
Abstract
Objectives:
Borderline personality disorder is a complex mental disorder that is associated with a high degree of suffering for the individual. Dialectical behaviour therapy has been studied in the largest number of controlled trials for treatment of individuals with borderline personality disorder. The conversational model is a psychodynamic treatment also developed specifically for treatment of borderline personality disorder. We report on the outcomes of a randomised trial comparing dialectical behaviour therapy and conversational model for treatment of borderline personality disorder in a routine clinical setting.
Method:
Participants had a diagnosis of borderline personality disorder and a minimum of three suicidal and/or non-suicidal self-injurious episodes in the previous 12 months. Consenting individuals were randomised to either dialectical behaviour therapy or conversational model and contracted for 14 months of treatment (n = 162 commenced therapy). Dialectical behaviour therapy involved participants attending weekly individual therapy, weekly group skills training and having access to after-hours phone coaching. Conversational model involved twice weekly individual therapy. Assessments occurred at baseline, mid-treatment (7 months) and post-treatment (14 months). Assessments were conducted by a research assistant blind to treatment condition. Primary outcomes were change in suicidal and non-suicidal self-injurious episodes and severity of depression. We hypothesised that dialectical behaviour therapy would be more effective in reducing suicidal and non-suicidal self-injurious behaviour and that conversational model would be more effective in reducing depression.
Results:
Both treatments showed significant improvement over time across the 14 months duration of therapy in suicidal and non-suicidal self-injury and depression scores. There were no significant differences between treatment models in reduction of suicidal and non-suicidal self-injury. However, dialectical behaviour therapy was associated with significantly greater reductions in depression scores compared to conversational model.
Conclusion:
This research adds to the accumulating body of knowledge of psychotherapeutic treatment of borderline personality disorder and supports the use of both dialectical behaviour therapy and conversational model as effective treatments in routine clinical settings, with some additional benefits for dialectical behaviour therapy for persons with co-morbid depression.
Keywords
Borderline personality disorder (BPD) is associated with a high degree of suffering, high rates of suicide attempts (Lieb et al., 2004) and a lifetime suicide mortality rate of approximately 10% (Black et al., 2004). Beyond high levels of symptomatic impairment, large-scale studies have shown pervasive social and functional impairment (Gunderson et al., 2011). Depression commonly co-occurs with BPD (Beatson and Rao, 2013). Within mental health settings, approximately 10% of all psychiatric outpatients and between 15% and 25% of psychiatric inpatients meet criteria for BPD (Leichsenring et al., 2011). During the past 30 years, there has been considerable progress in treatments developed and evaluated for BPD. Psychiatric medication is not a recommended first-line treatment as it does not alter the course of the disorder and psychotherapy is the indicated treatment for BPD (National Collaborating Centre for Mental Health (NCCMH), 2009; National Health and Medical Research Council (NHMRC), 2012).
A number of cognitive behavioural therapies have been developed or adapted specifically for the treatment of BPD with varying degrees of evidence from randomised trials (Stoffers et al., 2012). Dialectical behaviour therapy (DBT) is one of these therapies and targets skill development to build a ‘life worth living’ (Linehan and Wilks, 2015). DBT has been the focus of more clinical trials than any other psychotherapy for BPD (Cristea et al., 2017). Across these trials, results generally show a reduction in suicidal and non-suicidal self-injurious (NSSI) episodes and psychiatric hospital admissions. Beyond cognitive behavioural therapies, there is evidence from randomised trials for numerous psychodynamic therapies developed specifically for the treatment of BPD (Bateman and Fonagy, 1999, 2009; Clarkin et al., 2007; Gunderson and Links, 2014). Conversational model (CM) was originally developed by Hobson and Meares and then further developed by Meares as a specific model to treat BPD, targeting the development of a healthy sense of self (Meares, 2004, 2012). It focuses heavily on the therapeutic relationship as a template for other relationships and aims to help individuals increase their capacity to build a reflective awareness of inner events (Meares, 2012: 20). CM has been evaluated for BPD in a published study (Stevenson and Meares, 1992), utilising a pre-post design, with a replication study (Korner et al., 2006), using a treatment as usual waiting list control, but has not yet been tested in a randomised trial. Both CM studies showed significant reduction in suicidal behaviour and NSSI, and hospital admissions after 1 year of therapy, with gains maintained at 5-year follow-up (Stevenson et al., 2005).
There are two studies, adequately powered by large sample sizes and where DBT was delivered with fidelity, which have compared DBT with another ‘active’ treatment. Linehan et al. (2006a) compared DBT with ‘treatment by experts’ that included clinicians in the community with expertise in treating BPD using non-DBT treatments. DBT was found to be superior on outcomes of suicide attempts, treatment retention and service utilisation. McMain et al. (2009, 2012) compared DBT with general psychiatric management (GPM), a psychodynamic therapy with a medication algorithm and found both treatments demonstrated significant reductions in suicidal behaviour and NSSI between pre-treatment and post-treatment, as well as on a range of other clinically relevant measures.
There is no direct evidence from comparisons of active models developed specifically for the treatment of BPD that any one form of psychotherapy is superior to any other model. In the most recent Cochrane review of BPD (Stoffers et al., 2012), the authors outlined several limitations of studies of outpatient psychotherapeutic treatment for BPD. Many have small sample sizes (range, n = 47–180). Apart from DBT, most treatments have only been evaluated in one or two studies (Stoffers et al., 2012) and the majority of studies have been conducted by investigators who developed the treatment or who have a strong allegiance to one particular model (Bateman and Fonagy, 2009; Giesen-Bloo et al., 2006; Levy et al., 2006; Linehan and Wilks, 2015).
Among psychotherapy studies in which all investigators have allegiance to one particular model, outcomes have been consistently in support of that treatment model (Luborsky et al., 1999). Researcher allegiance is now well recognised as affecting results (Leichsenring et al., 2017). Hence, replications are needed, particularly by independent researchers not involved in treatment development. Furthermore, most have been conducted in university settings by highly trained therapists; consequently, it is unclear how well effects would generalise to real-world clinical settings (Roy-Byrne et al., 2003).
The aims of this study were (1) to evaluate DBT in a routine clinical setting and compare it against an active treatment and (2) to compare CM against another therapy for BPD with an established evidence base. CM was selected as the active treatment for this study based on the promising evidence and because it is one of few treatments specifically designed for treatment of BPD that is taught and used in Australia (Korner and McLean, 2017). This study attempted to address some of the limitations identified above.
Method
Study design
This is a single-site, two-armed parallel randomised controlled trial (RCT) designed to investigate the effectiveness of CM and DBT in a public sector mental health service in Australia. The sample population comprised adults with a primary diagnosis of BPD and recent suicide attempts and/or NSSI episodes. The main aim of this study was to compare CM with DBT for two primary outcomes at post-treatment (14 months): (1) change in the number of combined endpoint episodes of suicidal behaviour and NSSI and (2) change in depression severity. We expected that (1) both treatments would lead to significant change after 14 months, (2) DBT would be more effective in reducing the number of episodes of suicidal and NSSI after 14 months and (3) CM would be more effective in reducing depression severity after 14 months. The study was approved by the Hunter New England Human Research Ethics Committee (Reference Number: 06/12/13/5.11) and registered with the Australian New Zealand Clinical Trials Registry (ACTRN 12612001187831).
Participants
This study was conducted at the Centre for Psychotherapy, a specialist outpatient service for BPD and/or Eating Disorders of the Hunter New England Mental Health Service, located in Newcastle, New South Wales, Australia. Referrals were accepted from community mental health teams, general practitioners or private therapists. There were no treatment costs for patients. Recruitment started in January 2007, and the final sample size of 162 was reached in April 2013. The final post-treatment data (14 months) collection occurred in June 2014.
The inclusion criteria for this study (and the service) were as follows: (1) BPD according to Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) criteria (American Psychiatric Association (APA), 1994) – with the diagnosis of BPD made by a consultant psychiatrist using the Structured Clinical Interview for the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (SCID-II; First et al., 1995); (2) three episodes of suicide attempts and/or NSSI in the past 12 months, where NSSI behaviour is defined in accordance with the Suicide Attempt and Self-injury Count (SASI-Count; Linehan and Comtois, 1996) as acute, intentional self-injurious behaviour such as cutting, overdosing, burning and deliberate self-poisoning without the intention of dying; and (3) aged between 18 and 65 years. The exclusion criteria for this study were as follows: disabling organic conditions, current acute psychotic illness, antisocial behaviour that posed a significant threat to staff and fellow patients, developmental disability, living more than 1 hour’s drive from the treatment centre, inability to speak or read English, current substance dependence other than nicotine (as measured by SCID-I; but eligible for entry once no longer meeting the criteria for dependence) and prior treatment with DBT or CM (as reported by the patient).
Procedure
Upon referral, patients were allocated an appointment for an initial assessment with an allied health clinician or nurse therapist (all with a minimum of 5 years’ mental health experience) to determine whether they met eligibility criteria for the service. If they met the criteria, they attended a diagnostic interview with a consultant psychiatrist.
All patients meeting the inclusion criteria were invited by a research assistant to participate in the study. Patients were provided with a full explanation of the procedures and study conditions. Written informed consent was obtained from all participants. Participants received AUD$20 per assessment to cover transport and related costs. Consenting participants were randomly allocated to either DBT or CM. Figure 1 illustrates the flow of participants in the RCT.
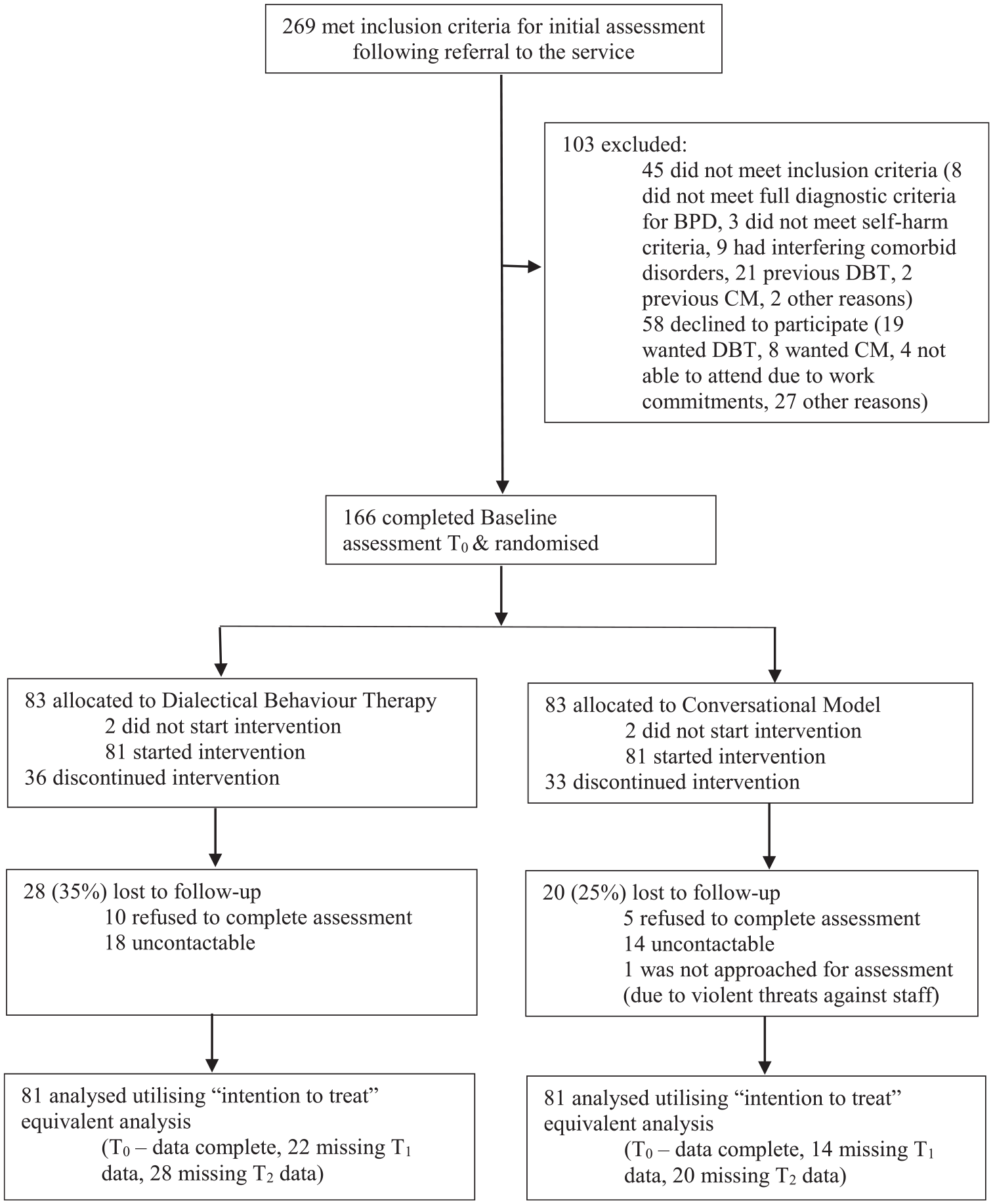
Flowchart of participants (CONSORT diagram).
A stratified randomisation procedure was used to maximise the likelihood of comparable distributions across groups for gender and antidepressant use. A computerised formula with blocked randomisation (blocks of 4) was used by an independent research manager of the health service. A sealed, opaque envelope containing randomisation status was given to participants at the end of their assessment. Participants were instructed not to tell the research assistant the treatment to which they had been randomised. After randomisation, the waiting list manager in the service allocated participants to a therapist. Participants commenced therapy within 2 weeks of randomisation.
As is consistent with psychotherapy trials for BPD, medication was not standardised; its type and amount were decided on an individual basis by participants’ medication providers (general practitioners or psychiatrists).
Assessments
Data were collected at three time points: baseline (T0), mid-treatment mark of 7 months (T1) and post-treatment at 14 months (T2). Follow-up data are being collected at three additional time points: 1 year (T3), 2 years (T4) and 5 years (T5) follow-up. Only time points T0, T1 and T2 will be reported in this article, with T2 the primary endpoint.
Experienced research assistants with a minimum bachelor’s degree in psychology conducted all research assessments, blind to treatment allocation status. To maintain blindness, the research assistant was scheduled to work at different times to when the skills training groups were run.
Primary outcome measures
There were two primary outcomes: change from baseline to post-treatment in (1) number of episodes of suicidal and NSSI and (2) self-reported depression severity scores. While the primary outcome comparison was baseline to post-treatment, two other planned comparisons were also assessed: change from baseline to mid-treatment and from mid-treatment to post-treatment.
The specific measures used to evaluate each outcome are summarised below with the outcome domain identified first, followed by the measure used:
(a) Combined outcome of any episode of suicidal and non-suicidal self-injury: the SASI-Count (Linehan and Comtois, 1996; Linehan et al., 2011). The SASI-Count is a brief clinician-administered measure categorised into suicide attempts and non-suicidal acts within a specified period. This study utilised an adapted time frame of behaviour occurring within the past 7 months. The SASI-Count is a briefer version of the Suicide Attempt Self Injury Interview (SASII; Linehan et al., 2006b) which assesses self-injury in more detail. The SASII has demonstrated good reliability and validity. The SASI-Count was chosen over the SASII to reduce assessment burden.
(b) Depression severity: Beck Depression Inventory II (BDI-II; Beck et al., 1996). We chose the BDI-II because in our clinical experience dysphoria and self-reported depression are often the symptoms that clients report as most distressing, and because several previous seminal studies of BPD have incorporated the BDI-II (Bateman & Fonagy, 1999; Linehan et al., 1991; 2006a; McMain et al., 2009). The BDI-II is a self-report instrument designed to assess and detect the severity of current (past 2 weeks) depressive symptoms and contains 21 descriptive statements frequently reported by individuals diagnosed with depression. Each of the items contains a 4-point severity-rating scale. It is a widely used, reliable measure of depressive symptoms. It has high internal consistency and correlates well with other self-report measures of depression and with clinician ratings of depression (r = 0.60–0.90; see Beck et al., 1987, for a review).
Secondary outcome measures
(a) BPD Severity: Borderline Personality Disorder Severity Index (BPDSI-IV; Arntz et al., 2003). The BPDSI is a semi-structured interview based on DSM-IV criteria, assessing the frequency and severity of various aspects of BPD. It has 70 items and the reference period is 3 months. It has high inter-rater reliability and high internal consistency (intra-class correlation = 0.97, Cronbach’s α = 0.93), and high concurrent and discriminant validity.
(b) Interpersonal problems: Inventory of Interpersonal Problems (IIP; Horowitz et al., 1988). The IIP is a self-administered questionnaire for assessment of subjectively experienced interpersonal difficulties. The IIP and its derivatives provide an overall quantitative index of interpersonal problems and scores on eight subscales. Each subscale consists of eight items answered on 5-point scales from 0 (Not at all) to 4 (Extremely). It has high internal consistency (Cronbach’s α = 0.96) and good convergent validity (Horowitz et al., 1988).
(c) Dissociation: Dissociative Experiences Scale (DES; Bernstein and Putman, 1986). The DES is a 28-item self-report measure designed to quantify dissociative experiences. The DES has strong internal reliability (mean Cronbach’s α = .93), very good convergent validity and good predictive validity with Dissociative Identity Disorder and PTSD.
(d) Sense of self: Sense of Self Inventory (SSI; Basten, 2008). The SSI is a 23-item self-report measure designed to identify several core components that reflect the subjective and continuous experience of being an individual, authentic person who is in control of their own mental and physical activities. Participants indicate responses on a 4-point Likert scale ranging from 1 (Strongly Agree) to 4 (Strongly Disagree).
(e) Mindfulness: Kentucky Inventory of Mindfulness Skills (KIMS; Baer et al., 2004). The KIMS is a 39-item self-report inventory used for the assessment of mindfulness skills. Mindfulness is generally defined to include focusing one’s attention in a nonjudgmental way or accepting the experience occurring in the present moment (Baer et al., 2004). Participants indicate responses on a 5-point Likert scale ranging from 1 (Never or very rarely true) to 5 (Very often or always true). The instrument has good internal consistency and adequate to good test–retest reliability. It demonstrates good content and concurrent validity, correlating positively with other related measures.
(f) Emotion regulation: The Difficulties in Emotion Regulation Scale (DERS; Gratz and Roemer, 2004). The DERS is a 36-item self-report questionnaire designed to assess multiple aspects of emotion dysregulation during times of distress. Participants indicate responses on a 5-point Likert scale ranging from 1 (Almost never) to 5 (Almost always). The DERS has been found to have high internal consistency (Cronbach’s α = 0.93), good re-test reliability, and adequate construct and predictive validity.
Treatment
Patients were required to commit to 14 months of twice weekly psychotherapy in either programme: twice weekly individual therapy sessions in the CM condition, and a once weekly individual therapy session and once weekly skills training group session in the DBT condition.
DBT
DBT is a manualised treatment (Linehan, 1993a, 1993c) for BPD that combines treatment strategies from behavioural, cognitive and supportive psychotherapies. In this study, it included weekly individual pre-treatment sessions for approximately 4 weeks. Pre-treatment sessions included orientation to the treatment model, exploring goals and eliciting a commitment to therapy. Pre-treatment sessions were followed by concurrent weekly individual and skills training group sessions for 12 months. Individual therapy sessions took approximately 1 hour per week and applied directive, problem-oriented techniques (including behavioural skill training, contingency management and cognitive modification) alongside supportive techniques. The skills group met weekly for 2.5 hours and followed a psycho-educational format. It included teaching and application of skills, and targeted practice.
Participants had access to telephone coaching with their individual therapist during working hours. Outside of this, participants had access to a telephone service staffed by a roster of DBT therapists, available 7 days per week from 8:30 a.m. to 10:00 p.m. DBT therapists attended a weekly consultation team meeting designed to provide support and assist therapists to be adherent to treatment.
The 14-month schedule allowed for the pre-treatment phase in DBT to occur before participants commenced 48 sessions of skills training that occurred concurrently with individual therapy.
CM
Participants in the CM treatment arm attended twice weekly individual therapy for 14 months. The treatment model was developed by Meares (2004) and is outlined in a published treatment manual (Meares, 2012). The sessions were approximately 1 hour and were nondirective with the focus on understanding the patient’s emotional experience and actively describing that back to the patient. The therapist actively looks for subtle signs of emotionally misunderstanding the patient, leading to mutual self-reflection and repair of the moment of disconnection in the therapeutic relationship. High value was placed on the patient’s real experience (as against socially acceptable experience) and the development of an authentic personal narrative. The patient was encouraged to find links between the maladaptive relationship patterns they had developed in their current social world and the relationship pattern they had with the therapist.
Fourteen months of therapy was selected as the treatment length to match that being received in the DBT condition. Previous research on CM has involved treatment of 1 or 2 years duration. There was no explicit pre-treatment phase in CM; however, it involved an extended assessment that occurred at the beginning of the 14 months.
Therapists
Treatment was delivered by 32 therapists, all with a minimum of 2 years of clinical experience. Therapists were employed in the government health service and not hired specifically for this trial. The majority were employees of the Centre for Psychotherapy; some therapists were employed in community or hospital mental health settings and served as visiting therapists. Disciplines included psychologists, psychiatrists or psychiatric trainees, social workers, mental health nurses and occupational therapists. Some therapists provided treatment in both models (n = 12), some provided treatment in DBT only (n = 7), and some in CM only (n = 13). The number of participants treated by the 32 therapists ranged from 1 to 16 and there was a different pattern among those who provided only one therapy (n = 20) with a mean number of patients of 2.42 (median = 2) compared with those who provided both (n = 12, mean = 9.67, median = 9.5).
Supervision
Therapists providing treatment in the DBT arm of the trial were required to complete a minimum of 4 days of DBT training. Many had completed additional 2-day training sessions with the treatment developer’s training company, Behavioral Tech. The majority completed 10-day DBT intensive training with Behavioral Tech.
Therapists providing treatment in the CM arm of the trial attended an introductory programme; this involved a series of a minimum of 6 × 2-hour seminars. For psychiatric trainees and psychiatrists, due to scheduling difficulties, the initial training involved meeting one on one with a staff specialist psychiatrist (N.B.) with extensive experience in the model. The majority of therapists in the CM arm of the trial had either completed or were completing a 3-year part-time diploma in CM with the treatment developer’s training organisation, Australian and New Zealand Association of Psychotherapy.
Treatment fidelity
Fidelity was monitored through supervision. Therapists delivering DBT attended a weekly consultation team meeting. Therapists who had only recently learned DBT also received individual supervision initially. All CM therapists were involved in weekly supervision with an experienced supervisor either individually or in pairs.
Modality-specific adherence scales were used to evaluate treatment fidelity and will be reported in the ‘Results’ section. DBT sessions were rated by a coder trained in the use of the Dialectical Behavior Therapy Global Rating Scale (Linehan, 1993b). An overall score of 4 or higher indicates that the session was conducted adherently. Reliability checks were conducted between the coder and a member of Linehan’s team. In the absence of a suitable adherence scale for CM at the start of the study, one was developed for use for this study. CM sessions were rated by a coder trained in the use of the Newcastle Adherence Scale for CM (NASCOM; Goldman, 2012). The NASCOM is a 25-item scale in which the items have been demonstrated to have good inter-rater reliability and good discriminant validity, in that it could distinguish between adherent CM and DBT sessions. Reliability checks were conducted between the coder and the scale developer.
Adherence raters were blind to treatment allocation. A randomly selected 5% sample of all sessions was rated for adherence. Therapists were not provided with the results of the adherence coding until all participants had finished therapy, as it is unrealistic that such feedback would be accessible in a real-world setting.
Statistical analysis
Sample size
The planned number of participants in the study was 162, based on the assumption that two-thirds would be retained at post-treatment (i.e. 54 participants per intervention condition). Family-wise Bonferroni-corrected statistical tests were employed throughout – namely alpha divided by 2 for the two primary outcome measures (i.e. 0.025), and alpha divided by 6 for the secondary outcome measures (i.e. 0.0083). It was expected that a retained sample of 108 participants at post-treatment would provide sufficient statistical power (80%) to detect modest population associations (e.g. simple or partial correlations, standardised regression weights for group comparisons or interactions, etc.) of 0.30 or higher for the primary outcome measures, using two-tailed statistical tests in the sample, or 0.34 or higher in the case of the secondary outcome measures; which equates to the detection of standardised population differences between treatment conditions (i.e. Effect Sizes) of 0.59 and 0.67, respectively.
Analysis
All patients who were randomised and attended a minimum of one treatment session after the baseline assessment were included in the analysis. All available data from the three time points were included in each analysis (not just complete pairs), using specific planned comparisons to examine differences between time points (and account for the repeated-measures component of the variance). For consistency, major outcome analyses involving continuous measures were based on change scores from baseline (T0), expressed as either mid-treatment (T1) or post-treatment (T2) minus baseline phase. Negative binomial models were utilised in the analyses examining suicide attempts, NSSI and their aggregation, effectively treating these data as counts. All of the analyses included as a co-variate the baseline raw scores for the particular measure being investigated. Generalised linear modelling techniques (generalised estimating equations, GEEs) were used to examine differences between groups in the changes over time (with within-subject variation coded using subject IDs and study time point); an ‘independent’ working correlation matrix was specified (i.e. uncorrelated repeated measurements), with other patterns also examined that confirmed the stability of parameter estimates. For both primary and secondary outcomes, z scores were also calculated to illustrate standardised change, expressed in relation to the grand SD of change. SPSS 22.0 software package for Windows was used for statistical analyses.
Treatment of missing data
As shown in Figure 1, 28 participants were lost to follow-up evaluation at post-treatment in the DBT condition, compared with 20 participants in the CM condition. To take into account missing data and maximise usage of all available data, major analyses comprised a series of generalised linear models (and, where appropriate, GEE analyses), together with some supplementary sensitivity analyses (e.g. restricted to participants completing post-treatment assessments).
Results
Recruitment
Participant flow across the trial is presented in Figure 1. In total, 269 patients were referred to the service during the recruitment period, of whom 45 did not meet inclusion criteria for the study and 58 declined to participate. A total of 166 people consented to randomisation and completed research assessments. Four of these did not attend the first therapy appointment, leaving 162 participants included in the study (see Figure 1) who gave written informed consent and attended at least one therapy session.
Patient characteristics
Selected demographic and clinical characteristics of the two groups are presented in Table 1. Participants were mainly single, White Caucasian women in their 20s, with varying levels of education. The two groups showed no imbalances at baseline after randomisation with regard to sociodemographic and clinical characteristics.
Baseline sociodemographic and clinical characteristics of participants.
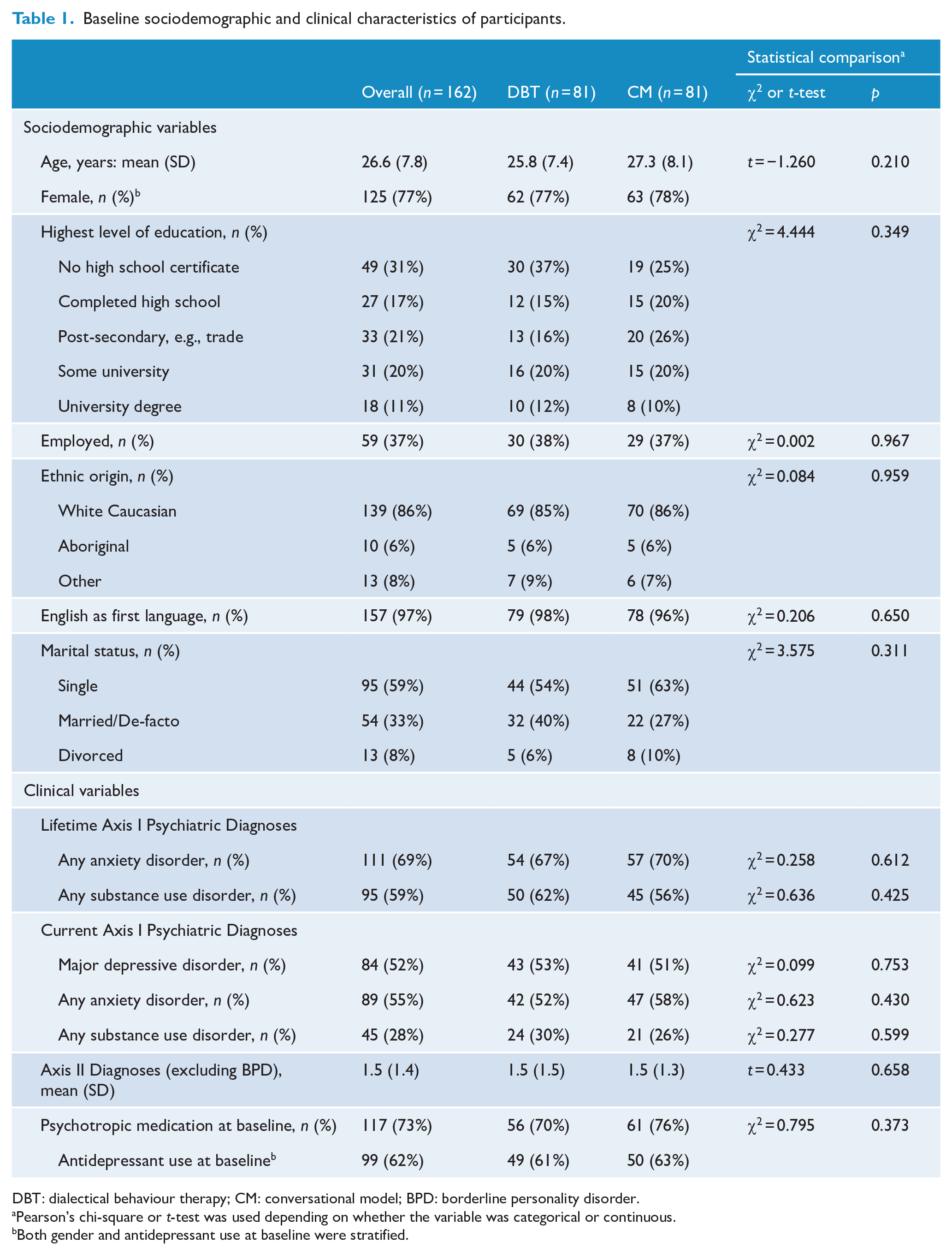
DBT: dialectical behaviour therapy; CM: conversational model; BPD: borderline personality disorder.
Pearson’s chi-square or t-test was used depending on whether the variable was categorical or continuous.
Both gender and antidepressant use at baseline were stratified.
Treatment outcomes
Intent-to-treat analyses showed a significant reduction over time in both primary outcomes of (1) any suicidal and/or NSSI (Wald’s χ2 = 41.59, p < 0.001) and (2) depression severity (Wald’s χ2 = 142.02, p < 0.001). These results are detailed in Table 2. There were no significant differences between DBT and CM on suicidal and/or NSSI. Suicidal behaviour and NSSI were also examined separately, showing a similar pattern of results (see Table 2 and Figures 2–4). There were no deaths in either group. Compared to CM, DBT was associated with a significant differential benefit in depression severity scores from baseline to mid-treatment (Wald’s χ2 = 8.05, p = 0.005) and from baseline to post-treatment (Wald’s χ2 = 8.00, p = 0.005); see the group × time interaction effects in Table 2 and the associated mean changes displayed in Figure 5.
Generalised linear model results of primary outcomes of suicide attempts and NSSI and depression severity.
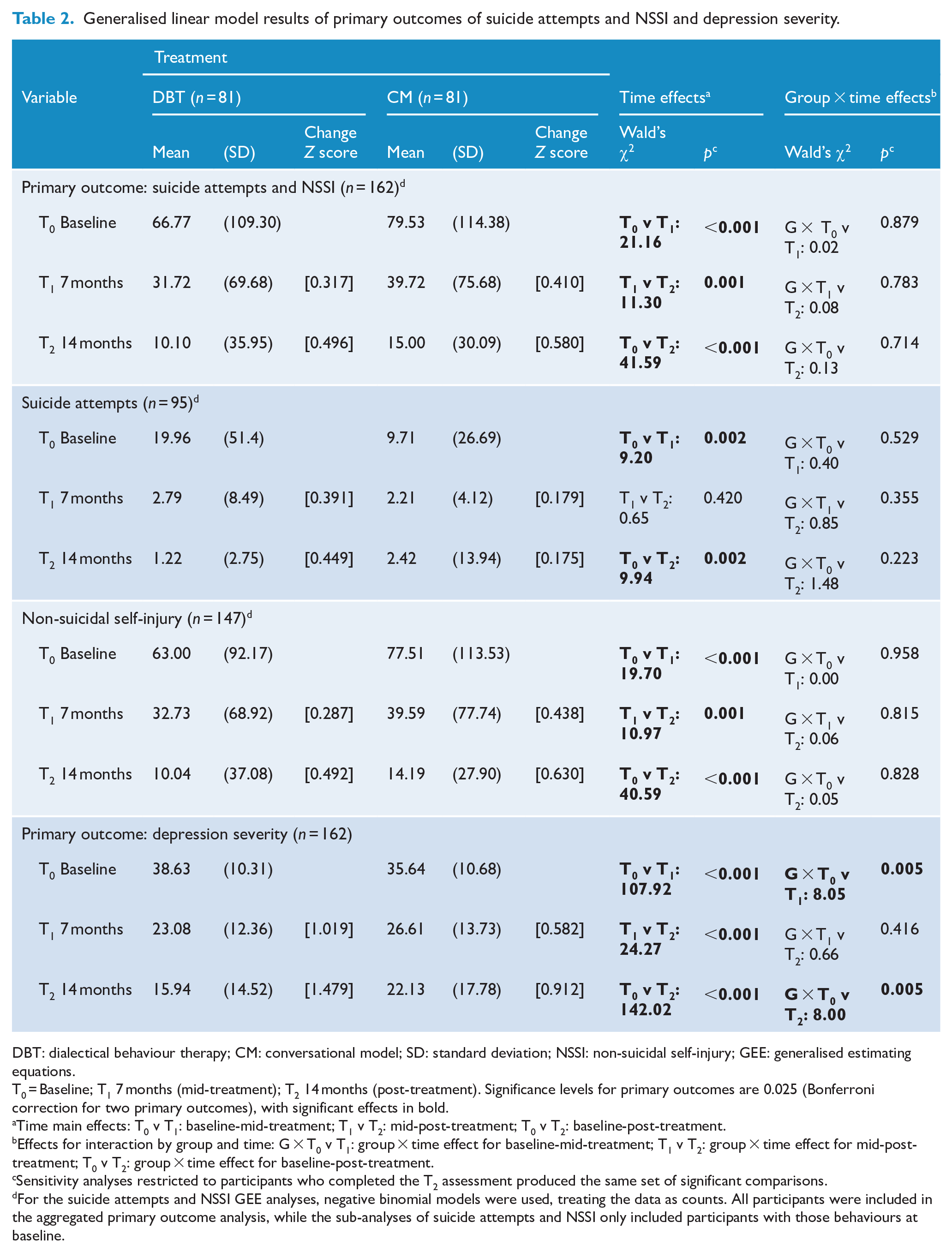
DBT: dialectical behaviour therapy; CM: conversational model; SD: standard deviation; NSSI: non-suicidal self-injury; GEE: generalised estimating equations.
T0 = Baseline; T1 7 months (mid-treatment); T2 14 months (post-treatment). Significance levels for primary outcomes are 0.025 (Bonferroni correction for two primary outcomes), with significant effects in bold.
Time main effects: T0 v T1: baseline-mid-treatment; T1 v T2: mid-post-treatment; T0 v T2: baseline-post-treatment.
Effects for interaction by group and time: G × T0 v T1: group × time effect for baseline-mid-treatment; T1 v T2: group × time effect for mid-post-treatment; T0 v T2: group × time effect for baseline-post-treatment.
Sensitivity analyses restricted to participants who completed the T2 assessment produced the same set of significant comparisons.
For the suicide attempts and NSSI GEE analyses, negative binomial models were used, treating the data as counts. All participants were included in the aggregated primary outcome analysis, while the sub-analyses of suicide attempts and NSSI only included participants with those behaviours at baseline.
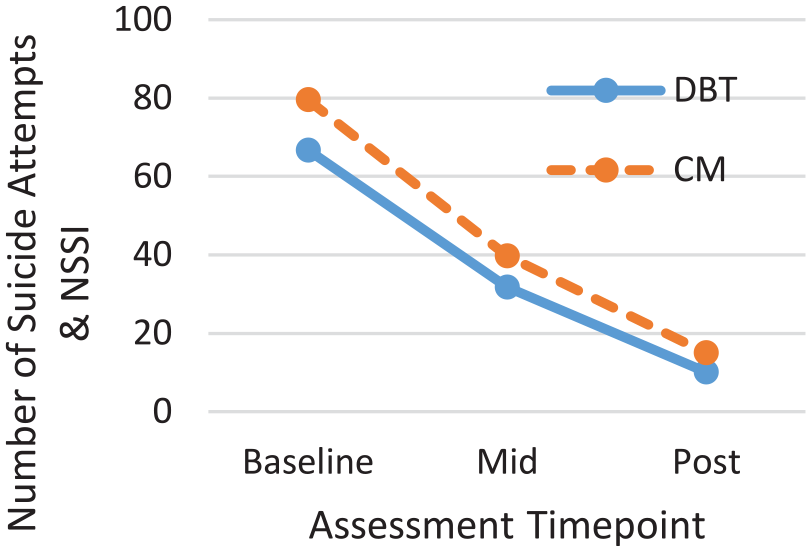
Mean number of suicide attempts and NSSI across T0-T2 time points by condition.
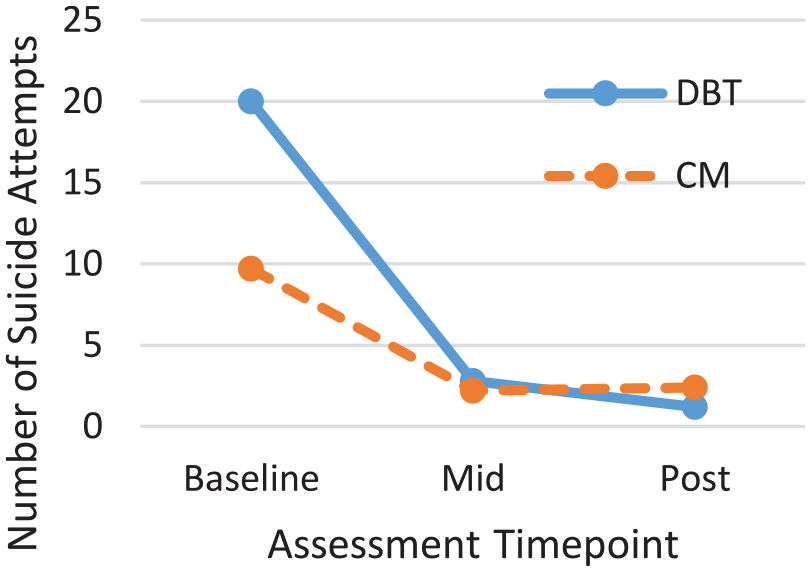
Mean number of suicide attempts across T0-T2 time points by condition.
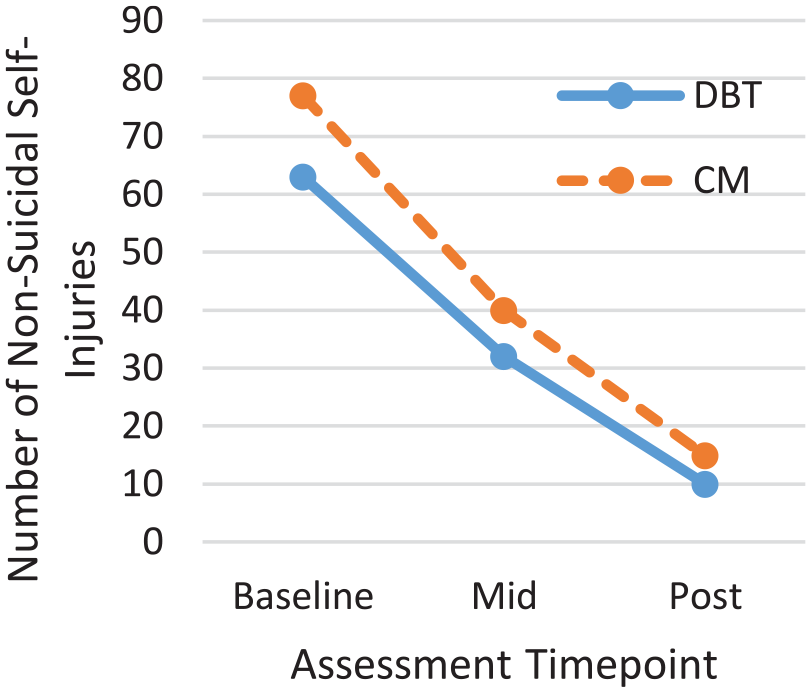
Mean number of episodes of NSSI across T0-T2 time points by condition.
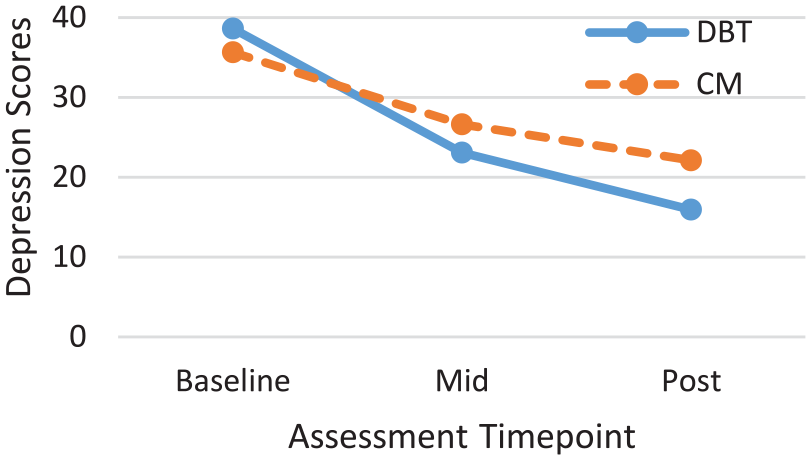
Depression severity scores (BDI-II) across T0-T2 time points by condition.
At baseline, 78% of the overall sample fell in the ‘severe’ BDI-II category (score of 29–63), comprising 83% of the DBT condition and 74% of the CM condition. At post-treatment, only 25% fell in the ‘severe’ category, comprising 18% of the DBT condition and 30% of the CM condition.
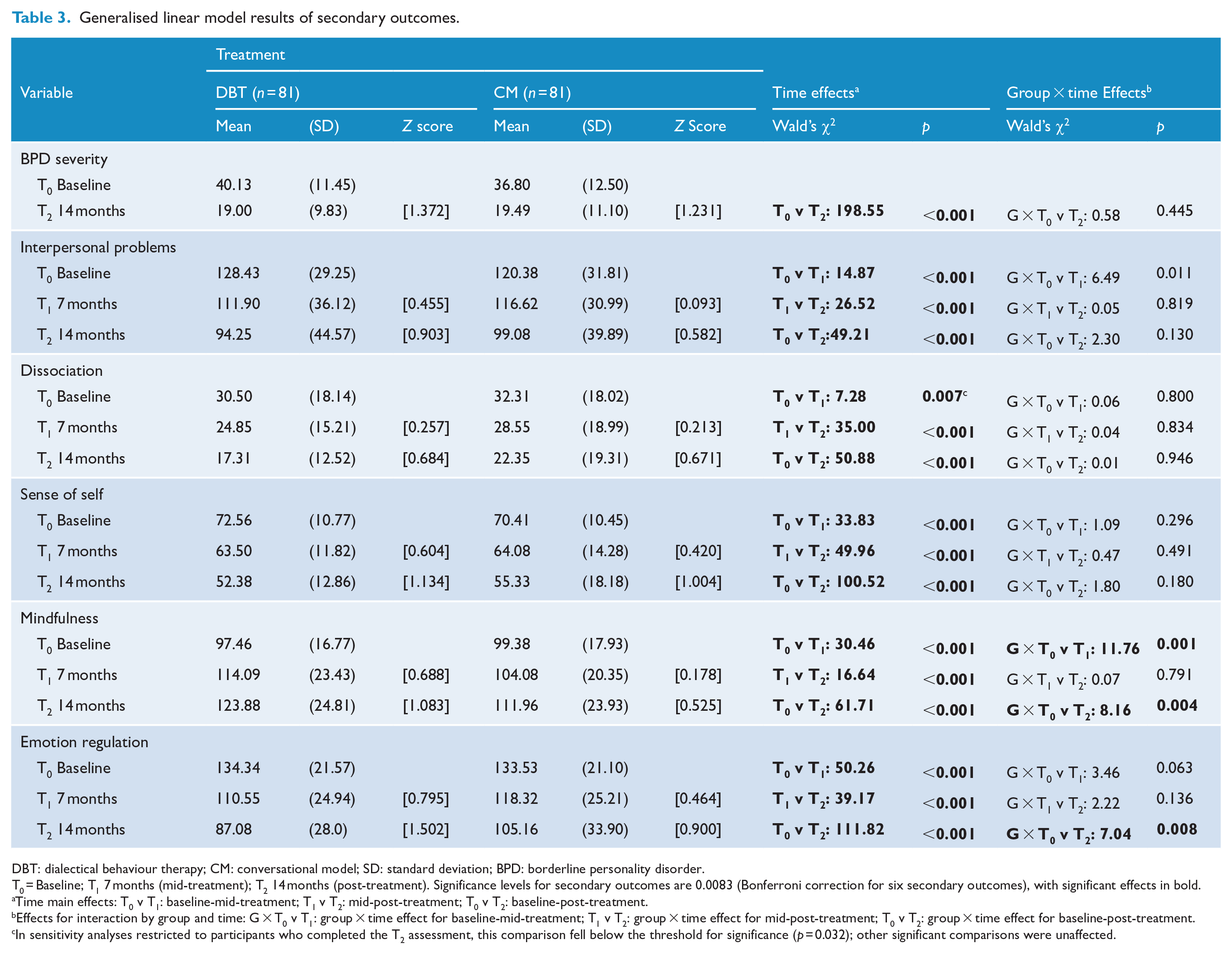
Analyses of all secondary outcomes showed significant improvement over time (see Table 3). Based on the absence of group × time interactions, there were no significant differences between DBT and CM with respect to changes in BPD severity, interpersonal problems, dissociation or sense of self. DBT showed a significant differential benefit between baseline to mid-treatment (Wald’s χ2 = 11.76, p = 0.001) and baseline to post-treatment (Wald’s χ2 = 8.16, p = 0.004) in improving mindfulness skills and from baseline to post-treatment in changes in emotion regulation skills (Wald’s χ2 = 7.04, p = 0.008).
Generalised linear model results of secondary outcomes.
DBT: dialectical behaviour therapy; CM: conversational model; SD: standard deviation; BPD: borderline personality disorder.
T0 = Baseline; T1 7 months (mid-treatment); T2 14 months (post-treatment). Significance levels for secondary outcomes are 0.0083 (Bonferroni correction for six secondary outcomes), with significant effects in bold.
Time main effects: T0 v T1: baseline-mid-treatment; T1 v T2: mid-post-treatment; T0 v T2: baseline-post-treatment.
Effects for interaction by group and time: G × T0 v T1: group × time effect for baseline-mid-treatment; T1 v T2: group × time effect for mid-post-treatment; T0 v T2: group × time effect for baseline-post-treatment.
In sensitivity analyses restricted to participants who completed the T2 assessment, this comparison fell below the threshold for significance (p = 0.032); other significant comparisons were unaffected.
Comparison of treatment completers and those who dropped out
Of those assigned to DBT, 45 (56%) completed the full 14 months of treatment, compared to 48 (59%) of those assigned to CM. Those who did not continue with treatment were encouraged to attend for assessments; however, only 36% completed their post assessment. In contrast, 98% of those who completed treatment completed their post assessment.
We conducted two-way analyses of variance (treatment group × treatment drop-out status) examining baseline differences and found only one significant interaction effect, F(1, 158) = 6.50, p = 0.012, for baseline BPD severity. Within the DBT group, those who dropped out had higher scores on the BPDSI (mean = 43.28, SD = 10.90) than those who completed treatment (mean = 37.60, SD = 11.37). The opposite pattern occurred in the CM group, with those who dropped out having lower scores (mean = 34.27, SD = 12.96) compared with those who completed treatment (mean = 38.53, SD = 13.43). Overall, time spent in treatment was comparable for participants in DBT (n = 81, mean = 10.38, SD = 4.49 months) and CM therapy (n = 81, mean = 10.59, SD = 4.60 months). Likewise, among participants who dropped out, time spent in treatment was comparable for DBT (n = 36, mean = 5.86, SD = 2.85 months) and CM therapy (n = 33, mean = 5.64, SD = 3.18 months; F(1, 67) = 0.96, p = 0.758).
Adherence
The average adherence score on the DBT Adherence Rating Scale was 4.1 (Linehan, 1993b) and 77% of sessions had a score of 4.0 or above. The average adherence score on the Newcastle Adherence Scale for Conversational Model was 3.9, and 99% of sessions had a score of 2 or above (the cut-off for adherence). For the 12 therapists providing both DBT and CM, 30 sessions of DBT and 30 sessions of CM were assessed on the scale for the alternative therapy, for example, DBT sessions were rated on the CM adherence scale and vice versa. All 60 sessions were identified as non-adherent, confirming that therapists were delivering the treatment the patient was randomised to and not blending the two therapies.
Discussion
This study is the first effectiveness study using a randomised design of DBT and CM for treatment of suicidal and NSSI behaviour and depression severity among persons with BPD. Consistent with our first hypothesis, we found that, on average, people who received either DBT or CM had significantly less suicidal behaviour and NSSI after 14 months of treatment. The other two hypotheses were not supported. It was predicted that DBT would reduce suicidal behaviour and NSSI more than CM. This was not the case. This was surprising, as DBT deliberately and explicitly targets suicidal behaviour and NSSI, whereas CM does not. However, these results are consistent with findings from CM studies that suicidal and NSSI improves without direct targeting (Korner et al., 2006; Stevenson et al., 2005; Stevenson and Meares, 1992). This result aligns with a previous RCT comparing DBT and a BPD adapted psychodynamic treatment (McMain et al., 2009) that found no significant differences between the two active treatments.
It was also hypothesised that CM would be associated with greater improvements in depression severity scores than DBT. Although both interventions were associated with significant reductions in depression severity scores over time, DBT was associated with statistically significantly lower scores than CM across the treatment year. This was also surprising, as previous studies of DBT have shown inconsistent impacts on depression severity scores (Stoffers et al., 2012). In contrast, CM in a previous wait list control study (Stevenson and Meares, 1992) showed substantial changes in depression severity. Numerous factors may explain why DBT performed superior to CM in reducing depression severity: in this study, depression was assessed based on self-report measures and these may present a different picture than clinician-administered scores; alternately, DBT may involve more behavioural activation which has a large amount of evidence in support of reducing depression (Ekers et al., 2014). This result provides evidence for DBT impacting on patient’s internal experience beyond purely behavioural problems.
For a range of secondary outcomes, in the domains of BPD severity, dissociation, interpersonal difficulties and sense of self, both treatment conditions contributed to significant improvements over time, with no significant differential changes between the therapies. These results are consistent with previous research when two active psychotherapies are compared with each other; there is usually no significant difference in outcome (Asarnow and Ougrin, 2017). DBT was superior to CM in improving mindfulness and emotion regulation scores. This is less surprising since these constructs are explicitly taught in DBT (Linehan, 1993c) and the wording in these measures uses the same language as that taught in DBT (Baer et al., 2004; Gratz and Roemer, 2004). However, it does suggest that in DBT, two key areas explicitly targeted do change in response to treatment.
The dropout rates in this study were comparable across the two treatments (41% for CM and 44% for DBT). Dropout rates in this study were higher than in the DBT efficacy studies (16% in Linehan et al.’s, 1991, original study and 25% in Linehan et al., 2006a), but similar to other independent trials of DBT (43% in Clarkin et al., 2007, 37% in Verheul et al., 2003, and 38% in McMain et al., 2009).
There was an interesting finding that those who dropped out of DBT had higher scores on BPD severity than those who completed treatment. The opposite pattern occurred for the CM group, such that those who dropped out had lower scores on BPD severity than those who completed treatment. It is not clear what it is about DBT that means there was higher drop-out rates for those who were more severe or correspondingly why those who were less severe would be more likely to drop out of CM. This is an important area for future investigation.
Strengths and limitations
There are many strengths to the current effectiveness study. The service had already been the setting of an RCT comparing 6 months of DBT with waiting list control (Carter et al., 2010). Therefore, the feasibility of running an RCT at this service had already been established. The sample size for the current trial was sufficiently large, relative to most previously published RCTs in the field of BPD, providing adequate power to examine differential changes across the primary and secondary outcomes. In their recent Cochrane review of psychological therapies for BPD, Stoffers et al. (2012) suggest ‘there is an urgent need for independent research endeavours’ (p. 77). The current trial goes some way to providing such evidence, given that no author is a treatment developer, nor have they worked clinically alongside the treatment developers. The co-principal investigators (C.J.W. and N.B.) are both trained in and deliver both models of therapy, and each is allegiant to one of the treatment models, as evidenced through training they provide (C.J.W. to DBT and N.B. to CM). This provides a counter-balance to prevent overall researcher allegiance (Luborsky et al., 1999).
Several elements in the trial were designed to reduce potential bias. Blindness of raters during assessments of outcome variables, and for adherence, reduced potential bias. By measuring adherence in both models, cross-contamination of one by the other could be excluded. Stoffers et al. (2012) have criticised the majority of trials of psychological therapies for BPD on the basis of the amount of professional contact, in that control group participants did not receive comparable amounts of professional attention. In this study, participants in the CM condition attended twice weekly individual therapy, while those in the DBT condition attended once weekly individual therapy and once weekly skills training. As such, the amount of attention received was comparable.
There are a number of limitations of the study. As evidenced by the baseline SDs in Table 2 for the recent suicidal and NSSI measures, there was a large degree of variation in these count-based indices, reflective of real-world variation in treatment-seeking samples. We dealt with this variability in two ways, by utilising negative binomial GEE analyses and by restricting the associated sub-analyses to participants who exhibited those specific behaviours at baseline; however, other approaches to such distributional and service-delivery challenges may be worth considering. On the other hand, therapies tend to be targeted towards reducing exhibited behaviours, rather than avoidance of potential future behaviours, particularly among individuals with long-standing conditions presenting to services; consequently, our sub-analyses are likely to have real-world relevance.
Ideally, a third arm, involving a minimal treatment control group, would have also been included. Without this, we are unable to eliminate the possibility that changes that occurred resulted from exposure to common external factors or regression to the mean. However, it was deemed unethical for persons at known risk of suicide to be denied an evidence-based psychotherapeutic treatment when one was available. The significant results found in this study are greater than what would have been expected if there had been no intervention; for example, in the DBT condition there was a standardised (z-score) change in depression severity from baseline to post-treatment of 1.48, and 0.91 in the CM condition (see Table 2), which clearly exceed the benefits previously reported for minimal treatment control conditions. We do not have information about the reasons why people dropped out of treatment and those who dropped out were much less likely to attend for their assessments than those who remained in treatment.
In most clinical trials, therapists only deliver one intervention or all therapists deliver both. In this study, some therapists delivered only one model, and some delivered both. This is in keeping with what would frequently occur in routine clinical settings but introduces some potential therapist bias.
Although accessing any other psychotherapy outside of the trial was prohibited, there was no control of psychiatric medications. The two treatment arms were stratified for antidepressant use at baseline. Other psychiatric medications were not controlled. However, as several guidelines for treatment of BPD (NCCMH, 2009; NHMRC, 2012) report little evidence that medication treatment in BPD is effective, this is not an important confounding factor.
Conclusion
Both DBT and CM were associated with significant improvements in suicide attempts and NSSI. The findings add to the evidence pool that DBT can be applied in routine clinical settings with good outcomes, outside of tightly controlled research settings. This study is the first evaluation of CM in a randomised design. On most outcomes, CM produced comparable results to DBT, with a similar level of fidelity and treatment retention. DBT was associated with significantly better improvements than CM for depression severity. Hence, DBT should be considered in preference to CM for individuals with co-morbid BPD and depression.
Footnotes
Acknowledgements
The authors wish to acknowledge the involvement of the study participants, without whom this research would not be possible. We are grateful to all the therapists in the trial: Agatha Conrad, Bridgette Lupton, Carla Walton, Christopher Willcox, Craig Hamilton, Dyani Nevile, Harsimrat Sandhu-Singh, Jane Middleby-Clements, Jennifer Koorey, Jodie Fleming, Joy Herron, Jude Robinson, Karen Calabria, Kath McPhillips, Katrina Bell, Kumudu Rhatnayaka, Leonie Funk, Leslie Pollock, Linda Bragg, Linda Kerr, Lisa Blackwell, Maria Walker, Marianne Ayre, Megha Mulchandani, Natalie McCall, Nick Bendit, Phoebe Webber, Stella Dyer, Subhra Bhattacharyya, Thomas Bellamy, Yolandie Goodyear and Zoe Walker.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: No external research funding was obtained for this project. We acknowledge the support of Hunter New England Mental Health Service and thank the Centre for Brain and Mental Health Research (University of Newcastle) for providing a small grant specifically to cover the cost of adherence coding.
Trial Registration
Australian New Zealand Clinical Trials Registry: ACTRN12612001187831.