
Abstract
Objective:
In the 1990s, large differences in beliefs about the helpfulness of treatments for mental disorders were observed between the Australian public and health professionals. This study evaluates whether gaps in public and professional beliefs remain by comparing beliefs of the public and health professionals on the helpfulness of interventions and likely prognosis for six mental health problems: depression, depression with suicidal thoughts, early schizophrenia, chronic schizophrenia, social phobia, and post-traumatic stress disorder.
Methods:
Mental health literacy surveys based around a vignette of a person with a mental disorder were carried out in a nationally representative sample of the Australian public (n=6019) in 2011 and samples of Australian general practitioners, psychiatrists, and psychologists (n=1536) in 2012. Respondents were asked to rate the helpfulness of a range of interventions and the likely outcome with or without appropriate professional treatment. Differences between groups were examined with chi-square tests.
Results:
There were many significant differences in treatment beliefs, but most of these were small in size. Medium-sized differences tended to be consistent across vignettes and relate to the greater belief by the public in the helpfulness of close family or friends, a counsellor, vitamins and minerals, a special diet or avoiding certain foods, and having an occasional alcohol drink to relax. In contrast, professionals showed a greater belief in psychotherapy and cognitive behaviour therapy for depression and anxiety, and antipsychotics for schizophrenia. Findings on prognosis showed mostly small differences in beliefs.
Conclusions:
Overall, the results indicate that the views of the public and professionals are more aligned than in the 1990s. There are now few large gaps in treatment beliefs, but there remain some areas that could be improved.
Introduction
One important component of mental health literacy (Jorm et al., 1997a) is knowledge about what professional help and treatments are effective for mental health problems. A nationally representative survey of Australians in 1995 highlighted the poor mental health literacy of the Australian public in relation to treatment beliefs (Jorm et al., 1997c). Compared with mental health professionals, the public were less likely to believe in the helpfulness of standard treatments such as antidepressants for depression and antipsychotics for schizophrenia. Mental health specialists (i.e. psychiatrists and psychologists) were also thought to be much less helpful than generic counsellors. However, the public believed in the helpfulness of some interventions that professionals thought were unhelpful, including vitamins, minerals, and special diets. General population surveys in other countries have confirmed the different views of the public from those of professionals around the effectiveness of mental health treatments (Angermeyer and Matschinger, 2005; Lauber et al., 2005; Wang et al., 2007). These major differences in treatment beliefs are problematic because they may affect willingness to seek professional help (Rüsch et al., 2011; ten Have et al., 2010), as well as the type of help sought, treatment compliance (Pyne et al., 2005), and ultimately, the mental health and functioning of people with mental disorders.
Over the last decade or so, there has been concerted effort to improve the mental health literacy of the public in Australia and other countries (e.g. Hegerl et al., 2008; Hickie, 2004; Joa et al., 2008). Strategies such as public education campaigns and mental health first aid training (Kitchener and Jorm, 2008) have included beliefs in the effectiveness of mental health treatments and professional help-seeking as key targets for improvement. These strategies appear to be working, with evidence suggesting that beliefs about treatments and mental health providers have changed over the years (Reavley and Jorm, 2012; Schomerus et al., 2012). The most recent survey of mental health literacy in Australian adults was conducted in 2011 and found that antidepressants were generally rated favourably for treating depression, while psychiatrists and psychologists were endorsed as effective for a variety of mental health problems (Reavley and Jorm, 2011). However, treatment beliefs of the public have not yet been directly compared with the beliefs of health professionals, whose views may also have changed over time.
Alongside the original Australian adult mental health literacy survey carried out in 1995, parallel surveys of general practitioners, psychiatrists, clinical psychologists, and mental health nurses were conducted between 1996 and 1998 to act as a standard against which to compare the public (Caldwell and Jorm, 2000; Jorm et al., 1997b). While additional national surveys of Australian adults were carried out in 2003–2004 and 2011, no corresponding survey of professional beliefs was conducted in that period. An updated survey of professional beliefs is important to see whether gaps in public and professional beliefs still remain, given changes in the evidence base over the intervening 16 years. Furthermore, the most recent survey of the public included some additional mental health problems that were not covered in the earlier professional surveys (Reavley and Jorm, 2011). To remedy this, a mental health literacy survey of Australian health professionals was carried out in 2012 (Morgan et al., 2013). This survey complemented the matching nationally representative survey of the Australian public conducted in 2011 and covered six mental health problems (depression, depression with suicidal thoughts, early schizophrenia, chronic schizophrenia, social phobia, and post-traumatic stress disorder).
In this paper, we directly compare public and professional beliefs on the helpfulness of interventions and beliefs about prognosis for six mental health problems. We compare data from the 2011 national survey of mental health literacy with data on professional beliefs collected from the 2012 survey of health professionals. This information can be used to assist in the design of campaigns to improve the mental health literacy of both professionals and the public.
Methods
Professional samples
The methods of the survey of health professionals have been previously described (Morgan et al., 2013). A questionnaire was mailed to 6848 health professionals registered with Medicare Australia in June 2012. The sample of professionals consisted of a random sample of 3000 general practitioners (GPs), a random sample of 1800 registered clinical psychologists, and all active psychiatrists (2048). We obtained 1536 returned surveys (22.4%) from 518 GPs (17.3%), 506 psychiatrists (24.7%), and 498 clinical psychologists (27.7%), with 14 respondents not indicating a profession. Responses for each of the six vignette types were: depression (n=280), depression with suicidal thoughts (n=261), early schizophrenia (n=237), chronic schizophrenia (n=259), social phobia (n=242), and post-traumatic stress disorder (PTSD; n=257). To determine the representativeness of our sample on basic demographics, we obtained data from the Department of Human Services (DHS) on the age and gender distributions of the professional populations that we sampled from (Department of Human Services, 2013, personal communication). In our sample of GPs, the distribution of age was significantly different to the population distribution (p<0.001), as was gender (p<0.001). Our sample was overrepresented by female GPs (50.3 vs. 42.1%) and GPs aged 50 or older (59.1 vs. 48.0%). For psychiatrists, the distribution of age was significantly different to the population distribution (p<0.001), with an overrepresentation of older psychiatrists (66.5 vs. 51.6%). However, the proportion of male and female psychiatrists was not significantly different to that in the Australian population of psychiatrists. Our sample of clinical psychologists was not significantly different from the population of clinical psychologists in the distribution of age or gender.
Sample of the public
The public survey involved computer-assisted telephone interviews with a national sample of 6019 Australians aged 15 years or older (Reavley and Jorm, 2011). Interviews were conducted between January and April 2011 by the Social Research Centre. A “dual frame” approach was used, with the sample contacted by random-digit dialling of both landlines and mobile phones. The response rate for the survey was 44.0%, defined as completed interviews (6019) out of sample members who could be contacted and were confirmed as in scope (n=13,636). Responses for each of the six vignettes were: depression (n=1016); depression with suicidal thoughts (n=1008); early schizophrenia (n=1002); chronic schizophrenia (n=993); social phobia (n=992); and PTSD (n=1008).
Survey questions
The survey was comparable to the survey used in the 1990s and was based on a vignette of a person with a mental disorder. On a random basis, respondents were presented with one of six vignettes: depression, depression with suicidal thoughts, early schizophrenia, chronic schizophrenia, social phobia, and PTSD. Members of the public were randomly assigned to receive either male (“John”) or female (“Jenny”) versions of the vignette, whereas health professionals received the male version of the vignettes. All vignettes were written to satisfy diagnostic criteria according to DSM-IV and ICD-10 and have been published previously (Jorm et al., 2005; Reavley and Jorm, 2011). The depression vignette and the early schizophrenia vignette were also identical to those used in the 1996 survey of health professionals (Jorm et al., 1997c).
After being presented with the vignette, respondents were asked a series of questions, some of which are relevant to the present paper and are described in detail here. Respondents were asked what, if anything, they thought was wrong with the person described in the vignette and a series of questions about the likely helpfulness of various interventions. The interventions were: a typical GP or family doctor; a typical chemist (pharmacist); a counsellor; a social worker; a telephone counselling service, such as Lifeline; a psychiatrist; a psychologist; help from close family; help from close friends; a naturopath or a herbalist; the clergy, a minister or priest; John tried to deal with his problems on his own; vitamins and mineral, tonics, or herbal medicines; pain relievers, such as aspirin, codeine, or Panadol; antidepressants; antibiotics; sleeping pills; antipsychotics; tranquillizers such as Valium; becoming physically more active; reading about people with similar problems and how they have dealt with them; getting out and about more; attending courses on relaxation, stress management, meditation or yoga; cutting out alcohol altogether; psychotherapy; cognitive behaviour therapy (CBT); hypnosis; being admitted to a psychiatric ward of a hospital; undergoing electroconvulsive therapy; having an occasional alcoholic drink to relax; going on a special diet or avoiding certain foods; consulting a website that give information about the problem; consulting an expert using email or the web; consulting a book giving information about the problem; and receiving information from a health educator. The response scale was helpful, harmful, neither, depends, don’t know. The wording for the interventions across the two surveys remained the same, except that in the survey of health professionals, pain relievers were referred to as analgesics and sleeping pills as sedatives/hypnotics. Respondents were also asked about the likely result if John/Jenny had the sort of professional help that the respondent thought was most appropriate, as well as the likely result if John/Jenny did not receive any professional help. Respondents could select from seven responses: full recovery with no further problem; full recovery, but problems would probably reoccur; partial recovery; partial recovery, but problems would probably reoccur; no improvement; get worse; and don’t know.
Ethics
The two surveys received ethical approval from the Human Research Ethics Committee at the University of Melbourne. The survey of health professionals was also approved by the External Requests Evaluation Committee at the DHS, which conducted the mail-out on our behalf to comply with privacy legislation. Follow up of nonresponders was not permitted by the DHS.
Statistical analysis
Beliefs of each professional group were pooled together, as overall there was a consensus, despite a few notable differences in treatment beliefs (Morgan et al., 2013). Ratings of each intervention were dichotomized with helpful scored 1 and all other responses scored 0. Ratings of likely prognosis with and without professional help were collapsed into four levels for ease of interpretation: full recovery, partial recovery, no improvement, get worse. Responses of “don’t know” were treated as missing. Chi-square tests were used to evaluate whether there were differences between members of the public and health professionals in ratings of helpfulness of interventions and ratings of prognosis. Due to the large number of statistical tests carried out and the large community sample, we used the more conservative p<0.001 as the significance level. We also report Cramer’s V as a measure of the strength of the association, as it can be used with variables that have more than two categories (Field, 2009). Cramer’s V varies from 0 to 1, with small, medium, and large effect sizes represented by 0.1, 0.3, and 0.5, respectively. In this paper, we focus on reporting the differences between the samples, rather than absolute ratings of helpfulness in each sample, as these have already been reported (Reavley and Jorm, 2011).
Results
Helpfulness of interventions for depression
Table 1 shows the percentage of health professionals and members of the public who rated each intervention as helpful for depression and depression with suicidal thoughts. Ratings were broadly similar across the two similar vignettes. There were many significant differences between the public and the professionals in ratings of helpfulness, but most were small in size. Examination of differences that were approximately medium in size reveals that the public gave much higher endorsement of the helpfulness of close friends and much lower endorsement of CBT than professionals. Furthermore, there were several interventions that were rated helpful by a significant minority of the public (approximately 40–50%), but received much lower endorsement by professionals (<10%). These were taking vitamins and minerals, having an occasional alcoholic drink to relax, and using a special diet or avoiding certain foods. Also noteworthy is that, although fewer members of the public thought antidepressants would be helpful, the difference was small in both vignettes.
Interventions rated by public and health professionals as helpful for depression or depression with suicidal thoughts.
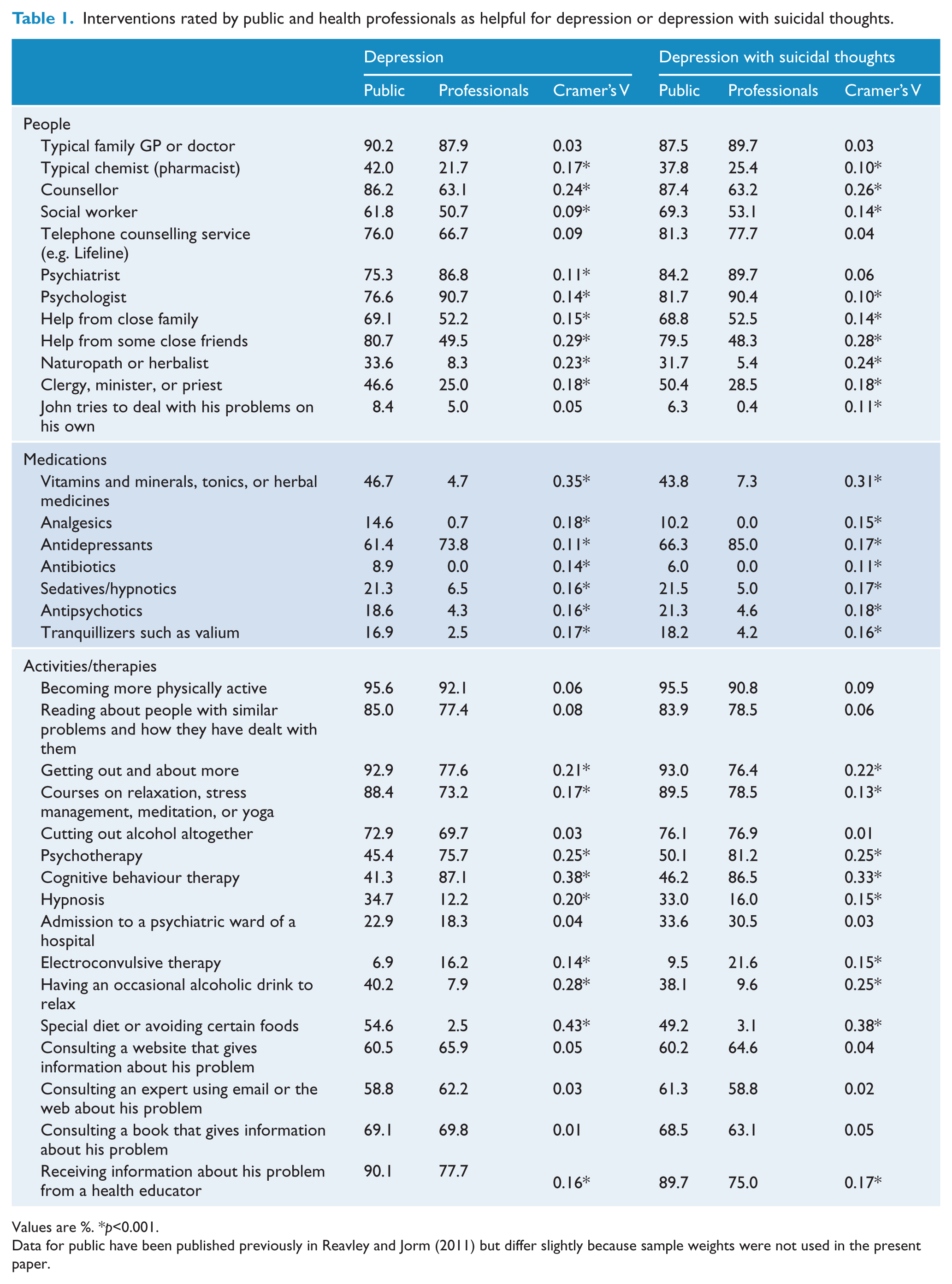
Values are %. *p<0.001.
Data for public have been published previously in Reavley and Jorm (2011) but differ slightly because sample weights were not used in the present paper.
Helpfulness of interventions for schizophrenia
Table 2 presents the results on helpfulness of interventions for early schizophrenia and chronic schizophrenia. There were many significant differences between members of the public and professionals. These differences were largely similar across the two vignettes, but were often small in size. In general, interventions tended to be rated as helpful more often by the public than professionals. A notable exception was antipsychotics, which was endorsed by most professionals but only by about 50% of the public (a medium effect-size). Other medium effects were observed for interventions that a majority of the public believed were helpful but had much lower rates of endorsement by professionals. These were seeing a counsellor, getting help from close friends, taking antidepressants, becoming more physically active, getting out and about more, taking courses on relaxation, using a special diet or avoiding certain foods, and receiving information from a health educator.
Interventions rated by public and health professionals as helpful for early schizophrenia or chronic schizophrenia.
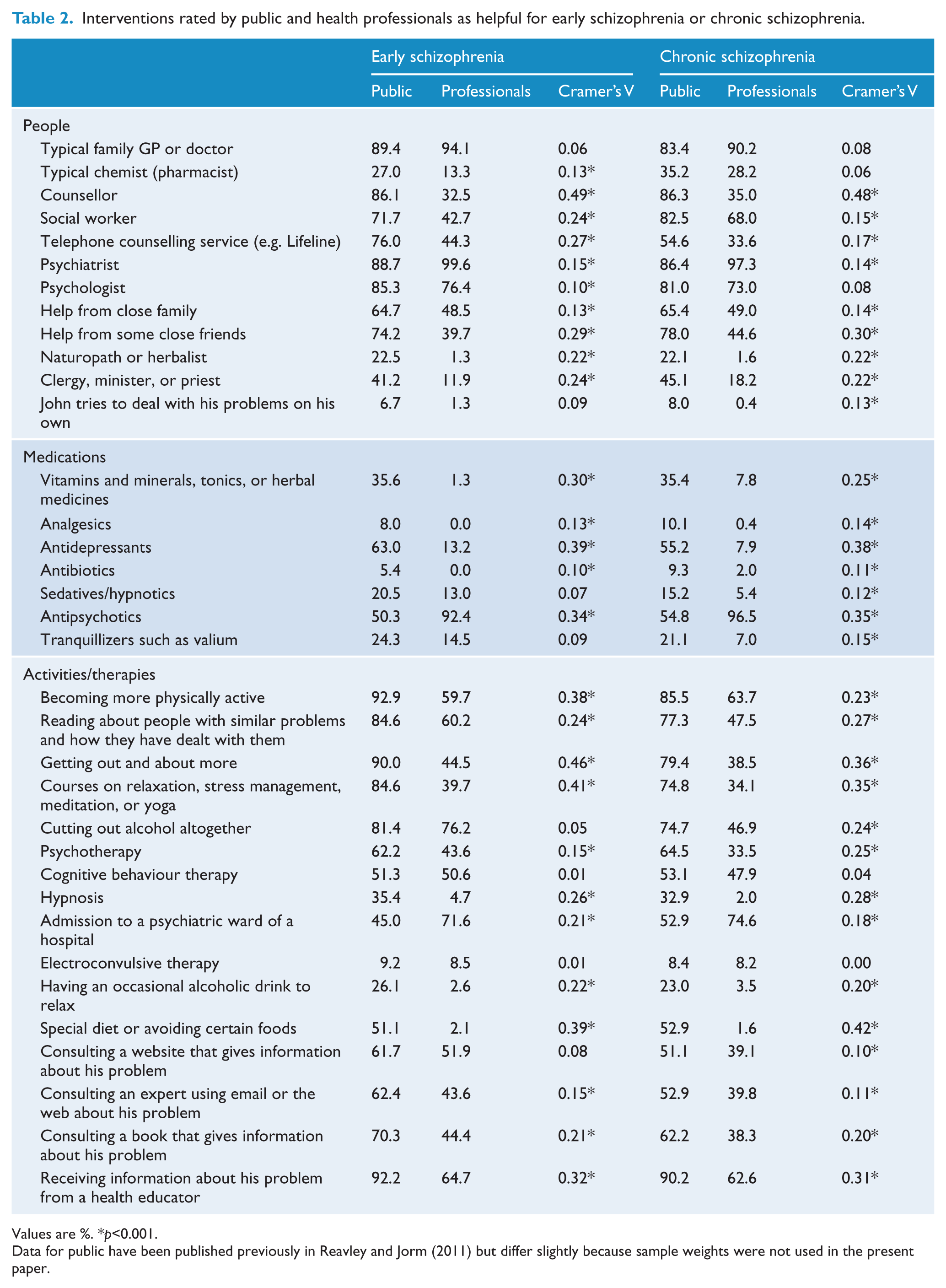
Values are %. *p<0.001.
Data for public have been published previously in Reavley and Jorm (2011) but differ slightly because sample weights were not used in the present paper.
Helpfulness of interventions for anxiety disorders
Ratings of interventions for social phobia and PTSD by the public and professionals are shown in Table 3. Again, we focus on differences between the two samples that were approximately medium in size, given the many significant differences observed. A majority of the public endorsed the helpfulness of counsellors, close family, close friends, and getting out and about more, whereas fewer professionals did so. However, the public had much lower endorsement of CBT than professionals. Similar to the depression vignettes, a sizeable minority of the public, but very few professionals, thought that taking vitamins and minerals, having an occasional alcoholic drink to relax, and using a special diet or avoiding certain foods would be helpful.
Interventions rated by public and health professionals as helpful for social phobia or post-traumatic stress disorder.
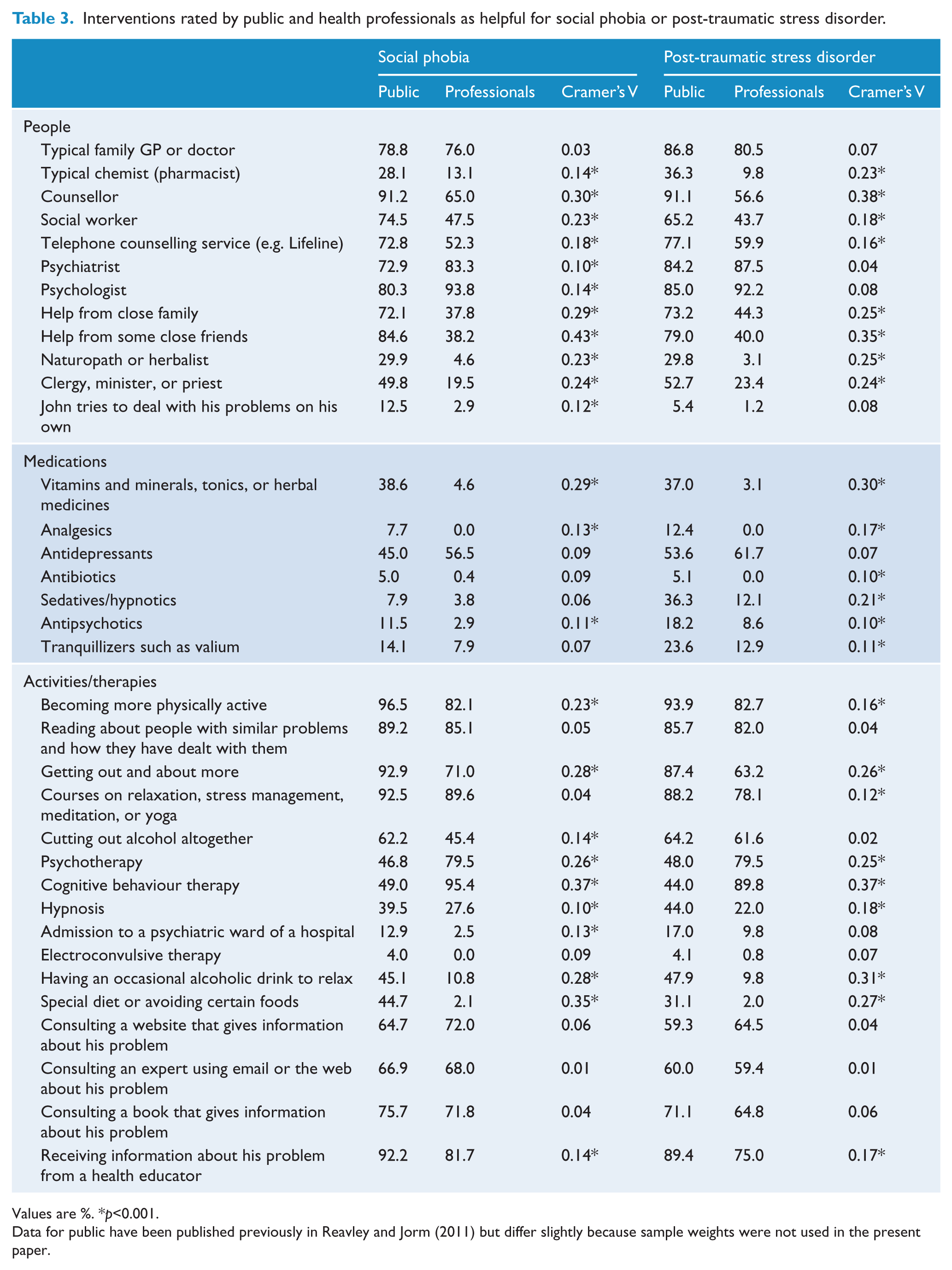
Values are %. *p<0.001.
Data for public have been published previously in Reavley and Jorm (2011) but differ slightly because sample weights were not used in the present paper.
Likely prognosis with and without professional help
As shown in Table 4, for both depression vignettes, the professionals were more optimistic about full recovery with professional help than the public were. Conversely, the public thought that depression would get worse without treatment, whereas the professionals showed more varied predictions, with partial recovery a strong possibility in addition to getting worse.
Beliefs of public and health professionals about likely prognosis with and without professional help for depression, depression with suicidal thoughts, early schizophrenia, chronic schizophrenia, social phobia, and post-traumatic stress disorder.
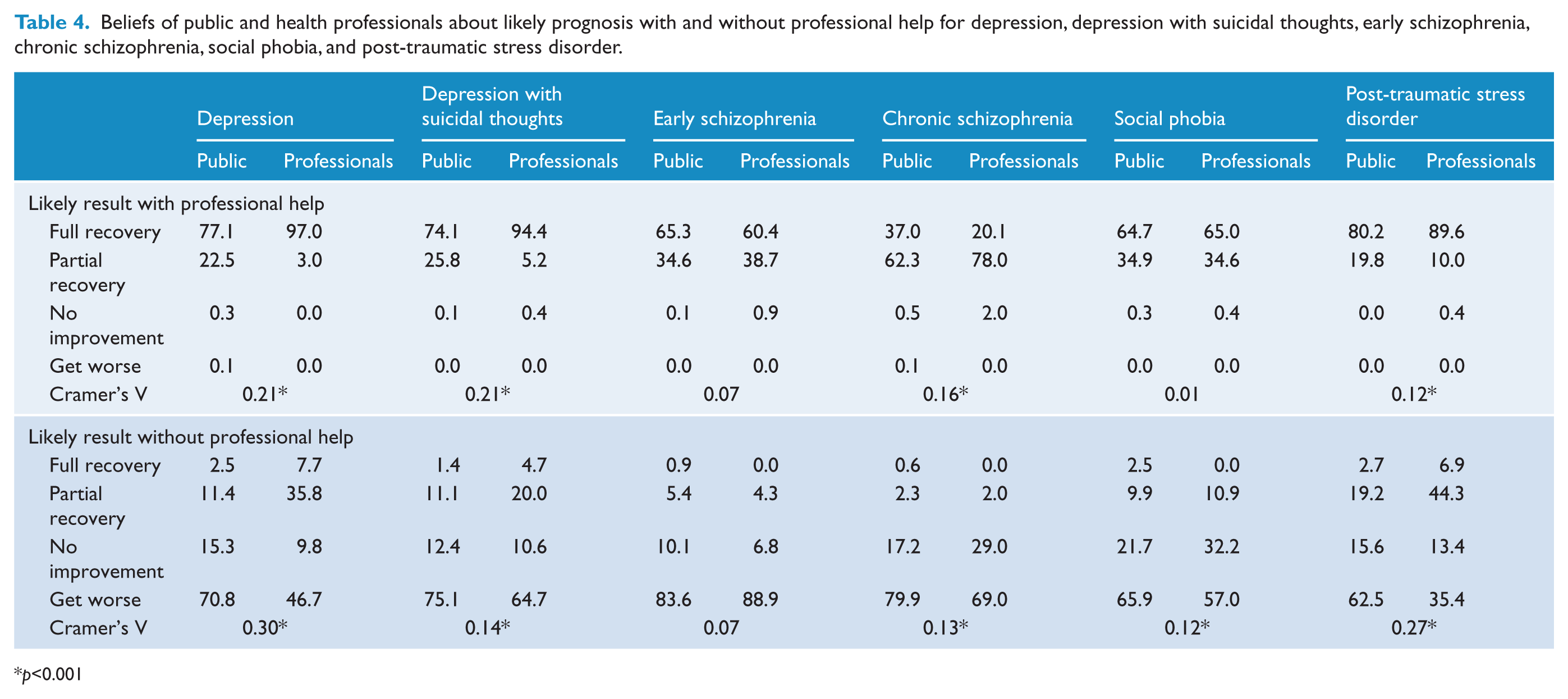
p<0.001
There were no significant differences between the public and professionals for the likely result with or without professional help for early schizophrenia: most agreed it would get worse without treatment, and that with treatment, there would be full or partial recovery.
There was a small difference in beliefs about outcomes for chronic schizophrenia with professional help, as more professionals thought there would be partial recovery rather than full recovery. Outcomes without professional help were fairly similar across the two samples, but fewer professionals thought it would get worse; instead, some indicated that there would be no improvement.
Both the public and professionals predicted similar outcomes for social phobia with professional help. There was a small difference in the outcome from no professional help, with slightly more professionals predicting no improvement and somewhat fewer predicting getting worse compared with the public.
For PTSD, there was a small difference in beliefs about outcome after receiving professional help, with professionals more optimistic about full recovery than the public. Professionals tended to indicate a better prognosis without professional help than the public, as a significant proportion thought that there would be partial recovery and fewer thought that it would get worse.
Discussion
This paper sought to clarify whether differences between health professionals and members of the public remain in beliefs about the effectiveness of mental health treatments and prognosis. It appears that most of the large gaps in treatment beliefs identified in the 1990s have narrowed, although there is still room for improvement. Some gaps have narrowed or closed because beliefs of the public have moved closer to professionals, whereas for others, change has occurred in both groups. Sizeable differences in intervention beliefs between the two groups are largely consistent across vignettes and relate to the greater belief by the public in the helpfulness of close family or friends, a counsellor, vitamins and minerals, a special diet or avoiding certain foods, and having an occasional alcoholic drink to relax; and greater belief by professionals in psychotherapy and CBT, as will be discussed further. Findings on prognosis differ across mental disorders, but any differences between the public and professionals were only small or medium in size. With the exception of early schizophrenia, the public tended to believe that, without treatment, mental disorders would get worse, whereas professionals predicted a range of possible outcomes including partial recovery, no improvement, and getting worse. The other notable difference was in the prognosis of depression with treatment, where the public were less optimistic about full recovery than professionals. Comparing the current findings with previous surveys, it appears that professional beliefs have remained stable over time, but the public has become slightly less optimistic about full recovery (Jorm et al., 1997c; Reavley and Jorm, 2012).
There is now only a small gap in beliefs about the helpfulness of antidepressants for depression. Previously, the public tended to view antidepressants as harmful, whereas professionals almost universally endorsed their effectiveness (Jorm et al., 1997c). Over time, the public has warmed to antidepressants, but interestingly the views of professionals have tempered somewhat, with responses of “depends” from a significant minority of professionals (Morgan et al., 2013). This change may have been influenced by several meta-analyses that have suggested antidepressant efficacy is equivocal in mild-to-moderate depression (Fournier et al., 2010; Kirsch et al., 2008). Furthermore, the public’s belief in the helpfulness of antidepressants for depression has spread to the treatment of schizophrenia. As few professionals shared this view, there was a medium-to-large discrepancy in beliefs. It should be noted, though, that over the same period the early schizophrenia vignette has increasingly been described as depression by members of the public (Reavley and Jorm, 2012).
Members of the public endorsed informal sources of help such as friends and family for all disorders, whereas professionals were less likely to believe them helpful. This is consistent with previous reports in Australia and other countries (Jorm, 2012). Turning to family and friends for help is not problematic if they provide appropriate support, or if professional help is also sought. However, community members often report they are not confident in assisting someone with a mental health problem, and a substantial minority do not encourage professional help (Jorm and Kitchener, 2011). Promising steps have occurred to improve the support and assistance that community members provide to people with a mental disorder, as mental health first aid training has grown to reach at least 1% of the Australian adult public so far (Jorm and Kitchener, 2011).
Also consistent across disorders was the difference between professionals and the public in beliefs about the helpfulness of counsellors, with members of the public rating them higher than professionals. Whilst it is encouraging that the public’s belief in the helpfulness of psychiatrists and psychologists has moved closer to the beliefs of professionals since 1995, (particularly in contrast to some European countries, where almost a third believe that professional care for mental health problems is worse than or equal to no help (ten Have et al., 2010)), the public still typically rated counsellors as more helpful than psychiatrists or psychologists. The reasons for this are unclear, as psychiatrists and psychologists are registered professionals wedded to science-based practice, unlike “counsellors”. Although ratings of psychiatrists and psychologists have improved over the years, beliefs in the main treatment modalities they provide for depression and anxiety (e.g. psychotherapy, CBT, antidepressants) have not increased to the same degree. It may be thought that this is because the public is unfamiliar with the terms used (e.g. CBT), but the generic term “psychotherapy” was also not highly endorsed. As only half of Australian adults believe that psychotherapy/CBT is helpful for depression or anxiety, these could be targets for improvement. Indeed, the American Psychological Association has recognized the poor image of psychotherapy in the eyes of the American public and has launched initiatives aimed at improving the awareness of psychotherapy and its effectiveness (Anderson, 2012).
There was a reliable pattern of public/professional differences across disorders about the helpfulness of vitamins and minerals, tonics, and herbal medicines, a special diet or avoiding certain foods, and having an occasional drink to relax. While these were rarely endorsed by professionals, a substantial minority of the public believed them to be helpful. Indeed, the public’s belief in the helpfulness of a special diet has increased over the years (Reavley and Jorm, 2012). These beliefs could be targeted for improvement. Several lifestyle activities were highly rated by the public for each of the mental health problems in this study: becoming more physically active, reading about people with similar problems, getting out and about more, and courses on relaxation. Even though the percentage of professionals rating these as helpful has increased over the years (Morgan et al., 2013), some significant differences remain between the two groups because members of the public also changed their beliefs over the period (Reavley and Jorm, 2012). These gaps are especially notable for schizophrenia, where fewer professionals believe these interventions to be helpful.
This study has several limitations, which suggest caution in interpretation of results. The response rate for health professionals was quite low, which suggests the professional sample may not be representative of the three professional groups in Australia. Our sample of professionals was somewhat overrepresented by female GPs, older GPs, and older psychiatrists, but was well matched in age and gender against the population of clinical psychologists. It is difficult to predict how this may have impacted on ratings of helpfulness or prognosis, given that our samples were not large enough to investigate age and gender differences. The response rate from the professional survey in 1996 was much higher (61% to 75% depending on the profession), but response rates from postal surveys of health professionals have been getting smaller over time (Cook et al., 2009) and a similar study of mental health literacy in Australian pharmacists reported a similar rate of response (O’Reilly et al., 2010). Another limitation is that the survey was based on a constrained vignette of a person with a mental disorder, which was designed to be simple for the public, but gave only a limited clinical picture for professionals to work from. Responses were also limited in that they could not convey the strength of helpfulness of interventions or the reasons for each belief. Finally, different methodologies were used to collect data from the public (telephone interview) and the professionals (postal survey).
With these limitations in mind, the study gives an updated comparison of whether the public has similar beliefs to health professionals on the effectiveness of mental disorder treatments. Overall, the results indicate a better picture than in the 1990s, particularly for depression, with the views of the public and professionals more aligned and few large gaps in treatment beliefs. Nevertheless, there remain some areas that could be improved, such as the relatively low endorsement of psychotherapy or CBT for depression and anxiety disorders.
Footnotes
Acknowledgements
We thank the Commonwealth Department of Human Services for conducting the mail-out to the health professionals and for providing the data on the population age and gender distribution of general practitioners, psychiatrists, and clinical psychologists.
Funding
This research was funded by an NHMRC Australia Fellowship, NHMRC Program Grant 566529 and the Commonwealth Government Department of Health and Ageing.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.