
Abstract
Objectives:
Concerns about fragmented mental health service delivery persist, particularly for people with severe and persistent mental illness. The objective was to review evidence regarding outcomes attributed to system-level intersectoral linkages involving mental health services and non-clinical support services, and to identify barriers and facilitators to the intersectoral linkage process.
Methods:
A systematic, qualitative review of studies describing attempts to coordinate the activities of multiple service agencies at the policy, program or organisational level was conducted. Electronic databases Medline, PsycINFO and EMBASE were searched via OVID from inception to July 2012.
Results:
Of 1593 studies identified, 40 were included in the review – 26 in adult and 14 in vulnerable youth populations. Identified mechanisms to promote positive system-level outcomes included: interagency coordinating committees or intersectoral/interface workers engaged in joint service planning; formalised interagency collaborative agreements; a single care plan in which the responsibilities of all agencies are described; cross-training of staff to ensure staff culture, attitudes, knowledge and skills are complementary; service co-location; and blended funding initiatives to ensure funding aligns with program integration. Identified barriers included: adequacy of funding and technology; ensuring realistic workloads; overcoming ‘turf issues’ between service providers and disagreements regarding areas of responsibility; ensuring integration strategies are implemented as planned; and maintaining stakeholder enthusiasm.
Conclusions:
System-level intersectoral linkages can be achieved in various ways and are associated with positive clinical and non-clinical outcomes for services and clients. Some linkage mechanisms present greater implementation challenges than others (e.g. major technology upgrades or co-location in geographically remote areas). In some instances (e.g. co-location) alternative options may achieve equivalent benefits. Publication bias could not be discounted, and studies using high-quality research designs are scarce. The limited information base applicable to system-level integration argues strongly for the evaluation of the models that evolve in the rollout of the national Partners in Recovery initiative.
Introduction
There continues to be concern, in Australia and internationally, about the fragmentation of mental health service delivery, particularly for those individuals with severe and persistent mental illness with complex needs requiring services from multiple agencies (Hogan, 2003; Rosenberg et al., 2009; The President’s New Freedom Commission on Mental Health, 2003). In particular, individuals with complex symptom sets such as co-morbid substance abuse, intellectual disability and forensic issues or involvement with the child welfare system have been considered high risk for falling through the gaps of service delivery systems (Castle, 2011; Rosenheck et al., 2003). Although high-quality clinical treatment is the responsibility of mental health services, it is beyond the scope of most clinical mental health services to also provide general medical services, housing, accommodation support, psychosocial support, community and domiciliary services, income security, and employment/training services, which can also be essential for successful community living (Australian Health Ministers, 2009; Whiteford, 1994). A lack of coordination between the various sectors responsible for the treatment, care and support of people experiencing severe mental illness impedes access to services with consequent poor health and social outcomes (Dill and Rochefort, 1989; Rosenheck et al., 2003). The problems associated with implementing an integrated service system have been well documented in the Australian context (Australian Parliament, 2006; Council of Australian Governments, 2006; Rosenberg et al., 2009).
From the outset of the National Mental Health Strategy in Australia in 1992, the need for linkages between the mental health sector and other government and non-government services was considered critical to the provision of effective community-based treatment and support (Australian Health Ministers, 1992; Whiteford, 1994). The first National Mental Health Policy and plan required: the mainstreaming of mental health services to bring them under the same administrative umbrella as other health services (Singh, 1992; Whiteford et al., 1993); the integration of hospital (inpatient) mental health services with community mental health services (Whiteford et al., 1993); and intersectoral linkages requiring access to housing and community services (mostly operated outside of health departments) for individuals with mental illness and psychiatric disability living in the community (Whiteford, 1992a; Whiteford, 1992b). Following deinstitutionalization, with most people with severe and persistent mental illness now cared for in the community, poor linkages between the health, housing, employment and income support sectors became evident (Behan et al., 1994; HREOC [Human Rights and Equal Opportunity Commission], 1993). In facilities where adequate community and residential support services had not accompanied downsizing or closure of psychiatric beds, common consequences were substandard accommodation, homelessness, incarceration and unnecessary admissions to hospitals (Hoult and Burchmore, 1994).
The development of an integrated service system has been challenging, as responsibility for the various services span a range of portfolios in Commonwealth and State jurisdictions and the non-government and private sectors. Systemic barriers, such as the administrative and financial separation of these service sectors, have impeded the seamless delivery of the range of necessary services. The Commonwealth Disability Services Act 1986 had recognised that people with psychiatric disability were eligible for services but afforded them a low priority (Whiteford, 1994). This was changed with the Commonwealth State Disability Agreement 1991 and the Commonwealth Disability Discrimination Act 1992, which made it unlawful to discriminate against people with disability, including those with psychiatric disability. An attempt was then made to align the policies and programs of health, housing and community services departments when relevant Ministers in all jurisdictions endorsed the findings of the Mental Health Forum on Intersectoral Linkages (Mental Health Forum on Intersectoral Linkages, 1995). Nevertheless, there remained a substantial problem in providing equitable access to people with psychiatric disability, given the relatively small growth in expenditure in that program in the following decade. Intersectoral reform was largely unsuccessful; a ‘silo’ mentality continued to exist within government departments at the Commonwealth and State/Territory level (e.g. mental health, health, housing, education, disability, geriatrics, child and family services) (Betts and Thornicroft, 2001).
By 2006, multiple factors were coalescing to pressure governments for action. The reforms being demanded were in areas within and outside the health portfolio, and involving Commonwealth, State and Territory government responsibilities. The failures highlighted by the Not for Service report (Mental Health Council of Australia, 2005), the findings of the Senate inquiry into mental health, and the high profile media cases of Cornelia Rau and Vivian Solon, emphasised the need for better coordinated government services. While the problems being addressed by the 2006 COAG National Action Plan on Mental Health (Council of Australian Governments, 2006) covered a number of areas, it gave attention to the need to improve services to those with the highest need; specifically, those individuals with severe and persistent mental illness. The highlighted failures for these individuals were not just in the health system but also in the disability support and housing sectors. This was essentially a return to the concerns raised in the intersectoral reform plank of the first plan (Whiteford, 1994).
Internationally, there is an extensive literature primarily from the United States describing attempts to address the fragmentation of mental health and related services. A wide variety of strategies have been used, from the individual client (micro) level to the system (macro) level (Dill and Rochefort, 1989; Rosenheck et al., 2003), and several large-scale, multi-site studies have been attempted (e.g. Bickman, 1996; Goldman et al., 2002; Lehman et al., 1994). Most research has focused on partnerships within the health sector, between specialist mental health services and primary care (Butler et al., 2011; Kathol et al., 2010), and on initiatives at the individual level that aim to link the client to necessary services through the use of case managers or care coordinators (Bruns et al., 2010; Stewart et al., 2012). However, there has been much less attention paid to describing initiatives to facilitate system-level integration or coordination, and even less about the outcomes of, and facilitators and barriers to, system-level intersectoral linkages between mental health clinical services and non-clinical support services. Non-clinical support services, in the Australian context, are spread across a range of administratively, financially and organisationally distinct providers and government portfolios. The current paper focuses on these linkages because these arrangements pose particular challenges to integration, although some of the possible solutions (e.g. a common medical record) may also apply to integration between areas within health.
Tieman and colleagues (2007) provide an overarching definition of integration as the ‘development of more comprehensive approaches to care provision that [depend] on formal relationships or structural arrangements to organise and deliver that care’ (p. 57). Randolph et al. (1997) note that integration should be divided into: (a) direct service delivery level integration, in which the needs of the individual are met ‘without altering the systems in which the services are provided’ (p. 370); and (b) system-level integration, which is any ‘attempt to improve the service system for a defined population’ (p. 370), and may involve linkages between agencies and programs or reconfiguring or consolidating agencies. Randolph notes, however, that system level integration should be viewed as a continuum comprising a variety of strategies from information-sharing through to arrangements involving the coalescing of service provision and/or funding under a single authority (Randolph et al., 2002). For the purposes of this paper, we use the term ‘system-level intersectoral linkages’ (also referred to as ‘system-level integration’) as per the definition provided by Randolph (Randolph et al., 1997; Randolph et al., 2002). Importantly, we consider that this definition enables the inclusion of a broad range of strategies. There may be some contention regarding whether the employment of a non-clinical support worker (such as an employment specialist) within a mental health service would constitute direct clinical or system-level integration. For the purposes of this study, it met criteria for the latter in that it results in an alteration of the systems in which the services are provided. An example of direct clinical integration would be subsuming new non-clinical support roles into the job description of a clinical case manager, or care coordination involving brokering linkages between agencies, both of which do not result in an alteration to the systems in which care is provided. However, it is important to note that the implementation of a strategy does not necessarily ensure that integration has been achieved, which is a more empirical question.
A previous systematic review (Cameron and Lart, 2003) commissioned by the UK National Health Service (NHS) sought to identify and describe models of joint working across the NHS and social services interface, as well as factors promoting and hindering the success of identified models. They described four models of joint working, three of which occurred at the system level: (1) placement schemes; (2) multiagency teams and projects; and (3) strategic level working (i.e. joint planning/commissioning/purchasing). Factors promoting and hindering joint working were grouped into three themes: (1) organisational issues; (2) cultural and professional issues; and (3) contextual issues. Outcomes were not described separately for system-level intersectoral linkages, and the scope of the review encompassed the entire health/social care system. The outcomes of intersectoral strategies specifically involving mental health services and non-clinical support services, and associated facilitators and obstacles, warrant further examination.
The authors sought to systematically review the evidence regarding outcomes attributed to system-level intersectoral linkages involving mental health services and non-clinical support services. Specifically, the aims of the study were to:
Summarise the evidence regarding the effectiveness of system-level intersectoral linkages involving mental health services and non-clinical support services; and
Identify factors that act as barriers and facilitators to the linkage process.
Methods
Search methodology
The systematic review adhered to guidelines recommended by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Moher et al., 2009). Electronic databases Medline, PsycINFO and EMBASE were searched via OVID from their respective inception years to July 2012. The following search string was utilised to identify potentially relevant articles: (Psychiatric Service* OR Mental Health Service* OR Mental Health System*) AND (Employment OR Vocational OR Education OR Accommodation OR Residential OR Housing OR Welfare OR Income OR Community OR Disability) AND (Link* OR Integrat* OR Intersectoral* OR Multiagency OR Interagency OR Partnership* OR Reform*) AND (Outcome* OR Effect* OR Impact* OR Challenge* OR Barrier* OR Facilitat*).
There were no limitations to the language of publication. Titles and abstracts were initially screened for relevance. Full-text versions of potentially eligible papers were retrieved and reviewed.
Inclusion/exclusion criteria
Non-peer reviewed reports published by governments or other organisations were excluded from the review. Eligible reports fulfilled the following criteria:
They described a system-level intersectoral linkage, defined as any attempt to improve the service system for a defined population by implementing linkages between agencies and programs or reconfiguring or consolidating agencies at the policy, program or organisational level (Randolph et al., 1997; Randolph et al., 2002). Reports describing efforts to link individual clients to multiple services, for example through case management or care coordination, were not considered for inclusion because these strategies do not alter the systems in which such services are provided (Randolph et al., 1997). Reports that said services were integrated but did not describe the mechanisms by which integration was attempted were excluded.
The intersectoral linkage was between clinical services and any combination of the non-clinical support sectors utilised by people experiencing mental health problems (i.e. excluding services for substance use disorders and physical health).
Outcomes were described for either:
The services involved; and/or The clients served.
To ensure that outcomes could be appropriately linked to the integration mechanisms described we required that all necessary information was available within a given report, and that cross-referencing was not required. Although the study sought to describe facilitators and barriers to system-level intersectoral activities, these were not considered in terms of inclusion criteria for the review, but rather, were documented where available.
Data extraction
The following variables were extracted from articles identified as meeting criteria for inclusion: geographical location of services; year of data collection; target population; study design and level of evidence; the non-clinical sectors linked to mental health by the described model/intersectoral intervention; description of the mechanism utilised to link the services; data source; client and/or service-level outcomes; any identified facilitators to the linkage process; and any identified barriers to the linkage processes.
We used the National Health and Medical Research Council levels of evidence hierarchy to classify the study designs (NHMRC, 2000). The levels in the hierarchy are: Level I – evidence obtained from a systematic review of all relevant randomised controlled trials; Level II – evidence obtained from at least one properly designed randomised controlled trial; Level III-1 – evidence obtained from well-designed pseudo-randomised controlled trials (alternate allocation or some other method); Level III-2 – evidence obtained from comparative studies with concurrent controls and allocation not randomised (cohort studies), case-control studies, or interrupted time series with a control group; Level III-3 – evidence obtained from comparative studies with historical control, two or more single-arm studies, or interrupted time series without a parallel control group; and Level IV – evidence obtained from case series, either post-test or pre-test and post-test.
Qualitative analysis
The key findings regarding intersectoral service activity derived from included studies were tabulated and descriptively summarised to provide an overview of factors to consider with regard to multiagency policymaking. The implications of intersectoral activity for particular age brackets (e.g. youth and adult populations) and sectors (e.g. employment) were also considered.
Results
Included studies
Forty studies met inclusion criteria (Figure 1; Table 1), grouped into three study categories: (1) Adult populations (multiple sectors) – 10 studies reporting on adult populations and multiple sectors and are summarised in Supplementary Table 1; (2) Vulnerable youth populations (multiple agencies) – 14 studies described intersectoral linkages designed to improve outcomes for vulnerable youth populations and the multiple agencies serving them; these are summarised in Supplementary Table 2; and (3) Adult populations (integrating clinical and employment services) – 16 studies of adults reported specifically on the effects of integrated clinical and employment services; these studies have been summarised separately from other studies of adults in Supplementary Table 3.
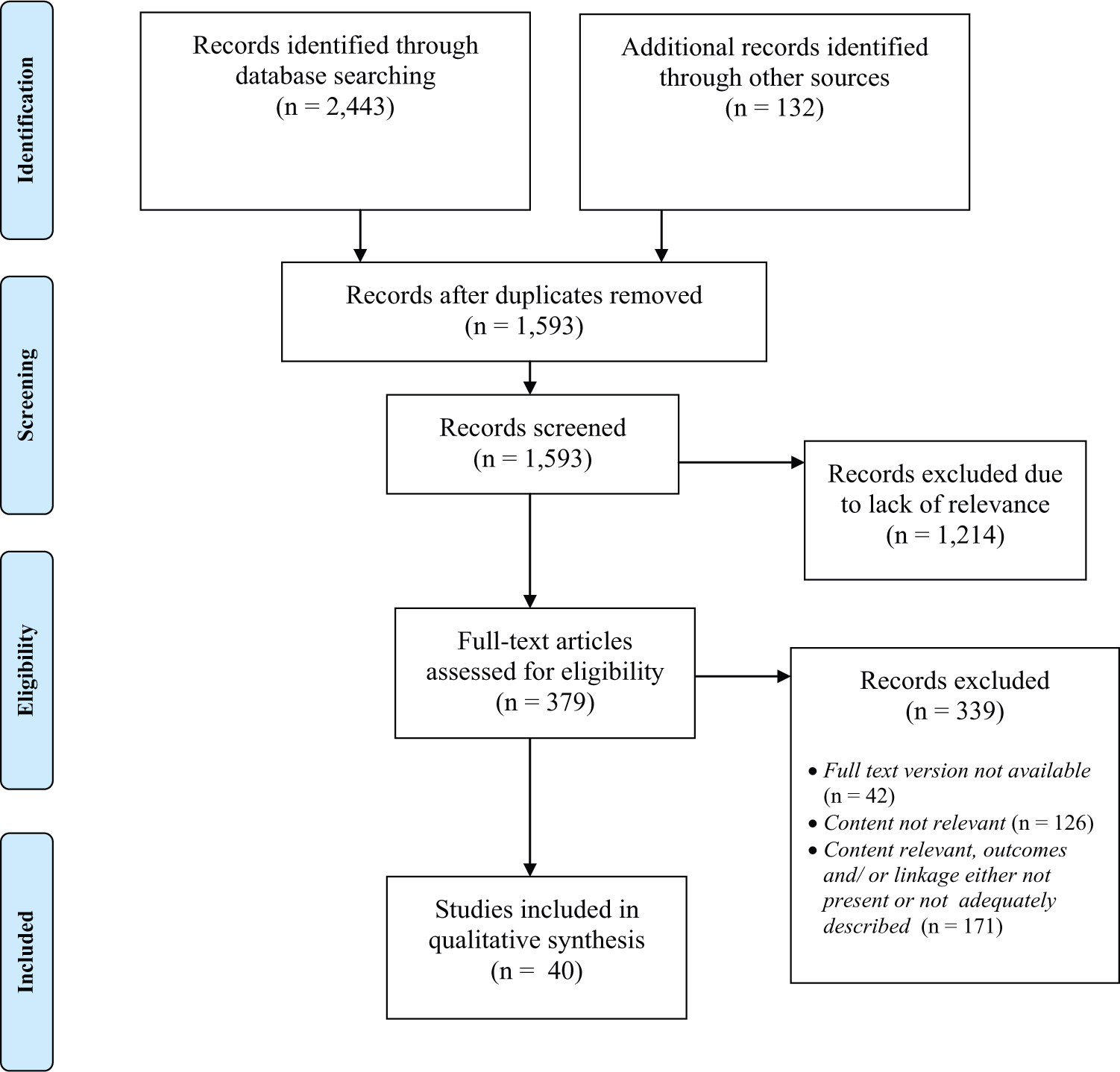
Summary of process for identifying articles meeting inclusion criteria.
Studies meeting criteria for inclusion in qualitative synthesis (n=40).
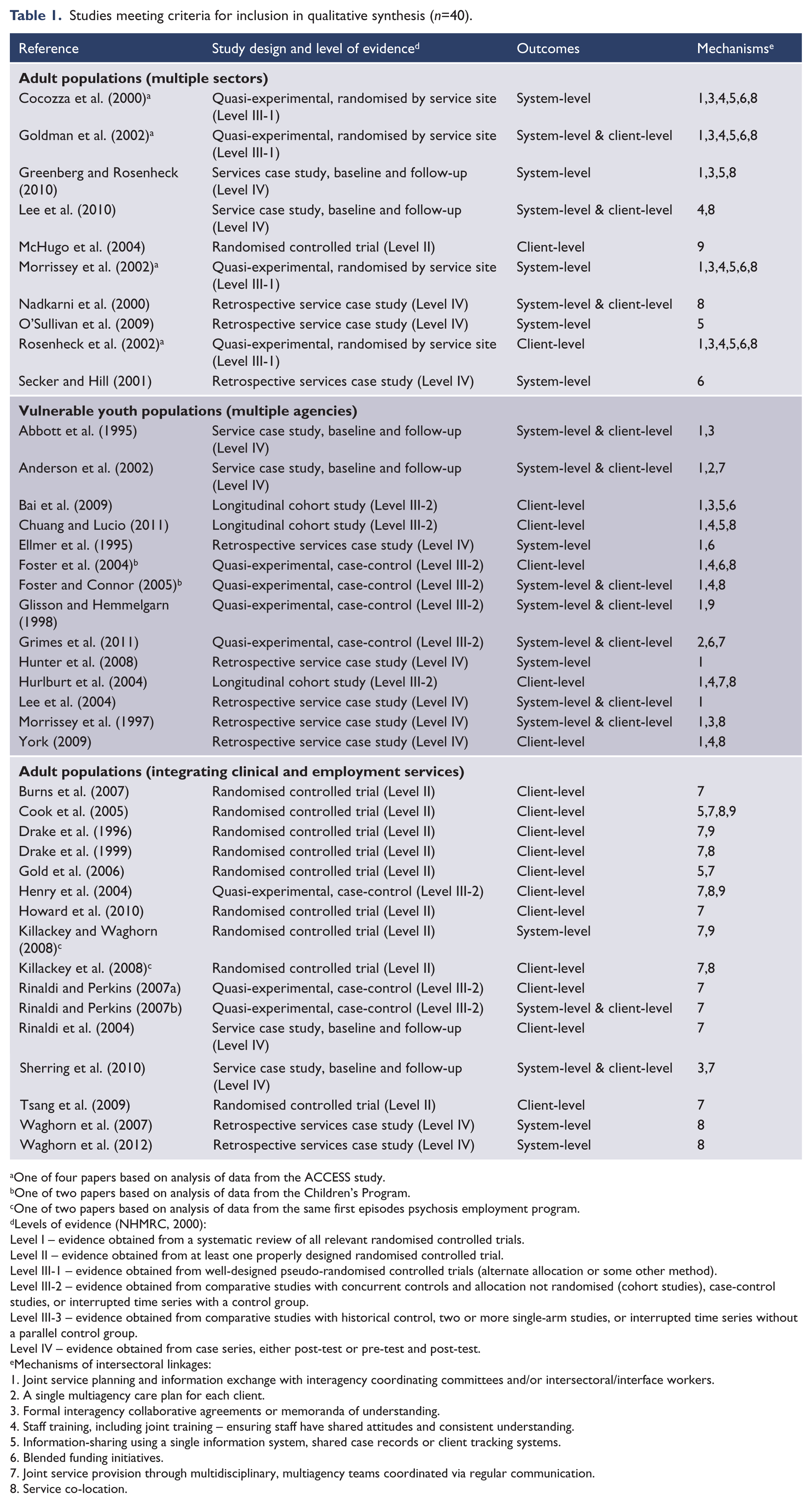
One of four papers based on analysis of data from the ACCESS study.
One of two papers based on analysis of data from the Children’s Program.
One of two papers based on analysis of data from the same first episodes psychosis employment program.
Levels of evidence (NHMRC, 2000):
Level I – evidence obtained from a systematic review of all relevant randomised controlled trials.
Level II – evidence obtained from at least one properly designed randomised controlled trial.
Level III-1 – evidence obtained from well-designed pseudo-randomised controlled trials (alternate allocation or some other method).
Level III-2 – evidence obtained from comparative studies with concurrent controls and allocation not randomised (cohort studies), case-control studies, or interrupted time series with a control group.
Level III-3 – evidence obtained from comparative studies with historical control, two or more single-arm studies, or interrupted time series without a parallel control group.
Level IV – evidence obtained from case series, either post-test or pre-test and post-test.
Mechanisms of intersectoral linkages:
Joint service planning and information exchange with interagency coordinating committees and/or intersectoral/interface workers.
A single multiagency care plan for each client.
Formal interagency collaborative agreements or memoranda of understanding.
Staff training, including joint training – ensuring staff have shared attitudes and consistent understanding.
Information-sharing using a single information system, shared case records or client tracking systems.
Blended funding initiatives.
Joint service provision through multidisciplinary, multiagency teams coordinated via regular communication.
Service co-location.
Service administration by a single lead agency.
Included studies described intersectoral linkages between mental health services and a diverse array of non-clinical support sectors including: judicial/forensic services; social services; mainstream education; special education; vocational support services; child welfare agencies; substance abuse services; supported employment; housing support services; government welfare and other community-based services. Populations studied included homeless, forensic, persons with first episode psychosis and persons with chronic mental illness.
Several studies reported data from the same primary study, including four from the ACCESS study, two from the Children’s Program and two from an employment program for persons with first episode psychosis. Some programs, including large programs such as ACCESS, received special and sometimes time-limited funding to implement the linkages (e.g. funding for taking people out for coffee, exercise programs, discretionary money etc.).
Study quality varied, with only 14 of the 40 included studies using any form of randomisation. The four papers based on the ACCESS study randomised based on service site and 10 other studies randomised at the level of the individual service recipients (i.e. randomised controlled trials; see Table 1). Sixteen papers reported on case study designs with no comparison control group, with only six of these collecting baseline data. Levels of evidence were not equally distributed across the three broad study categories. Notably, studies in adult populations (multiple sectors) were virtually all Level III-1 and Level IV. Studies in vulnerable youth populations (multiple agencies) were either Level IV or Level III-2. Of studies in adult populations (integrating clinical and employment services) about half were Level II, and the remainder were Level III-2 or Level IV.
Twenty-two of the 40 studies reported system-level outcomes, and 30 reported client-level outcomes, with 12 studies reporting both. Studies of integrated mental health and vocational services were most likely to report on client-level outcomes. For studies reporting these outcomes, sample sizes varied widely, ranging from 14 to 7055 people, the majority with a sample of less than 500 clients. The number of services included in service-level outcome analyses also varied, ranging from a single service provider to 32 separate agencies.
Mechanisms of intersectoral linkage
The studies described a range of mechanisms for promoting collaborative intersectoral practice (see Table 1). These were variously defined, and were generally poorly delineated from each other. However, they can be broadly classified into the following nine categories:
Joint service planning and information exchange with interagency coordinating committees and/or intersectoral/interface workers (n=18 studies);
A single multiagency care plan for each client (n=2 studies);
Formal interagency collaborative agreements or memoranda of understanding (n=9 studies);
Staff training, including joint training – ensuring staff have shared attitudes and consistent understanding (n=10 studies);
Information-sharing using a single information system, shared case records or client tracking systems (n=10 studies);
Blended funding initiatives (n=9 studies);
Joint service provision through multidisciplinary, multiagency teams coordinated via regular communication (n=17 studies);
Service co-location (n=19 studies); and
Service administration by a single lead agency (n=6 studies).
The use of different linkage mechanisms varied by category of study, reflecting the nature of the services being linked. For example, the most common linkage mechanism was service co-location, being used in almost half of all studies. Joint service planning was also common, being a feature of many studies involving adult populations (multiple sectors) and vulnerable youth populations (multiple agencies), but none of those in adult populations (integrating clinical and employment programs). Conversely, joint service provision arrangements were only a common feature in studies of adult populations (integrating clinical and employment programs).
Service outcomes of intersectoral linkage
Outcomes reported were overwhelmingly positive, particularly with regard to improvements in interagency communication, greater mutual understanding of and empathy for each other’s services, and reduced bureaucracy and improved service efficiency. System-level integration strategies were also associated with service outcomes such as improved cost efficiency across sectors (Abbott et al., 1995; Anderson et al., 2002; Foster and Connor, 2005; Rinaldi and Perkins, 2007b) and improved capacity for non-clinical staff to manage mental health needs (Hunter et al., 2008; Lee et al., 2010; Nadkarni et al., 2000).
Within the studies reviewed, exceptions to the positive outcomes are worth noting, and potentially represent a more balanced view on intersectoral service reform. Within studies of adults, Secker and Hill (2001) reported stakeholder perspectives on the UK pooled financing initiative under the 1999 Health Act. Despite the scheme, interagency support was restricted to a minority of agencies from comparable practice contexts. The policy emphasis on partnerships was considered too narrow, and failed to be translated into the desired whole-of-systems approach. Foster and Connor (2005) reported that although delivering services for youth through a ‘system of care’ led to substantially reduced expenditure in non-clinical sectors, this only partially offset the higher costs accrued by mental health services participating in the comprehensive system. In synthesising the results from studies of the ACCESS program, Goldman and colleagues (2002) concluded that providing funds and technical support to promote service system integration may improve integration on a local level (i.e. between mental health and other agencies within a given community) but may not do so at a system-wide level (i.e. across human service agencies at a macro level).
Client outcomes of intersectoral linkage
Positive client outcomes such as improvements in clinical functioning and employment prospects were also encouraging in terms of the impact of system-level intersectoral practices on individuals. The benefits of intersectoral collaboration were not limited to the clinical service sector. For example, system-level integration strategies were associated with outcomes such as: improved accommodation stability (Goldman et al., 2002; Lee et al., 2010; McHugo et al., 2004; Rosenheck et al., 2002); reduced child foster placements (Abbott et al., 1995); reduced recidivism rates/involvement with the juvenile justice sector (Anderson et al., 2002; Foster and Connor, 2005; Foster et al., 2004); and improved vocational outcomes (Burns et al., 2007; Cook et al., 2005; Drake et al., 1996; Drake et al., 1999; Gold et al., 2006; Killackey et al., 2008; Rinaldi and Perkins, 2007b; Rinaldi et al., 2004; Sherring et al., 2010; Tsang et al., 2009).
However, exceptions to positive outcomes were also found for the effect on client outcomes. Negative findings were reported by reports from the ACCESS program (Cocozza et al., 2000; Goldman et al., 2002; Morrissey et al., 2002; Rosenheck et al., 2002), in which system-level intersectoral strategies designed to address homelessness among persons with severe mental illness were evaluated on a large scale. Targeted efforts to implement integration strategies through earmarked funding and technical assistance did not lead to better client outcomes above and beyond high-quality clinical services such as assertive community treatment (Goldman et al., 2002). It has been suggested that the lack of a positive effect could be explained by the implementation of integration strategies at some of the comparison sites (Morrissey et al., 2002; Rosenheck et al., 2002).
Within studies of youth populations, Chuang and Lucio (2011) investigated two types of intersectoral links between child welfare agencies, schools and outpatient mental health services. Administratively oriented collaborative arrangements including staff co-location, shared records and information management systems were associated with reduced odds of children receiving needed school-based and outpatient mental health services. Authors highlight that such strategies do not guarantee the quality of services, and without a shared vision services may suffer. Glisson and Hemmelgarn (1998) reported that interorganisational coordination through centralisation of authority led to a diffusion of responsibility amongst direct service providers, and consequently had a negative effect on service quality. They highlight that efforts to improve children’s service systems should consider a focus on fostering positive organisational climates rather than exclusively directing effort towards top-down service configurations.
Finally, in the context of implementing evidence-based, integrated supported employment practices, the evidence for improving non-vocational outcomes is equivocal (Drake et al., 1996). Importantly, these studies did not test the specific effects of the extent of integration between clinical and vocational services and subsequent outcomes. Rather, they provide indirect evidence that when integration is included in a set of service principles of supported employment, the integrated services consistently outperform segregated vocational services (Waghorn et al., 2012).
Facilitators of intersectoral linkage
Facilitators of intersectoral activity were identified. The most commonly identified factor attributed to the success of interagency collaborations related to improvements in communication between services, and subsequently increased access to multidisciplinary resources and staff-friendly networks (Abbott et al., 1995; Anderson et al., 2002; Chuang and Lucio, 2011; Cook et al., 2005; Drake et al., 1996; Drake et al., 1999; Henry et al., 2004; Hunter et al., 2008; Killackey and Waghorn, 2008; Lee et al., 2004; O’Sullivan et al., 2009). Strong senior leadership from each service sector supporting integration and mechanisms for early resolution of conflict/issues between services was also important (Cocozza et al., 2000; Ellmer et al., 1995; Lee et al., 2004). The achievement of a shared perspective, or some form of mutual understanding and an increase in intersectoral empathy, was also frequently cited as critical to the success of working across organisations (Abbott et al., 1995; Anderson et al., 2002; Chuang and Lucio, 2011; Waghorn et al., 2012). Co-location of services was also considered to be important (Drake et al., 1999; Henry et al., 2004; Lee et al., 2010; Nadkarni et al., 2000), as was the intensity and number of linkages between services (Bai et al., 2009). Some studies reported that the clarity of a chain of responsibility or accountability facilitated interagency cooperation (Chuang and Lucio, 2011; Grimes et al., 2011; McHugo et al., 2004). The presence of a strategic plan or coordinating body was also considered essential to the success of system-level integration strategy implementation (Cocozza et al., 2000; Waghorn et al., 2012), as was the ongoing monitoring of joint service effectiveness (Ellmer et al., 1995; Gold et al., 2006; Waghorn et al., 2012).
Barriers to intersectoral linkage
Studies described a range of barriers to the implementation of system-level intersectoral linkages. The most commonly identified barriers related to resource constraints with respect to funding, time, workloads and technology (Abbott et al., 1995; Anderson et al., 2002; Chuang and Lucio, 2011; Cocozza et al., 2000; Ellmer et al., 1995; Gold et al., 2006; Hunter et al., 2008; Killackey and Waghorn, 2008; Lee et al., 2004; Morrissey et al., 1997; Morrissey et al., 2002; Rosenheck et al., 2002; Secker and Hill, 2001; Sherring et al., 2010; Waghorn et al., 2007; Waghorn et al., 2012). ‘Turf issues’ relating to differences of opinion between service providers and disagreements regarding areas of responsibility were also commonly cited as significant impediments to the success of interagency initiatives (Abbott et al., 1995; Anderson et al., 2002; Chuang and Lucio, 2011; Glisson and Hemmelgarn, 1998; Hunter et al., 2008; Killackey and Waghorn, 2008; Lee et al., 2004; Secker and Hill, 2001; Sherring et al., 2010; Waghorn et al., 2007; Waghorn et al., 2012). Client confidentiality and the legal ramifications of and barriers to information-sharing were also problematic (Anderson et al., 2002; Chuang and Lucio, 2011; Hunter et al., 2008; Lee et al., 2004; Secker and Hill, 2001; Waghorn et al., 2007). One study (Hunter et al., 2008) reported that mental health stakeholders felt negatively about closer intersectoral links, as they were concerned about the potential increase in inappropriate referrals to their services. Another (Greenberg and Rosenheck, 2010) reported that waning stakeholder enthusiasm for intersectoral strategies may impede subsequent growth in levels of joint planning and coordination. The need to ensure an adequate ‘dosage’ of system integration strategies was highlighted strongly by the failure of the ACCESS program interventions to affect measurable client outcomes (Morrissey et al., 2002; Rosenheck et al., 2002).
Establishing intersectoral linkages
Few studies described the process of initially establishing an intersectoral collaboration. Three studies (Ellmer et al., 1995; Goldman et al., 2002; York, 2009) reported the use of competitive grants to garner interest from multiple agencies in participating in intersectoral reforms. Another two (Lee et al., 2004; O’Sullivan et al., 2009) described how clinical services solicited interest in intersectoral collaboration via direct stakeholder consultation. Anderson and colleagues (2002) highlight that for a collaborative system of care to coalesce, there must be a consensus amongst stakeholders from the outset regarding values, goals, language and definitions.
Discussion
The literature review suggests that system-level intersectoral linkages can be achieved in a variety of ways and are associated with positive outcomes for services and clients in both clinical and non-clinical contexts. The standout issue needed to promote effective service integration is arguably the hardest to achieve; that is, ensuring mutual respect and understanding of roles with streamlined communication between all the services involved in the care and support of clients.
Other mechanisms found to promote positive outcomes included formal interagency memoranda, joint service planning and provision, single cross-agency care plans, cross-training of staff, shared case records, integrated funding, service co-location and a lead agency for coordination. However, there were multiple barriers to achieving integration, including inadequate funding and technology, excessive workloads, disagreements relating to service responsibilities, client confidentiality and maintaining stakeholder buy-in.
Methodological considerations
The findings from this study contribute a more detailed, systematically derived description of the outcomes of, and facilitators and obstacles to, intersectoral strategies involving mental health services than has been available previously. However, five main methodological considerations warrant attention when interpreting the findings of this study. Firstly, the overwhelmingly positive findings in the literature should be seen in light of probable publication bias. It is probable that negative findings regarding intersectoral systems reforms have been documented, but not submitted or accepted for publication. This review found only 40 studies meeting eligibility criteria and, of these, several were sourced from the same evaluations.
Secondly, only 14 studies employed a study design involving randomisation procedures (10 at the individual level and four at the service level). Collectively, the identified literature may be subject to a range of biases, with these varying across study categories due to the different balance of designs used in each. For example, studies in adult populations (multiple sectors) were virtually all Level III-1 and Level IV, the latter category including numerous qualitative studies. Level IV studies are particularly susceptible to selection bias, non-representativeness, and performance bias, as acknowledged in some studies (e.g. Greenberg and Rosenheck, 2010). In this study category, all Level III-1 studies were from the ACCESS program, which may be subject to problems such as poor allocation concealment. One study noted diffusion of innovation as a possible source of bias in their results (Morrissey et al., 2002). Studies in vulnerable youth populations (multiple agencies) were either Level IV or Level III-2. Non-representativeness was noted as an issue in some Level III-2 studies (e.g. Foster et al., 2004). Studies in adult populations (integrating clinical and employment services) accounted for all but one of the Level II studies. Inability to blind employment specialists to the treatment assignment of the subjects was one possible source of bias noted in the Level II studies (e.g. Tsang et al., 2009).
Thirdly, despite relatively broad inclusion and exclusion criteria, many of the studies identified in the literature search were excluded because they did not meet the inclusion criteria of taking a system-level approach, or describing service or client outcomes. Inadequate description of complex interventions is common, and others have recommended the development of standardised approaches to describing intervention content as one possible solution. There remains a need for further high-quality studies in the field that address system-level approaches with client and service level outcomes, and provide a critical appraisal of the intersectoral linkages.
Fouthly, some studies (such as ACCESS) may have received additional funding to support the necessary linkages. It is possible that these incentives may introduce bias. Notably, additional services could allow for better consumer engagement and improved service and consumer outcomes. Others did not mention funding, but it cannot necessarily be assumed that implementation was supported within their existing service budget or framework. In other cases, it was not possible to determine whether the funding arrangements might constitute a possible source of bias.
Fifthly, this study was subject to many of the problems associated with reviews involving heterogeneous studies. One of these was that estimates of the size of the effects of system-level intersectoral linkages were not able to be made. In some cases this was due to the qualitative nature of the data collected in some studies. In quantitative studies, we were limited by the broad array of outcomes assessed, which meant that there were few measures on which there were sufficient common outcome data for comparison. Another problem was that, as the majority of reviewed articles included multiple intersectoral linkage mechanisms and did not provide outcomes by each mechanism, it was not possible to tease out the positive outcomes attributable to individual linkage mechanisms. The development of methods for identifying the ‘essential ingredients’ of complex interventions, such as those examined in this review, remains a significant challenge in healthcare evaluation (Bower et al., 2006). In addition, this review included numerous studies presenting qualitative results. Quality standards for assessing the results from qualitative studies are lacking. When examining qualitative health services research, it is also important to consider the social context of services (Popay et al., 1998). We have attempted to address this issue of context in our analysis of the integration of services, as outlined in Supplementary Tables 1–3.
Implications for the Australian context
Most of the mechanisms identified above are relevant for Australia. Some, such as a single information system or services administered by a single lead agency, would be hard to achieve in most areas in the short to medium term. However, having a shared care plan and regular communication has been shown to achieve many of the same benefits. All of the identified barriers would apply in Australian service settings.
In some parts of Australia, geographic circumstances pose unique implementation difficulties ( Killackey and Waghorn, 2008; Waghorn et al., 2007). Specifically, co-location of employment specialists in mental health settings may not always be possible, despite the evidence-base in support of such practices (Waghorn et al., 2007). Nonetheless, the ‘enhanced intersectoral links’ (Sherring et al., 2010) approach; that is, the implementation of procedures for facilitating and monitoring referrals from mental health teams to several disability employment services in the local region; represents a promising alternative in Australia. Structural barriers to the high fidelity implementation of evidence-based supported employment can be overcome where the Federal disability employment system is bypassed (Killackey and Waghorn, 2008).
The emphasis in the literature for benefits to the child and adolescent health, education and welfare sectors is a reminder that these populations need to be included in intersectoral reform initiatives. Positive outcomes of Australian intersectoral initiatives were also reported where mental health services were linked at the system-level to welfare and community-based non-government services (Lee et al., 2010; O’Sullivan et al., 2009) and multiple child serving agencies (Lee et al., 2004).
The Australian Government has allocated AUD$549.8 million over five years to the new Partners in Recovery (PiR) program (Roxon et al., 2011), to create and strengthen between-service partnerships and referral mechanisms, and facilitate recovery for individuals with severe and persistent mental illness (Department of Health, 2012). Implementation models will vary by Medicare Local region; however, evidence regarding optimal service delivery models is scarce. A national evaluation (to be completed in 2016) will provide broad evidence of PiR’s effectiveness. However, the limited information base applicable to system-level integration – what works, for whom, in what settings and why – argues strongly for evaluation of the models that evolve in the rollout of the PiR initiative.
Footnotes
Funding
This work was supported by the Mental Health Services Branch, Commonwealth Department of Health and Ageing and the National Health and Medical Research Council Centre for Research Excellence in Mental Health Systems Improvement (APP1041131).
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.