
Abstract
Objective:
To examine child developmental outcomes in preschool-aged children exposed to antidepressant medication in pregnancy and compare their outcomes to children not exposed.
Method:
A prospective case-controlled study of 20 children exposed to antidepressants in pregnancy and 21 unexposed controls was available from the Victorian Psychotropic Registry. Child development outcomes at 4 years of age were assessed using the Wechsler Preschool and Primary Scale of Intelligence, third edition; the Movement Assessment Battery for Children; Behaviour Rating Inventory of Executive Functioning–Preschool; and the Child Behavior Checklist (1.5–5 years). Maternal depression was assessed using the Beck Depression Inventory-II in pregnancy and at four time points across infancy and early childhood.
Results:
Children exposed to antidepressants in pregnancy had no statistically significant differences compared to unexposed children on any of the measures of child development undertaken. There was a trend to slightly lower scores in motor development with a small effect size for two scales of the Movement Assessment Battery for Children: balance – Cohen’s d=0.36; aiming and catching – Cohen’s d=0.34.
Conclusions:
The finding of no effect on cognition and behaviour are consistent with other previous studies conducted with younger children. Likewise, the trend towards lower motor development is similar to earlier findings from this study and a number of other similar studies. Given this trend there is a need for future research that focuses on this area of development in older children using robust measures of motor development.
Introduction
Approximately 2% of Australian women use an antidepressant medication while they are pregnant (Lewis et al., 2012). Studies from other developed countries suggest that rates of antidepressant use in pregnancy are rising (Jimenez-Solem et al., 2013). Rates in the USA of antidepressant use are 7% or higher (Andrade et al., 2008; Cooper et al., 2007). However, there are relatively few studies that have examined the outcomes for children of such intrauterine exposure, and very few which have followed children beyond infancy (Gentile and Galbally, 2010). There are few studies that have followed a cohort of children where antidepressant use has been properly characterized in pregnancy up to 4 years of age and to date no studies have followed children beyond 6 years of age (Klinger et al., 2011; Mattson et al., 1999; Nulman et al., 2012). This leaves important clinical questions about the safety of antidepressant prescription during pregnancy unanswered.
The possibility of many of the potential adverse effects of antidepressant medication exposure on child development have mostly not been sufficiently examined and this was confirmed in a recent systematic review and meta-analysis (Ross et al., 2013). However, poor neonatal adaptation does appear to be a well-established effect and has been found in a large number of studies, confirmed in a systematic review and meta-analysis, and was also found in earlier data in the study of focus for this paper (Galbally et al., 2009; Grigoriadis et al., 2013). Whether this represents a vulnerability to later adverse neurological and developmental outcomes or is a transient state of discontinuation or toxicity is unclear without follow up of later child outcomes. A study that specifically followed up exposed neonates who had displayed poor neonatal adaptation and a control group of exposed infants who had not had poor adaptation found no significant difference in cognition but did find lower social abilities in early childhood, as measured on the Denver Developmental test (Klinger et al., 2011).
The studies that have looked at developmental outcomes for children exposed to antidepressants in pregnancy have not found effects on global cognitive outcomes; measures for this include the Bayley Scales of Infant Development, the Wechsler tests of cognitive development, and the McCarthy Scales (Galbally et al., 2011; Klinger et al., 2011; Mattson et al., 1999; Nulman et al., 1997, 2002, 2012). But it remains that studies examining longitudinal child developmental outcomes following antidepressant exposure in pregnancy are limited (Gentile and Galbally, 2010). However, within the limited literature there are now five studies that have found moderate differences in motor development (Casper et al., 2003, 2011; Galbally et al., 2011; Hanley et al., 2013; Mortensen et al., 2003). However, no study has used an observer rated and validated, specific measure of motor development.
In this current study we provide a further report from the Victorian Psychotropic Registry study, which used a prospective case–control design to examine cognitive development, executive function, motor development and behaviour at 4 years of age in a group of children exposed to antidepressants in pregnancy and an unexposed control group.
Materials and methods
The Victorian Psychotropic Registry study recruited 61 participants in early pregnancy commencing in 2004. This comprised of 32 antidepressant exposed cases and 29 matched controls who were neither depressed nor on antidepressant medication. The antidepressants included 27 women on selective serotonin reuptake inhibitors (SSRIs), three women on serotonin and noradrenaline reuptake inhibitors (SNRIs), one woman on a tricyclic antidepressant (TCA) and one woman on a noradrenergic and specific serotonergic antidepressant (NaSSA). Of these participants, one control had a stillbirth and two antidepressant cases ceased antidepressants prior to delivery. As these were all singleton pregnancies the child participant numbers are the same as maternal participants. Further details of recruitment and findings postpartum and at 18 months of age are contained in previous publications (Galbally et al., 2009, 2011; Lewis et al., 2010).
The Mercy Health Human Research Ethics Committee approved this study. A written informed consent statement was obtained from each adult participant. Women were excluded on the grounds of substance abuse, intellectual disability, and serious physical and psychiatric illness requiring inpatient admission. Inclusion criteria included currently pregnant and English proficiency.
The study had six waves for data collection: pregnancy, delivery, 1 month postpartum, 18 months, 4 years and then 5 years of age. At Wave 5, undertaken when children were 4 years of age, a total of 41 participants remained: 20 cases and 21 controls. This attrition represents a loss of 32% of the original sample over the 5 years of follow up from pregnancy to 4 years of age and is examined further in the results.
Measures
Maternal characteristics and birth outcomes
At pregnancy, delivery, 1 month postpartum, 18 months and 4 years of age a purpose-designed questionnaire was used to assess demographics, and alcohol, tobacco and illicit substance use, prescribed medications, maternal stress and coping.
Neonatal discontinuation symptoms
Within 1 week of delivery the details of birth outcomes and complications including symptoms of poor neonatal adaptation were recorded (Galbally et al., 2009). Discontinuation symptoms were rated within 1 week of delivery based on nine items identified from previous studies (Galbally et al., 2009). For the current analysis these symptoms were initially combined using principle components factor analysis with varimax rotation, which provided two clear factors accounting for 44.2% and 15.7% of the variance, respectively. The item loading on these factors showed that the first factor represented CNS symptoms such as tremor, crying, yawning and sneezing and the second factor weighted heavily on gastrointestinal symptoms such as diarrhoea and vomiting. Standardized factor scores were saved for each factor and used in analysis.
Fetal antidepressant exposure
Within the above purpose-designed questionnaire, a specific item was used to assess current antidepressant use at each assessment point. Each participant was asked if they were currently taking an antidepressant, and, if so, to select from a list of common medications. They were also asked to indicate dosage and when they had commenced the medication.
Perinatal maternal depression
In pregnancy, after delivery, at 1 month postpartum, 18 months postpartum and at 4 years depressive symptoms were assessed using the Beck Depression Inventory, second edition (BDI-II). The BDI-II is a 21-item self-report measure assessing the presence and severity of depressive symptoms. It is a highly reliable measure with established construct validity. The coefficient alpha for outpatients is 0.92 and the test-retest reliability 1 week apart showed a correlation of 0.93 (Beck, 1988).
Child development at 4 years of age
Children were assessed on average at 4 years and 1 month (standard deviation: 2 months) by a trained and experienced neuropsychologist using the Wechsler Preschool and Primary Scale of Intelligence, third edition (WPPSI-III) and the Movement Assessment Battery for Children (Movement ABC-2). The neuropsychologist was blinded to the status of participants. Mothers were asked to complete the Behaviour Rating Inventory of Executive Functioning–Preschool (BRIEF-P) and the Child Behavior Checklist (CBCL).
The WPPSI-III measures intellectual functioning in specified cognitive domains: Verbal IQ, Performance IQ and Processing Speed. The WPPSI-III also provides a Full Scale IQ score measuring general intellectual ability. It is regarded as the gold standard for assessing cognitive ability with tests available from 2 years of age to adulthood. The Movement ABC is a clinician administered test of child gross and fine motor development between 3 years and 16 years (Henderson et al., 1992). The assessment consists of eight tasks assessing three areas of motor development: manual dexterity, aiming and catching (ball skills) and balance (static and dynamic balance).
The BRIEF-P is a parent proxy rating scale designed to specifically measure the range of behavioural manifestations of executive function in preschool-aged children. It is one of the few measures available which specifically examines executive functioning in preschool-aged children. The BRIEF-P consists of 63 items, which were completed by the mother (Isquith et al., 2005). The measure provides scores on several subscales (Inhibit, Shift, Emotional Control, Working Memory and Plan/Organize), as well as four combined indices (Inhibitory Self-Control Index (ISCI), Flexibility Index, Emergent Metacognition Index and Global Executive Composite Index). These scales measure difficulties with self-regulation, and difficulty inhibiting impulses, modulating emotions, adapting to change, sustaining working memory and planning and organizing problem-solving as compared to the subjects’ peers. Thus, higher scores indicate evidence of poorer executive function.
Child behaviour was measured using the revised Child Behavior Checklist 1.5–5. This widely used measure provides a measure of the behavioural and emotional problems of young children as reported by their parents (Achenbach and Ruffle, 2000). The CBCL is a reliable, valid and widely used measure of children’s competencies and problem behaviours as reported by parents, and provides scores on externalizing, internalizing and total behaviour problem scales.
Results
Maternal and child socio-demographic characteristics
Demographic characteristics for participants at pregnancy, 1 month postpartum and 18 months have been reported in previous publications (Galbally et al., 2009, 2011; Lewis et al., 2010). At recruitment there were no statistically significant differences on maternal age, years of education, and alcohol and smoking in pregnancy between exposed and control groups, suggesting that the groups were well matched. Table 1 presents a comparison of demographics, birth outcomes and depression scores for those retained and lost to the study. Marital status and gestational age at delivery in weeks were the only group difference to reach statistical significance. On examining the latter as a dichotomous group, premature delivery at less than 37 weeks of gestation compared to term delivery, there was no significant difference between groups.
Demographic and birth outcomes from baseline by groups retained and lost at Wave 5 (4 years of age).
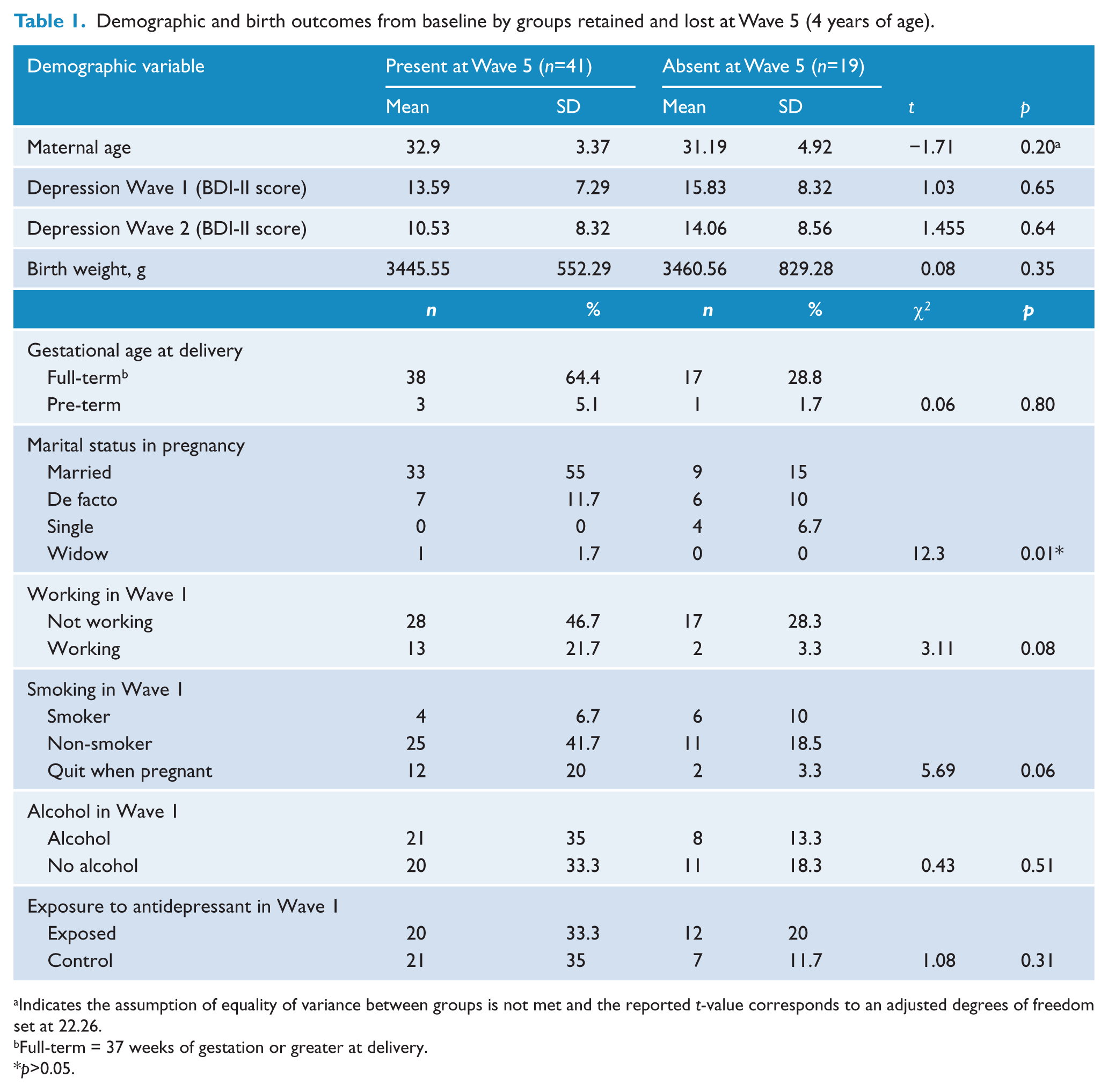
Indicates the assumption of equality of variance between groups is not met and the reported t-value corresponds to an adjusted degrees of freedom set at 22.26.
Full-term = 37 weeks of gestation or greater at delivery.
p>0.05.
Poor neonatal adaptation and child developmental outcomes
At 4 years of age there were 20 exposed children retained within the study and of these nine had experienced one or more symptoms of poor neonatal adaptation as neonates and 11 children exposed to antidepressants in pregnancy had not displayed discontinuation symptoms as neonates. The presence or absence of any neonatal discontinuation symptoms were initially examined using independent t-tests between those with and without discontinuation symptoms on the Full Scale IQ, Movement ABC Total score and BRIEF-P Global Executive Composite score; the CBCL Internalizing score and Externalizing score indicated no statistically significant difference between the two groups. However, when the two factors were examined (CNS discontinuation symptoms and gastrointestinal discontinuation symptoms), the CNS symptoms were statistically significantly correlated with the Movement ABC Balance total score. These results are presented in Table 2. There were no other significant findings with any other key child developmental outcomes.
Pearson’s correlations for factor scores for neonatal discontinuation symptoms and child development outcomes at 4 years (n=40).
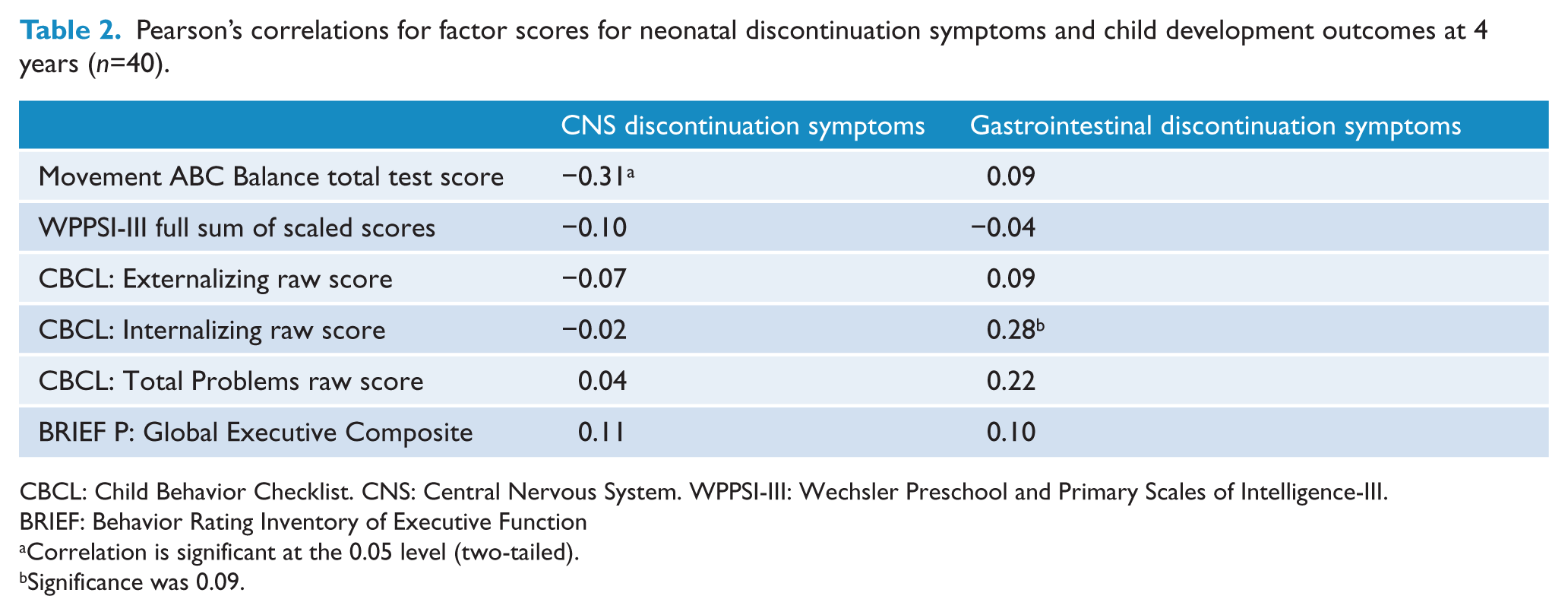
CBCL: Child Behavior Checklist. CNS: Central Nervous System. WPPSI-III: Wechsler Preschool and Primary Scales of Intelligence-III. BRIEF: Behavior Rating Inventory of Executive Function
Correlation is significant at the 0.05 level (two-tailed).
Significance was 0.09.
Child developmental outcomes
Tables 3 and 4 provide the mean differences for children’s performance on the WPPSI-III and scores on the BRIEF-P. There were no statistically significant differences on scales of the WPPSI-III Full Scale IQ or the BRIEF-P Total score. Trends were noted towards higher scores for exposed children were noted on subscales of the WPPSI-III (Matrix Reasoning) and Executive Function, measured by the BRIEF-P, and lower scores on the Processing Speed Quotient scale of the WPPSI-III in exposed children. The PSQ is comprised of two subscales: Coding and Symbol Search. The first is associated with motor development and the later with language development. An independent sample t-test was undertaken to examine differences between children exposed to antidepressants and controls on the Coding and Symbol Search subtests of the WPPSI-III. There was no statistically significant difference for exposed children compared to controls of either subtest; however, scores were lower for exposed children on Coding (mean=12.55 (SD=8.53)) compared to controls (mean=14.43 (SD=5.69)) than for Symbol Search (exposed children: mean=10.37 (SD=5.28); controls: mean=11.05 (SD=5.93)) – therefore the difference being greater for Coding than for Symbol Search. When Cohen’s d effect sizes were calculated, the effect size for Coding was Cohen’s d=0.26, representing a small effect size, whereas for Symbol Search this was only Cohen’s d=0.12. This suggests that the trend towards lower PSQ scores in antidepressant exposed children is a result of lower Coding scores, which may be an indication of psychomotor functioning.
Child cognitive outcomes in those children exposed to antidepressants in pregnancy compared to control children.
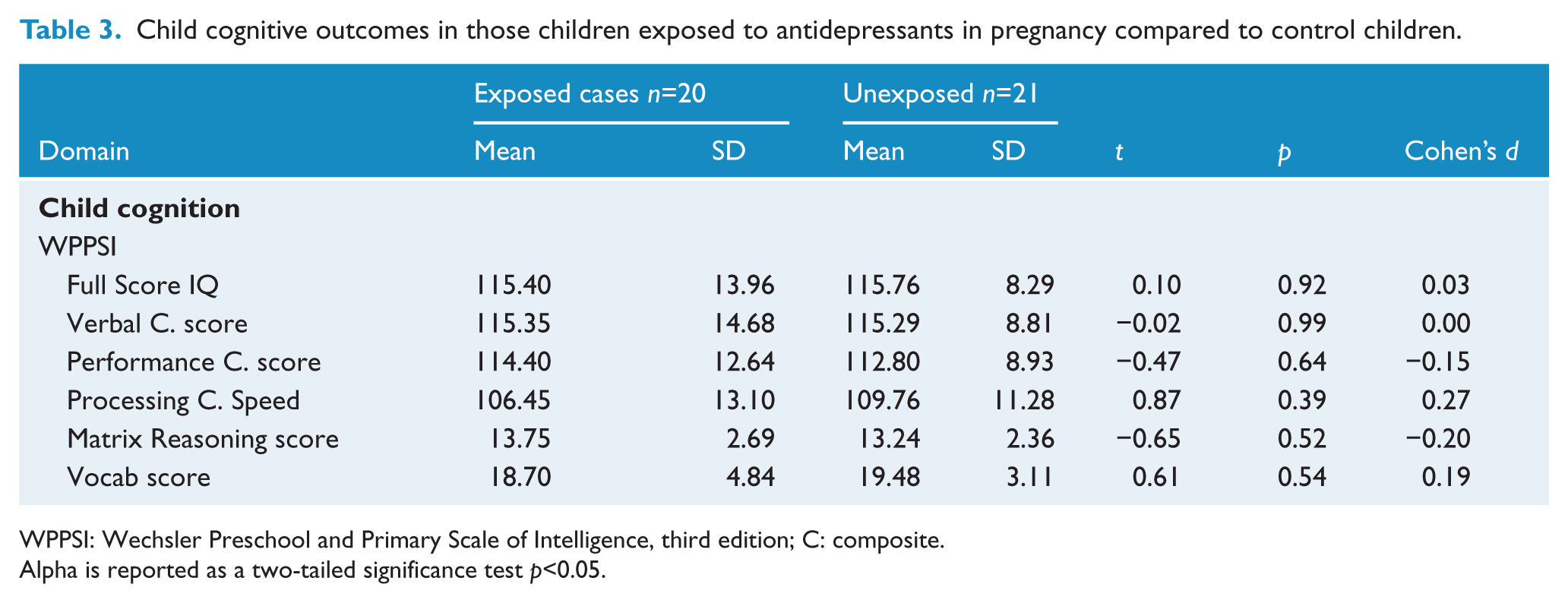
WPPSI: Wechsler Preschool and Primary Scale of Intelligence, third edition; C: composite.
Alpha is reported as a two-tailed significance test p<0.05.
Child executive function outcomes in those children exposed to antidepressants in pregnancy compared to control children.
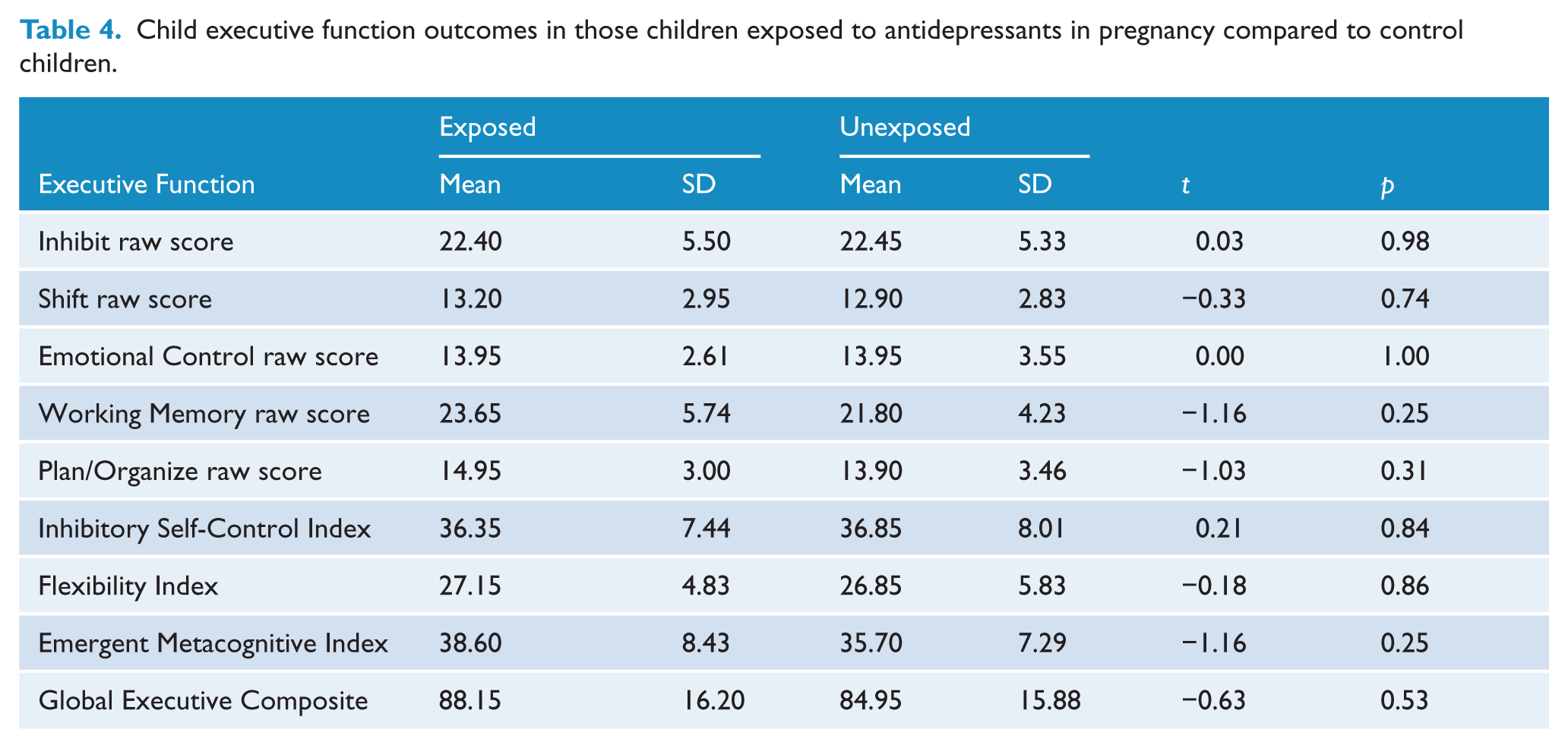
Table 5 provides the mean differences for children’s performance on Movement ABC and scores on the measure of child behaviour (CBCL). For Movement ABC, both the Aiming and Catching and the Balance scales showed lower mean scores for exposed children than controls, reaching a moderate effect size of Cohen’s d=0.34 and d=0.36, respectively. The total score for Movement ABC was also lower in the exposed children, although with a small effect size of Cohen’s d=0.21. These results failed to reach statistical significance. The mean percentile for exposed children on Aiming and Catching was 51.20 (SD=34.56) and for controls it was 64.60 (SD=27.76). For Balance the mean percentile for exposed children was 61.60 (SD=23.14) and for controls it was 70.57 (SD=18.74). Further analysis was undertaken controlling first for the amount of exposure to maternal depression in pregnancy, and then for gestational age at delivery. Neither covariate changed the findings. We then examined the aiming and catching percentile score, which did place some of the exposed sample in the ‘at risk’ group defined as equal or below the 15th centile. There were no control participants who had scores below the 15th centile on Aiming and Catching, whereas, in contrast, three exposed participants were below the 15th and two of these were below the 5th centile. These children would be considered at high risk for a motor co-ordination disorder. Fisher’s exact probability test was calculated in order to compare the number who fall into the clinical range on motor problems for each group and this showed no significant difference given the very small numbers identified to be in the ‘at risk’ group.
Child motor development and social and emotional development in those exposed to antidepressants in pregnancy and controls.
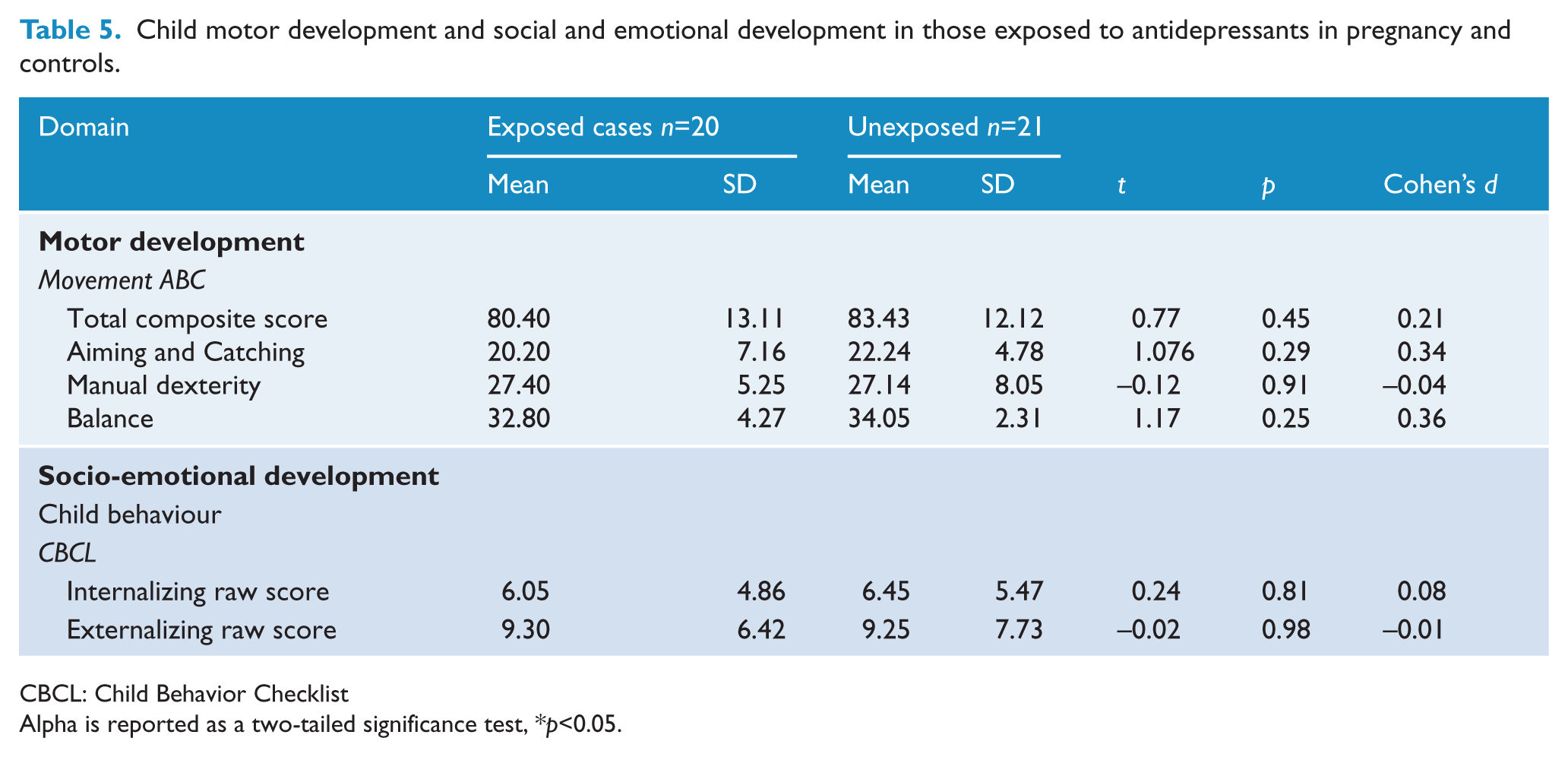
CBCL: Child Behavior Checklist
Alpha is reported as a two-tailed significance test, *p<0.05.
The CBCL mean differences for Internalizing and Externalizing scores between groups were not statistically significant.
Maternal depression and child developmental outcomes
Table 6 reports the correlation coefficients for maternal depression scores, as measured by the BDI-II, in pregnancy, after delivery and at 4 years postpartum in relation to child developmental outcomes at 4 years of age. The significant associations found were that WPPSI-III and BRIEF-P were both significantly associated with both Internalizing and Externalizing scores. However, maternal depression was not significantly associated with any of the child developmental outcomes. These findings did suggest that maternal depression across pregnancy, infancy and early childhood is significantly correlated.
Maternal depression and child outcomes for the full sample.
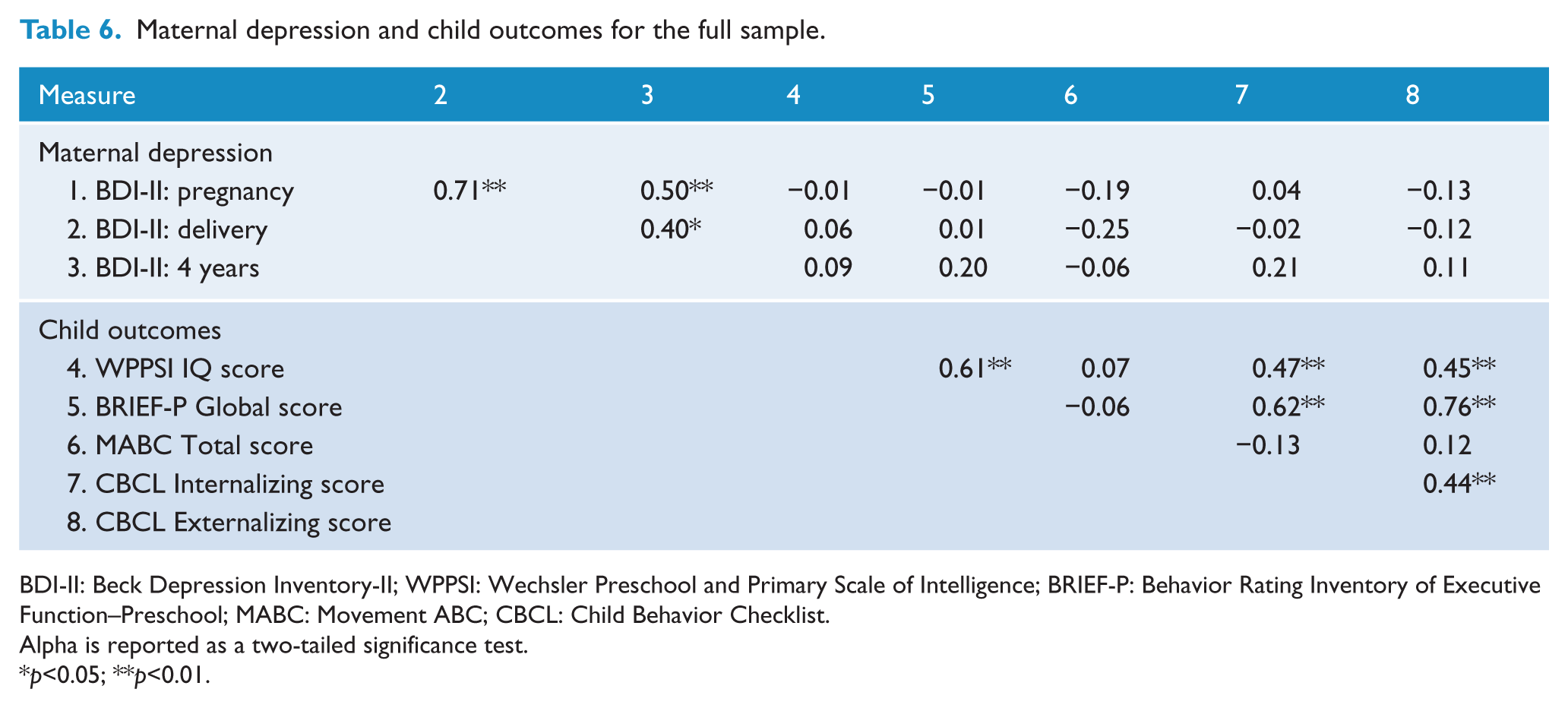
BDI-II: Beck Depression Inventory-II; WPPSI: Wechsler Preschool and Primary Scale of Intelligence; BRIEF-P: Behavior Rating Inventory of Executive Function–Preschool; MABC: Movement ABC; CBCL: Child Behavior Checklist.
Alpha is reported as a two-tailed significance test.
p<0.05; **p<0.01.
Discussion
The findings of this study build on the previous findings from the Victorian Psychotropic registry, which at 18 months of age found subtle differences in motor development in children exposed to antidepressants (Galbally et al., 2011). The current findings show tentative but far from conclusive evidence that this may continue. Notably, the current findings are not statistically significant within a small sample and if ‘real’ seem at worst to be very subtle differences, which appear to become less pronounced with age.
Poorer motor development in exposed children has been found in an additional four separate studies to date (Casper et al., 2003, 2011; Hanley et al., 2013; Mortensen et al., 2003). The psychomotor scale of the Bayley Scales of Infant Development was used in three of these studies and, of note, also in the earlier wave of this current study. The fourth study to identify poorer motor development used the Boel – a screening measure undertaken by child health nurses. No other study to date has investigated motor development in 4 year olds and none have used a specific neuropsychological measure of motor development such as the Movement ABC. The interesting finding in comparing the differences in motor development within this study at 18 months and then in the same children at 4 years of age, is that at this older age the gap between groups appears to have narrowed. Whether this is due to a washout effect as children develop, or due to the more accurate measure of motor development used at 4 years of age is unclear. These findings highlight the importance of following children well into childhood to examine developmental outcomes after antidepressant exposure in the fetal period.
The reason why long-term follow up is required is that the effects on child development from in utero exposure to antidepressants may only be apparent in older age groups. However, it should also be noted that findings in early life may also resolve as a child matures (Galbally et al., 2012; Mayes and Ward, 2003). Furthermore, the concept that exposure may be either detrimental or potentially protective to development within the context of maternal depression is supported by both animal and human studies, some of which have found poorer outcomes following exposure to antidepressants, while other studies show enhanced development in exposed offspring (Lee et al., 2001; Rayen et al., 2011; Weikum et al., 2012). This study found that matrix reasoning was slightly higher in exposed than in control children, although not reaching a statistically significant difference, with the higher scores on matrix reasoning representing better functioning on this test. However, it was also found that exposed children had slightly higher scores on the BRIEF-P, representing poorer executive functioning.
A further challenge of examining child development in the context of pregnancy exposure is the potential for exposure from any stage of pregnancy to have later effects on offspring. Research into stress and anxiety exposure in pregnancy has shown that both the sex of offspring and the timing of these exposures is crucial, resulting in either negative or positive effects on later child development (Lewis et al., 2014; O’Connor et al., 2002; Pawluski et al., 2012). However, a significant limitation of this study is the numbers retained at 4 years of age, making analysis of individual agents, more sophisticated statistical analysis and an examination of timing of exposure and sex not viable. While the attrition rate of 32% is well within those expected for longitudinal studies, and especially one recruiting a clinical group, this study remains small (Fischer et al., 2001; Gustavson et al., 2012; Tambs et al., 2009). The previous studies that have found motor development effects using the Bayley Scales of Infant Development in younger children have likewise been small – ranging from 31 to 51 exposed participants and a smaller number of controls (Casper et al., 2003, 2011; Hanley et al., 2013). This suggests that recruiting and retaining a prospective cohort of children exposed to antidepressants in pregnancy and a control group is a challenging area of research. Future consideration of research into factors which aid recruitment and retention of participants in longitudinal research may be beneficial to researchers in this area.
The serotonin system is a complex system, which during fetal development plays a wide role in the developing nervous system. As such, exposures to agents that alter serotonin levels for the developing fetus have the theoretical potential to have wide ranging effects on neurodevelopment. If other examples, such as the antiepileptic drug sodium valproate or alcohol, are considered, then these effects may not be apparent until later stages of child development or even into adolescence and adulthood. It is reassuring that there are now a number of studies that have examined global cognitive function in children exposed to antidepressants in pregnancy and the consistent findings have been of no difference to control children. This study adds to this by also finding no difference on a comprehensive measure of cognitive function: WPPSI-III. In addition, this study specifically examined executive function, which is important in longer-term educational and developmental outcomes (Zelazo, 2008). However, reassuringly this study showed no statistically significant differences between exposed children and controls on executive function.
The limitations of this study include the lack of an unmedicated, depressed, second control group, the inclusion of three groups of antidepressants, and also the overall numbers within this study.
Child behavioural and early emotional development, as measured by the CBCL, were neither associated with maternal depression nor were there differences found in exposed children compared to controls. The CBCL has now been used in several studies of antidepressant exposure and most have found no difference for exposed children (Misri et al., 2006; Nulman et al., 2012; Oberlander et al., 2007). While one study did find higher Internalizing scores in exposed children, when maternal mood in pregnancy and postpartum and Apgar scores were controlled for, SSRI exposure was no longer a significant predictor of Internalizing scores (Oberlander et al., 2010).
Studies that can answer questions about child developmental outcomes following antidepressant exposure are challenging; they require the recruitment of a large enough sample to examine individual agents, a second control group of unmedicated, depressed, pregnant women to adequately account for the effects of exposure to maternal depression and they need to follow up the sample for long enough so any developmental outcomes that might only be apparent in older children can be measured. In addition, to study potentially subtle effects requires robust, comprehensive developmental measures undertaken by skilled, trained professionals. This type of study requires commitment by researchers over a lengthy period of time and funding bodies to support longitudinal studies.
Studies suggest the primary concern for women and the reason for ceasing antidepressant use in pregnancy is fear of the unknown effects exposure may have on the fetus (Einarson, 2005; Ververs et al., 2006). The onus is now on researchers in the important area of health to deliver accurate and robust findings so women and clinicians are able to make informed choices about the treatment of depression in pregnancy. However, to date, findings on child development outcomes are reassuring and these findings continue to reassure clinicians and women.
Footnotes
Acknowledgements
The authors wish to thank Helena Sandahl, Yasna Blandin de Chalain, Amanda Williamson, Elaine Kelly, Mercy Hospital for Women, Deakin Centre for Mental Health and Wellbeing, and the women and children who participated in this study.
Funding
This research was funded by a Neuroscience Research Grant, Pat and Toni Kinsman Postnatal Depression Grant and grants from Pfizer, Lundbeck and Wyeth.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.