
Abstract
The negative effects of social disintegration and lack of social support on suicidality in adolescence have been documented by quite a few studies [1–5]. Family and parents provide one of the most important resources for social support during adolescence. A lack of parental care, a component of parental bonding according to the Parental Bonding Instrument (PBI) [6], along with family disintegration, can have a rather immediate effect on suicidality during childhood and adolescence [7]. However, there is only little evidence about a possible link between adverse parental child-rearing and suicidal ideation, suicidal attempts or suicide committed in adulthood. Although studies examined this link in early adulthood [8, 9], we are aware of only one case–control study examining the link between the PBI and serious suicidal behaviour among adults age 55 years and older [10]. Although this study showed significantly higher rates of paternal control in individuals with suicidal behaviour, the PBI showed no significant effect when taking intercorrelations between the PBI and other risk factors into account.
Beside other aetiological factors, we assume that stressful life events or chronic stressful circumstances influence the onset of suicidality in adulthood. The skills allowing individuals to cope with these stressors can reduce vulnerability to mental illness and suicidality. Those skills, like ‘participating, tolerating diversity and mutual responsibility …’, are ‘… associated with positive experiences of early bonding, attachment, relationships, communication and feelings of acceptance’ [11]. Therefore, one can hypothesize a possible link between adverse parental child-rearing during childhood and suicidality in adulthood to the extent that adverse parental child-rearing hampers the development of skills that can enhance a person's resilience in stressful situations; take, for example, social competence [12] and positive self-esteem [13].
When examining the association between parental bonding and suicidality in adulthood, one must consider the close relationship of suicidality to depression [14, 15] and other mental disorders like anxiety [16] or alcohol abuse/dependence [17, 18]. For instance, a recent study [19] found clinical depression associated with suicidal ideation with a population attributable risk of 46.9%. Therefore, adjusting for the effect of these mental disorders on suicidality seems necessary to make sure that a possible finding of an association between parenting and suicidality is not simply an artefact. Since data from six European countries were used, we had to adjust for possible country-specific differences of parental child-rearing styles.
The aim of the present study was to answer the following two questions:
Is there an association between adverse parental child-rearing and suicidality in adulthood? If the above hypothesis holds true, which of the three dimensions of the PBI (care, overprotection or authoritarianism) has the strongest association with suicidality?
Method
Recruitment procedure
European Study of Epidemiology of Mental Disorders (ESEMeD) is a cross-sectional household survey in a stratified multistage probability sample of 21 425 adult respondents (age 18 years and older) living in non-institutional settings in six European countries (Belgium n = 2419, France n = 2894, Germany n = 3555, Italy n = 4712, the Netherlands n = 2372, Spain n = 5473) [20, 21]. The overall response rate was 61.2%. Using computer-assisted interview techniques, the respondents were interviewed at home with a revised version of the World Mental Health Composite International Diagnostic Interview [22], which is subdivided into 38 different sections.
The interview was divided into two parts. Part I included the screening questions for most mental disorders, basic sociodemographic and risk factor data, and was administered to all respondents. All participants responding positively to any of the screening questions had to complete the Composite International Diagnostic Interview section of the specific disorder prompted by that question, as stipulated by DSM-IV criteria. Part II was administered to Part I respondents meeting the lifetime criteria for any core disorder and to a probability subsample (25%) of other Part I respondents not meeting any criteria [21].
Suicidality
After asking if respondents ever had one of the following experiences, the respondents were confronted with these two situations: ‘You seriously thought about committing suicide’ and ‘You attempted suicide’. The structure of these two dichotomous variables made it possible to construct a new variable with three mutually exclusive categories labelled ‘suicidality’. The new variable's first category was labelled ‘no ideation’ – here respondents had not thought about committing suicide. The second category was labelled ‘ideation’. Here respondents had thought about committing suicide without attempting it, while respondents of the third category (‘attempt’) had attempted suicide after thinking about it.
The parental bonding instrument
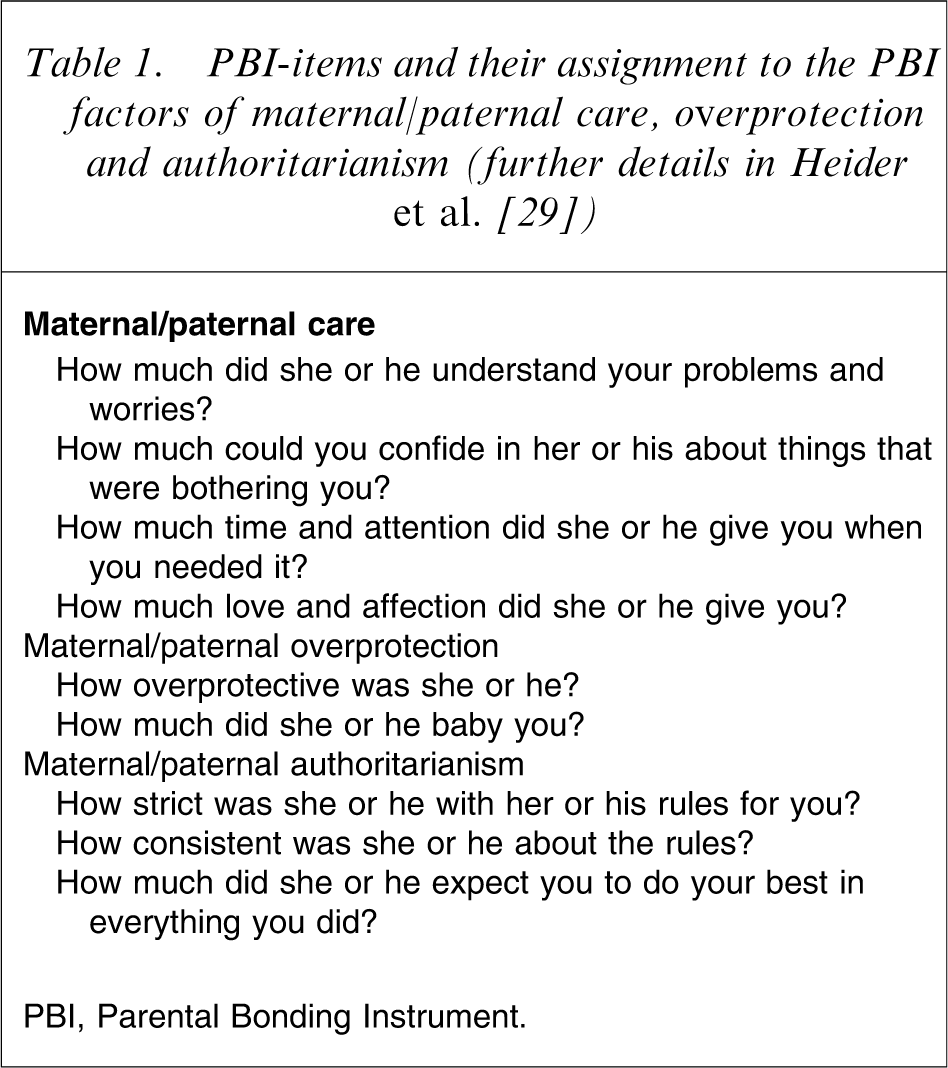
Developed by Parker et al. [6] the original PBI desired to measure the perceived parental rearing styles of care and overprotection as respondents remembered them from the first 16 years of life. It consists of 25 items assessed separately for mother and father. In a number of studies the PBI proved a reliable and valid measure of actual and not merely perceived parenting [6, 23–26].
After controversy whether a two- or a three-factor solution for the PBI might be more appropriate, some recent studies have used confirmatory factor analyses to show the pre-eminence of three-factor models of the PBI with the additional dimension ‘authoritarianism’ [27, 28]. In a previous study the authors were also able to confirm this three-factor structure for the nine-item short form of the PBI used in ESEMeD, as shown in Table 1 [29].
PBI-items and their assignment to the PBI factors of maternal/paternal care, overprotection and authoritarianism (further details in Heider et al. [29])
Sample
The PBI was administered to all Part II respondents plus those with alcohol- or drug-related problems. While 8813 respondents completed either the paternal or the maternal scale, there were responses from 8255 respondents who fully answered all nine questions of the PBI short scale we used for both of their parents. We had to pay attention to the fact that we wanted to investigate the relationship between an adverse parental child rearing style and suicidality in adulthood. Therefore, all respondents with an onset of suicidality during their first 16 years of life were excluded from the analysis resulting in n = 7762. As data for the education variable were missing for 22 respondents, 7740 respondents (Belgium n = 867, France n = 1324, Germany n = 1151, Italy n = 1604, Netherlands n = 944, Spain n = 1850) remained for analysis. Table 2 provides an overview of the sample's sociodemographic characteristics as well as the percentages for the three categories of ‘suicidality’.
Sociodemographic characteristics of the respondents by country (n = 7740). The European Study of Epidemiology of Mental Disorders project
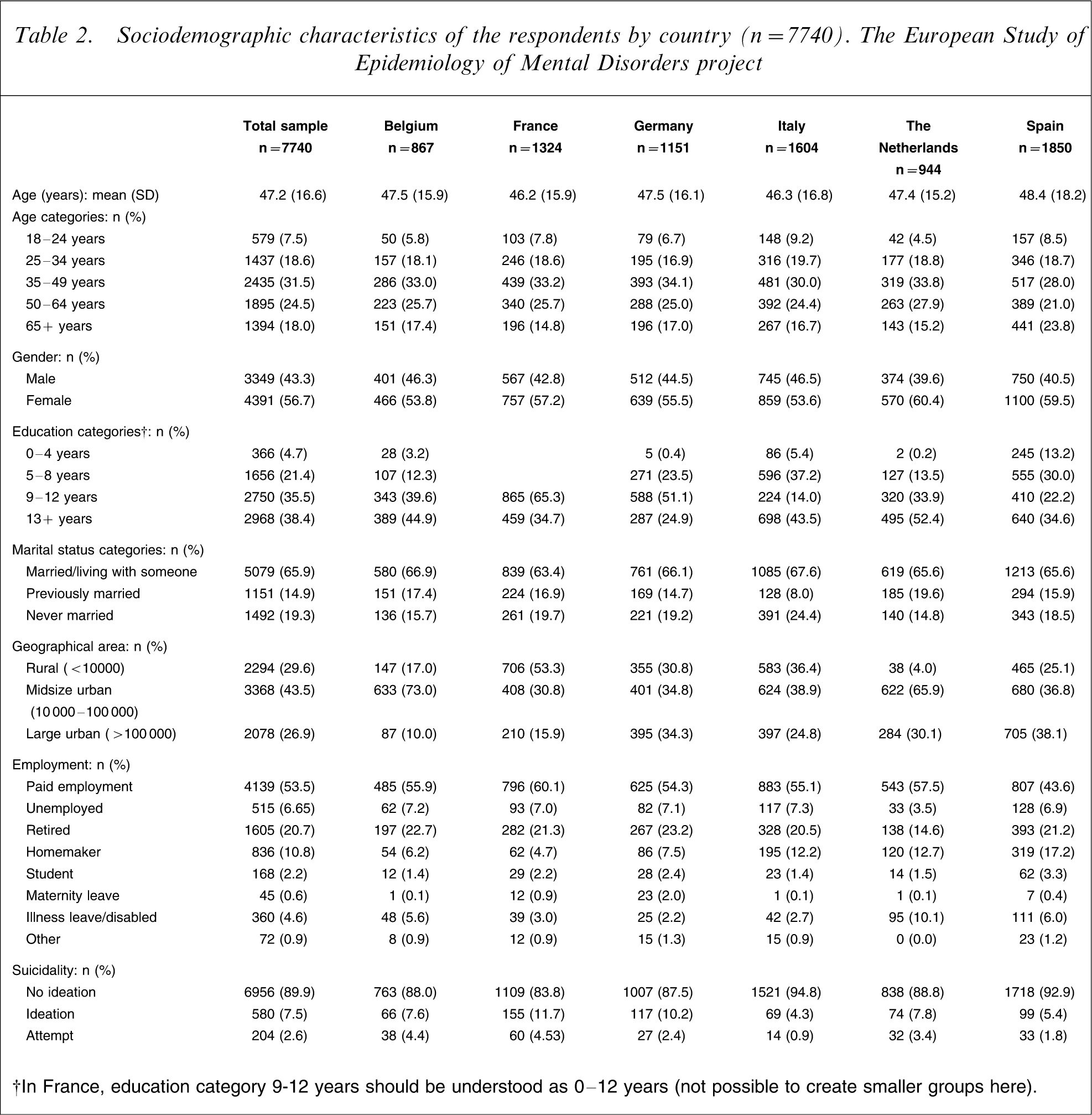
†In France, education category 9-12 years should be understood as 0-12 years (not possible to create smaller groups here).
Statistical analysis
The 2×3 (maternal and paternal) factor scores, extracted from the PBI-items, were used as explanatory variables in a multinomial logistic regression model with the outcome variable ‘suicidality’ in its three categories. Additionally, this model contains a set of important socio-demographic characteristics, the respondents’ citizenship, as well as dichotomous indicator variables for lifetime ‘mood disorder’ (including major depression and dysthymia), ‘alcohol abuse/dependence’ and lifetime ‘anxiety disorder’ (including social phobia, simple phobia, panic disorder, generalized anxiety disorder and agoraphobia), according to DSM-IV.
In order to test for observable heterogeneity across countries, all interaction terms between countries and PBI-scores were added to the regression model. This was undertaken because we had to assume that even non-significant effects of the PBI-scores might exhibit considerable variance. The effects of the explanatory variables are presented by means of relative risk ratios (RRRs). In doing this it should be noted that the RRRs for the explanatory variables are presented for all three categories of ‘suicidality’. This is possible because multinomial logistic regression ‘… can be thought of as simultaneously estimating binary logits for all comparisons among the dependent categories’ [30].
One convenient way to obtain the desired results is to utilize the procedure ‘listcoef’ in Stata after the estimation of a multinomial logistic regression analysis. ‘Listcoef’ is part of Scott Long's SPost package of Stata ado files which can be downloaded at http://www.indiana.edu/∼jslsoc/spost.htm. We decided to present the comparisons between ‘ideation’ versus ‘no ideation’ and ‘attempt’ versus ‘no ideation’, which currently correspond to a conventional output of a multinomial logistic regression with the base category ‘no ideation’. The additional comparison of ‘attempt’ versus ‘ideation’ differentiates between the other sets of estimated coefficients (see Table 3: the coefficients of the third column are the ratio between the second and the first column).
The multinomial logistic regression model with the three-categorical outcome variable suicidality: effects as relative risk ratios, n = 7740. The European Study of Epidemiology of Mental Disorders project
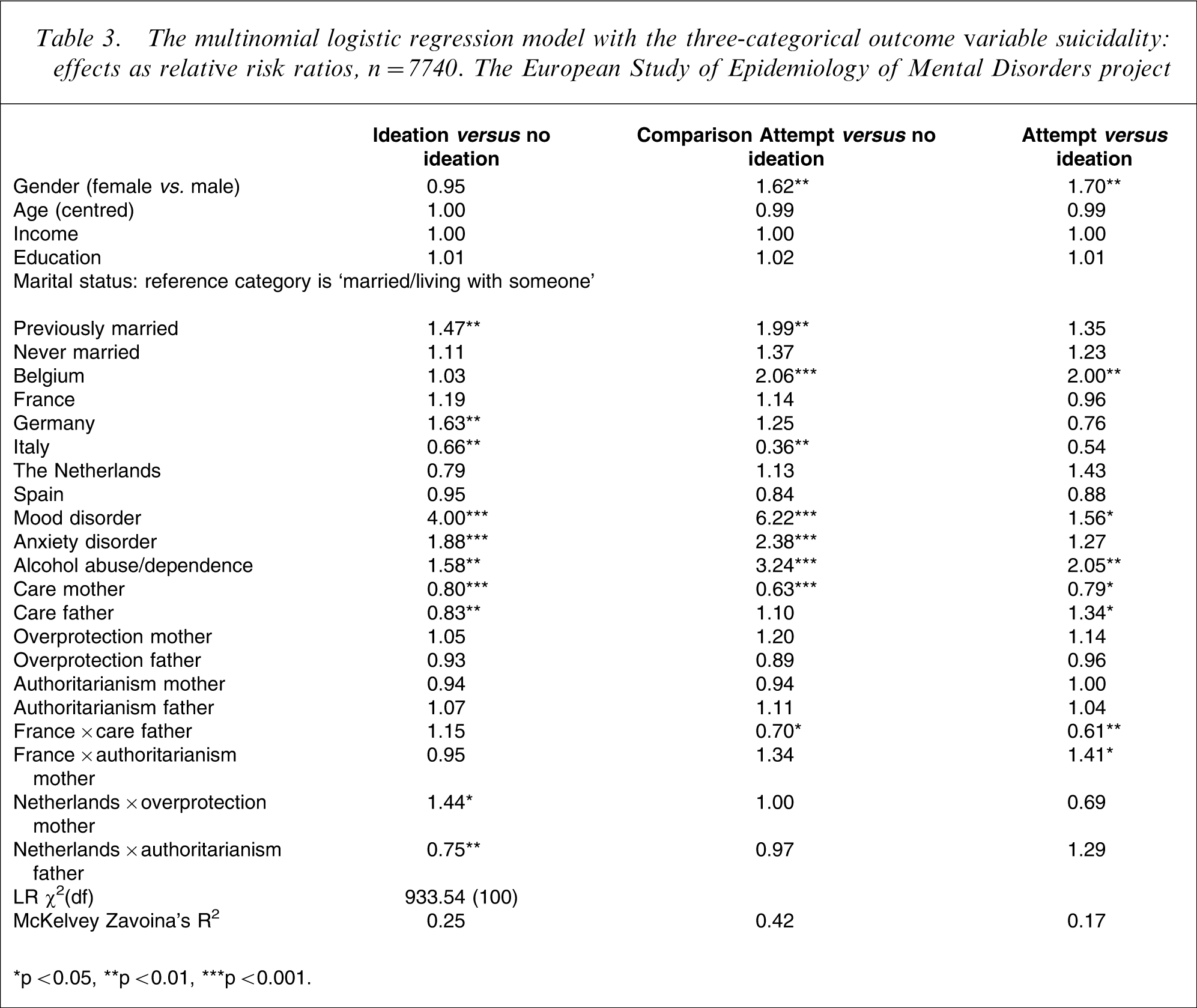
∗p < 0.05, ∗∗p < 0.01, ∗∗∗p < 0.001.
Concerning testing the country effects, effect coding was chosen over the more popular dummy coding. This form of contrasting allows one to test the deviation of single countries from an ‘average European’ effect, the so-called grand mean. McKelvey-Zavoina's Pseudo-R2 was chosen to test the significance of each comparison of the entire multinomial logistic regression model. This was done because the conventional log-likelihood-based McFadden's Pseudo-R2 severely underestimates the reduction error [31].
Results
Among the sociodemographic characteristics, the respondents’ sex and marital status were the only variables that showed significant effects, as seen in Table 3. The comparisons between ‘attempt’ versus ‘no ideation’ (RRR = 1.62) and ‘attempt’ versus ‘ideation’ (RRR = 1.70) indicated an increasing risk of ‘attempt’ for women. Respondents previously married showed a significantly higher risk for ‘ideation’ versus ‘no ideation’ (RRR = 1.47) and ‘attempt’ versus ‘no ideation’ (RRR = 1.99) than respondents of the reference group currently ‘married or living with someone’.
In Germany (RRR = 1.63), there was a significantly higher risk for ‘ideation’ (vs. ‘no ideation’) than in the average of all examined countries. In Italy the risks for ‘ideation’ (RRR = 0.66) and ‘attempt’ (0.36) were both lower than in the average of all six European countries. In Belgium the risk for ‘attempt’ (vs. ‘no ideation’ and vs. ‘ideation’) was significantly two times higher than the average of all countries.
As expected, mood disorder showed strong effects on ‘ideation’ (RRR = 4.00) and ‘attempt’ (RRR = 6.22), whereby the risk of ‘attempt’ was significantly greater than for ‘ideation’ (RRR = 1.56). Alcohol abuse/dependence showed significant effects on all three comparisons, while only the comparisons between ‘ideation’ versus ‘no ideation’ and ‘attempt’ versus ‘no ideation’ showed significant effects for anxiety disorder.
Maternal care showed significant effects on all three comparisons; the risk of ‘ideation’ (RRR = 0.80) and ‘attempt’ (RRR = 0.63) decreases with increasing maternal care, and the risk of ‘attempt’ decreases in comparison to ‘ideation’ (RRR = 0.79). With respect to paternal care, the comparison of ‘ideation’ versus ‘no ideation’ showed a similar effect (RRR = 0.83). However, there was no significant effect on the comparison between ‘attempt’ and ‘no ideation’ which resulted in a significant RRR of 1.34 when comparing ‘attempt’ and ‘ideation’. Neither ‘overprotection’ nor ‘authoritarianism’ showed any significant effect. Among 3×36 possible interaction terms between countries and PBI items, the bottom of Table 3 includes only those five that reached statistical significance in one of the three comparisons.
Discussion
As we always keep the main goal when examining suicidality in mind, we want to find factors whose modification potentially helps to prevent suicide. Against this background the present study aims to examine the influence of three parental rearing styles (Care, Overprotection, Authoritarianism) measured by a short form of the PBI [29] on the incidence of suicidality in adulthood in six European countries.
Our first question found an association between adverse parental rearing and suicidality in adulthood. The study's most important results involve the associations between a lack of maternal and paternal care on the one hand and suicidality on the other. As the most predominant parenting dimension, lack of care has also been found to be depressogenic in a number of studies preoccupied with parental bonding [24, 32–34] and is associated with the occurrence of anxiety disorders [35]. This more strongly emphasizes the presence of these associations even when the existence of lifetime ‘mood disorder’, lifetime ‘anxiety disorder’ and lifetime ‘alcohol abuse/dependence’ was taken into account.
Country differences (interaction terms) were only minor in nature taking into account the fact that we checked for 3×36 possible effects. Furthermore, we found the prevalence of ‘ideation’ and ‘attempt’ in Italy to be lower than the average of all six countries of the ESEMeD, which coincides with Schmidtke et al. [36], who likewise found Italy to have the lowest suicide rates among the countries investigated here (see figure 1 in [36]). We were able to find significant gender differences for ‘attempt’ but not for ‘ideation’. The higher risk of suicidal attempt for females agrees with a number of studies [37–40]. We also saw that previously married individuals show higher ‘suicidality’ rates than married people, which is in accordance with previous studies [41].
The present study has the advantage over most previous studies on suicidality, since it is based on a large representative population sample stemming from the ESEMeD. The respondents’ information about ‘ideation’ and ‘attempt’ was self-reported and, thus, subject to recall bias and denial. Individuals having committed suicide were not included in the analysis for obvious reasons. Insufficient information from non-responders did not allow us to examine whether their responses differed from those who did respond. Nevertheless, we assume we have underestimated the prevalence of suicidality, since individuals with suicidal behaviour tend to refuse participation in surveys more often [42, 43]. The low response rate (61.2%) may have also influenced the tendency to underestimate the prevalence of suicidality. This does not automatically imply that we have underestimated the association between parental child-rearing styles and suicidality, but we also cannot rule this underestimation out. Furthermore, although we used an abbreviated form, the PBI is a well-established instrument with good psychometric properties [44].
While suicidality and all psychiatric diagnoses were assessed as lifetime occurrences implying that their onset/offset was not taken into account, other factors like education or marital status were recorded at the moment of the interview.
Although these limitations and the cross-sectional nature of the data do not allow a strict causal interpretation of the results, the association found between parenting and suicidality in adulthood supports the hypothesis that parenting has a long-term impact on suicidality beyond the well-known short-term effects in adolescence. With the data available we unfortunately could not use a preferred path model in a prospective study design to investigate the structure of the associations we suspected between parental child-rearing, the possible mediating variables social competence, self-esteem and the outcome variable suicidality in adulthood.
A previous study [45] found a relationship between adverse parenting (as measured by the PBI) and low self-esteem, thereby showing that these suspected associations are not purely speculative. Further, since single people are more likely to commit suicide [41, 46], and assuming that this is at least partially caused by their inability to form a supportive social network as a consequence of adverse childhood experiences, we think that future studies in this direction can be profitable. Nevertheless, we have to be aware that suicidality is caused by multiple risk factors [47]. For instance, Mann [48] developed a model of suicidal behaviour that includes personality factors like aggression and impulsivity or the neurobiological factor of serotonergic activity in addition to well-known factors like depression or psychosis. It is therefore important to keep in mind that the association between parental bonding and suicidality can only be one piece of the whole puzzle.
The preventive character of parental care provides an opportunity to implement public mental health programs aiming to increase parents’ understanding of the basic needs of their offspring such as emotional warmth and protection. In order to ‘… enhance family protective factors and to reduce risk factors associated with severe behavioural and emotional problems in preadolescent children …’ the advantages of prevention on a universal population-level and on more individual levels are well balanced in a multilevel strategy in the Triple-P-Positive Parenting Program [49]. The Triple-P can serve as an example for effective prevention where the use of a multilevel strategy enables us to take into account parents’ individual needs and their mode of required assistance, as well as the differing levels of mental and behavioural dysfunction in children. Following these steps, it becomes possible to establish better (more caring) parenting environments in special high-risk groups as well as in the entire population, which promotes the development of children's social and emotional competencies: individual skills that are not the only important protective factors in the prevention of suicide.
Furthermore, strengthening families’ material resources as well as improving the integration of families into society may be appropriate social-political means for the medium-term creation of a caring family environment and thus a long-term reduction of suicidality in adulthood. As with other psychiatric disorders we would argue that only a combination of complementary strategies can be sufficient to reduce the vulnerability to suicidality by activating the protective effects of parental care. Adjustments of single strategies and their mixture in accordance with cultural differences could be necessary for a successful intervention [50].
Footnotes
Acknowledgements
This project was funded by the European Commission (Contract QLG5-1999-01042); the Piemont Region (Italy), Fondo de Investigacion Sanitaria, Instituto de Salud Carlos III, Spain (FIS 00/0028), Ministerio de Ciencia Y Tecnologia, Spain (SAF 2000-158-CE), Department de Salut, Generalitat de Catalunya, Spain, other local agencies and by an unrestricted educational grant from GlaxoSmithKline.
European Study of Epidemiology of Mental Disorders is carried out in conjunction with the World Health Organization World Mental Health (WMH) Survey initiative.