
Abstract
Objective:
The aim of this study was to develop scales to assess mental health literacy relating to affective disorders, anxiety disorders and schizophrenia/psychosis.
Method:
Scales were created to assess mental health literacy in relation to depression, depression with suicidal thoughts, early schizophrenia, chronic schizophrenia, social phobia and post-traumatic stress disorder using data from a survey of 1536 health professionals (general practitioners, clinical psychologists and psychiatrists), assessing recognition of these disorders and beliefs about the helpfulness of interventions. This was done by using the consensus of experts about the helpfulness and harmfulness of treatments for each disorder as a criterion. Data from a general population survey of 6019 Australians aged ≥ 15 was used to examine associations between scale scores, exposure to mental disorders and sociodemographic variables, to assess scale validity.
Results:
Those with a close friend or family member with a mental disorder had significantly higher mean scores on all mental health literacy scales, providing support for scale validity. Personal experience of the problem and working with people with a similar problem was linked to higher scores on some scales. Male sex, a lower level of education and age > 60 were linked to lower levels of mental health literacy. Higher scores were also linked to a greater belief that people with mental disorders are sick rather than weak.
Conclusions:
The scales developed in this study allow for the assessment of mental health literacy in relation to depression, depression with suicidal thoughts, early schizophrenia, chronic schizophrenia, social phobia and PTSD. Those with exposure to mental disorders had higher scores on the scales, and analyses of the links between scale scores and sociodemographic variables of age, gender and level of education were in line with those seen in other studies, providing support for scale validity.
Introduction
Mental health literacy has been defined as ‘knowledge and beliefs about mental disorders which aid their recognition, management or prevention’ (Jorm et al., 1997a). Poor mental health literacy reduces the likelihood of receiving appropriate treatment for a mental disorder, increasing the risk of adverse long-term outcomes (Gulliver et al., 2010; Thompson et al., 2008; Wang et al., 2003). In the context of evidence that approximately two-thirds of those who meet the criteria for a mental disorder fail to seek professional help (Burgess et al., 2009), surveys in a number of countries have assessed mental health literacy in the general population (Angermeyer et al., 1993; Croghan et al., 2003; Magliano et al., 2004, Priest et al., 1996). In Australia, these include the national surveys of mental health literacy in the adult population that were carried out in 1995, 2003–2004 and 2011 (Jorm et al., 1997a; Jorm et al., 2005; Reavley and Jorm, 2011a).
These surveys have largely focused on the recognition of mental disorders, often described in vignettes, and beliefs about appropriate treatments. Recognition of a problem is typically the necessary first step to seeking help from an appropriate professional, with failure to recognise signs and symptoms as indicating a mental disorder likely to delay help-seeking (Gulliver et al., 2010). Beliefs about the helpfulness of interventions also impact on help-seeking and treatment compliance; for example, someone with a negative attitude towards antidepressants may be less likely to be prescribed these medications, less likely to fill prescriptions and less likely to benefit overall (Pyne et al., 2005). Surveys in several countries have shown that negative attitudes towards medications such as antipsychotics and antidepressants are common, while psychological and complementary therapies and self-help strategies tend to be viewed more positively (Angermeyer et al., 1993; Angermeyer et al., 2005; Jorm et al., 1997a; Priest et al., 1996).
One of the principal ways in which the mental health literacy of the general population may be assessed is by comparing recognition of disorders and beliefs about treatments with those of health professionals (Dunn et al., 2009; Lauber et al., 2005). In this way, the beliefs of health professionals act as a standard by which to assess the beliefs of members of the public. In 1996, in an attempt to compare public and professional beliefs, Jorm and colleagues conducted surveys of Australian general practitioners (GPs), psychiatrists and clinical psychologists on their beliefs about interventions and outcomes for depression and schizophrenia (Jorm et al., 1997b). In 2012, this survey was again carried out to assess differences between professional groups and whether beliefs had changed in the period between the surveys (Morgan et al., 2013b).
In these surveys, comparison between groups was done on an item-by-item basis. However, composite scale scores offer the advantage of being able to assess mental health literacy on a continuum, thus enabling quantitative analyses of links with other variables and comparisons between different populations and population groups. The current study aimed to build on and extend previous work by using data from the 2012 survey of health professional beliefs to develop scales to quantify mental health literacy in the general population in relation to depression, depression with suicidal thoughts, early schizophrenia, chronic schizophrenia, social phobia and post-traumatic stress disorder (PTSD). A further aim was to assess the relationships between scale scores and sociodemographic factors and exposure to mental disorders to explore scale validity.
Methods
General community survey
The general community survey involved computer-assisted telephone interviews with a national sample of 6019 people aged ≥ 15 (Reavley and Jorm, 2011a). The survey was carried out by the survey company Social Research Centre. A dual frame approach was used, with the sample contacted by random-digit dialling of both landlines and mobile phones. Interviews were conducted between January and April 2011. The response rate for the survey was 44.0% (40.8% for the landline sample and 47.3% for the mobile phone sample), defined as completed interviews (6019) out of sample members who could be contacted and were confirmed as in scope (13,636). Overall, 4324 interviews were conducted on landlines and 1696 on mobiles.
Survey interview
The interview was based on a vignette of a person with a mental disorder. On a random basis, respondents were read one of six vignettes: depression, depression with suicidal thoughts, early schizophrenia, chronic schizophrenia, social phobia and PTSD. Respondents were also randomly assigned to receive either male (John) or female (Jenny) versions of the vignette. All vignettes were written to satisfy the diagnostic criteria for either major depression or schizophrenia according to the Diagnostic and Statistical Manual of Mental Disorders, fourth edition and the International Classification of Diseases, 10th edition and have been published previously (Jorm et al., 2005; Reavley and Jorm, 2011a). The numbers of respondents assigned to each vignette were: depression (1016); depression with suicidal thoughts (1008); early schizophrenia (1002); chronic schizophrenia (993); social phobia (992); and PTSD (1008). There were no significant differences between vignettes in regard to age, sex, marital status, level of education, country of birth and location of respondents.
After being presented with the vignette, respondents were asked what, if anything, they thought was wrong with the person described in the vignette, how the person could best be helped and a series of questions about the likely helpfulness of a wide range of interventions (rated as likely to be helpful, harmful or neither for the person described in the vignette). The interventions were: a typical GP or family doctor; a typical chemist (pharmacist); a counsellor; a social worker; a telephone counselling service, such as Lifeline; a psychiatrist; a psychologist; help from close family; help from close friends; a naturopath or a herbalist; the clergy, a minister or priest; John/Jenny tried to deal with his problems on his own; vitamins and mineral, tonics or herbal medicines; pain relievers, such as aspirin, codeine or Panadol; antidepressants; antibiotics; sleeping pills; antipsychotics; tranquillisers, such as Valium; becoming physically more active; reading about people with similar problems and how they have dealt with them; getting out and about more; attending courses on relaxation, stress management, meditation or yoga; cutting out alcohol altogether; psychotherapy; cognitive behavioural therapy; hypnosis; being admitted to the psychiatric ward of a hospital; undergoing electroconvulsive therapy; having an occasional alcoholic drink to relax; going on a special diet or avoiding certain foods; consulting a website that gives information about the problem; consulting an expert using email or the Web; consulting a book giving information about the problem; and receiving information from a health educator.
The rest of the interview involved questions on beliefs about long-term outcomes, knowledge of causes and risk factors, beliefs associated with stigma and discrimination, contact with people like those in the vignette and the health of the respondent. Only the questions relevant to the analyses in this article are described in more detail here. To assess contact with people like those in the vignette, respondents were asked the following:
Has anyone in your family or close circle of friends ever had problems similar to John’s?
Have they received any professional help or treatment for these problems?
Have you ever had problems similar to John’s?
Have you received any professional help or treatment for these problems? and
Have you ever had a job that involved providing treatment or services to a person with a problem like John’s?
Survey of health professionals
Participants
The methods of the survey of health professionals have been previously described (Morgan et al., 2013b) A questionnaire was posted to 6848 health professionals registered with Medicare Australia in June 2012. The sample of professionals consisted of a random sample of 3000 GPs who had provided more than 50 services in the past year, a random sample of 1800 registered clinical psychologists and all active psychiatrists (2048). We obtained 1536 returned surveys from 518 GPs, 506 psychiatrists and 498 clinical psychologists (14 respondents did not indicate a profession). Response rates were 17.3%, 24.7% and 27.7%, respectively. Responses for each of the six vignette types were: depression (280), depression with suicidal thoughts (261), early schizophrenia (237), chronic schizophrenia (259), social phobia (242) and PTSD (257).
Questionnaire
The questionnaire was based on that used for the phone interviews with members of the general population described previously. On a random basis, respondents were sent a questionnaire with one of six vignettes, stratified by profession type. In this survey, all vignettes referred to a male (John) as, due to the fact that the surveys were distributed by a third party and returned anonymously, it was not possible to ensure equal numbers of male and female vignettes. Furthermore, previous research on members of the Australian public in which the sex of the vignette was randomized found that it made very little difference to responses (Jorm et al., 1997c).
After being presented with the vignette, respondents were asked what, if anything, they thought was wrong with the person described in the vignette and a series of questions about the likely helpfulness of the interventions listed previously. In the survey of health professionals, pain relievers were referred to as analgesics and sleeping pills as sedatives/hypnotics.
Respondents were also asked questions about the likely outcome for the person in the vignette if they received professional help and if they did not. Stigmatising attitudes were also assessed. Data relating to these questions is not relevant to the aims of the current study and will be reported elsewhere (Reavley et al., 2013, submitted).
Coding of open-ended responses
Responses to the question of what was wrong with the person in the vignette were coded based on the pre-coded categories similar to those used in previous surveys (Jorm et al., 1997a; Wright et al., 2005). For the general community survey, these are described in more detail elsewhere (Reavley and Jorm, 2011a). For this study, responses to the depression and depression with suicidal thoughts vignettes were coded with a Yes if depression was mentioned. For the early schizophrenia and chronic schizophrenia vignettes, responses of either psychosis, psychotic disorder or schizophrenia were coded as Yes. For the social phobia vignette, responses were coded with a Yes if social phobia, social anxiety or social anxiety disorder were mentioned. For the PTSD vignette, responses were coded with a Yes if PTSD was mentioned.
The mental disorders described in the vignettes were correctly identified by the majority of professionals, supporting the validity of the vignettes. Depression was identified by 95% of professionals in both depression vignettes, and 12% also identified suicidal thoughts in the depression with suicidal thoughts vignette. Ninety-five percent of professionals identified psychosis, a psychotic disorder, or schizophrenia in the early and chronic schizophrenia vignettes, 90% of professionals identified PTSD in the PTSD vignette, and 86% identified social phobia or social anxiety in the social phobia vignette.
Scale development
Data from the survey of health professionals was used to identify items to be included in the scales to assess mental health literacy for each vignette. In both the 1996 and 2012 surveys, consensus on intervention helpfulness was defined as occurring when at least 66% of each profession rated an intervention as helpful and consensus on harmfulness was defined as occurring when at least 50% or each profession rated an intervention as harmful. To maintain a consistent approach and to allow for comparisons between studies, the same convention was followed in this study. We considered it appropriate to use data on helpfulness beliefs from all professional groups combined as, for the items which received ratings above 66%, the effect size of the difference between groups reached small to medium only in regard to antidepressants for depression with suicidal thoughts (95% for GPs, 90% for psychiatrists and 72% for clinical psychologists) (Morgan et al., 2013b). As outlined in that study, interventions rated as helpful by over 66% of each profession largely reflected the evidence base and the clinical practice guidelines.
For helpfulness and harmfulness beliefs, the interventions used to develop the scales were as follows:
Scale scoring
For each vignette a scale score was calculated on the following basis: one point was given for correct recognition of the disorder described, one point for every intervention listed previously in this article that was classified as helpful and one point for every intervention listed previously that was classified as harmful. Consideration was given to the option of item weighting, in this case assigning a greater weight to the item relating to correct recognition. However, given evidence of the limited psychometric or practical benefits of weighting, this option was not taken (Downey, 1979).
Statistical analysis
Descriptive statistics for the scales were calculated. To explore the differences between subgroups, linear regression models were generated with scale scores as dependent variables and the following as predictor variables: sex, age, level of education, country of birth, language spoken at home, having a family member or friend with the problem described in the vignette, having personal experience of the problem and working with people with the problem. A second set of regression models was generated with scale scores as dependent variables and scales assessing stigmatising attitudes as predictor variables. These scales assess personal stigmatising attitudes and attitudes perceived in others (Reavley and Jorm, 2011b) and are defined as the personal weak not sick, personal dangerous/unpredictable, perceived weak not sick and perceived dangerous/unpredictable (Yap et al., 2013). Self-reported willingness to have contact with the person described in the vignette was assessed using the five-item social distance scale developed by Link et al. (1999). These analyses were adjusted for sex, age, level of education, country of birth, language spoken at home, having a family member or friend with the problem, having personal experience of the problem and working with people with the problem.
A pre-weight was applied to adjust for the dual frame design and the respondent chance of selection. The achieved sample was close to the Australian national population in terms of geographical distribution; however, there was an under-representation of men and of younger adults, and an over-representation of university-educated persons and persons with an English-speaking background. A population weight was used to adjust for these biases. All analyses were performed using Intercooled Stata 12 (StataCorp LP, College Station, Texas, USA).
Results
Descriptive statistics for the scales are given in Table 1. Regression analyses exploring differences in scale scores according to sociodemographic characteristics, personal experience of mental disorders and exposure to those with the disorders are given in Table 2. Regression analyses exploring differences in scale scores according to stigmatising attitudes are given in Table 3.
Descriptive statistics for mental health literacy scales.
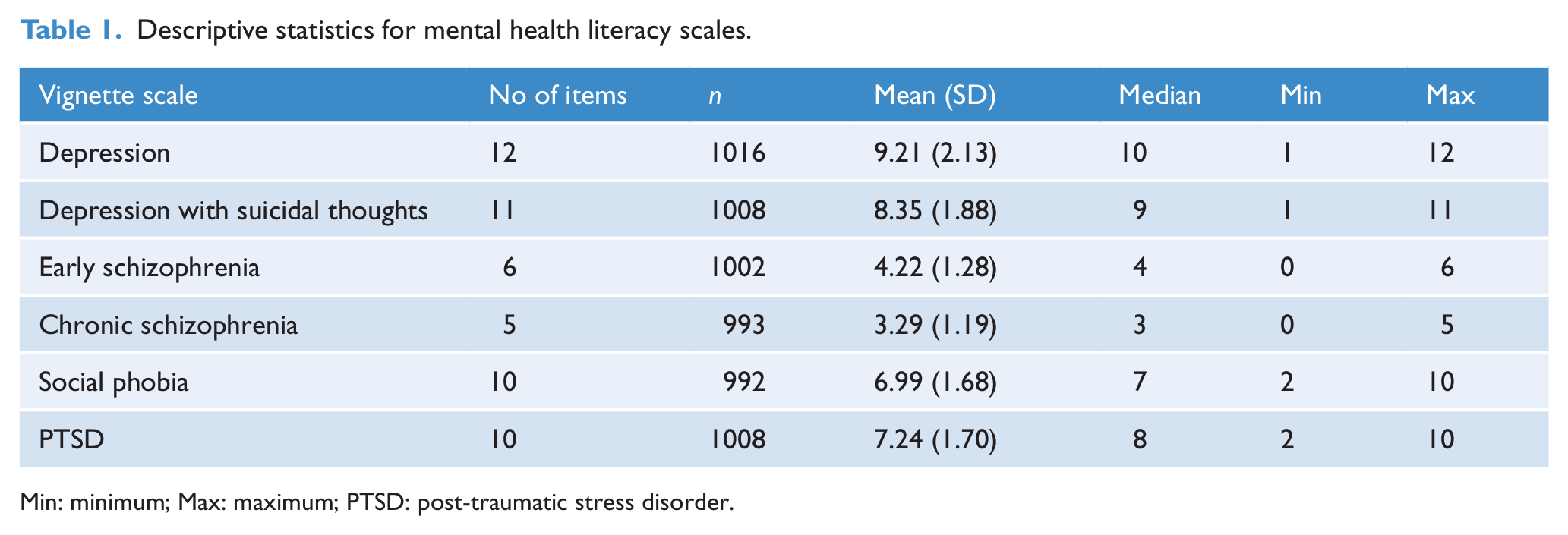
Min: minimum; Max: maximum; PTSD: post-traumatic stress disorder.
Summary of linear regressions exploring differences in scale scores according to sociodemographic characteristics and exposure to mental disorders.
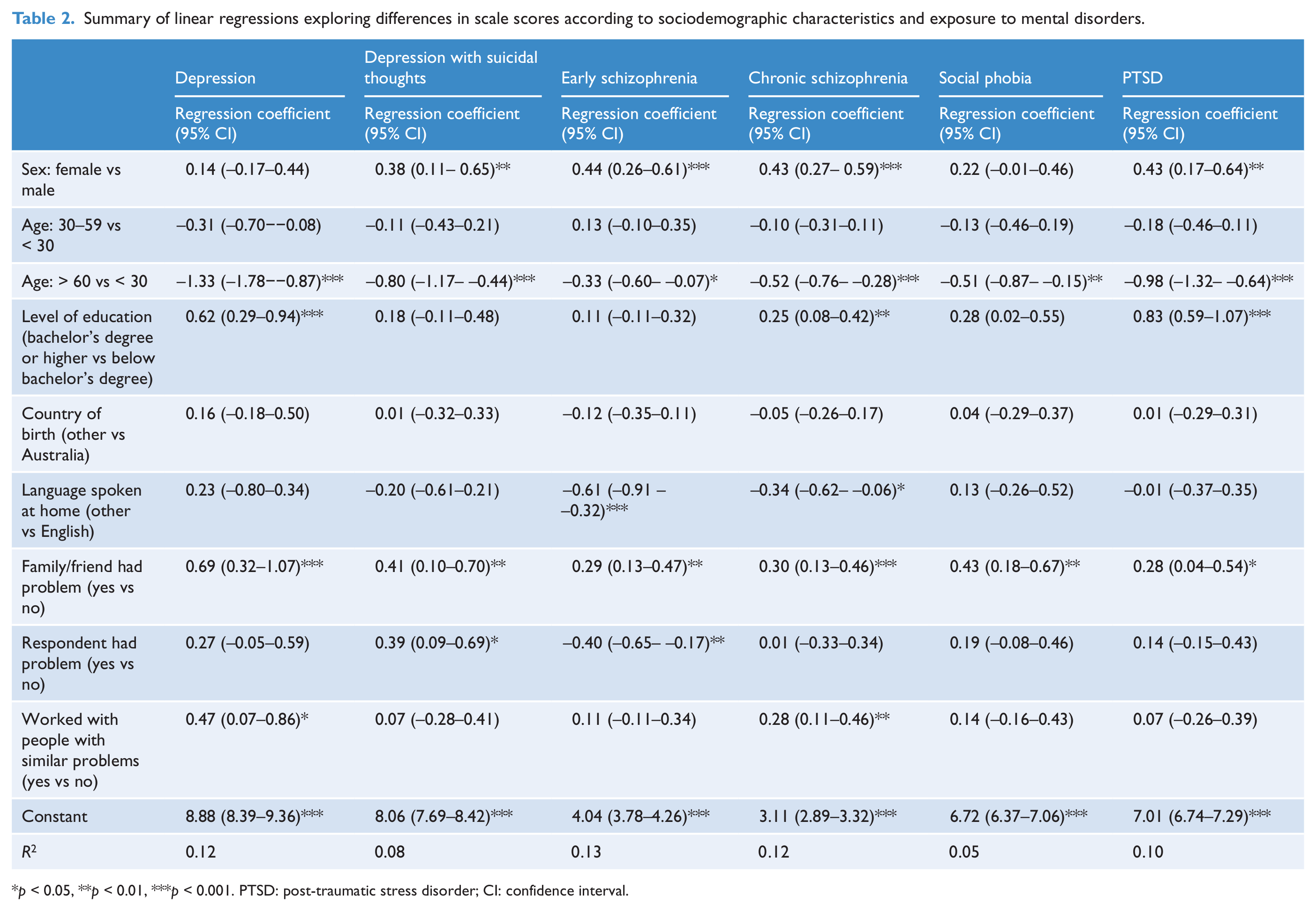
p < 0.05, **p < 0.01, ***p < 0.001. PTSD: post-traumatic stress disorder; CI: confidence interval.
Summary of linear regressions exploring differences in scale scores according to stigmatising attitudes.
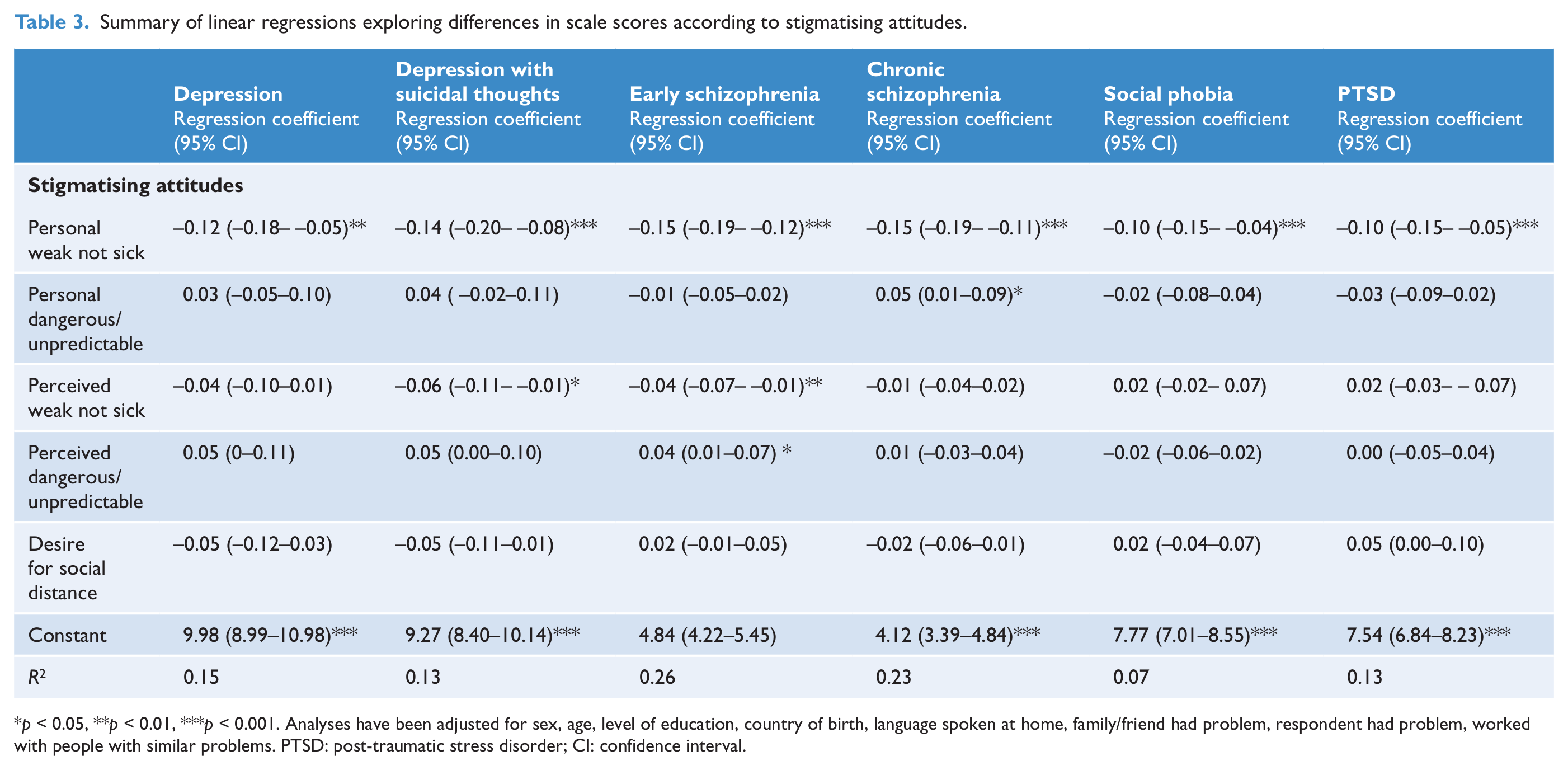
p < 0.05, **p < 0.01, ***p < 0.001. Analyses have been adjusted for sex, age, level of education, country of birth, language spoken at home, family/friend had problem, respondent had problem, worked with people with similar problems. PTSD: post-traumatic stress disorder; CI: confidence interval.
Sociodemographic factors
Female sex was associated with significantly higher scores on the depression with suicidal thoughts, early schizophrenia, chronic schizophrenia and PTSD mental health literacy scales. Compared to those aged < 30 years, age > 60 years was associated with significantly lower scores on all scales. Having qualifications at bachelor’s level and above was associated with significantly higher scores on the depression, chronic schizophrenia and PTSD mental health literacy scales. Speaking a language other than English at home was significantly associated with lower scores on the early schizophrenia and chronic schizophrenia mental health literacy scales.
Exposure to mental disorders
The percentages [95% confidence interval (CI)] of those who had a close friend or family member who had experienced a problem similar to that described in the vignette were as follows: depression 67.6% (64.3–70.9), depression with suicidal thoughts 62.4% (58.9–65.9), early schizophrenia 51.7% (48.2–55.2), chronic schizophrenia 36.7% (33.4–40.1), social phobia 52.4% (48.8–56.0) and PTSD 46.0% (42.5–49.5) Having a friend or family member with a problem similar to that described in the vignette was significantly associated with higher scores on all scales.
Percentages (95% CI) of those who had experienced a problem similar to that described in the vignette were as follows: depression 33.0% (29.7–36.4), depression with suicidal thoughts 26.8% (23.8-30.1), early schizophrenia 13.3% (11.1-15.9), chronic schizophrenia 8.2% (6.5-10.3), social phobia 27.5% (24.3–30.8) and PTSD 21.8% (19.0-24.8). Having experienced a problem similar to that described in the vignette was significantly associated with higher scores on the depression with suicidal thoughts mental health literacy scale and with lower scores on the early schizophrenia mental health literacy scale.
Percentages (95% CI) for those who worked with people with mental health problems were as follows: depression 17.3% (14.8–20.0), depression with suicidal thoughts 17.8% (15.4–20.6), early schizophrenia 20.2% (17.5–23.1), chronic schizophrenia 20.8% (18.1–23.7), social phobia 17.4% (15.0–20.2) and PTSD 17.1% (14.5–19.9). Having worked with people with such problems was significantly associated with higher scores on the depression and chronic schizophrenia mental health literacy scales.
Stigmatising attitudes
Lower scores on the personal weak not sick scale were significantly associated with higher scores on all mental health literacy scales. Higher scores on the personal dangerous/unpredictable scale were significantly associated with higher scores on the chronic schizophrenia mental health literacy scale. Lower scores on the perceived weak not sick scale were significantly associated with higher scores on the depression with suicidal thoughts and early schizophrenia mental health literacy scales. Higher scores on the perceived dangerous/unpredictable scale were significantly associated with higher scores on the early schizophrenia mental health literacy scale. Thus, a higher level of mental health literacy regarding these disorders is linked to a greater belief in them as illnesses rather than weakness.
Discussion
This article reports on the development of scales to assess mental health literacy in relation to depression, depression with suicidal thoughts, early schizophrenia, chronic schizophrenia, social phobia and PTSD. Scales were based on the correct recognition of the disorder as described in a vignette and agreement with health professionals about which treatments would be helpful. The validity of the scales is supported by the findings that those with exposure to mental disorders typically had significantly higher mean scores. Analyses of the links between scale scores and sociodemographic variables of age, sex and level of education were also in line with those seen in other studies, providing further support for scale validity.
Having a family member or a close friend with a problem similar to that described in the vignette predicted significantly higher scores on all scales. Knowing someone with a mental disorder is relatively common and those in contact with someone with a disorder would be more likely to recognise signs and symptoms as being linked to a particular diagnosis and would also be likely to know about the types of treatments (helpful or unhelpful) undertaken by the person. Thus, these results strongly support the validity of the scales.
There was no clear pattern of association between personal experience of a problem similar to that described in the vignette and scale scores, with personal experience predicting significantly higher scores on only the depression with suicidal thoughts mental health literacy scale. There is evidence that experience of treatments is linked to beliefs about helpfulness (Aikens et al., 2008; Dahlberg et al., 2008), and it is possible that the relatively small numbers of people experiencing problems similar to the lower prevalence disorders led to insufficient statistical power to detect differences in these scales. In addition, the scales relating to early and chronic schizophrenia have fewer items and lower scale reliability.
The finding that working with people with similar problems did not predict significantly higher scores on all scales (but only on the depression and chronic schizophrenia mental health literacy scales) may be explained by the wide range of people in such roles, not all of whom would be expected to have expertise in mental health problems. Percentages of respondents in this category were also lower than those with a close friend or family member with problems, thus reducing the power to detect differences.
The association between male sex and lower scores on all scales other than those relating to depression and social phobia is consistent with other literature suggesting that female sex is associated with better mental health literacy (Burns and Rapee, 2006; Cotton et al., 2006; Swami, 2012). Lower scores for older respondents (≥ 60 years) also reflect the findings in other studies showing that older people are less likely to recognise depression in a vignette and less likely to believe that health professionals are helpful (Fisher and Goldney, 2003; Hasin and Link, 1988). Lower levels of mental health literacy in those with lower education have also been seen in other studies (Dunn et al., 2009; Kaneko and Motohashi, 2007). In the current study, scores were lower in those speaking a language other than English only for the scales relating to early and chronic schizophrenia. This finding indicates that they have less knowledge of the specialist mental health-care systems, perhaps because of language barriers or because they have come from other countries with different health-care systems.
It is often argued that improving mental health literacy can reduce stigmatising attitudes towards people with mental disorders. However, while mental health literacy has improved in recent years, particularly in regard to improved understanding of the biological causes of mental illness, this has not been accompanied by similar positive changes in stigmatising attitudes (Schomerus et al., 2012). The analysis of links between the mental health literacy scales and the stigma scales presented here is in line with these findings, i.e. a higher level of mental health literacy is linked to a greater belief in these disorders as illnesses rather than weakness. However, increased scores on the mental health literacy scales were not associated with a reduced belief in dangerousness/unpredictability or reduced desire for social distance.
Limitations of the study include the lack of assessment of aspects of mental health literacy other than recognition and beliefs about helpfulness of interventions. These include causes and risk factors which, due to the desire to minimise respondent burden, were not included in the health professionals’ survey. Thus, these scales are appropriate for use when the aim is to assess recognition and help-seeking, but other measures would need to be developed to assess other aspects of mental health literacy. The small number of items in some scales, notably the chronic schizophrenia mental health literacy scale, also limits the usefulness of the scales.
Further research is necessary to explore the validity and usefulness of the scales. This may include assessing associations with help-seeking for mental health problems and mental health first-aid behaviours. Such research should also explore the usefulness of the scales in other populations, which may have different health systems, and conceptualisations about mental disorders.
Conclusions
In an extension of previous work which enabled comparisons between groups in the areas of mental disorder recognition and treatment beliefs on an item-by-item basis, the scales developed in this study allow for the assessment of a continuum of mental health literacy in relation to depression, depression with suicidal thoughts, early schizophrenia, chronic schizophrenia, social phobia and PTSD. Those with more exposure to mental disorders had higher scores on the scales and analyses of the links between scale scores and sociodemographic variables of age, sex and level of education were in line with those seen in other studies, providing support for scale validity. Further work would need to explore the validity and usefulness of the scales in other contexts.
Footnotes
Acknowledgements
We would like to thank the Commonwealth Department of Human Services for conducting the mail-out to the health professionals.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
The General Community study was funded by the Commonwealth Government Department of Health and Ageing. The authors receive salary support from the National Health and Medical Research Council.