
Abstract
Background:
Throughout pregnancy, women are at an increased risk of depression, with prevalence estimates between 6.5% and 18%. Global prevalence of antenatal antidepressant use is considerably lower at 3%.
Objective:
The present study determined the proportion of women taking antidepressants across pregnancy in New Zealand. We investigated whether variation exists across age bands, area-level deprivation and ethnicities, and identified how many women experienced unmedicated depression.
Method:
Antenatal data (n = 6822) consisted of primarily third-trimester interviews conducted with mothers participating in Growing Up in New Zealand, a longitudinal study investigating child development. Women were asked about their antidepressant intake during pregnancy and assessed on antenatal depression symptoms using the Edinburgh Postnatal Depression Scale. Antidepressant use data were also compared to population-level data from Statistics New Zealand’s Integrated Data Infrastructure.
Results:
Antidepressant prevalence across pregnancy was 3.2%, with a 2.7% prevalence in trimester one and 2.6% following the first trimester. There was no significant difference in usage within age bands and area-level deprivation quintiles. Ethnicity-specific data revealed that Pasifika and Asian ethnicities had the lowest antidepressant use, and New Zealand Europeans the highest. The rate of unmedicated depression, where women met the Edinburgh Postnatal Depression Scale criteria for significant depressive symptoms but did not receive antidepressants during pregnancy, was 11.8%, indicating that antenatal depression treatment may be inadequate. Greater rates of unmedicated depression were seen for younger women (
Conclusions:
Antenatal antidepressant use in New Zealand follows global prevalence estimates and highlights possible undertreatment of antenatal depression in New Zealand. Future research including other treatment types (e.g. behavioural therapy) is needed to evaluate whether undertreatment occurs across all treatment options.
Introduction
Pregnancy is a time of increased vulnerability to the onset or recurrence of depression, with an estimated global prevalence of antenatal depression between 6.5% and 18% (Gavin et al., 2005; Okagbue et al., 2019). Recognised risk factors cover a combination of psychosocial and socioeconomic influences, such as environmental stressors, adverse life experiences, young maternal age, and being part of an ethnic minority group (Biaggi et al., 2016; Underwood et al., 2017).
Untreated antenatal depression has been linked to numerous detrimental effects (Andersson et al., 2004; Jarde et al., 2016; Underwood et al., 2017). For the mother-to-be, these include increased nausea and vomiting, prolonged sick leave, and increased likelihood of developing postpartum depression (Andersson et al., 2004; Underwood et al., 2017). In terms of pregnancy outcomes, untreated antenatal depression was found to increase the risk of preterm birth and low birth weight (Jarde et al., 2016).
Clinical guidelines for antenatal depression follow those of depression management at other life stages, with additional considerations for the pregnancy and the foetus (Kirby et al., 2019; Molenaar et al., 2018). For mild depression, psychological interventions such as cognitive behavioural therapy (CBT) are recommended. For moderate to severe or treatment-resistant depression, guidelines advise that antidepressants can be used in combination with psychological interventions, following a thorough risk-benefit analysis and maternal consent (Kirby et al., 2019; Malhi et al., 2021; Molenaar et al., 2018). Selective serotonin reuptake inhibitors (SSRIs) are the preferred first-line treatment option, with the exception of paroxetine (Kirby et al., 2019; Molenaar et al., 2018).
Studies that have investigated outcomes of antidepressant use during pregnancy have yielded inconsistent results, with many presenting limitations such as poor study design, lack of control for underlying illnesses, recall bias and selection bias, which makes it difficult to draw conclusions regarding empirical results (Grigoriadis et al., 2014; Huang et al., 2014; Roerecke et al., 2013; Udechuku et al., 2010). In their review, Udechuku et al. (2010) concluded that antidepressant use in pregnancy was relatively safe, though antidepressant use appears to slightly increase the risk of preterm birth, neonatal adaptation syndrome, congenital cardiac malformations (specific to paroxetine) and possibly persistent pulmonary hypertension of the newborn (PPHN).
Consequently, physicians are reluctant to prescribe antidepressants to women during pregnancy (Bilszta et al., 2011). This hesitancy is reflected in the relatively low prevalence of pregnancies exposed to antidepressants (3%) (Molenaar et al., 2020) and in the large-scale discontinuance of antidepressants consistently observed across pregnancy (Jimenez-Solem et al., 2013; Petersen et al., 2011; Ramos et al., 2007; Zoega et al., 2015). For those who do continue to use antidepressants across pregnancy, the most recurrent predictors are low income and older maternal age (⩾35 years) (Jimenez-Solem et al., 2013; Ramos et al., 2007).
In New Zealand, antenatal antidepressant use has become more prevalent, rising from 3.1% in 2005 to 4.9% in 2014 (Donald et al., 2021). Age-specific dispensing showed a pattern of increased antidepressant use with increasing age (Donald et al., 2021). Concerning ethnicity, NZ Europeans are dispensed antidepressants at a considerably higher rate than any other ethnicity (Donald et al., 2021). In 2014, 4.7% of women who identified as NZ Europeans/Other were prescribed antidepressants in their first trimester, compared to 2.4% of Māori, 1.0% Pasifika and 0.5% Asians (Donald et al., 2021). These demographic differences are consistent with antidepressant dispening patterns in the NZ adult population more broadly (Wilkinson and Mulder, 2018).
The potential threats that antenatal depression and antidepressant use during pregnancy pose to pregnancy outcomes and child development illustrate why early detection of depression and access to NZ-specific data is vital. Therefore, we aimed to identify the prevalence of antenatal antidepressant use in NZ. Furthermore, we aimed to identify antidepressant use across trimesters, ethnicities, age groups, and deprivation levels using data from mothers from the Growing Up in New Zealand (GUiNZ) birth cohort study. Our study also compared these results to population-level data for pregnant New Zealand women, obtained through Statistics New Zealand’s Integrated Data Infrastructure (IDI), to evaluate how closely aligned the study results are in relation to the overall population of pregnant New Zealand women.
The literature also points to a large gap between antenatal depression prevalence and antidepressant use in pregnancy, indicating that many women live with untreated antenatal depression. Undertreatment is especially likely as empirical evidence shows that many women receive no formal treatment for antenatal depression, medical or otherwise (Kelly et al., 2001; Marcus et al., 2003). The links between untreated antenatal depression and numerous detrimental mother and child outcomes illustrate a need to establish the magnitude of this undertreatment (Andersson et al., 2004; Jarde et al., 2016; Underwood et al., 2017). Therefore, this study also aimed to identify the proportion of mothers from GUiNZ experiencing antenatal depression symptoms and not receiving antidepressants. We made the following predictions. First, antidepressant prevalence among pregnant New Zealand women would be in line with the international prevalence estimates (Molenaar et al., 2020). Second, antidepressant use would substantially decrease across trimesters, consistent with global trends (Donald et al., 2021; Jimenez-Solem et al., 2013; Petersen et al., 2011; Ramos et al., 2007; Zoega et al., 2015). Third, women aged ⩾ 35 years would show the highest percentage of antidepressant use across pregnancy, consistent with previous research, as well as evidence that antidepressant use increased with increasing age in NZ (Donald et al., 2021; Jimenez-Solem et al., 2013; Ramos et al., 2007; Donald et al., 2021; Wilkinson and Mulder, 2018).]. Fourth, there would be a positive association between antidepressant use and deprivation, in line with evidence that low income is a predictor of greater antidepressant use across pregnancy
Methods
Participants and general procedure
The participants in this study were mothers from Growing Up in New Zealand; a longitudinal study with several data collection waves intended to investigate six interrelated domains that impact child development. These include health and wellbeing, psychological and cognitive development, education, family and whānau (extended family), culture and identity, and neighbourhoods and societal context (Morton et al., 2015). All participating mothers lived within a geographical area covering the three contiguous District Health Board (DHB) regions Auckland, Counties-Manakau and Waikato (this area covers around one-third of the NZ population) and had due dates between 25 April 2009 and 25 March 2010 (Morton et al., 2013). Participants were similar to national birth statistics in terms of maternal age, ethnicity and socioeconomic indicators (Morton et al., 2014). Ethics approval was provided by The NZ Ministry of Health Northern Y Regional Ethics Committee, and all participating women gave written informed consent. For a more comprehensive account of cohort study design and sample recruitment, see Morton et al. (2013).
The antenatal data were collected through face-to-face computer-assisted interviews (all in English) taking place in the participants’ homes. These were conducted for 5664 women during their third trimester of pregnancy. The remaining 1158 women completed the antenatal interviews after their children were born. All 6822 participants were included in the analysis for this current study.
Measures
Antidepressant use
Women in the GUiNZ sample were asked whether they took antidepressants during the first trimester and after the first trimester. Women were then categorised as taking antidepressants and not taking antidepressants for the following time periods: in the first trimester, after the first trimester, any time in pregnancy.
Antenatal depression
The Edinburgh Postnatal Depression Scale (EPDS) was used to measure antenatal depression symptoms (Cox et al., 1987). The scale screens for depression through 10 self-report items that assess the cognitive and affective aspects of depression. Although the tool was created to measure postnatal depression, it is valid and frequently used to screen for antenatal depression (Cox et al., 1996; Jairaj et al., 2019; Kozinszky and Dudas, 2015). An EPDS score of 13 or higher indicates that an individual has significant antenatal depressive symptoms (total maximum score is 30, with each item score being 0–3) (Waldie et al., 2015). The reported sensitivity and specificity for major depression in pregnancy using this cut off are 0.83 and 0.90, respectively (National Collaborating Centre for Mental Health, 2014).
Unmedicated depression
Using the antidepressant and EPDS data, a composite variable indicating unmedicated depression was created within the GUiNZ sample and categorised as follows: unmedicated depression, medicated depression and neither. Unmedicated depression indicated that a woman met the EPDS criteria for significant depressive symptoms but did not receive antidepressants during pregnancy. Medicated depression signified antidepressant use during pregnancy regardless of EPDS score. Neither indicated that the woman did not meet the EPDS criteria for significant depressive symptoms nor received any antidepressants during pregnancy.
Sociodemographic variables
Self-prioritised/main maternal ethnicity was coded into five Level 1 Statistics New Zealand categories (Didham, 2005): NZ European, Māori (indigenous population in NZ), Pasifika, Asian, and Other (including the ‘Middle Eastern, Latin American and African’ Level 1 category). For descriptive results, both total response ethnicity and self-prioritised ethnicity were reported. Total response ethnicity allows for individuals to belong to one or more ethnic groups, a common occurrence in NZ (Didham, 2005). Self-prioritised ethnicity is defined as the main ethnicity identified by the mother. For analyses, self-prioritised ethnicity was used so as to comply with the assumption of independence.
Maternal age was self-reported and classified into three age bands: ⩽ 24 years, 25–34 years and ⩾ 35 years. Area-level deprivation was established through geocoding of address data using the NZDep2006 Index (Salmond et al., 2007). The measure was divided into quintiles, where quintile 1 represented the least deprived- and quintile 5 the most deprived areas.
Data analysis
Comparison to NZ population data
Population-level data for pregnant NZ residents was used to assess whether our sample was reflective of the overall NZ population of pregnant women. The population-level data were obtained through Statistics New Zealand’s IDI. The IDI is a comprehensive database with administrative and survey data on NZ-specific people and households that are de-identified and linked at the individual level. For a more detailed account of the IDI, see Milne et al. (2019). Within the IDI, all women with at least one successful pregnancy for the fiscal year 2009/2010 (i.e. July 2009 to June 2010, roughly corresponding to the year of GUiNZ births) were identified through birth records from the Department of Internal Affairs (DIA). Activity in key datasets, including health, tax, education and injury claims, was then used to determine if the women were likely to be in the resident NZ population (Gibb et al., 2016; Zhao et al., 2018). With this method, the estimated resident population should fall within 2% of the official resident population (Gibb et al., 2016). The IDI also enabled us to obtain relevant demographic information on the women, including total response ethnicity and age, as well as area-level deprivation measured by the NZDep 2013 index (Atkinson et al., 2014). Estimated date of conception was back-calculated from the child’s gestational age at birth provided through the DIA birth records. From these estimations, approximate trimester dates were calculated. To allow for a fair comparison with GUiNZ, we defined this period as trimester one and after trimester one. Trimester one was defined as 13 weeks from conception, and after trimester one was defined as the period between the end of trimester one and birth.
In addition, we linked data from the Ministry of Health community pharmaceutical dispensing collection to the resident pregnant population to detect antidepressant medication dispensing during pregnancy. The medications included SSRIs (citalopram, fluoxetine, paroxetine, escitalopram and sertraline), monoamine oxidase inhibitors (MAOIs)/reversible inhibitors of monoamine oxidase A (RIMAs) (tranylcypromine, phenelzine and moclobemide), a serotonin and noradrenaline reuptake inhibitor (SNRI) (venlafaxine), tricyclic antidepressants (TCAs) and related agents (amitriptyline, nortriptyline, dosulepin, doxepin, clomipramine, imipramine, trimipramine and maprotiline), a tetracyclic antidepressant (TeCA) (mianserin), and a noradrenergic and specific serotonergic antidepressant (NaSSA) (mirtazapine). Recorded by the NZ Pharmaceutical Management Agency (PHARMAC), the pharmaceutical collection comprises information on subsidised prescription medication dispensed by community pharmacists.
Antidepressant use across pregnancy was calculated by dividing the number of women who indicated that they had used antidepressants anytime in pregnancy by the total study population. The same calculation was performed for antidepressant use during the first trimester and following the first trimester of pregnancy. In the current study, these proportions are presented as percentages.
GUiNZ-specific analyses
Using data from the GUiNZ sample, we ran cross-tabulations between each sociodemographic variable and the proportion of women using antidepressants across pregnancy. From these proportions, we performed chi-square tests to investigate any association between antenatal antidepressant use and the sociodemographic variables.
Separate cross-tabulations were also run between the unmedicated depression variable and each of the sociodemographic variables. For the resulting proportions, we ran chi-square tests to establish the link between this variable and the sociodemographic variables.
Analyses using GUiNZ data were carried out using R version 3.6.1 and R studio version 1.2.1335. For the chi-square analyses, statistical significance was set at an alpha level of .05. Data management and analyses using IDI data were conducted using SAS Enterprise Guide version 7.1
Results
Descriptive results
Table 1 shows that the proportions of NZ Europeans (61.7%) and Māori (18.5%) in the GUiNZ sample were slightly lower compared to pregnant women in the overall NZ population (66.9% and 24.1%, respectively). Conversely, Pasifika, Asian and Other ethnicities have a somewhat greater representation in the GUiNZ sample than in the pregnant NZ population. This is likely due to the GUiNZ sample being taken from DHB regions with a high prevalence of Asian and Pasifika ethnic groups (Mehta, 2012; Ministry of Health, 2016). However, the distribution of ethnicities is generally comparable across the GUiNZ sample and the population. We also measured self-prioritised ethnicity in the GUiNZ sample; 53.0% identified as NZ European, 14.0% as Māori, 14.7% as Pasifika, 14.7% as Asian and 3.5% as Other. For age-bands, the proportion of 25- to 34-year-old’s in the GUiNZ sample (55.5%) is slightly higher than in the NZ population of pregnant women (51.2%), though largely, the sample has a similar distribution in age bands relative to the NZ population. For area-level deprivation, the sample shows a comparable distribution to the NZ population.
Sociodemographic characteristics of GUiNZ participants and the overall NZ population of pregnant women.
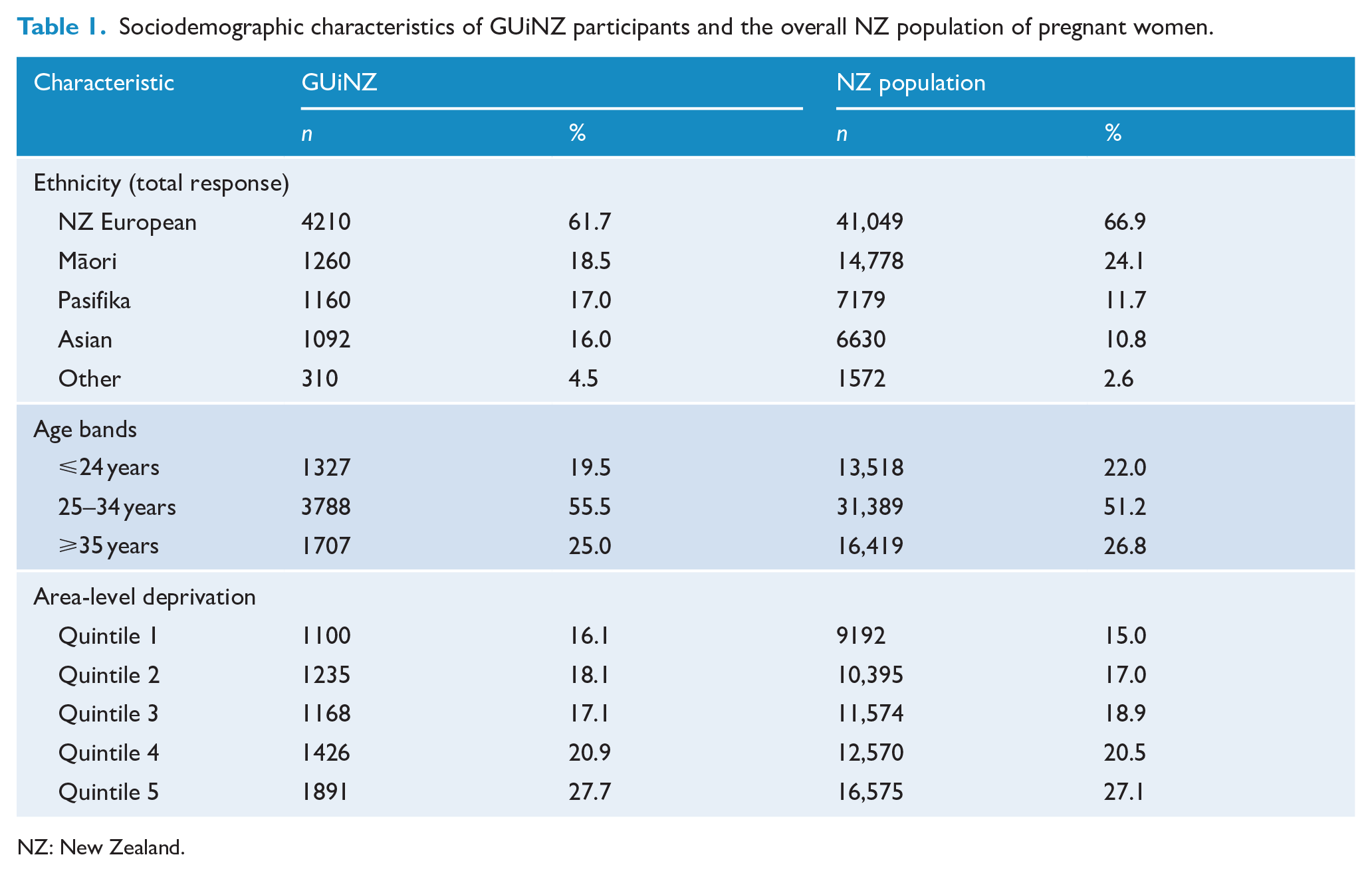
NZ: New Zealand.
Comparing GUiNZ and the NZ population on antenatal antidepressant use
The IDI database results for the fiscal year 2009/2010 showed a prevalence of 4.4% for antenatal antidepressant use in the pregnant NZ population overall, comparatively higher than the 3.2% identified for the GUiNZ sample (see Figure 1). While Figure 1 also shows that the prevalence in trimester one and after trimester one in the IDI sample (3.2% and 3.1%, respectively) was greater than that compared to GUiNZ (2.7% and 2.6%, respectively), both samples showed a relatively stable prevalence in antidepressant use across this period.
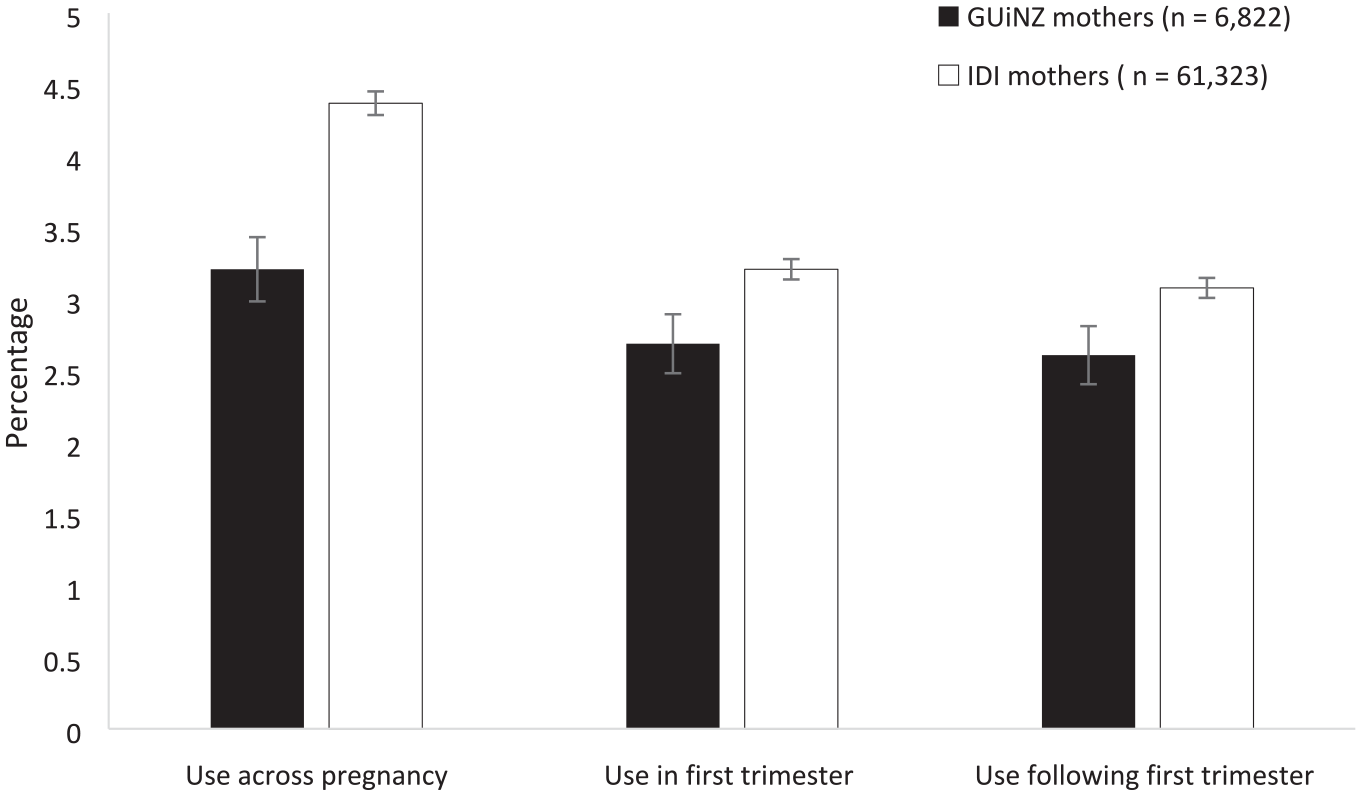
GUiNZ and IDI antenatal antidepressant use overall and by pregnancy stage.
In Figure 2, we present a comparison of the two samples by sociodemographic variables. As the IDI data for ethnicity is based on total response ethnicity, we chose to use total response ethnicity for the GUiNZ sample so that fair comparisons could be made.
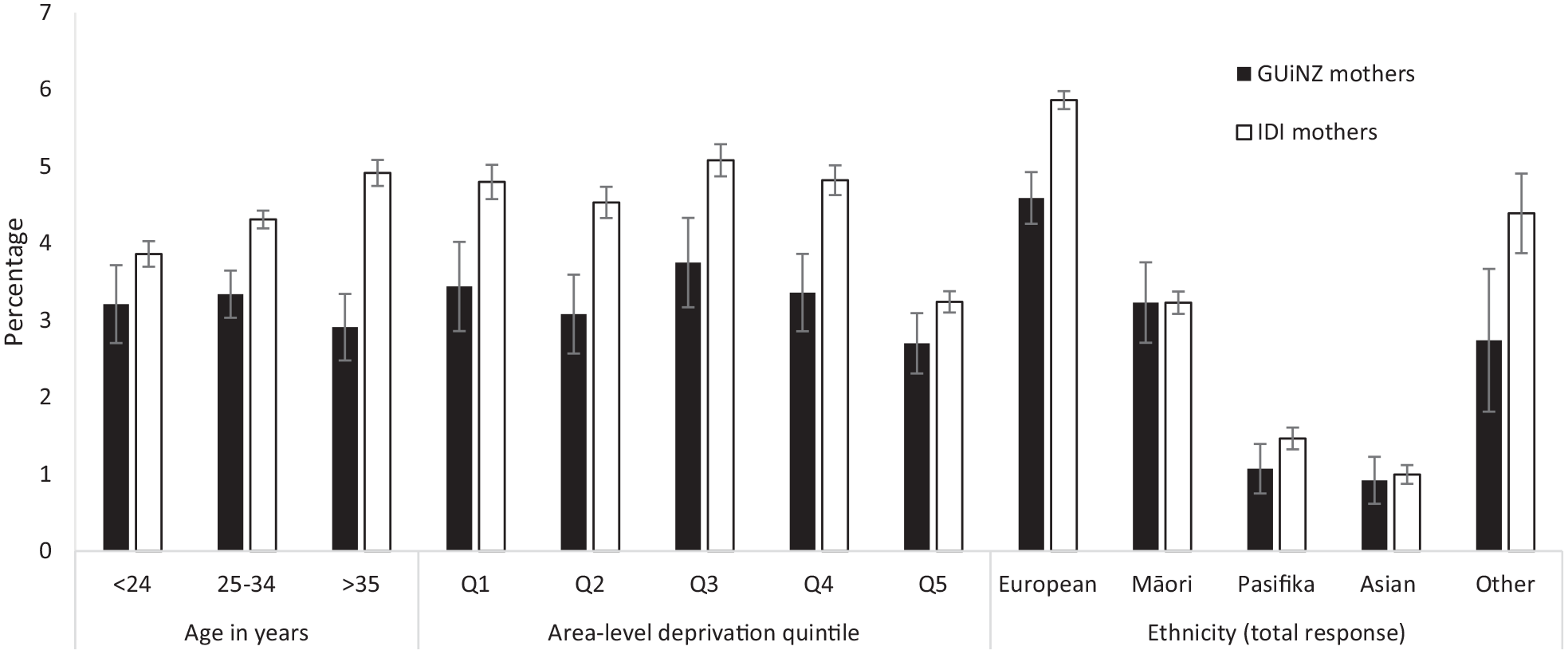
GUiNZ and IDI antenatal antidepressant use by sociodemographic variables.
Figure 2 reveals similar trends for antidepressant use across the two groups, though with higher use reported across most groups in the IDI compared to GUiNZ. A similar trend of slightly lower use in the age band < 24 years compared to the 25–34 years age category was present in both the IDI and GUiNZ. For the oldest age group (>35 years), the IDI and GUiNZ differed. Whereas dispensing in the IDI showed that this age band received the greatest proportion of antidepressants, the GUiNZ sample revealed that the age band received a slightly lower number of antidepressants than the two other age bands. For area-level deprivation, both the GUiNZ and the IDI data showed a markedly lower antidepressant use for the women living in high deprivation areas. However, this disparity is more pronounced in the IDI data. Classified by ethnicity, the two samples showed a similar pattern where Europeans had the highest antidepressant prevalence, with Pasifika and Asian showing the lowest prevalence.
Antidepressant intake in the GUiNZ sample
Chi-square tests showed that there was no significant difference in the proportion of women that received antidepressants during pregnancy across age bands χ2(2, N = 6175) = 0.632, p > 0.05 and area-level deprivation χ2(2, N = 6173) = 2.729, p > 0.05. However, analysis of antenatal antidepressant use based on self-prioritised ethnicity showed significant variation χ2(4, N = 6803) = 61.08, p < 0.001. Women of European ethnicity had the highest antidepressant use during pregnancy (4.8%), followed by Other (2.7%), Māori (2.4%), Pasifika (0.9%) and Asian (0.7%).
Unmedicated antidepressant intake in pregnancy for GUiNZ
In our sample, 11.8% of women were experiencing unmedicated antenatal depression (see Figure 3). Figures 3 also reveals significant disparities in rates of unmedicated depression across age bands χ2(4, N = 6175) = 97.075, p < 0.001, ethnicities χ2(8, N = 6165) = 241.72, p < 0.001, and area-level deprivation χ2(4, N = 6173) = 93.68, p < 0.001. Prevalence of unmedicated depression was highest for women aged 24 and under at 20.6%. In contrast, women aged 35 and over experienced the lowest rate of unmedicated depression at 7.8%. Classification by ethnicity also revealed considerable differences. Women of Pasifika ethnicity had the highest rate of unmedicated depression at 23.1%, followed by Māori women at 16.9%. The lowest rate of unmedicated depression was reported for women of European ethnicity at 7.5%. Unmedicated depression trends by area-level deprivation showed an increase in the prevalence of unmedicated depression with increasing deprivation level; quintile 5 areas experienced unmedicated depression at the highest rate (17.8%), followed by quintile 4 (11.4%), quintile 3 (10.0%), quintile 2 (8.1%) and quintile 1 (7.9%) deprivation areas.
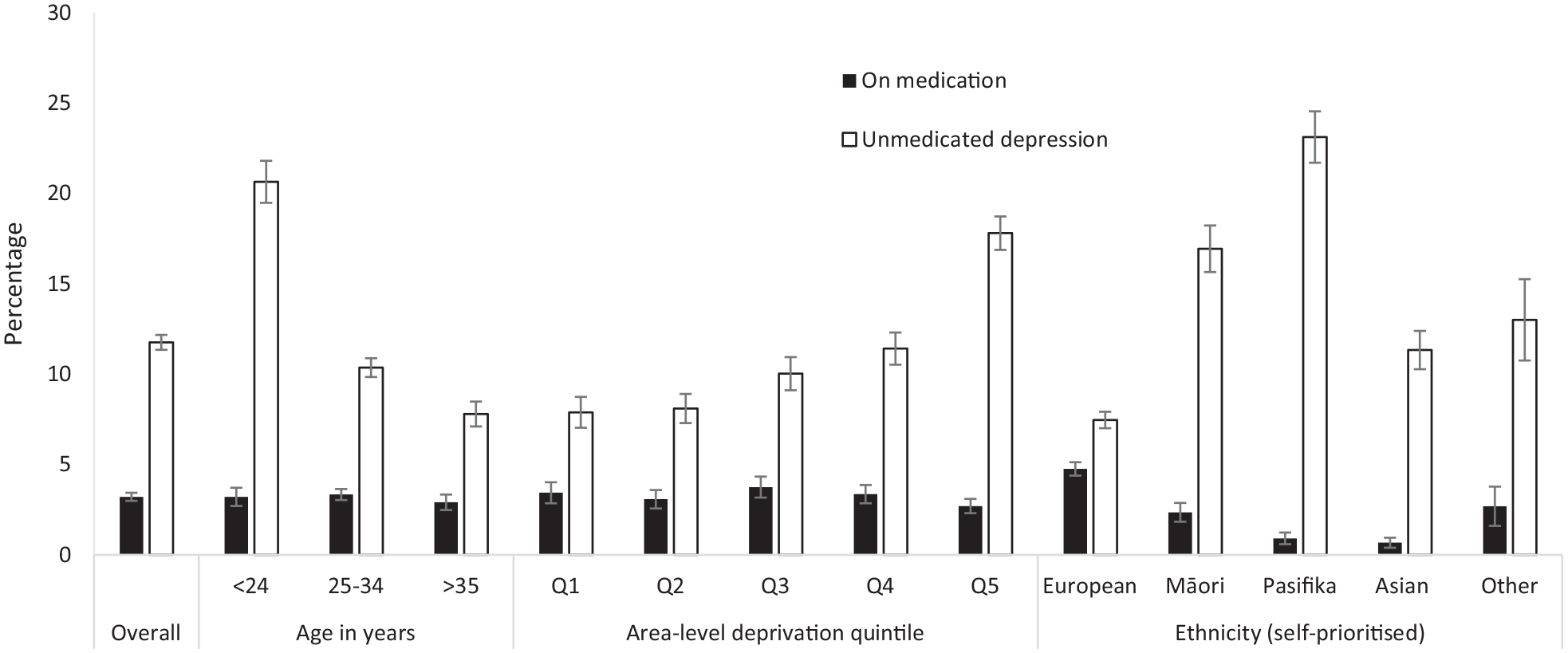
Medication and unmedicated overall and by sociodemographic groups.
Discussion
We explored antenatal antidepressant use in NZ through the analysis of data from Growing Up in New Zealand. In line with our hypothesis and parallel with international estimates, the prevalence of antidepressant use in our sample was 3.2% (Molenaar et al., 2020). Antidepressant use remained relatively stable across pregnancy in our sample, decreasing marginally from 2.7% in the first trimester to 2.6% following the first trimester. Previous studies have shown large-scale cessation during pregnancy, thought to be related to an unwillingness to prescribe antidepressants due to potential risks their use poses to the foetus (Grigoriadis et al., 2014; Huang et al., 2014; Roerecke et al., 2013; Udechuku et al., 2010). Compared to previous research, the reduction in use observed in this study is negligible (Donald et al., 2021; Jimenez-Solem et al., 2013; Petersen et al., 2011; Ramos et al., 2007; Zoega et al., 2015). However, while we observed stable use over pregnancy in our sample, we were unable to determine what the pre-pregnancy dispensing prevalence was like nor whether there was a reduction from trimesters two to three, as this information was not collected. Had this information been available, we might have seen a clearer pattern in antidepressant cessation during pregnancy.
Comparing the GUiNZ sample with the population data in the IDI showed that antenatal antidepressant prevalence was higher across all variables in the NZ population. The overall prevalence of antidepressant use in the pregnant NZ population was 4.4%. However, it is important to note that we worked with two different kinds of data (dispensing data in the IDI and self-report data from GUiNZ), which may contribute to these differences in antenatal antidepressant prevalence. With dispensing data, it is impossible to conclude whether mothers took all antidepressants issued. Moreover, with self-report data, there may be a risk of under-reporting medication intake, particularly due to the sensitive nature of mental illness and antidepressant use (Krumpal, 2013). In addition, the IDI data were related to women across all 20 of NZ’s DHB regions, whereas women from the GUiNZ sample were contained within only three of these regions. These regions also have a higher proportion of Pacific and Asian women, which are ethnic groups that show a lower prevalence in antidepressant dispensing (Donald et al., 2021; Mehta, 2012; Ministry of Health, 2016; Wilkinson and Mulder, 2018). Another factor that could influence the two datasets differently is that antidepressants can be used to treat disorders beyond depression, particularly various anxiety disorders (Shatzberg, 2000). Women in the GUiNZ study were not asked if they were taking medication for anxiety. Consequently, some antidepressant use in the sample might have gone unreported, as women may have been taking antidepressants for anxiety and were unaware that their medication was classified as an antidepressant.
As a result of the differences in data collection between the GUiNZ sample and the IDI data, the comparison aimed to look for consistency of trends, not prevalence. For the IDI data, women aged 35 and over had the highest antidepressant usage, whereas for the GUiNZ sample, this age group reported the lowest antidepressant usage. However, the difference in antidepressant use across age bands was not statistically significant in the GUiNZ sample. With all other trends being comparable, we feel confident that the GUiNZ sample is generally representative of the patterns observed in the overall pregnant NZ population, even if differences are less pronounced.
Inconsistent with our hypothesis, antenatal antidepressant use did not differ at a statistically significant level across age bands. This result deviates from empirical evidence that has identified older maternal age as a predictor of increased antidepressant use across pregnancy, and from the trend of increased antidepressant use with increasing age reported in the overall NZ population (Donald et al., 2021; Jimenez-Solem et al., 2013; Ramos et al., 2007; Wilkinson and Mulder, 2018). Women who become pregnant at a younger age are at greater risk of antenatal depression (Biaggi et al., 2016). Consequently, our results could reflect disproportionate use of antidepressants compared to rates of depression across age bands. Exploration of the unmedicated depression variable reveals support for this suggestion, as mothers in the youngest age band (
Ethnicity-stratified antidepressant use revealed a pattern similar to the one identified in NZ pregnant women and in the overall NZ population (Donald et al., 2021; Wilkinson and Mulder, 2018). Women of NZ European ethnicity used antidepressants at a notably higher rate than other women, particularly Māori, Pasifika and Asian mothers. Underwood et al. (2017) showed that women of Pasifika and Asian ethnicities within the GUiNZ cohort were at increased risk of antenatal depression when compared to NZ European women. Therefore, it is unlikely that higher rates of antenatal depression among NZ European women produced higher rates of antidepressant use observed within this ethnic group. The results from the unmedicated depression variable also illustrate that this is unlikely to be the case, as Pasifika women had the highest rate of unmedicated depression, followed by Māori and Asian ethnicities.
Unexpectedly, classification by area-level deprivation did not uncover significant differences in antidepressant use. Research evidence has shown that low income is associated with increased antenatal antidepressant usage and increased likelihood of antenatal depression (Biaggi et al., 2016; Jimenez-Solem et al., 2013; Ramos et al., 2007). Similar to the age band variable, this implies that one group, women living in high deprivation areas, likely have a higher overall rate of depression. Thus, disproportionate antidepressant use compared to rates of depression could also be occurring within the deprivation variable. Indeed, the unmedicated depression variable shows that rates of unmedicated antenatal depression increased as deprivation levels increased.
In line with our hypothesis, the unmedicated variable revealed that a large proportion of women were experiencing depression without receiving antidepressants. Whereas 3.2% of women reported antidepressant use, 11.8% of pregnant women reached the threshold for depression but did not report taking antidepressants. These results indicate that undertreatment may be prevalent in NZ, placing mothers and infants at increased risks of poor health outcomes (Andersson et al., 2004; Jarde et al., 2016; Underwood et al., 2017). It is possible that some women with unmedicated depression may have been receiving other forms of psychiatric treatment; however, prior research has shown that a large proportion of women do not receive any form of treatment for antenatal depression (Kelly et al., 2001; Marcus et al., 2003). We did not have access to information about non-pharmacological treatment prevalence within the sample; therefore, further investigation incorporating other treatment types is needed to understand the extent of undertreatment that may be occurring.
Disparities between rates of unmedicated depression between socioeconomic variables elucidate a range of determinants for unmedicated antenatal depression in NZ. In terms of age, young pregnant women (
Pregnant women of Pasifika ethnicity showed a prevalence of unmedicated depression more than three times that of expectant NZ Europeans. Māori and Asian women were also significantly more likely to have unmedicated depression than NZ Europeans. Further research is needed into what may be underlying these differences.
Previous research has indicated stigma as a major deterrent in help-seeking behaviour related to mental illness across Asian cultures (Kishore et al., 2011; Lauber and Rössler, 2007). There is also evidence of a preference for non-pharmacological treatment options within non-European ethnic groups, including spiritual healing methods in Asian cultures as well as whānau and community-based treatment approaches in those of Māori and Pasifika ethnicity (Agnew et al., 2004; Kishore et al., 2011; Lauber and Rössler, 2007; Metcalfe et al., 2013; Norris et al., 2011).
However, while differential treatment preferences across ethnic groups may explain the differences in medication prevalence, it does not elucidate why we are observing a higher prevalence of unmedicated depression in non-European ethnic groups. Data from The New Zealand Health Study of 2017/2018 indicate that socioeconomic factors could be influencing rates of unmedicated depression, at least among those of Māori and Pasifika ethnicities (Ministry of Health, 2019). The study found that adults and children of Māori and Pasifika ethnicities were over two times more likely to not fill prescriptions due to cost than NZ Europeans (Ministry of Health, 2019). This indicates that barriers to accessing healthcare may be underlying some of these ethnic differences.
In terms of deprivation, prevalence of unmedicated antenatal depression increased as deprivation level increased. Jatrana et al.’s (2010) study on access to prescription medication in NZ identified the cost of medication as a likely factor in shaping these results. In their research, living in a high deprivation area was a significant predictor of avoiding filling prescriptions due to cost. The possible socioeconomic costs of accessing medication for certain ethnic groups and those living in high deprivation imply that there may be an unmet need for mental health support in some pregnant women. It may be beneficial for healthcare professionals interacting with pregnant women to screen for depression during pregnancy and ensure that adequate support and treatment options are available, particularly for women with an increased risk.
We are aware that our study may have some limitations. Our research has the potential for recall bias, as the antenatal interviews took place primarily in the third trimester of pregnancy, with some also conducted following birth. Further, data collection for the GUiNZ sample occurred through self-report measures, leaving room for social desirability bias, particularly due to the sensitive nature of the questions and the possible stigma associated with mental illness (Kishore et al., 2011; Krumpal, 2013; Lauber and Rössler, 2007). However, we are confident that our findings are generally reflective of the overall NZ population as a result of our comparison with the IDI data.
The limited ability to determine the extent of undertreatment without access to non-pharmacological treatment data presents an additional limitation. For this reason, we suggest that future studies should include both medical and non-pharmacological data to better assess the magnitude of undertreatment. As distinct adverse pregnancy outcomes have been linked to specific antidepressants taken during pregnancy, such as paroxetine and congenital cardiac defects, we make a further recommendation for future research to elucidate the distribution of antenatal antidepressant use for classes of- and specific antidepressants (Grigoriadis et al., 2014; Huang et al., 2014; Kirby et al., 2019; Molenaar et al., 2018; Roerecke et al., 2013; Udechuku et al., 2010).
The current study has several strengths. Our sample was ethnically and socioeconomically diverse and large. In addition, access to the IDI data allowed for a comparison between the GUiNZ sample and the overall pregnant NZ population. Thus, we are confident that our sample is not strongly biased in terms of demographics, as general trends were consistent. A unique additional strength of our study was the ability to go beyond antenatal antidepressant prevalence to look at rates of unmedicated depression.
Overall, our study demonstrated that antenatal antidepressant use in NZ follows global estimates, and we were able to examine demographic differences in antidepressant use. More significantly, we observed high rates of unmedicated depression, indicating an unmet need for adequate mental healthcare during pregnancy. This is particularly true for mothers of young maternal age, women that are part of an ethnic minority group and those living in high deprivation areas. These findings warrant further investigation to establish the magnitude of undertreatment and underlying causes of unmedicated depression, in order to reduce health inequities and improve overall maternal and infant outcomes.
Footnotes
Acknowledgements
The study has been designed and conducted by the Growing Up in New Zealand study team, led by the University of Auckland. The authors acknowledge the contributions of the original study investigators: Susan M.B. Morton, Polly E. Atatoa Carr, Cameron C. Grant, Arier C. Lee, Dinusha K. Bandara, Jatender Mohal, Jennifer M. Kinloch, Johanna M. Schmidt, Mary R. Hedges, Vivienne C. Ivory, Te Kani R. Kingi, Renee Liang, Lana M. Perese, Elizabeth Peterson, Jan E. Pryor, Elaine Reese, Elizabeth M. Robinson, Karen E. Waldie and Clare R. Wall. The views reported in this paper are those of the authors and do not necessarily represent the views of the Growing Up in New Zealand investigators. We also acknowledge Nicholas Bowden and Dr Sheree Gibb from the University of Otago for providing code that allowed us to identify antidepressant dispensings in the IDI.
Availability of data and materials
The Growing Up in New Zealand and IDI data cannot be shared by the authors. The study data that support the findings of this study are available from Growing Up in New Zealand but restrictions apply to the availability of these data, which were used under licence for the current study, and so are not publicly available. Growing Up in New Zealand data can be made available to external researchers with permission from the study’s Data Access Committee, providing that the Data Access Protocol is followed. Details of this can be found on the study’s website www.growingup.co.nz. Research who wish to use the IDI must submit an application through Statistics New Zealand. Requests require a concept paper describing the purpose of data access, ethical approval at the applicant’s institution, and provision for secure data access. Further details can be found at ![]() .
.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Growing Up in New Zealand has been funded by the New Zealand Ministries of Social Development, Health, Education, Justice and Pacific Island Affairs; the former Ministry of Science Innovation and the former Department of Labour (now both part of the Ministry of Business, Innovation and Employment); the former Ministry of Women’s Affairs (now the Ministry for Women); the Department of Corrections; the Families Commission (now known as the Social Policy Evaluation and Research Unit); Te Puni Kokiri; New Zealand Police; Sport New Zealand; the Housing New Zealand Corporation; and the former Mental Health Commission, The University of Auckland and Auckland UniServices Limited. Other support for the study has been provided by the NZ Health Research Council, Statistics New Zealand, the Office of the Children’s Commissioner and the Office of Ethnic Affairs. Dr. Stephanie D’Souza and Associate Professor Barry Milne were funded by the New Zealand Ministry of Business, Innovation and Employment (MBIE) as part of A Better Start National Science Challenge.