
Abstract
Objectives:
This study investigated associations between sexual orientation and measures of suicidality and non-suicidal self-injury in Australian adults. Previous studies of sexual orientation and suicidality have been limited by unclear conceptualisations of suicidal intent, failure to differentiate between homosexuality and bisexuality, inattention to gender differences and use of convenience-based samples.
Methods:
A large (N = 10,531) representative national sample of Australian adults was used to investigate associations between sexual orientation (heterosexual, homosexual, bisexual) and (1) suicidal ideation, (2) attempted suicide and (3) non-suicidal self-injury, for males and females separately, in a series of sequentially adjusted logistic regression models.
Results:
Sexual minority participants were at greater risk of suicidality and self-injury than heterosexuals, after adjusting for age and other covariates, with patterns of risk differing by sexual orientation and gender. Compared with their heterosexual counterparts, gay men, but not bisexual men, were more likely to report suicidal ideation (odds ratio = 3.05, 95% confidence interval = [1.65, 5.60]) and suicide attempts (odds ratio = 4.16, confidence interval = [2.18, 7.93]). Bisexual women, but not lesbian women, were more likely to report suicidal ideation (odds ratio = 4.40, confidence interval = [3.00, 6.37]) and suicide attempts (odds ratio = 4.46, confidence interval = [2.41, 8.24]). Neither bisexual nor gay men were more likely than heterosexual men to report self-injury. However, bisexual women, but not lesbian women, were more likely than heterosexual women to report self-injury (odds ratio = 19.59, confidence interval = [9.05, 42.40]). Overall, bisexual females were at greatest risk of suicidality and self-injury.
Conclusion:
Clinicians working with sexual minority populations are encouraged to openly discuss suicidal and self-injurious thoughts and behaviours with their clients and may consider using therapeutic strategies to reduce internalised stigma and enhance personal and social resources.
Introduction
Individuals who do not identify as heterosexual are at increased risk of suicidal ideation and attempts relative to their heterosexual counterparts (Balsam et al., 2005; Cochran and Mays, 2000a). In a large systematic review, King et al. (2008) found that lesbian, gay and bisexual people aged 12 years and above had a greater than twofold excess risk of lifetime suicide attempts (risk ratio = 2.47, 95% confidence interval [CI] = [1.87, 3.28]). Contemporary theorists and researchers attribute most, if not all, of this risk to the stigma suffered by minority sexual groups (Herek and Garnets, 2007), conceptualised via the minority stress model (Meyer, 2003) (Figure 1). This is supported by results from a population-based national survey in the United States; the correlation between mental health problems and sexual orientation was largely explained by non-heterosexuals’ experience with discrimination, with differences on mental health measures reduced following statistical adjustment for measures of discrimination (Mays and Cochran, 2001).
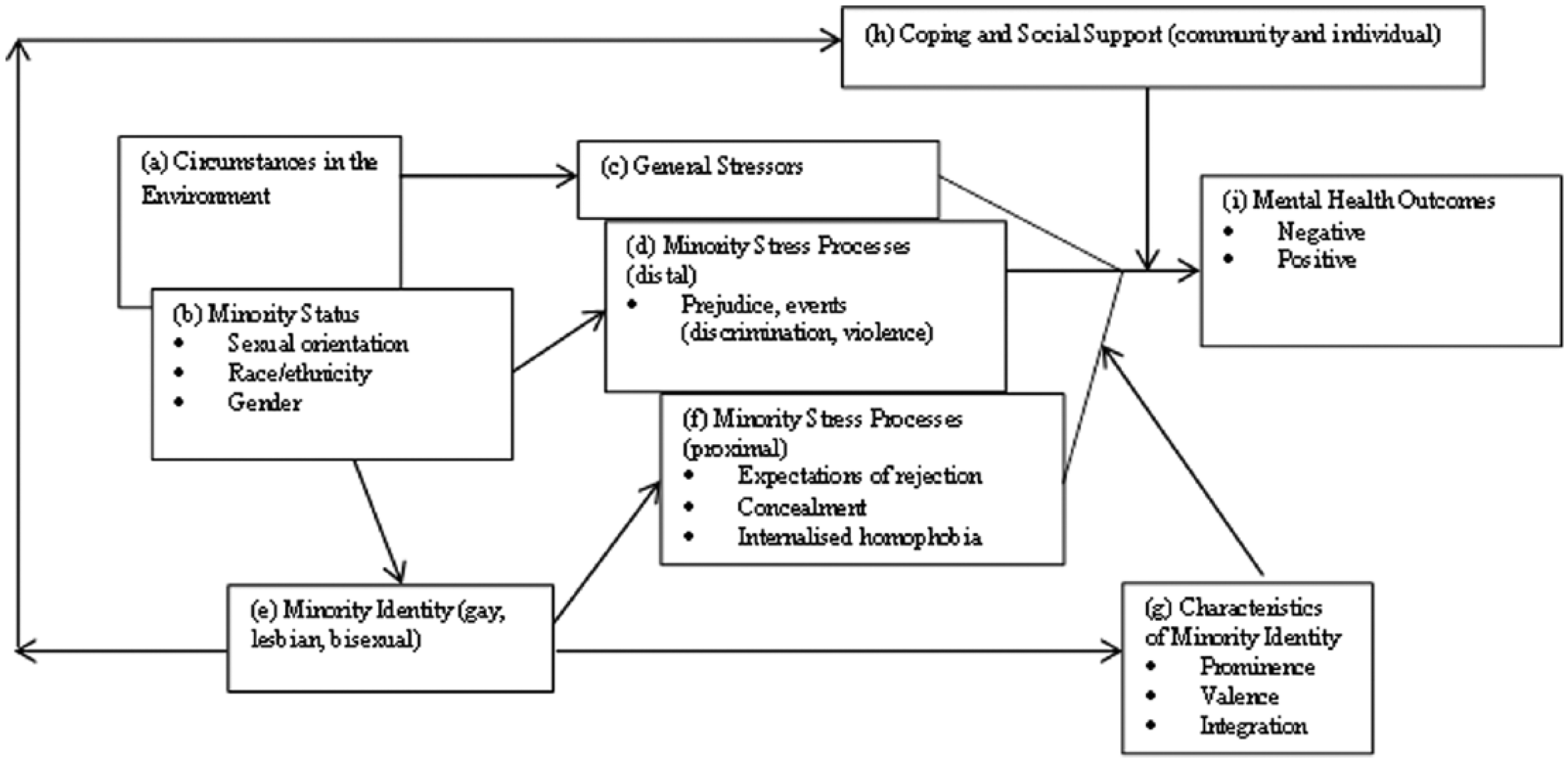
Minority stress processes in lesbian, gay and bisexual populations.
Non-heterosexual orientation has also been associated with increased risk of non-suicidal self-injury (NSSI) (Deliberto and Nock, 2008; Gollust et al., 2008), defined as the deliberate, self-inflicted destruction of body tissue resulting in immediate damage, without suicidal intent and for purposes not culturally sanctioned (Nixon et al., 2008). Common NSSI methods include skin cutting, scratching and self-battery (Nock, 2010). NSSI is a significant problem worldwide; a recent meta-analysis of 119 studies of non-clinical samples reporting 128 NSSI prevalence estimates from 18 countries calculated adjusted pooled lifetime prevalence estimates at 17.2% (95% CI = [8.0, 26.3]) among adolescents (studies where the mean age was between 10–17 years), 13.4% [4.5, 22.3] among young adults (studies where the mean age was between 18 and 24 years) and 5.5% [1.7, 16.3] among adults (studies where the mean age was ⩾25 years) (Swannell et al., 2014). In Australia, population-based figures indicate that 8.1% of Australians have engaged in at least one lifetime episode of NSSI (Martin et al., 2010). Although NSSI and suicidality differ in lethality, motivations and patterns, requiring different management and treatment strategies (Messer and Fremouw, 2008), they are commonly comorbid (Andover et al., 2005). Compared to sexual orientation and suicidality, the link between sexual orientation and NSSI has received little research interest. There is some evidence, though, that the link can be partly attributed to sexual stigma (Alexander and Clare, 2004).
Early research on the association between sexual orientation and self-destructive behaviour, while informative, suffered from a number of flaws. Most studies comprised convenience samples of volunteers, frequently recruited through help-seeking organisations (e.g. individuals receiving counselling) and community activities (e.g. gay/lesbian festivals). While recruiting in this manner is an effective way of increasing sample size, it also leads to potentially biased samples (Cochran and Mays, 2000a). More recent studies have attempted to reduce such bias (Cochran and Mays, 2006), and a substantial number of studies now comprise samples representative of underlying populations (for a review and meta-analysis, see Plöderl et al., 2013), although none in the Australian context.
Related to difficulties recruiting large enough samples, most previous research has combined homosexual and bisexual participants into one category and compared them with heterosexual participants. Similarly, many studies combine males and females into one category, obscuring differences across gender. This lack of differentiation between homosexuality and bisexuality and between males and females is problematic given inequalities in social understanding and acceptance between homosexual and bisexual individuals (Bostwick, 2012) and the power imbalance across gender (Rudman and Glick, 2008). Both social acceptance and power imbalance can influence the risk of suicidality and NSSI.
Accordingly, this study aimed to measure associations between sexual orientation and suicidal ideation, suicide attempts and NSSI in a large nationally representative sample in Australia. While previous research conducted in Australia has looked at associations between suicidality and sexual orientation (Jorm et al., 2002), this is the first Australian study to examine associations between NSSI and sexual orientation.
Method
Data source
Data were from the Australian National Epidemiological Study of Self-Injury (ANESSI), a national telephone survey of 12,006 Australians aged 10–100 years conducted in Australia in 2008. An overview of results and the study methodology have been published elsewhere (Martin et al., 2010). Only adults (age range 18–100 years, M = 52.1, standard deviation [SD] = 16.9) were included in this study (N = 10,531) to minimise the contribution of bias resulting from psychological distress due to the ‘coming out’ process, which more often occurs during adolescence (Herrell et al., 1999), and also because adolescence is characterised by self-identification, which includes exploring sexual orientation (Perrin, 2002).
Measures
For sexual orientation, participants were asked ‘which of these best describes you: heterosexual (straight), homosexual (gay/lesbian), bisexual (bi), or other?’ NSSI questions were based on previous research completed by the investigators (Hasking et al., 2008, 2010; Swannell et al., 2008) and existing NSSI survey instruments (Functional Assessment of Self-Injury, Self-Harm Behaviour Questionnaire, Deliberate Self-Harm Interview). Participants were first introduced to NSSI questions with the following statement: ‘The following questions are about self-injury. Self injury means deliberately hurting yourself or any part of your body without meaning to kill yourself. Do you understand this definition?’ followed by ‘Remember that if you feel uncomfortable you don’t have to answer these questions’. If participants understood the definition and did not object to continuing the interview, they were asked, ‘Over the past four weeks, have you self-injured?’ If participants answered ‘no’ to the 4-week NSSI, they were asked, ‘Have you ever, in your lifetime, self-injured?’ In participants who responded affirmatively, an additional question ‘When was the last time you self-injured?’ was also asked, enabling the identification of those participants who had self-injured in the period 1–12 months prior to the interview. Those who responded affirmatively were asked additional details about their NSSI (not relevant to this study). Although overdosing is a legitimate method of NSSI, because it is most commonly seen in suicide attempts, participants who reported overdosing as their only method of NSSI were not counted as self-injurers in an attempt to maintain strict delineation between suicidal and non-suicidal behaviours.
Suicidal ideation was measured via four questions from the General Health Questionnaire, 28-item version (GHQ-28) (Goldberg and Hillier, 1979), and prefaced by the phrase ‘Now I’m going to ask you some questions about when life may not be worth living’. Questions were as follows:
Over the past few weeks, have you … (a) felt that life isn’t worth living?; (b) thought of the possibility that you might do away with yourself?; (c) found yourself wishing you were dead and away from it all?; (d) found the idea of taking your own life kept coming into your mind?
previously shown to predict suicidality (Watson et al., 2001). These questions were followed by a specific question about suicide attempts: ‘Have you ever tried to kill yourself?’ Those responding affirmatively to this question were asked additional details about their attempt(s) (not included in this study).
Age group was specified as a categorical covariate, due to the strong negative correlation between NSSI prevalence and age (Kerr et al., 2010), and coded into five age groups (18–24, 25–34, 35–44, 45–54 and ⩾55 years). Psychological distress was also specified as a categorical covariate (high, mild, low distress) to evaluate the association between sexual orientation and suicidality/NSSI independent of general psychological distress. Psychological distress was measured with the General Health Questionnaire, 12 item version (GHQ-12) (Goldberg et al., 1997), a screening device used extensively worldwide in epidemiological studies (Puustinen et al., 2011). None of the four items from the GHQ-28 used to measure suicidal ideation were in the GHQ-12 used to measure psychological distress. Additional covariates included risky alcohol use and a history of illicit drug use. Risky alcohol use was defined as drinking more than seven standard drinks for males, or five standard drinks for females, more than once a week. A history of illicit drug was defined as use of at least one of the following drugs more than 10 times in a lifetime: cannabis, amphetamines, cocaine, ecstasy, inhalants, opioids, hallucinogens or any other drug reported by the respondent.
Data analysis
Numbers of participants identifying as heterosexual, homosexual and bisexual, and numbers of participants reporting 4-week suicidal ideation, lifetime suicide attempts and 12-month NSSI were expressed in proportions of the population, and stratified by gender. Survey weights (by age, gender and state for the Australian population, based on the 2006 census) were used in the estimation of prevalence estimates. Logistic regression models were used to investigate associations between sexual orientation and suicidal ideation, suicide attempts and NSSI. Preliminary analysis of the interaction between gender and sexual orientation was significant for suicidal ideation (Wald = 11.15, df = 2, p = 0.004), suicide attempts (Wald = 12.14, df = 2, p = 0.002) and NSSI (Wald = 15.74, df = 2, p < 0.001). All subsequent regression models considered males and females separately. Additional models sequentially adjusted for age and psychological distress, alcohol and illicit drug use as covariates. Age was included as a covariate due to the known association with the dependent variables, and psychological distress, alcohol and illicit drug use were added as covariates to determine possible effects on associations between sexual orientation, suicidality and NSSI.
Results
Overall, more males (1.8%) than females (0.8%) identified as homosexual, and more females (1.7%) than males (1.2%) identified as bisexual (χ2 = 19.50, p < 0.001) (Table 1). Across all sexual orientations, there was greater overlap among females reporting both suicide attempts and NSSI (39.7% of females reporting NSSI also reported at least one suicide attempt) compared with males (24.0% of males reporting NSSI also reporting at least one suicide attempt). Within the sexual orientation variable, bisexuality had the greatest overlap of NSSI and suicide attempts (53.3% of bisexual participants reporting NSSI also reported at least one suicide attempt). Across all sexual orientations and across gender, a general pattern emerged where the percentage of those reporting NSSI who also reported at least one suicide attempt was greater than the percentage of those reporting at least one suicide attempt who also reported NSSI.
Counts, proportions and 95% confidence intervals (CI) for sexual orientation, suicidal ideation, suicide attempt and non-suicidal self-injury (NSSI).
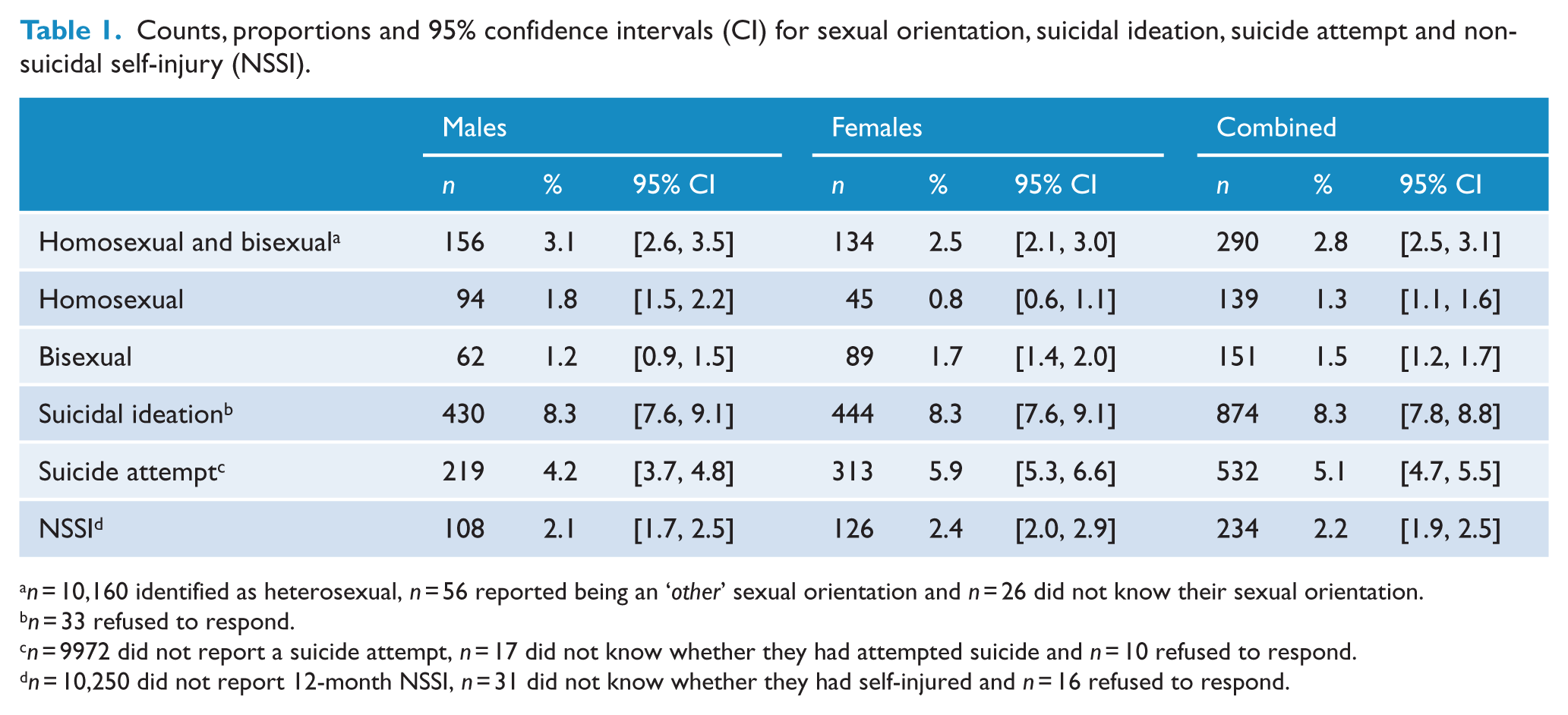
n = 10,160 identified as heterosexual, n = 56 reported being an ‘other’ sexual orientation and n = 26 did not know their sexual orientation.
n = 33 refused to respond.
n = 9972 did not report a suicide attempt, n = 17 did not know whether they had attempted suicide and n = 10 refused to respond.
n = 10,250 did not report 12-month NSSI, n = 31 did not know whether they had self-injured and n = 16 refused to respond.
Homosexuality and bisexuality as a combined category was associated with higher suicidal ideation, suicide attempts and NSSI for males and females after adjusting for age (Table 2). For males, odds were greatest for suicide attempts (odds ratio [OR] = 3.61, 95% CI = [2.21, 5.89], p < 0.001), while for females, odds were greatest for NSSI (OR = 16.45, 95% CI = [10.11, 26.79], p < 0.001). Further adjustment for age did not substantially affect the magnitude of the effect size; however, additional adjustment for psychological distress and alcohol and illicit drug use attenuated OR estimates towards the null value.
Odds of suicidal ideation, suicide attempt and non-suicidal self-injury (NSSI) by sexual orientation, males and females.
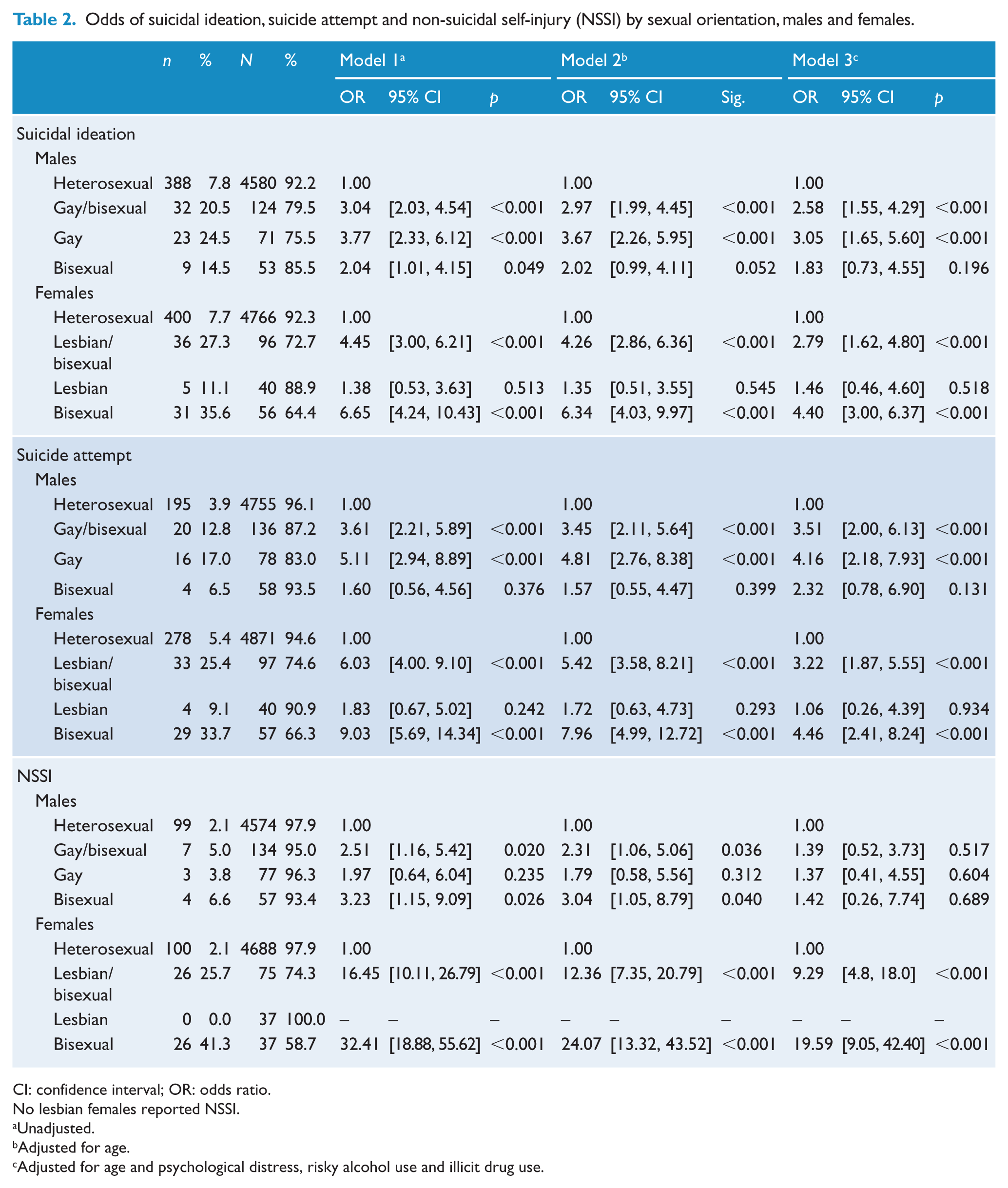
CI: confidence interval; OR: odds ratio.
No lesbian females reported NSSI.
Unadjusted.
Adjusted for age.
Adjusted for age and psychological distress, risky alcohol use and illicit drug use.
In analyses considering bisexuality and homosexuality separately, gay males, but not bisexual males, were more likely to report both suicidal ideation (OR = 3.77, 95% CI = [2.33, 6.12], p < 0.001) and suicide attempts (OR = 5.11, 95% CI = [2.94, 8.89], p < 0.001). Conversely, bisexual women, but not lesbian women, were more likely to report both suicidal ideation (OR = 6.65, 95% CI = [4.24, 10.43], p < 0.001) and suicide attempts (OR = 9.03, 95% CI = [5.69, 14.34], p < 0.001). ORs decreased when age, psychological distress, alcohol and illicit drug use were added to the models but differences remained statistically significant.
The pattern of results was different for NSSI (Table 2). Associations were not as strong for gay males who engaged in NSSI compared to heterosexual males (OR = 1.97, 95% CI = [0.64, 6.04], p = 0.235), and no lesbian females reported engaging in NSSI (Table 2). The association between NSSI and male bisexuality (OR = 3.23, 95% CI = [1.15, 9.09], p = 0.026) did not change substantially following adjustment for age (OR = 3.04, 95% CI = [1.05, 8.79], p = 0.040) and was attenuated after further adjustment for other covariates (OR = 1.42, 95% CI = [0.26, 7.74], p = 0.689). Odds of bisexual females engaging in NSSI were very high (OR = 32.41, 95% CI = [18.88, 55.62], p < 0.001) and remained high after adjusting for age, psychological distress, alcohol and illicit drug use.
Discussion
Findings from this study suggest that Australian adults who identify as either homosexual or bisexual have a higher risk of suicidal ideation, suicide attempts and NSSI compared to those who identify as heterosexual. However, important differences emerge when males and females, and homosexuality and bisexuality, are considered separately. Gay males were at higher risk of suicidal ideation and attempts, but not NSSI. Bisexual males were at moderate risk of NSSI, but this risk was reduced after adjustment for psychological distress. Compared to heterosexual females, lesbian females were not at greater risk of suicidality or NSSI, but bisexuality among females was associated with a higher risk of suicidality and a very high risk of NSSI. For both genders, bisexuality was associated with a greater risk of NSSI compared with homosexuality; this was a very strong association among bisexual females that was not substantially affected by adjustment for psychological distress.
More males than females identified as homosexual, and more females than males identified as bisexual. These results are consistent with results from another Australian telephone interview study which found 1.6% men identified as gay and 0.9% as bisexual, while 0.8% women identified as lesbian and 1.4% as bisexual (Grulich et al., 2003) and a large American survey (3.5% gay, 1.8% lesbian, 0.7% bisexual men, 1.1% bisexual women) (Conron et al., 2010).
Higher risk of suicidality and NSSI in homosexual and bisexual groups compared to heterosexual groups is also consistent with the minority stress model, which suggests that sexual minority group members are at greater risk of poorer mental health outcomes, suicidality and NSSI because they face unique, chronic stress due to sexual stigma, on top of routine stressors faced by members of nonminority groups (Meyer, 2003). These stressors are likely to also be associated with mental disorders, which are key antecedents to suicidal behaviour, particularly affective disorders (including depression), substance use disorders, anxiety disorders and schizophrenia (Ferrari et al., 2014; Li et al., 2011; Mann et al., 2005). Being a member of a sexual orientation minority group directly increases stress through prejudice, discrimination and violence, while expectations of rejection, concealment and internalised homophobia develop in response to minority identification and add to the unique stress experienced by sexual minorities (Figure 1). Additional aspects of Meyer’s (2003) model include the buffering effects of coping and social support (both individual and community), as well as characteristics of minority identity (i.e. how central to one’s identity the minority status is, valence and integration), which can either exacerbate or attenuate stress.
Results highlight the importance of considering gay males, lesbian females, bisexual males and bisexual females separately, taking them into account as distinct groups, since risk was not uniform across these categories. Furthermore, results suggest the importance of considering suicidal intent when examining self-harming behaviours, as the pattern of risk of NSSI differed from the pattern of risk of suicidality. The two groups at highest risk were gay males and bisexual females. Gay males were about three times more likely to have experienced suicidal ideation and almost four times more likely to have attempted suicide in their lifetime. Bisexual females were almost five times more likely to have experienced suicidal ideation, over six times more likely to have attempted suicide and almost 21 times more likely to have engaged in NSSI.
While any person belonging to a sexual minority may be subject to stigma and discrimination, thus increasing the risk of suicidality/NSSI, our results suggest that gay males and bisexual females are at particular risk. Evidence suggests that gay males experience greater sexual prejudice than lesbians, and this prejudice originates from heterosexual males, whose attitudes towards gay men are more hostile than their attitudes towards lesbians (Herek, 2000). In contrast, heterosexual women’s attitudes are not consistently different towards lesbians or gay men and are comparatively more positive (Kite and Whitley, 1996).
The greater risk of suicidality/NSSI among bisexual females compared with lesbian females could be due to bisexuality still being questioned as an authentic sexual orientation, discriminated against by both heterosexuals and homosexuals (Israel and Mohr, 2004) and resulting in increased stigma, greater invisibility and lack of within-group support. Bisexuality is frequently perceived as a transitional ‘phase’ on the way to being lesbian or gay, a safe label for individuals who lack the courage to come out as gay or lesbian (Ochs, 1996), a way to maintain heterosexual privilege and avoid societal prejudice (Israel and Mohr, 2004) or an excuse to temporarily enjoy a same-sex encounter and subsequently desert same-sex partners (Weiss, 2004). Alternatively, the association might be explained by cluster B personality traits which occur more commonly among females and include self-destructive behaviour and identity instability, commonly manifesting in confusion about sexual orientation.
The elevated risk of suicidality and NSSI among bisexuals found in this study is also consistent with research conducted among university students that found bisexual females, not lesbians, were at greater risk of NSSI (Whitlock and Knox, 2007), as well as results from a national population-based study in the United States which found that bisexual women had the poorest mental health and the highest prevalence of seven of nine Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV) mood and anxiety disorders (Bostwick, 2012). In Australia, one study has indicated that bisexual orientation was associated with worse mental health than homosexual orientation, but that the two groups did not differ on suicidality, although both were higher than the heterosexual group (Jorm et al., 2002). This study did not examine differences across gender.
The majority of homosexual and bisexual participants in this study did not experience suicidal ideation (79.5% of males, 72.7% of females), suicide attempts (87.2% of males, 74.6% of females) or NSSI (95.0% of males, 74.3% of females), suggesting some mitigation of protective factors against internalisation of sexual stigma. Both personal resources, such as resilience, hardiness and adaptive coping styles (Masten, 2001), and group resources, such as a sense of collective identity, strong affiliation with a group and linkage to a group with high self-esteem (Ashmore et al., 2004), have shown to protect against sexual stigma. Identifying and affiliating with like others allow individuals the opportunity to experience social environments in which they are not stigmatised, thereby reducing internalised stigma (Frable et al., 1997).
There are a number of limitations to be taken into account when interpreting the findings from this study. Measurement of suicide attempts and NSSI in the study were both self-report and retrospective, raising questions of reliability and recall bias. However, the secretive nature of self-destructive behaviours makes them difficult to measure otherwise. We believe that 12 months is not too great a time period in which to remember episodes of NSSI, and most people would remember attempting to kill themselves. In addition, the referent period for psychological distress (and suicidal ideation) referred to the past month, whereas the referent period for NSSI referred to the previous 12 months and for attempted suicide referred to the lifetime of participants. It is likely that adjustment of the association between sexual orientation and NSSI and attempted suicide for psychological distress (as a proxy for mental illness) under-estimates the contribution of mental illness associated with suicidal behaviour and NSSI. Suicidal ideation items selected from the GHQ-28, while not overlapping with the GHQ-12, are also likely to correlate with the GHQ-12 subset of items (used to measure psychological distress), which may be an additional source of measurement bias in analyses of the association between sexual orientation and suicidal ideation.
Also, while the study was strengthened using a nationally representative sample of the Australian population, no over-sampling of homosexual and bisexual groups was employed, and thus, the study was limited to relatively small number of cases of homosexual (n = 139) and bisexual (n = 151) participants, although these numbers are comparable to other studies researching this topic.
The accuracy of the sexual orientation variable was probably limited by social desirability bias, in that individuals may have been reluctant to identify as a sexual minority due to sexual stigma, particularly since they were potentially identifiable. Furthermore, participants who felt comfortable identifying as a sexual minority for this survey may have differed from those who chose not to identify as a sexual minority orientation since greater ‘outness’ is related to more positive mental health (Morris et al., 2001). Both these factors could have resulted in attenuation of the real association between sexual orientation and suicidality and NSSI in Australia. Factors associated with identifying as a sexual minority, perhaps relating to the impact of family responses to sexual orientation, and other potential consequences, such as bullying during adolescence, were items that were not available in the current dataset.
The one-dimensional nature (i.e. self-identification) of the sexual orientation measure also warrants consideration since sexual orientation comprises more than how a person identifies himself or herself and also includes sexual behaviour, desire, attraction, fantasies, and emotional, social and lifestyle preferences (Cochran and Mays, 2000b). However, there is some evidence that self-identification is the most accurate of the dimensions. The sexual orientation measure also lacked a category for transgender individuals, a very high-risk group for suicidality and NSSI (Herek et al., 2007). However, since transgender is not a sexual orientation per se (transgender refers to people whose gender identity, gender expression or behaviour does not confirm to that typically associated with the sex to which they were assigned at birth), it was outside the scope of the study. Furthermore, the prevalence of transgendered persons is very low (1:2000 for transwomen and 1:4500 for transmen (Olyslager and Conway, 2007)) and so would be difficult to draw conclusions from a population-based sample of the size employed in this study.
The results of this research have important implications for mental health clinicians and for wider society. First, clinicians are encouraged to discuss suicidality and NSSI with sexual minorities because they are at higher risk than the sexual majority. Particular attention should be given to whether suicidal intent is or is not present, as this will directly influence management. Reviewing the individuals’ personal and group resources might highlight areas for intervention, such as improving resilience, teaching adaptive coping skills or locating appropriate support groups. Increased affiliation with sexual minority support groups can help to reduce internalised sexual stigma, learn ways to cope with external stigma and obtain emotional and instrumental support (Herek and Garnets, 2007). Support groups might be especially helpful for bisexual females where their collective identity is weaker and the divide between homosexuality and bisexuality is more problematic. Affirmative practice is an appropriate therapy for sexual minorities as it enhances resilience and positive sense of self by increasing understanding and acceptance of one’s sexual orientation, increasing understanding of stigma and how it affects mental health and teaching healthy ways to cope (Eubanks-Carter et al., 2005).
If sexual stigma contributed to the increased prevalence of suicidality and NSSI among sexual minorities in this study, results suggest that Australian society must continue to work towards destigmatisation of sexual minorities. Non-heterosexual individuals are still often denigrated, discredited and constructed as invalid relative to heterosexuals; interventions designed to ‘cure’ homosexuality are still being used (Bieschke et al., 2006); marriage between same-sex couples is currently not yet legally recognised, and only one anti-discrimination law regarding sexual orientation exists at the federal level (the Fair Work Act 2009, Australian Human Rights Commission, 2011).
Future research in this area could be strengthened by more clearly investigating factors that modify the relationship between sexual orientation and suicidality and NSSI, such as level of ‘outness’, level of resilience, sense of affiliation and internalisation of sexual stigma. The measurement of cluster B traits would help to clarify the association between female bisexuality and NSSI. Finally, the measure of sexual orientation would ideally be multidimensional and include self-identification, sexual behaviour, desire and attraction, fantasies, and emotional, social and lifestyle preferences, in order to obtain a more accurate assessment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.