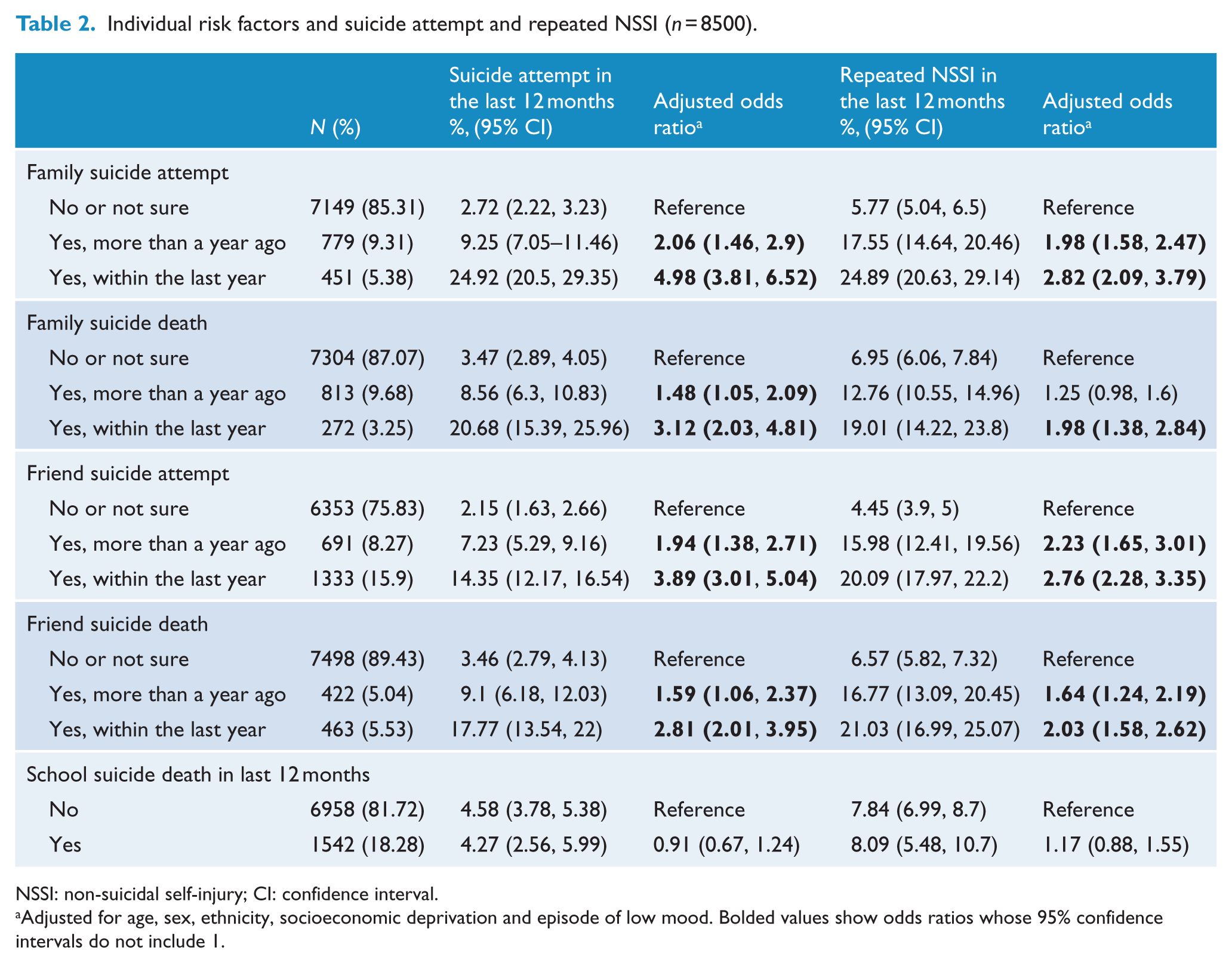
NSSI: non-suicidal self-injury; CI: confidence interval.
Adjusted for age, sex, ethnicity, socioeconomic deprivation and episode of low mood. Bolded values show odds ratios whose 95% confidence intervals do not include 1.
Exposure to the suicide attempt of a family member within the last year or more than a year ago also increased the odds of reporting repeated NSSI. If a family member completed suicide, the odds of frequent self-injurious behaviours were increased in students only exposed within the last year. The odds of a suicide attempt also increased with exposure to a friend’s suicide attempt or completing within the last year or more than a year ago. A similar increase in odds ratio was seen with repeated NSSI when exposed to a friend’s suicide attempt or completed suicide within the last year or more than a year ago. In contrast, while 18.3% of students were in schools with a suicide death in previous 12 months, this did not significantly increase the rates of suicide attempts or repeated NSSI.
Discussion
In this nationwide representative survey of secondary school students in New Zealand conducted in 2012, approximately 1 in 20 students reported a suicide attempt in the last 12 months and 1 in 13 reported more than 3 episodes of self-harm, in the last 12 months.
We found evidence of increased risk of NSSI and suicide attempts by students exposed to suicide deaths or suicide attempts by their friends or families. In our study, exposure to friends or family dying by suicide or attempting suicide were relatively common ranging from 3.3% to 15.9%. We found that exposure to both fatal and non-fatal suicidal behaviour among friends or family increased an individuals’ risk of suicide and repeated self-harm, especially those exposed within the previous 12 months. This is in keeping with research in Canada (Swanson and Colman, 2013), Ireland (McMahon et al., 2013) and the United States (Feigelman and Gorman, 2008) that has shown a link between exposure to suicidal behaviours of close friends and/or relations and increased risk of suicidal ideation, suicide attempts or deaths by suicide.
In contrast, we found little evidence of contagion of NSSI or suicide attempts within the school community. In particular, there was little evidence of clustering of suicide attempts within schools and no association between a suicide death in the school community and increased risk of suicide attempts among students. Clustering of suicide attempts was 7% at the school-level, but dropped to 1% once covariates were added to the model. This suggests that schools with high rates of suicide attempts among students is more to do with the background demographic characteristics of the school’s student population rather than the school context and may explain how clusters of suicide behaviours in schools may be interpreted as contagion between students (Manski, 2000). Our findings support a social learning theory mechanism of contagion of self-harm behaviours as students appeared to be more influenced by friends or family members as opposed to students within the school environment. It remains possible that other shared factors such as abuse could explain the relationship between family members and NSSI and suicide attempts. However, this would not explain the relationship with peers and the contagion of self-harming behaviours.
In keeping with past research, students reporting an episode of low mood had the highest risk of both repeated NSSI and suicide attempts (Hawton et al., 2012). Female students and students from homes with socio-economic deprivation were at increased risk of suicide attempts and repeated NSSI, but their impact was much less compared with the effects of low mood. Pasifika students and Maori students reported the highest rates of suicide attempts compared with other ethnic groups. Once age, gender, socioeconomic deprivation and low mood were taken into consideration in multivariate models, the magnitude of ethnic differences were attenuated. This suggests that some of these ethnic differences may be explained in part by the disproportionate socioeconomic deprivation experienced by Pasifika students and Maori students. This highlights an important need to also look at individual level demographic factors in targeting interventions to reduce the overall risk of suicidal behaviours in New Zealand adolescents. Of note, Pasifika students were the least likely to engage in repeated self-harm but were the most likely to have reported suicide attempt in the preceding 12 months. The reasons for this divergence are unclear, but may reflect cultural norms around accepted ways of coping of distress.
There are several limitations to this study. First, the proportion of students reporting repeated NSSI were slightly lower than what has recently been reported in literature (Hawton et al., 2012) and highlights the variation in definitions in this field. Our criteria specifically excluded actions students knew would have a fatal consequence. Most previous literature has defined NSSI behaviour as one or more episodes in a 12 months period. Hawton (Hawton et al., 2012) in his review found that there was approximately a 50% repetition rate of NSSI meaning that only half were repeat self-harmers. This likely explains our lower rate of repeated self-harm behaviour. Second, the data are from a cross-sectional data set, making it difficult to interpret any causality. It is possible that students who are injuring themselves or attempting suicide are more likely to recall friend or family member’s suicidal behaviours. Conversely students may underreport family suicides because of the stigma associated with mental health problems in society. Longitudinal prospective data would help elucidate this relationship. The survey only included students enrolled at school and at school on the day of the survey. While the response rate of students who took part in this survey were reasonable, adolescents who are most at risk might be underrepresented as absenteeism is linked with a myriad of social and psychiatric factors (Ingul et al., 2012). Finally, it remains difficult to rule out if the increased risk of repeated self-harm behaviours and suicide attempts are due to contagion or other shared events such as trauma that would have directly caused the increased risk of suicide attempts or repeated NSSI.
In summary, the overall rates of suicide attempts and repeated self-harm in New Zealand school students were common with female sex, ethnicity (Maori and Pacific), socioeconomic deprivation and, particularly with low mood being significant risk factors. There was evidence to suggest contagion effects of suicide behaviours within peer groups and family networks as additional significant risks for students. These findings highlight the significant impact exposure to suicide among close friends and family may have on an adolescent’s mental health well-being, implying that there should be a heightened alert especially within the first year after exposure. In contrast, there was little evidence of contagion of a suicide death within the school environment. Recent discussions in this journal (Krysinska et al., 2016) demonstrate the importance of systematic strategies to reduce suicide, including increasing access to psychosocial interventions. This ideally would be done through school based health services and to follow best practice guidelines (Carter et al., 2016).
Footnotes
Acknowledgements
Thanks to all the students, staff and schools who participated in the survey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The Youth’12 project was funded by the Ministries of Youth Development, Social Development, Health, Education and Justice; the Department of Labour; Families Commission; and the Alcohol Advisory Council of New Zealand. We would also like to acknowledge the support of Toshiba (Australia) Pty Limited.
Implications and Contribution
Adolescent suicide and repeated self-harm behaviours are a significant problem for the individual and their families. The study highlights extra support may be required after a suicide attempt of a friend or family member as it is associated with increased suicide and self-harm behaviour in the adolescent.